
Vol. 25 - Num. 97
Originales
Menores víctimas de violencia de género: ¿se les atiende adecuadamente en el ámbito sanitario?
Ana Belén Arredondo Provechoa, Rafael Jiménez Alésb, M.ª Llanos de la Torre Quiraltec, Raquel Páez Gonzálezd, M.ª Luisa Poch Olivée, Antonio Gancedo Barandaf
aEnfermera. Servicio de Calidad, Formación e Investigación. Complejo Asistencial Hospitalario de León. Profesora asociada. Universidad de León. León. España.
bPediatra. CS La Roda de Andalucía. Sevilla. España.
cPediatra. CS Labradores. Logroño. La Rioja. España.
dPediatra. CS 5B. Albacete. España.
eNeuropediatra. Servicio de Pediatría. Hospital San Pedro. Logroño. La Rioja. España.
fPediatría Social. Unidad de Pediatría. Hospital Universitario Fundación Alcorcón. Alcorcón. Madrid. España.
Correspondencia: AB Arredondo. Correo electrónico: abarredondo@saludcastillayleon.es
Cómo citar este artículo: Arredondo Provecho AB, Jiménez Alés R, de la Torre Quiralte MLL, Páez González R, Poch Olivé ML, Gancedo Baranda A. Menores víctimas de violencia de género: ¿se les atiende adecuadamente en el ámbito sanitario? . Rev Pediatr Aten Primaria. 2023;25:31-40.
Publicado en Internet: 24-03-2023 - Número de visitas: 11352
Resumen
Introducción y objetivos: el objetivo fue conocer la opinión de los/as pediatras que atienden a personas menores de edad, que son hijos/as de mujeres víctimas de violencia de género (VG), sobre la formación que reciben y las herramientas con las que cuentan para su abordaje, incluyendo la propia formación y el grado de implicación que asumen en esas situaciones.
Material y métodos: se realizó un estudio descriptivo transversal mediante una encuesta validada utilizando Formularios de Google. Se difundió entre sanitarios/as que trabajan con personas menores de edad a través de sociedades científicas, a las que se solicitó colaboración, y de la lista de distribución PEDIAP de RedIris que agrupa a los profesionales mencionados.
Resultados: respondieron a la encuesta un total de 407 profesionales. Los profesionales contemplaron la VG entre los problemas sociales de los niños, niñas y adolescentes (NNA) que acuden a sus consultas como poco frecuente: el 71% de las respuestas (el 5,6% lo consideraban frecuente). Respecto a la formación, solo el 19% de los profesionales sanitarios consultados consideran que se les ofrece suficiente formación, y solo el 15% piensan que poseen los conocimientos adecuados en esta materia.
Conclusiones: aunque la VG es un problema que debe ser atendido por los profesionales sanitarios, la formación adaptada a ese ámbito, en cuanto a herramientas de detección y de intervención, sigue siendo escasa, lo que puede influir en la infradetección o en un abordaje inadecuado de la misma, así como en una afectación de la salud de los/as hijos/as de las mujeres víctimas de VG.
Palabras clave
● Abuso infantil ● Formación ● Pediatría ● Violencia ● Violencia de género ● Violencia de pareja hacia la mujerINTRODUCCIÓN
La salud pública en su máxima expresión es el esfuerzo colectivo de la sociedad para crear condiciones en las que todas las personas puedan sentirse bien. La violencia, en cualquiera de sus formas, inhibe las condiciones necesarias para vivir bien. Destruye a los individuos, familias y comunidades1.
La violencia de género (VG) está presente en todos los países del mundo y se presenta indistintamente en todas las culturas, clases sociales, edades, niveles de educación, categorías económicas y grupos étnicos. La Ley Orgánica 1/2004 en su artículo 1.1 la define como “manifestación de la discriminación, la situación de desigualdad y las relaciones de poder de los hombres sobre las mujeres, se ejerce sobre estas por parte de quienes sean o hayan sido sus cónyuges o de quienes estén o hayan estado ligados a ellas por relaciones similares de afectividad, aun sin convivencia”, y “comprende todo acto de violencia física y psicológica, incluidas las agresiones a la libertad sexual, las amenazas, las coacciones o la privación arbitraria de libertad”. Ninguna sociedad puede jactarse de estar libre de ella. Las dimensiones globales del fenómeno son alarmantes2. Representa una de las violaciones de los derechos humanos más extendida, que niega a mujeres y niñas la igualdad, seguridad, dignidad, autoestima y el derecho a gozar de las libertades fundamentales. Además, supone un obstáculo para lograr los objetivos de igualdad, desarrollo y paz que marca la Declaración Universal de los Derechos Humanos3, anula la autonomía de la mujer y mina su potencial como persona y miembro de la sociedad4.
Los/as niños/as y adolescentes (NNA), hijos/as de mujeres víctimas de VG, son también víctimas tanto en lo que afecta a su salud, como en la vulneración de sus derechos5,6. Así, en la Convención sobre los Derechos del Niño, en su artículo 19 se indica: “Los Estados Partes adoptarán todas las medidas legislativas, administrativas, sociales y educativas apropiadas para proteger a los menores contra toda forma de perjuicio o abuso físico o mental, descuido o trato negligente, malos tratos o explotación, incluido el abuso sexual, mientras: se encuentren bajo la custodia de los padres, de un representante legal o cualquier otra persona que lo tenga a su cargo”7. Los niños y niñas, hijos/as de madres víctimas de violencia de género, pueden sufrir cualquiera de las tipologías clásicas de maltrato infantil, llegando incluso a morir a manos de los agresores de sus madres.
La presencia de violencia en la unidad familiar incrementa el riesgo de maltrato hacia los menores porque se establece una cultura de violencia en el hogar. Actualmente, se sigue sin considerar que los/as niños/as que viven en ambientes de VG son víctimas directas de esta. Pero son víctimas de maltrato por el hecho de vivir en un ambiente violento.
Las estadísticas8 muestran que del 26 al 73% de las familias en las que se han producido abusos a menores también había VG. Los menores pueden estar expuestos a la violencia en distintas situaciones9: (a) siendo testigos de ella; (b) escuchando cómo se produce sin verla; (c) observando la situación tras la violencia: moratones en la madre, muebles rotos, entre otros; (d) siendo conscientes de que se produce violencia, porque alguien se lo dice; y (e) viviendo donde se produce la violencia sin ser conscientes de que ocurre. No importa de qué modo se exponga a los menores a esta violencia, esta tiene muchísimo impacto en ellos y en algunos se equipara a los que sufren síndromes postraumáticos como consecuencia del abuso sexual, porque, además, del 30 al 60% de los hombres que abusan de sus parejas también abusan de sus hijos/as8.
Hay evidencia empírica que demuestra que crecer en un hogar en el que se cometen abusos puede poner en peligro el proceso de desarrollo de los NNA y sus capacidades tal como demuestran las Experiencias Adversas en la Infancia10. También sufren lesiones físicas, alteraciones del sueño y mayor propensión a padecer enfermedades psicosomáticas. Se presenta con distintas manifestaciones, como pueden ser el retraso en el crecimiento, en el proceso de adquisición del lenguaje y en la disminución de las habilidades motoras11,12. Desde el punto de vista psicológico, las consecuencias negativas incluyen problemas relacionados con la imagen del cuerpo, aparición de síntomas de depresión y ansiedad, intentos suicidas, mediocre funcionamiento psicosocial y deterioro de la autoestima y del bienestar psicológico. El abuso de sustancias estupefacientes, el riesgo de suicidio y los trastornos de la alimentación representan también otras condiciones mentales que pueden padecer los adolescentes. En resumen, una serie de experiencias adversas en su infancia que les desencadenará mayor morbi-mortalidad13.
Sería fundamental abordar esta problemática desde un modelo biopsicosocial que fomente entornos seguros, estables y enriquecedores en los que puedan crecer de forma saludable14.
En este trabajo se realizó, mediante una encuesta dirigida a los profesionales médicos que trabajan con NNA, la frecuencia con la que atienden a menores con VG, la formación que reciben y hasta qué punto se sienten preparados para abordar este problema de salud pública. También se han explorado algunas competencias relacionadas con la cumplimentación de la historia clínica y se ha intentado cuantificar el impacto de la pandemia por COVID-19 en los programas de concienciación y prevención, complementándose con una revisión narrativa de la literatura para analizar el efecto que tiene este tipo de violencia en los NNA y la importancia de los/as pediatras en casos en los que se producen abusos y maltrato en la unidad familiar.
La formación de los profesionales es clave para abordar estas situaciones tan complejas. Por ello, planteamos como objetivos conocer si los/as pediatras contemplan la VG entre los problemas sociales que detectan en los menores que atienden, su implicación y la formación ofertada que permita un mejor conocimiento de esta problemática.
MATERIAL Y MÉTODOS
Se realizó una revisión bibliográfica minuciosa de la bibliografía científica y en las bases de datos disponibles para conocer el panorama actual y la evolución de la violencia de género en los menores. Se revisaron PubMed-Medline, EMBASE, Cochrane Library plus, WOS y PsycBITE. Además de bases de datos nacionales como IME, Dialnet, IBECS, MEDES y Teseo. Se contemplaron los datos e informes del Ministerio de Sanidad y del Gobierno de España.
Se diseñó un estudio descriptivo transversal, realizado a través de una encuesta que fue validada por el propio grupo de investigación14. Se creó en Formularios de Google y se distribuyó con la colaboración de algunas sociedades científicas como AEPap, AEP y SEPS, que agrupan a los profesionales que atienden habitualmente a menores, desde diferentes grupos de trabajo, mediante un enlace que garantiza el anonimato y la voluntariedad. También se realizó una distribución a través de la lista de distribución PEDIAP14.
La encuesta se dirigió a profesionales médicos que trabajan con menores, particularmente a especialistas en Pediatría, en Medicina de Familia y Comunitaria, residentes de ambas especialidades y a otros profesionales que trabajan en Atención Primaria (AP) y hospitalaria, tanto en el ámbito público como privado en España. No se calculó el tamaño muestral y se intentó llegar al máximo número de profesionales. Se realizó durante los meses de junio y julio del año 2021.
La encuesta recoge datos sociodemográficos, aspectos sobre frecuencia de detección, formación, grado de conocimiento y de implicación de los profesionales a quienes se dirige la encuesta respecto a la VG, considerada como problema social que afecta a los menores en cuyos hogares ocurre (experiencia adversa en la infancia). Se puede ver la encuesta en la Figura 1.
| Figura 1. Encuesta dirigida a profesionales médicos que trabajan con menores | |
|---|---|
Sexo:
|
|
| Edad: (en años) | |
Titulación:
|
|
Puesto de trabajo (opción múltiple):
|
|
| Código postal de su centro de trabajo principal: | |
¿Con qué frecuencia atiendes en tu ámbito de trabajo a niños y jóvenes con problemas relacionados con violencia de género?:
|
|
Valora la formación que se te ha ofertado en los 3 últimos años sobre violencia de género:
|
|
¿Cómo consideras tus conocimientos en el abordaje de los problemas y necesidades sociales de los pacientes que atiendes referidos a la violencia de género en su hogar?:
|
|
| ¿Preguntas y anotas en la historia clínica sobre…?: | |
|
|
¿En qué medida estás de acuerdo con la siguiente afirmación relacionada con la influencia que ha tenido la pandemia de COVID-19 en los programas de prevención y concienciación sobre la violencia de género?:
|
|
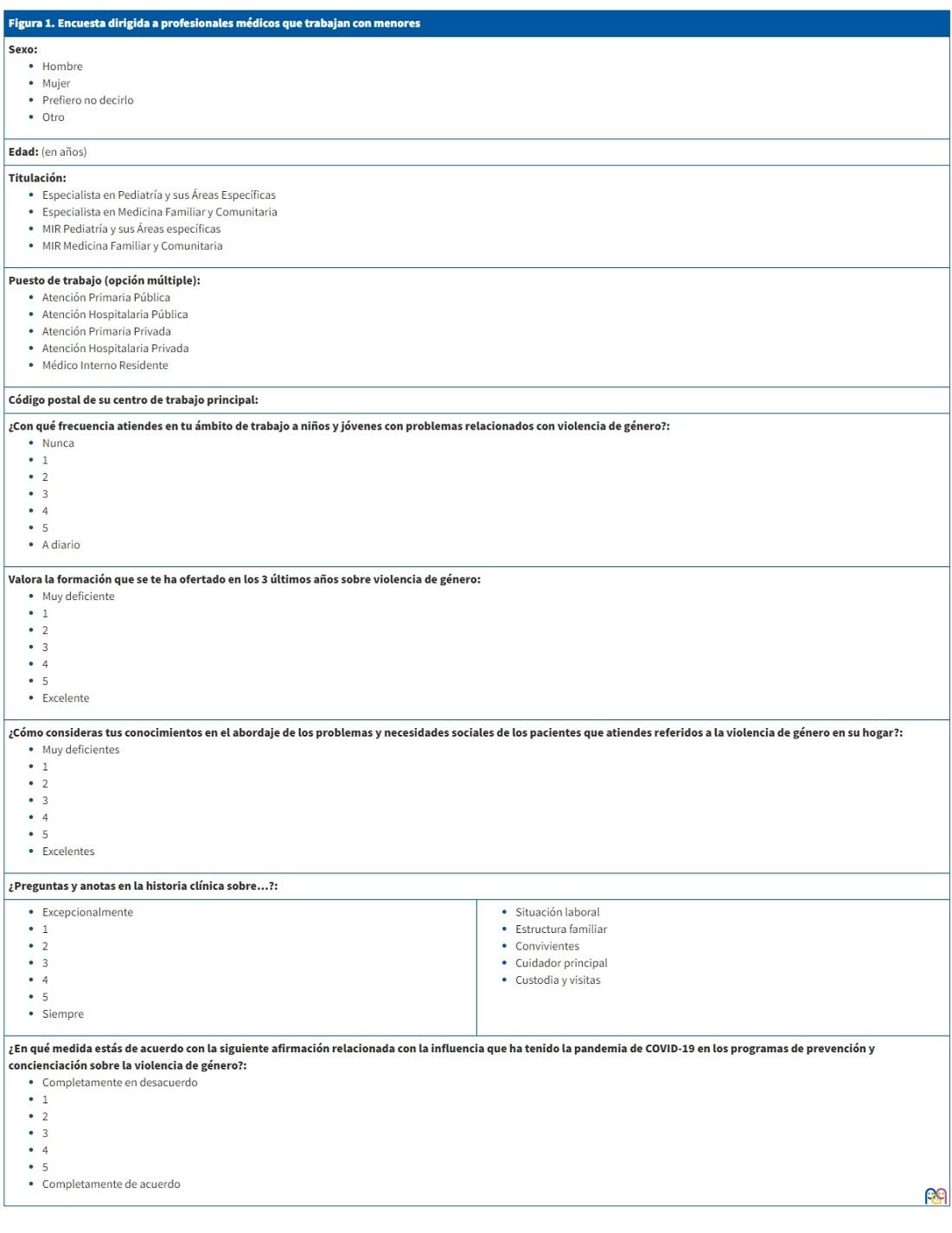
Los datos se recogieron en un formulario diseñado ad hoc y según se respondía la encuesta se registraban directamente en una tabla Excel, pudiendo conocer la evolución de las respuestas en tiempo real. Se enviaron recordatorios con el fin de obtener un mayor grado de participación.
Referido a ellas, se ofrecían las respuestas en formato cuantitativo en escala Likert. Respecto a las frecuencias: Nunca = 1; A diario = 5. Y respecto a la formación o conocimientos: Muy deficiente = 1; Excelente = 5.
Se añadieron y analizaron varias preguntas para conocer la implicación de los profesionales en este tema.
RESULTADOS
Respondieron a la encuesta un total de 407 profesionales. La media de edad fue de 47 años, siendo los mayores de 50 años el 49% (menores de 40 años, el 31%). El 82,31% (335) fueron mujeres. Los profesionales que más respondieron fueron los especialistas en Pediatría, el 91% (370), seguidos de los residentes de Pediatría, el 5,9% (24), los especialistas en Medicina Familiar y Comunitaria, el 2,7% (11), y los residentes de Medicina de Familia, el 0,5% (2). El 66% con dedicación exclusiva a AP. Y el 20% exclusivamente en hospital. El 14% restante combina ambas labores. Por comunidades autónomas (CC. AA.), Madrid fue la más representada (24% de las respuestas), seguida de Andalucía (17%) y Cataluña (9%). Galicia, Aragón, Islas Baleares y País Vasco representan del 5 al 7%. Trabajan en un entorno urbano un 86,5% y en un entorno rural un 13,5% (Tabla 1).
| Tabla 1. Violencia de género como problema social | ||||||
|---|---|---|---|---|---|---|
| Violencia de género | ||||||
| Frecuencia (respuestas) | Formación (respuestas) | Conocimientos (respuestas) | ||||
| 1-2 | 4-5 | 1-2 | 4-5 | 1-2 | 4-5 | |
| Total (407) | 71% | 6% | 58% | 19% | 58% | 14% |
| Hombres (70) | 71% | 4% | 57% | 19% | 51% | 14% |
| Mujeres (335) | 71% | 6% | 59% | 19% | 59% | 13% |
| Hospital (83) | 66% | 6% | 60% | 20% | 60% | 18% |
| Atención Primaria (275) | 74% | 5% | 55% | 21% | 56% | 14% |
| Edad <40 años (125) | 70% | 10% | 73% | 14% | 68% | 10% |
| Edad ≥50 años (200) | 74% | 4% | 56% | 21% | 53% | 16% |
| Medio rural (51) | 73% | 6% | 59% | 14% | 53% | 18% |
| Medio urbano (353) | 71% | 6% | 58% | 20% | 58% | 13% |
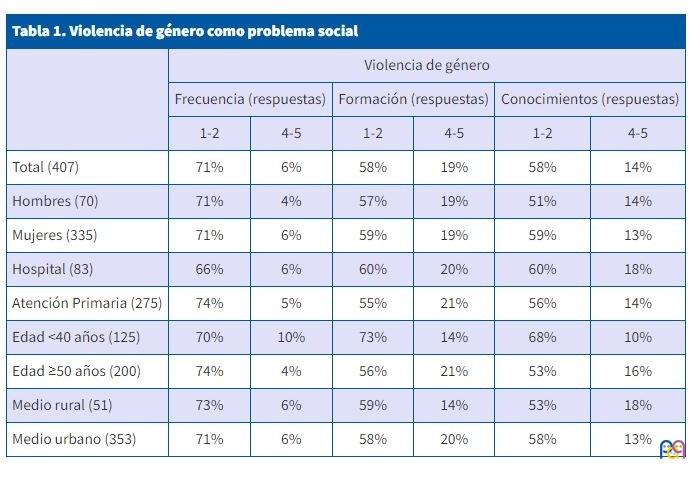
Los profesionales que respondieron contemplaron la VG entre los problemas sociales de los NNA que acuden a sus consultas como un problema poco frecuente: 71% de las respuestas (frente al 5,6% que lo consideraban frecuente). El grupo que lo detecta en mayor proporción son los “jóvenes” (<40 años), que responden como frecuente o muy frecuente en un 10%, en contraste con el resto de los grupos, que ofrecen porcentajes del 5% en ese dato. Los “mayores” (≥50 años) y los profesionales de AP refieren una menor detección (el 74% lo indica como un problema poco frecuente en su labor diaria). Sin embargo, en esos mismos grupos, se aprecian datos contrarios en cuanto a formación y conocimiento: los jóvenes refieren que se les ofrece menos formación y creen poseer menos conocimientos sobre VG respecto a sus colegas de más edad. Aunque, en general, en todos los grupos tanto la formación ofertada como los conocimientos reflejan porcentajes bajos.
Sobre los lugares de trabajo, rural (51) y urbano (353), se puede observar en la Tabla 1 que hay una frecuencia de detección similar en ambos grupos. Refieren mayor formación los profesionales que trabajan en el ámbito urbano; sin embargo, se muestran mayores conocimientos entre los que lo hacen en el ámbito rural. No se aprecian diferencias estadísticamente significativas entre hombres y mujeres respecto a las respuestas aportadas.
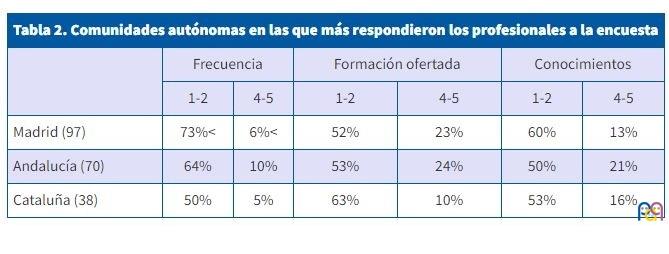
El análisis de las respuestas de las tres CC. AA. más representadas en este estudio nos muestra escasas diferencias en cuanto a frecuencia de detección, formación ofertada y conocimientos sobre el tema (Tabla 2). Andalucía presenta unos resultados mejores, en general, que Madrid y Cataluña.
| Tabla 2. Comunidades autónomas en las que más respondieron los profesionales a la encuesta | ||||||
|---|---|---|---|---|---|---|
| Frecuencia | Formación ofertada | Conocimientos | ||||
| 1-2 | 4-5 | 1-2 | 4-5 | 1-2 | 4-5 | |
| Madrid (97) | 73%< | 6%< | 52% | 23% | 60% | 13% |
| Andalucía (70) | 64% | 10% | 53% | 24% | 50% | 21% |
| Cataluña (38) | 50% | 5% | 63% | 10% | 53% | 16% |
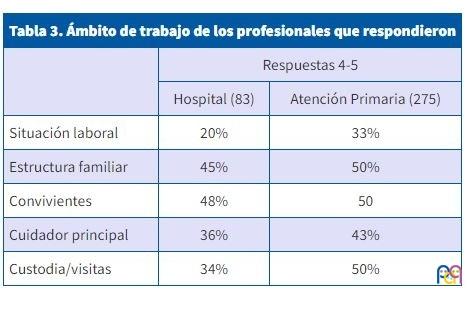
Con el fin de conocer la implicación de los profesionales en el abordaje de la VG como problema que afecta a los NNA que atienden, se indagó también sobre si los profesionales preguntaban y anotaban en las historias de los NNA cuestiones acerca de la situación familiar.
Son preguntas que a menudo nos aproximan a conocer la situación familiar y sus dinámicas, y que sirven con frecuencia para dar pie a que las mujeres nos comenten cómo se sienten en sus hogares.
Según las respuestas, solo la mitad (en el mejor de los casos) de los profesionales que atienden a NNA se interesa en preguntar por estas cuestiones. Se aprecia un mayor interés en el ámbito de la AP que en la atención hospitalaria (Tabla 3).
| Tabla 3. Ámbito de trabajo de los profesionales que respondieron | ||
|---|---|---|
| Respuestas 4-5 | ||
| Hospital (83) | Atención Primaria (275) | |
| Situación laboral | 20% | 33% |
| Estructura familiar | 45% | 50% |
| Convivientes | 48% | 50 |
| Cuidador principal | 36% | 43% |
| Custodia/visitas | 34% | 50% |
Por último, se les preguntó también si consideraban que la pandemia causada por el COVID-19 había afectado a los programas de prevención y concienciación sobre la VG. El 55% de los encuestados respondieron afirmativamente.
DISCUSIÓN
Los servicios sanitarios cuentan con profesionales de diferentes disciplinas (medicina, enfermería, trabajo social, psiquiatría, matronas, fisioterapeutas, terapeutas ocupacionales, etc.) que han de colaborar en el diagnóstico y tratamiento de las diversas problemáticas a las que pretende dar respuesta el sistema sanitario, haciendo posible la intervención desde un modelo de atención integral a la salud15,16. Los profesionales de la salud ocupamos un lugar privilegiado, no solo para detectar los casos y prestar la asistencia sanitaria adecuada a cada situación, sino también para orientarlas y derivarlas a otros recursos que consideren convenientes para su recuperación, y se incluyen también los recursos que se encuentran fuera del sistema sanitario, como programas específicos o puntos municipales de violencia17.
En cuanto a las respuestas de los participantes por grupos, sexo, edad, AP y hospital, podemos comentar los siguientes resultados.
Si nos fijamos en la edad, se aprecian diferencias en los dos grupos. El grupo que lo detecta en mayor proporción son los “jóvenes” (<40 años), que responden como frecuente o muy frecuente en un 10%, en contraste con el resto de los grupos, que ofrecen porcentajes del 5% en ese dato. Los “mayores” (≥50 años) y los profesionales de AP refieren una menor detección (el 74% lo indica como un problema poco frecuente en su labor diaria). Sin embargo, en esos mismos grupos se aprecian los datos contrarios en cuanto a formación y conocimiento: los jóvenes refieren que se les ofrece menos formación y creen poseer menos conocimientos sobre VG respecto a sus colegas de más edad. Aunque, en general, en todos los grupos tanto la formación ofertada como los conocimientos aportan porcentajes bajos.
Aunque en las últimas décadas ha habido más conciencia social entre los jóvenes españoles, podemos observar que en el ámbito sanitario la experiencia juega un papel muy importante y puede ser por esto que los conocimientos y la formación, en general, sean mayores.
Por último, podemos observar que, por lo general, la COVID-19 ha sido y sigue siendo una crisis sanitaria que ha afectado a todos los países en todos los ámbitos, pero sobre todo ha dejado huella en el ámbito sanitario. Por ello, los/as profesionales coinciden en que esta crisis ha afectado al desarrollo de los programas de VG que se habrán pospuesto por la emergencia sanitaria o, incluso, no se habrán llegado a celebrar por la saturación del equipo médico.
Teniendo en cuenta estos datos que explican los conocimientos de mujeres y hombres en el ámbito de la VG, en ningún momento de la encuesta llegan a tener conocimientos superiores al 18%, pero, ¿por qué son tan escasos los conocimientos en esta materia?, ¿hay oferta y poca iniciativa o hay iniciativa, pero poca oferta?
El primer paso consiste en animar a los profesionales a que se apunten a cursos sobre VG, para poder así mejorar la detección y la formación, y poder intervenir en situaciones donde la misma se presenta. Si se enfrentan a casos de abusos o violencias, es fundamental que sepan tomar la decisión más adecuada y crear un entorno lo más tranquilo posible18.
En cuanto a los ámbitos de trabajo y lugar de trabajo que se han estudiado en el presente artículo, se comparan dos áreas (hospital y AP) y dos lugares de trabajo distintos (rural y urbano). Se han establecido los valores 1-2 y 4-5 para indicar respectivamente “poco” y “mucho”.
En primer lugar, en cuanto a la AP (275 participantes) en comparación a la atención en hospitales (83 participantes), los datos son similares. Sin embargo, se aprecia un número mayor en la AP en cuanto a la formación ofertada y asistida; también los profesionales preguntan más a las familias de los menores que atienden sobre su situación laboral y estructura familiar que los que trabajan en hospitales. Aun así, los datos son parecidos. El que haya un número mayor en formación en el ámbito de AP nos hace reflexionar que quizá se oferte más formación en este campo porque son los primeros profesionales que entran en contacto con las víctimas, ya que muchas acuden directamente a urgencias por problemas relacionados con la VG, como traumatismos, heridas u otro tipo de lesiones en general.
En el presente estudio se han comparado también los porcentajes de la frecuencia, formación y conocimientos sobre VG en las áreas de Madrid (97 respuestas), Andalucía (70) y Cataluña (38). Como se observa en la Tabla 2, los resultados de una menor o mayor frecuencia, formación y conocimientos son muy parecidos entre ellos.
Por un lado, se puede destacar que en Andalucía hay un porcentaje más alto en frecuencia y conocimientos con respecto a Madrid y Cataluña. Entre los que han contestado 1-2 (poco) en formación, los resultados fueron muy parecidos (52% en Madrid frente a 53% en Andalucía y 63% en Cataluña).
Por otro lado, entre los que han contestado 4-5 (mucho), se puede destacar que en Andalucía hay una mayor frecuencia y conocimientos con respecto a Madrid y Cataluña (10% en frecuencia frente a 6 y 5%; 21% en conocimientos frente a 13 y 16%). Por lo que atañe la formación, se puede observar que Madrid y Andalucía tienen casi el mismo porcentaje (respectivamente, 23 y 24% frente al 10% de Cataluña).
Estos datos, nos llevan a concluir que es necesario que los servicios sanitarios de todas las CC.AA. oferten una formación completa, accesible y evaluable a todos los profesionales, de manera que los menores sean atendidos en condiciones de equidad. A veces, puede resultar complejo ofrecer formación en entornos rurales, ya que muchos pueblos y aldeas de nuestro país no tienen centros sanitarios cerca y han de desplazarse a las ciudades. Por ello, puede resultar más difícil ofrecer formación, ya que los sanitarios que trabajan en estos entornos son escasos y la formación, por ende, resultaría más costosa. Sin embargo, se observa que tienen mayor nivel de conocimientos (18%) en el entorno rural frente al 13% en el entorno urbano. Por otro lado, es cierto que los conocimientos sobre este tema son más dispares y, por ello, habría que mejorar la formación que se imparte en ambos ámbitos, primaria y especializada, y en ambos entornos, urbano y rural, para así dar una mejor atención a los menores víctimas de VG.
Tras analizar cuidadosamente los resultados obtenidos en el presente estudio en el que se han tenido en cuenta cuestiones sobre la formación de los pediatras en VG, se puede concluir lo siguiente.
En primer lugar, es fundamental una formación previa de los profesionales en todos los pasos del proceso sanitario, donde la formación es esencial para detectar y ofrecer una buena atención sanitaria a las personas menores de edad, hijos/as de mujeres víctimas de VG. Esto concuerda con los datos de otros estudios que concluyen con la afirmación de que, aunque ha aumentado la conciencia social sobre este tema, sigue faltando formación competente y más conciencia en todo el equipo médico. También se enfatiza la carencia de un buen diagnóstico de los casos y su pertinente notificación al resto del equipo o las autoridades, lo que provoca que no haya tratamientos o estudios muy desarrollados18.
Como se ha comentado anteriormente, se propone motivar y concienciar a los profesionales del problema real de la VG, para que asistan a estos cursos y sepan actuar en las situaciones de riesgo que puedan presentarse. Asimismo, si el conocimiento de este tema es mayor, los pediatras que deben tomar decisiones importantes para los pacientes tendrán más formación y más seguridad a la hora de elegir la opción más adecuada para el futuro de la víctima. Si se da más atención en este ámbito, las víctimas pueden ser evaluadas en programas especializados con equipos interdisciplinares en los que participen médicos, psicólogos, trabajadores sociales, centros de protección infantil y un equipo legal. Esto conlleva unos cuidados multidisciplinares para organizar proyectos preventivos y controlar las secuelas psicológicas y físicas. También se pueden desarrollar estrategias que tengan como objetivo garantizar la seguridad de los menores y prevenir las consecuencias potencialmente perjudiciales. Las consultas de Pediatría Social, escasas en todo el territorio nacional, son elementos eficaces que dinamizan la formación, así como la sensibilización de las y los profesionales que valoran la VG como un auténtico problema de salud, y son dispositivos claves en la coordinación, tanto de la AP como hospitalaria.
Es importante que la formación en VG sea generalizada en todas las provincias y ciudades del país, tanto en entornos rurales como urbanos, ya que esto fomentaría un trato igualitario y especializado en las víctimas, estén en el lugar de España que estén, para garantizar que todos los pacientes y sanitarios tengan el mismo acceso a los recursos e información sobre la VG.
En conclusión, con este artículo se han mostrado las carencias en la formación de los profesionales asistenciales en el ámbito de la VG y se han propuesto una serie de medidas para su detección precoz, que es de vital importancia para la salud integral de los niños, niñas y adolescentes hijos/as de mujeres víctimas de violencia de género, así como el respeto a sus derechos. Una de las limitaciones de este estudio fue la baja tasa de respuesta en general y la no participación de otros profesionales implicados en el trato integral de los menores, como, por ejemplo, trabajadores/as sociales, psicólogos/as y profesionales de enfermería.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este trabajo no ha contado con financiación económica, pero fue aceptado como “estudio de interés” en el Pacto de Estado contra la Violencia de Género.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del manuscrito publicado.
ABREVIATURAS
AP: Atención Primaria · CC. AA.: comunidades autónomas · NNA: niños, niñas y adolescentes · VG: violencia de género.
BIBLIOGRAFÍA
- Satcher D. Youth Violence Prevention: Building Local Power and Empowering Youths. Am J Public Health. 2021;111(S1):S.5-5.23.
- La violencia doméstica contra mujeres y niñas. Innocenti Digest. 2000;6. En: Unicef [en línea] [consultado el 09/03/2023]. Disponible en www.unicef-irc.org/publications/266-la-violencia-doméstica-contra-mujeres-y-niñas.html
- Informe de la Cuarta Conferencia Mundial sobre la Mujer: Beijing, 4-15 de septiembre de 1995. Nueva York: Naciones Unidas; 1996. En: Naciones Unidas [en línea] [consultado el 09/03/2023]. Disponible en www.un.org/es/conferences/women/beijing1995
- Organización Panamericana de la Salud. Violencia contra la mujer. Un tema de salud prioritario. Washington: 1998 [en línea] [consultado el 09/03/2023]. Disponible en https://iris.paho.org/handle/10665.2/42651
- Ley Orgánica 1/2004, de 28 de diciembre, de Medidas de Protección Integral contra la Violencia de Género [en línea] [consultado el 09/03/2023]. Disponible en www.boe.es/eli/es/rdl/2018/08/03/9
- Ley Orgánica 8/2015, de 22 de julio, de modificación del sistema de protección a la infancia y a la adolescencia [en línea] [consultado el 09/03/2023]. Disponible en www.boe.es/diario_boe/txt.php?id=BOE-A-2015-8222
- Convención sobre los Derechos del Niño; 2006. En: Unicef [en línea] [consultado el 09/03/2023]. Disponible en www.unicef.es/publicacion/convencion-sobre-los-derechos-del-nino
- Holt S, Buckley H, Whelan S. The Impact of Exposure to Domestic Violence on Children and Young people: a Review of the Literature. Child Abuse & Neglect. 2008;32:797-810.
- Walker Descartes I, Mineo M, Condado LV, Agrawal N. Domestic Violence and Its Effects on Women, Children, and Families. Pediatr Clin North Am. 2021;68:455-64.
- Boullier M, Blair, M. Adverse childhood experiences. Paediatrics and Child Health (United Kingdom). Churchill Livingstone [en línea] [consultado el 09/03/2023]. Disponible en www.paediatricsandchildhealthjournal.co.uk/article/S1751-7222(17)30291-3/fulltext
- Asamblea Mundial de la Salud, 49. (1996). Prevención de la violencia: una prioridad de salud pública. En: OMS [en línea] [consultado el 09/03/2023]. Disponible en https://apps.who.int/iris/handle/10665/203955
- Racionero Plaza S, Tellado I, Aguilera A, Prados M. Gender violence among youth: an effective program of preventive socialization to address a public health problem. AIMS Public Health. 2021;8:66-80.
- López Rodríguez RM, Peláez Moya S. Protocolo común para la actuación sanitaria ante la Violencia de Género. 2012. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2012 [en línea] [consultado el 09/03/2023]. Disponible en www.sanidad.gob.es/organizacion/sns/planCalidadSNS/equidad/saludGenero/vcm/ccicvggt/pcasmgf2012.htm
- Jiménez Alés R, Páez González R, De la Torre Quiralte MLL, Poch Olivé ML, Boukichou Abdelkader N, Andrés Esteban EM. Creación y validación de un instrumento para cuantificar actitudes, conocimientos y dificultades en el abordaje de los problemas sociales. An Pediatr (Barc). 2023, 21/feb. DOI: DOI: 1016/j.anpedi.2022.12.010.
- Foro general sobre Pediatria. En: RedIRIS; 2022 [en línea] [consultado el 09/03/2023]. Disponible en www.rediris.es/list/info/pediap.html
- Polo Usaola C, Romero Claver I, Pires Alcaide M, García Delgado C, Arredondo Provecho A, Muñoz Cano M, et al. Guía de actuación en atención especializada para abordar la violencia de pareja hacia las mujeres. Madrid: Consejería de Sanidad. Dirección General de Coordinación de la Asistencia Sanitaria; 2010 [en línea] [consultado el 09/03/2023]. Disponible en www.madrid.org/bvirtual/BVCM017023.pdf
- Strengthening Health System Responses to Gender based Violence in Eastern Europe and Central Asia: A Resource Package. Estambul; 2014. En: UNFPA Regional Office for Eastern Europe and Central Asia [en línea] [consultado el 09/03/2023]. Disponible en http://eeca.unfpa.org/sites/default/files/pub-pdf/WAVE-UNFPA-Report-EN.pdf
- Carnevale S, Di Napoli I, Esposito C, Arcidiacono C, Procentese F. Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence. Int J Environ Res Public Health. 2020;17:4463.