

Vol. 25 - Num. 97
Original Papers
Minors gender violence victims: are they correctly attended in healthcare settings?
Ana Belén Arredondo Provechoa, Rafael Jiménez Alésb, M.ª Llanos de la Torre Quiraltec, Raquel Páez Gonzálezd, M.ª Luisa Poch Olivée, Antonio Gancedo Barandaf
aEnfermera. Servicio de Calidad, Formación e Investigación. Complejo Asistencial Hospitalario de León. Profesora asociada. Universidad de León. León. España.
bPediatra. CS La Roda de Andalucía. Sevilla. España.
cPediatra. CS Labradores. Logroño. La Rioja. España.
dPediatra. CS 5B. Albacete. España.
eNeuropediatra. Servicio de Pediatría. Hospital San Pedro. Logroño. La Rioja. España.
fPediatría Social. Unidad de Pediatría. Hospital Universitario Fundación Alcorcón. Alcorcón. Madrid. España.
Correspondence: AB Arredondo. E-mail: abarredondo@saludcastillayleon.es
Reference of this article: Arredondo Provecho AB, Jiménez Alés R, de la Torre Quiralte MLL, Páez González R, Poch Olivé ML, Gancedo Baranda A. Minors gender violence victims: are they correctly attended in healthcare settings? . Rev Pediatr Aten Primaria. 2023;25:31-40.
Published in Internet: 24-03-2023 - Visits: 4034
Abstract
Background: the aim was to find out the opinion of paediatricians who care for minors who are victims of gender-based violence, on the training they receive and the tools they have to deal with it, including their own training and the degree of involvement they assume in these situations.
Methods: a descriptive cross-sectional study was carried out through a validated survey using Google Forms. It was disseminated among healthcare professionals working with minors through scientific societies that were asked to collaborate and through the PEDIAP distribution list of RedIris, which groups together the aforementioned professionals.
Results: a total of 407 professionals responded to the survey. Professionals considered GBV among the social problems of minors attending their offices as infrequent: 71% of responses (compared to 5.6% who considered it frequent). Regarding training, only 19% consider that they are offered sufficient training, and only 15% think that they have adequate knowledge in this area.
Conclusions: although GBV is a problem that needs to be addressed by health professionals, training adapted to this field, in terms of detection and intervention tools, remains scarce, which may influence under-detection or an inadequate approach to it, as well as affecting the health of the children of women victims of GBV.
Keywords
● Child abuse ● Formation ● Gender-based violence ● Intimate partner violence against women ● Pediatrics ● ViolenceINTRODUCTION
At its best, public health is the collective effort of society to establish conditions that promote the wellbeing of all individuals. Violence in any form inhibits the necessary conditions to live well. It is destructive to individuals, families and communities.1
Gender-based violence (GBV) exists in every country in the world and is found in all cultures, social classes, ages, levels of educational attainment and income and ethnic groups. In Spain, article 1.1 of Organic Law 1/2004 defines it as an expression of discrimination, the situation of inequality and the power relations prevailing between men and women, exercised against the violence exercised against women by their present or former spouses or by men with whom they maintain or have maintained analogous affective relations, with or without cohabitation, as an expression of discrimination, the situation of inequality and the power relations prevailing between the sexes women, encompassing all acts of physical and psychological violence, including offences against sexual liberty, threats, coercion and the arbitrary deprivation of liberty. No society can boast of being free of it. The global magnitude of this phenomenon is alarming.2 It is one of the most widespread violations of human rights, denying women and girls equality, safety, dignity, self-esteem and the right to enjoy the fundamental liberties. It also poses a barrier to the achievement of the strategic objectives of equality, development and peace established by the Universal Declaration of Human Rights,3 negates the autonomy of women and undermines their potential as individuals and members of society.4 Children and adolescents whose mothers are victims of GBV are also victims in terms of the deleterious impact on their health and the violation of their rights.5,6 Thus, Article 19 of the Convention on the Rights of the Child states that “States Parties shall take all appropriate legislative, administrative, social and educational measures to protect the child from all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse, while in the care of parent(s), legal guardian(s) or any other person who has the care of the child.”7 Children whose mothers are victims of GBV may suffer any of the traditionally recognised types of child abuse and may even die at the hands of the abusers of their mothers.
When there is violence at home, the risk of child abuse increases because a culture of violence takes root in the household. At present, it is still not recognised that children exposed to GBV in their immediate environment are direct victims of it. But they are victims of abuse just by living in a violent environment.
Statistical studies8 show that GBV is present in 26% of 73% of households in which minors are abused. Minors may be exposed to violence in different ways9: (a) witnessing it; (b) hearing acts of violence taking place without seeing them; (c) witnessing the aftermath of the violence, such as bruises in the mother or broken furniture; (d) being aware of the violence because they hear about it from someone else; and (e) living in an environment where violence occurs without being aware of it. Regardless of how minors are exposed to violence, it does have a significant impact on them, which in some cases is as severe as the post-traumatic stress resulting from sexual abuse, for, furthermore, 30 to 60% of men who abuse their partners also abuse their children.8
There is empiric evidence that shows that growing in a household where there is abuse can hinder the development and skills of children and adolescents. They may also suffer physical injury, sleep disturbances and be at higher risk of psychosomatic disorders. It may manifest in different ways, such as delayed growth, delayed language acquisition and motor skill deficits.10,11 From a psychological standpoint, the negative repercussions can include body-image problems, symptoms of depression and anxiety, suicidal behaviour, poor psychosocial functioning, low self-esteem, and decreased psychological wellbeing. Substance use, suicidality and eating disorders are other mental health disorders that adolescents may develop. In short, a series of negative experiences during childhood associated with an increased morbidity and mortality.12
It is essential to address this problem with a biopsychosocial approach through the promotion of safe, stable and enriching environments allowing healthy growth and development.13.
We conducted a study through a survey of medical professionals who work with children and adolescents on the frequency with which they managed minors exposed to GBV, the training they received on the subject and how competent they felt in approaching this public health problem. The survey also explored competencies related to documentation in the health record and the impact of the COVID-19 pandemic on prevention and awareness actions, and was supplemented with a narrative review of the impact of GBV on children and adolescents and the importance of paediatricians in cases in which there is abuse and mistreatment in the family unit.
The training of professionals is key to manage these very complex situations. For this reason, the aim of our study was to determine whether paediatricians consider GBV among the social problems they identify in the minors in their care, their involvement and the training offered and received allowing a better understanding of this problem.
MATERIAL AND METHODS
We conducted a thorough review of the scientific literature in the available databases to understand the current situation and trends in gender-based violence in minors. We searched the PubMed-Medline, EMBASE, Cochrane Library plus, WOS and PsycBITE databases. We also searched Spanish databases such as IME, Dialnet, IBECS, MEDES and Teseo. The review included data and reports from the Ministry of Health and the government of Spain.
We designed a cross-sectional descriptive study by means of a questionnaire previously validated by our research group.13 The questionnaire was created in the Google Forms platform and distributed through a link to the form with the collaboration of several scientific societies such as the Spanish Association of Primary Care Paediatrics (AEPap), Spanish Association of Paediatrics (AEP) and the Spanish Society of Social Paediatrics (SEPS), which gather the providers that usually manage minors in their practices, and through various working groups, ensuring anonymous and voluntary participation. The questionnaire was also distributed through the PEDIAP mailing list of primary care professionals.13
The survey was aimed at medical providers who worked with minors, particularly physicians specialised in paediatrics or family and community medicine, medical residents in either of these specialities and other professionals working in primary care (PC) and hospital settings, in either the public or private health care systems in Spain. We did not make a sample size calculation and instead attempted to reach the largest possible number of professionals. The survey was conducted in June and July 2021.
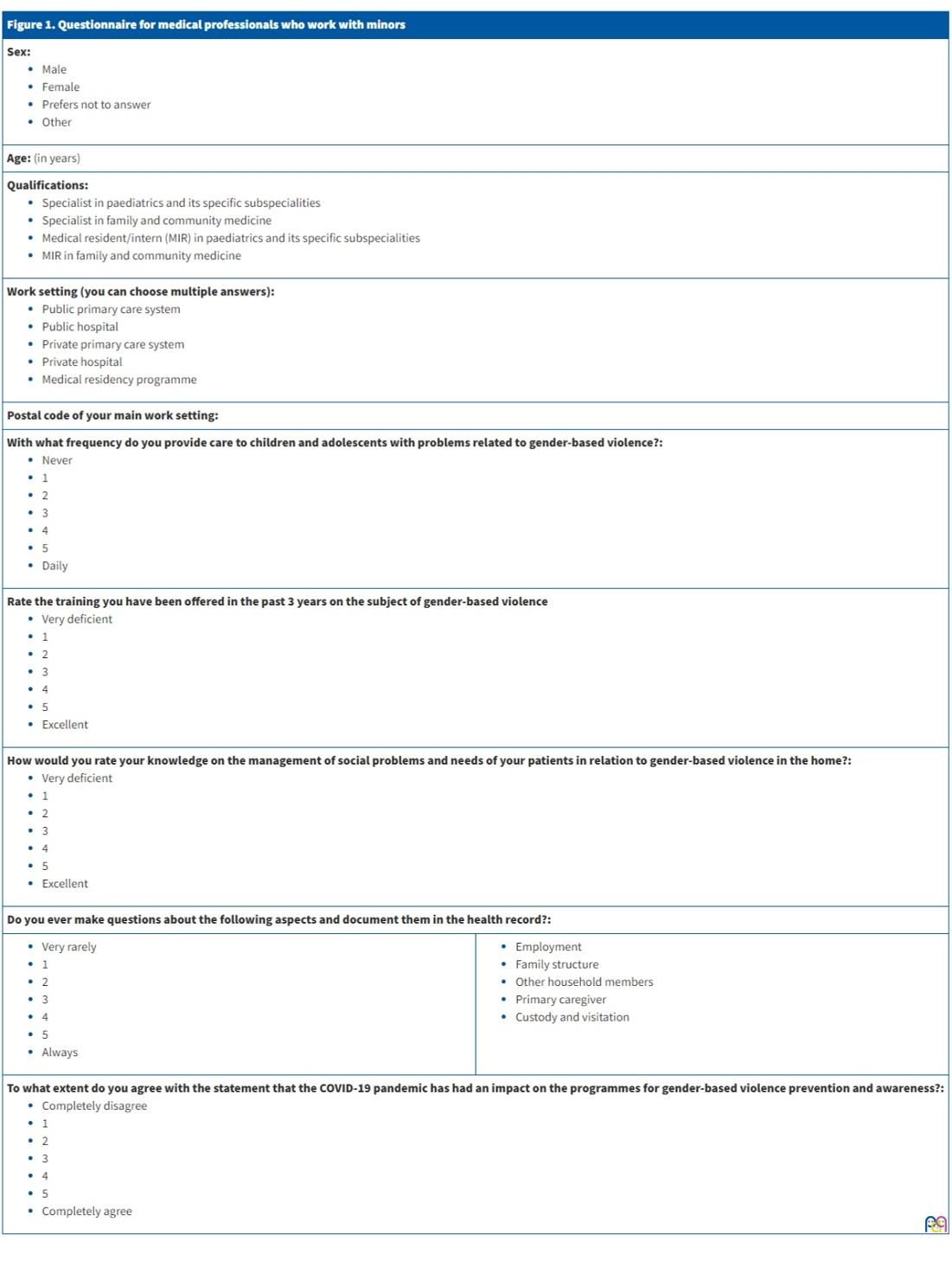
The questionnaire collected data on the sociodemographic characteristics, frequency of detection, training, level of knowledge and involvement of the professionals who participated in the survey in relation to GBV, with the latter understood as a social problem that affects minors exposed to it in the home (negative experience during childhood). The survey can be found in Figure 1.
| Figure 1. Questionnaire for medical professionals who work with minors | |
|---|---|
Sex:
|
|
| Age: (in years) | |
Qualifications:
|
|
Work setting (you can choose multiple answers):
|
|
| Postal code of your main work setting: | |
With what frequency do you provide care to children and adolescents with problems related to gender-based violence?:
|
|
Rate the training you have been offered in the past 3 years on the subject of gender-based violence
|
|
How would you rate your knowledge on the management of social problems and needs of your patients in relation to gender-based violence in the home?:
|
|
| Do you ever make questions about the following aspects and document them in the health record?: | |
|
|
To what extent do you agree with the statement that the COVID-19 pandemic has had an impact on the programmes for gender-based violence prevention and awareness?:
|
|
The data were collected in an ad hoc form and recorded directly in an Excel file as responses to the survey were submitted, which allowed us to monitor the evolution of the responses in real time. We sent out reminders to maximise participation.
The answers were quantitative, rated on a Likert scale. Frequencies were rated on a scale ranging from Never = 1 to Daily = 5. Training or knowledge were rated on a scale ranging from Very deficient = 1 to Excellent = 5.
We added and analysed several items to assess the involvement of respondents in this issue.
RESULTS
A total of 407 professionals participated in the survey. The mean age was 47 years, with 49% of respondents aged more than 50 years (age < 40 years, 31%). Out of the total sample, 82,31% (335) of respondents were female. The professionals that participated most frequently were specialists in paediatrics, amounting to 91% of the total (370), followed by residents in paediatrics, who amounted to 5.9% (24), specialists in family and community medicine, 2.7% (11), and residents in family medicine, 0.5% (2). Sixty-six percent worked exclusively in the PC setting. Twenty percent worked exclusively in the hospital setting. The remaining 14% worked in both settings. By autonomous community (AC) in Spain, we found that Madrid was the most represented region (24% of responses), followed by Andalusia (17%) and Catalonia (9%). The proportions of respondents from Galicia, Aragon, Balearic Islands and the Basque Country ranged from 5 to 7%. Lastly, 86.5% of respondents worked in urban settings and 13.5% in rural settings (Table 1).
| Table 1. Gender-based violence as a social problem | ||||||
|---|---|---|---|---|---|---|
| Gender-based violence | ||||||
| Frequency of detection (answers) | Training (answers) | Knowledge (answers) | ||||
| 1-2 | 4-5 | 1-2 | 4-5 | 1-2 | 4-5 | |
| Total (407) | 71% | 6% | 58% | 19% | 58% | 14% |
| Male (70) | 71% | 4% | 57% | 19% | 51% | 14% |
| Female (335) | 71% | 6% | 59% | 19% | 59% | 13% |
| Hospital (83) | 66% | 6% | 60% | 20% | 60% | 18% |
| Primary care (275) | 74% | 5% | 55% | 21% | 56% | 14% |
| Age <40 years (125) | 70% | 10% | 73% | 14% | 68% | 10% |
| Age ≥50 años (200) | 74% | 4% | 56% | 21% | 53% | 16% |
| Rural setting (51) | 73% | 6% | 59% | 14% | 53% | 18% |
| Urban setting (353) | 71% | 6% | 58% | 20% | 58% | 13% |
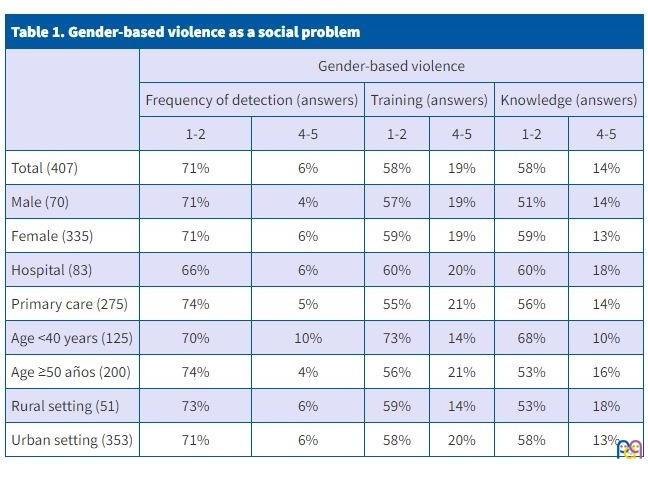
The professionals who responded considered GBV an infrequent social problem among the children and adolescents that they managed: 71% of respondents (compared to 5.6% who considered it a frequent problem). “Young” professionals (age < 40 years) were the group that detected GBV most frequently, with 10% reporting it was a frequent or very frequent problem, compared to all other age groups, in which 5% of professionals reported such frequency. Older clinicians (age ≥50 years) and PC professionals reported a lower frequency of detection (74% rated this issue as an infrequent problem in their daily practice). However, the responses regarding training and knowledge in these same groups appeared to be contradictory: young clinicians reported that they received less training and believed they were less knowledgeable about GBV compared to older colleagues. Although, overall, all groups generally rated the offered training and the level of knowledge as poor.
When it came to the geographical setting, the frequency of detection was similar in both groups, rural (51) and urban (353), as can be seen in Table 1. Professionals in urban settings reported receiving more training, but the perceived knowledge was greater among professionals in rural settings. There were no statistically significant differences between male and female respondents in any of these aspects.
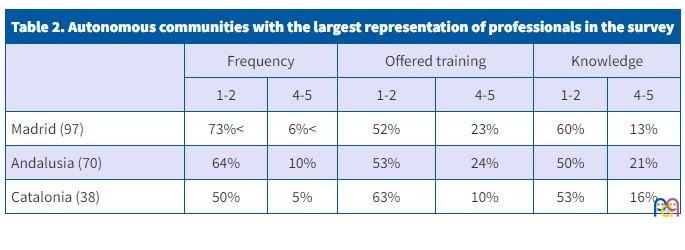
The comparison of the responses obtained from the 3 ACs in Spain most represented in our study evinced little variation in the frequency of detection of GBV and the training and knowledge on the subject (Table 2). The results were generally better in Andalusia compared to Madrid and Catalonia.
| Table 2. Autonomous communities with the largest representation of professionals in the survey | ||||||
|---|---|---|---|---|---|---|
| Frequency | Offered training | Knowledge | ||||
| 1-2 | 4-5 | 1-2 | 4-5 | 1-2 | 4-5 | |
| Madrid (97) | 73%< | 6%< | 52% | 23% | 60% | 13% |
| Andalusia (70) | 64% | 10% | 53% | 24% | 50% | 21% |
| Catalonia (38) | 50% | 5% | 63% | 10% | 53% | 16% |
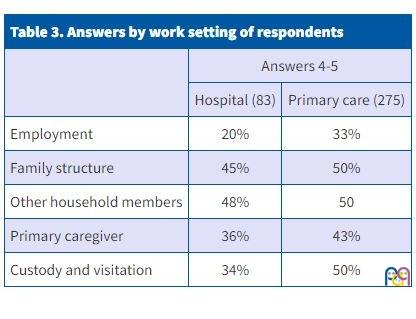
To assess the involvement of professionals in the management of GBV as a problem affecting children and adolescents in their care, we asked whether they assessed and documented in the health record aspects related to the circumstances of the family.
These are aspects that can often help us understand the situation and dynamics of the family and asking about them may encourage women to discuss what they experience at home.
Based on the received responses, in the best-possible scenario, only half of professionals who manage children and adolescents explore these aspects. We found a greater interest in their assessment in professionals in PC versus hospital settings (Table 3).
| Table 3. Answers by work setting of respondents | ||
|---|---|---|
| Answers 4-5 | ||
| Hospital (83) | Primary care (275) | |
| Employment | 20% | 33% |
| Family structure | 45% | 50% |
| Other household members | 48% | 50 |
| Primary caregiver | 36% | 43% |
| Custody and visitation | 34% | 50% |
Last of all, the questionnaire asked respondents whether they believed that the COVID-19 had had a negative impact on GBV prevention and awareness programmes. Fifty-five percent of respondents answered that it had.
DISCUSSION
Health care systems include professionals in different fields (medicine, nursing, social work, psychology, midwifery, physical therapy, occupational therapy, etc.) that need to collaborate in the diagnosis and treatment of the different problems that the system aims to address, enabling the management of these problems through a comprehensive care delivery model.14,15 As health care professionals we are in a privileged position to not only identify patients affected by GBV and deliver the appropriate care for each situation, but also to counsel them and refer them to other services considered appropriate for their recovery, including resources outside the health care system, such as specific programmes or municipal points of care for gender violence.16
The following were relevant results concerning the respondents in terms of groups, sex, age, and clinical setting (PC versus hospital).
Although in recent decades social awareness has been increasing among Spanish youth, in the health care field, experience plays an important role, and this may explain why training and experience are greater in older clinicians
Last of all, generally, the COVID-19 pandemic has been and continues to be a public health crisis that has affected every country in every field, but has had a particularly strong impact on the health care field. In consequence, respondents agreed that this crisis affected the development of GBV programmes, which had been postponed or even eliminated in the wake of the pandemic because health care teams were overwhelmed.
Considering the data concerning the knowledge of female and male practitioners on the subject of GBV, we see that good knowledge was not reported by more than 18% of professionals in any category of the survey, but why is knowledge on this subject so scarce? Is training available but motivation lacking, or is there motivation but scarce access to training?
The first step to remedy it would be to encourage professionals to take courses on GBV to improve their knowledge and the detection of GBV and be able to intervene once it is identified. If professionals face cases of abuse or violence, it is essential that they be able to make the best possible decisions and create a safe and supportive environment.17
The language and attitude of the paediatrician must be empathic, respectful and supportive of the child or adolescent. Paediatricians should explain to minors that their job is to safeguard their health and that their office is the place in which to discuss their difficulties. They also need to know how to make open-ended questions, avoid ambiguity and actively listen to minors and mothers. Training is also important.17
As regards the clinical and geographical settings where respondents carried out their practice, our survey compared two clinical settings (PC versus hospital) and two geographical settings (rural and urban). We established ratings of 1-2 to indicate low levels and 4-5 to indicate high levels.
Firstly, responses were similar in the PC setting (275 respondents) compared to the hospital setting (83 respondents). However, primary care providers reported a greater availability and participation in trainings and were more likely to ask families of minors in their care about their employment status and family structure compared to hospitalists. Even so, the figures were similar. A possible explanation to the fact that training was more frequent in the PC setting is that training may be offered most frequently in this field because PC providers are the first contact of victims with the health care system, of who many go directly to the emergency department for problems related to GBV, such as traumatic injuries, wounds and other lesions.
In this study, we also compared the percentages concerning the frequency of detection, training and level of knowledge on GBV in the regions of Madrid (97 responses), Andalusia (70) and Catalonia (38). As can be seen in Table 2, the results for each region were very similar in all of these aspects.
On one hand, there was a higher frequency of training and high levels of knowledge in Andalusia compared to Madrid and Catalonia. As regards the proportion of respondents who rated the offered training as 1-2 (low), the results were very similar (52% in Madrid versus 53% in Andalusia and 63% in Catalonia).
On the other hand, when it came to ratings of 4-5 points (high) for training and knowledge, we ought to highlight that the frequency was higher in Andalusia compared to Madrid and Catalonia (10% compared to 6 and 5% for training; 21% compared to 13 and 16% for knowledge). The percentage of respondents that rated training highly was nearly the same in Madrid and Andalusia (23 and 24%, respectively, versus 10% in Catalonia).
Our findings call for reflection and for advocating for universal training in every region of Spain to guarantee that minors get equitable care regardless of location and that professionals can have access to all the trainings they require. In some stances offering training in rural settings may be complicated, as many villages and towns in Spain do not have any health care facilities within a close distance and it may require travel to larger cities. Therefore, it may be difficult to offer training to rural clinicians, as there are few of them and their training would be more costly. Yet, a higher proportion (18%) of respondents from rural settings reported a high level of knowledge compared to respondents from urban settings (13%). On the other hand, there are disparities in the knowledge on this subject and therefore the training offered in both care settings (primary care and hospital-based speciality care) and both geographical settings (urban and rural) must be improved to also improve the care of minors who are victims of GBV.
After a careful analysis of the results obtained in the survey concerning the training of paediatricians on GBV, we concluded the following.
First, previous education of all health professionals involved in each of the steps of the health care process is essential in order to detect and offer appropriate care to minors who are children of women victims of GBV. This is consistent with the findings of past studies that have concluded that while social awareness of the issue has increased, there is still a lack of adequate training and awareness in the entire health care team should improve. Emphasis has also been placed on the deficient detection of cases and the pertinent reporting to the rest of the team or the authorities, due to which there are no properly developed management protocols or studies.17
As we already noted, we believe that health care professionals should be made aware of the actual problem that is GBV and encouraged to attend these trainings so they know how to act in any risk situations that may present to them. Furthermore, if their knowledge on the subject improves, the paediatricians who make decisions important for the patients will be prepared and more certain in choosing the most suitable option for the future of the victim. If more resources were devoted to the management of GBV, victims could be assessed in the framework of specialised programmes with multidisciplinary care teams including physicians, psychologists, social workers and child protection and legal services. This entails a multidisciplinary approach to care delivery with organization of preventive interventions and management of psychological and physical sequelae. Strategies can also be developed toward guaranteeing the safety of minors and prevent potentially deleterious repercussions. Social paediatrics services, which are scarce throughout Spain, could be drivers of training and contribute to raising the awareness of professionals of GBV as an actual health problem, while becoming key resources for coordination at both the PC and hospital levels.
It is important that training on GBV be offered universally, in every province and city in Spain, in rural as well as urban settings, as this would promote equitable and specialised care for victims of violence, wherever they are in the Spanish territory, in order to guarantee equal access to resources and information on GBV to all patients and clinicians.
In conclusion, this article evinces the gaps in the training of health care professionals on the subject of GBV and proposes a series of measures for its early detection, which is crucial to the health and overall wellbeing of the children and adolescents whose mothers are victims of gender-based violence, and for safeguarding their rights. One of the limitations of the study was the low response rate and the lack of participation or very limited participation of professionals involved in the comprehensive care of minors, such as social workers, psychologists and nurses.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. The study did not receive any form of funding, but was accepted as a “study of interest” in the State Pact on Gender Violence.
AUTHOR CONTRIBUTIONS
All authors contributed equally to the writing of the manuscript.
ABBREVIATIONS
AC: autonomous community · GBV: gender-based violence · PC: primary care.
REFERENCES
- Satcher D. Youth Violence Prevention: Building Local Power and Empowering Youths. Am J Public Health. 2021;111(S1):S.5-5.23.
- La violencia doméstica contra mujeres y niñas. Innocenti Digest. 2000;6. In: Unicef [online] [accessed 09/03/2023]. Available at www.unicef-irc.org/publications/266-la-violencia-dom%C3%A9stica-contra-mujeres-y-ni%C3%B1as.html
- Report of the Fourth World Conference on Women: Beijing, 4-15 September, 1995. New York: United Nations; 1996. In: Naciones Unidas [online] [accessed 09/03/2023]. Available at www.un.org/en/conferences/women/beijing1995
- Organización Panamericana de la Salud. Violencia contra la mujer. Un tema de salud prioritario. Washington: 1998 [online] [accessed 09/03/2023]. Available at https://iris.paho.org/handle/10665.2/42651
- Ley Orgánica 1/2004, de 28 de diciembre, de Medidas de Protección Integral contra la Violencia de Género [online] [accessed 09/03/2023]. Available at www.boe.es/eli/es/rdl/2018/08/03/9
- Ley Orgánica 8/2015, de 22 de julio, de modificación del sistema de protección a la infancia y a la adolescencia [online] [accessed 09/03/2023]. Available at www.boe.es/diario_boe/txt.php?id=BOE-A-2015-8222
- Convención sobre los Derechos del Niño; 2006. In: Unicef [online] [accessed 09/03/2023]. Available at www.unicef.es/publicacion/convencion-sobre-los-derechos-del-nino
- Holt S, Buckley H, Whelan S. The Impact of Exposure to Domestic Violence on Children and Young people: a Review of the Literature. Child Abuse & Neglect. 2008;32:797-810.
- Walker Descartes I, Mineo M, Condado LV, Agrawal N. Domestic Violence and Its Effects on Women, Children, and Families. Pediatr Clin North Am. 2021;68:455-64.
- World Health Assembly, 49. (1996). Prevention of violence: public health priority.. In: World Health Organization [online] [accessed 09/03/2023]. Available at https://apps.who.int/iris/handle/10665/179463
- Racionero Plaza S, Tellado I, Aguilera A, Prados M. Gender violence among youth: an effective program of preventive socialization to address a public health problem. AIMS Public Health. 2021;8:66-80.
- López Rodríguez RM, Peláez Moya S. Protocolo común para la actuación sanitaria ante la Violencia de Género. 2012. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2012 [online] [accessed 09/03/2023]. Available at www.sanidad.gob.es/organizacion/sns/planCalidadSNS/equidad/saludGenero/vcm/ccicvggt/pcasmgf2012.htm
- Jiménez Alés R, Páez González R, De la Torre Quiralte MLL, Poch Olivé ML, Boukichou Abdelkader N, Andrés Esteban EM. Creación y validación de un instrumento para cuantificar actitudes, conocimientos y dificultades en el abordaje de los problemas sociales. An Pediatr (Barc). 2023, 21/feb. DOI: DOI: 1016/j.anpedi.2022.12.010.
- Foro general sobre Pediatria. In: RedIRIS; 2022 [online] [accessed 09/03/2023]. Available at www.rediris.es/list/info/pediap.html
- Polo Usaola C, Romero Claver I, Pires Alcaide M, García Delgado C, Arredondo Provecho A, Muñoz Cano M, et al. Guía de actuación en atención especializada para abordar la violencia de pareja hacia las mujeres. Madrid: Consejería de Sanidad. Dirección General de Coordinación de la Asistencia Sanitaria; 2010 [online] [accessed 09/03/2023]. Available at www.madrid.org/bvirtual/BVCM017023.pdf
- Strengthening Health System Responses to Gender based Violence in Eastern Europe and Central Asia: A Resource Package. Istanbul; 2014. In: UNFPA Regional Office for Eastern Europe and Central Asia [online] [accessed 09/03/2023]. Available at http://eeca.unfpa.org/sites/default/files/pub-pdf/WAVE-UNFPA-Report-EN.pdf
- Carnevale S, Di Napoli I, Esposito C, Arcidiacono C, Procentese F. Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence. Int J Environ Res Public Health. 2020;17:4463.
Comments
This article has no comments yet.