
Vol. 26 - Num. 101
Originales
Adecuación de las prescripciones médicas en faringitis estreptocócicas y otitis media aguda a las guías terapéuticas
Marcelo Vivas Morescoa, Beatriz Barbarin Sorozabalb, Silvia García de Garayo Díazc, José Tomás Ramos Amadord
aPediatra. CS de Salvatierra. Álava. España.
bPediatra. CS de San Adrián. Navarra. España.
cMatemática. OSI Álava de Osakidetza. Álava. España.
dServicio de Pediatría. Hospital Clínico San Carlos. Madrid. Instituto de Investigación Sanitaria Hospital Clínico San Carlos (IdISSC). Universidad Complutense. Madrid. España.
Correspondencia: M Vivas. Correo electrónico: marcevivas@gmail.com
Cómo citar este artículo: Vivas Moresco M, Barbarin Sorozabal B, García de Garayo Díaz S, Ramos Amador JT. Adecuación de las prescripciones médicas en faringitis estreptocócicas y otitis media aguda a las guías terapéuticas . Rev Pediatr Aten Primaria. 2024;26:35-43. https://doi.org/10.60147/c4a39d2d
Publicado en Internet: 05-02-2024 - Número de visitas: 15311
Resumen
Fundamento y objetivo: analizar el grado de adecuación a las guías terapéuticas de consenso de las prescripciones por parte de los pediatras de Atención Primaria (AP) en casos de faringoamigdalitis aguda (FAA) y otitis media aguda (OMA).
Material y métodos: estudio observacional retrospectivo con obtención de datos de los registros electrónicos de las historias clínicas de los pacientes con OMA supurada y FAA estreptocócica en pacientes de 0 a 14 años que residen en Álava (País Vasco, España), en 18 meses de estudio.
Resultados: en el grupo de pacientes con OMA supurada han sido evaluados 238 episodios obteniendo un grado de adecuación terapéutica del 56,7% y siendo la infradosificación la principal causa de inadecuación. En el grupo de pacientes con FAA estreptocócica han sido evaluados 1721 episodios obteniendo un grado de adecuación terapéutica del 57%, siendo las principales causas de inadecuación la sobredosificación y las pautas de corta duración.
Conclusiones: tanto en OMA supurada como en FAA estreptocócica el grado de adecuación terapéutica es algo más bajo comparado con otros estudios analizados. Ambos procesos infecciosos son de frecuentes diagnóstico y tratamiento en AP, razón por la cual es de vital importancia la mejora en su adecuado tratamiento. Otro punto de mejora es el correcto registro en la historia clínica de los pacientes.
Palabras clave
● Faringitis aguda ● Otitis media aguda ● TratamientoINTRODUCCIÓN
Dos procesos infecciosos frecuentemente diagnosticados y tratados en la consulta médica diaria de Pediatría de Atención Primaria (AP) son la otitis media aguda (OMA) y la faringitis o faringoamigdalitis aguda (FAA). Por ello es de suma importancia la correcta implementación de las guías terapéuticas para dichos procesos, para así prescribir antibióticos en los casos en que realmente estén justificados, ajustándolos a las dosis y días de duración recomendados. En el siguiente estudio se busca analizar el grado de adecuación a las guías terapéuticas de la FAA y la OMA por parte de los pediatras de AP, ya que en la práctica diaria se tiene la percepción general de que los errores en la prescripción antibiótica ocurren con relativa frecuencia. Para ello, se evaluó de manera retrospectiva durante 18 meses el grado de adecuación terapéutica en FAA estreptocócica y en OMA supurada en Pediatría de AP en la región de Álava (País Vasco, España), tomando como referencia las guías publicadas para dichas patologías por la Asociación Española de Pediatría (AEP).
MATERIAL Y MÉTODOS
Se diseñó un estudio observacional retrospectivo con obtención de datos de los registros electrónicos de las historias clínicas de los pacientes de forma anónima, con autorización previa, dividiéndolos en dos grupos: un grupo con los pacientes con diagnóstico de FAA estreptocócica y otro con los pacientes con diagnóstico de OMA supurada. Para la selección de los casos se han utilizado los códigos de la Clasificación Internacional de Enfermedades y Problemas Relacionados con la Salud, décima edición (CIE-10). Los códigos utilizados para OMA supurada han sido H66011 (OMA supurativa oído derecho), H66012 (OMA supurativa oído izquierdo), H66013 (OMA supurativa bilateral) y H66019 (OMA supurativa oído no especificado); y los utilizados para FAA estreptocócica han sido J020 (faringitis estreptocócica) y J0300 (amigdalitis aguda estreptocócica). El límite de edad en ambos grupos ha sido de 0 a 14 años. Los pacientes estudiados residen en la región de Álava (País Vasco, España) y han sido diagnosticados por alguno de los dos procesos entre el 1 de septiembre de 2021 y el 1 de marzo de 2023 (18 meses).
En cada uno de los grupos se ha analizado la adecuación a las actuales recomendaciones de tratamiento tomando como referencia para FAA estreptocócica el documento de consenso sobre el diagnóstico y tratamiento de la FAA publicado por la AEP en el año 20111 (y actualizado en el año 20202), y para OMA supurada, el documento de consenso sobre etiología, diagnóstico y tratamiento de la OMA publicado por la AEP en el año 20123.
Las variables analizadas en ambos grupos han sido: edad al diagnóstico ( en caso de varios procesos en el plazo de tiempo estudiado se toma como edad la del primer episodio diagnosticado), sexo, último peso registrado, principio activo del antibiótico, dosis diaria, intervalo de administración, relación de la dosis diaria con último peso registrado del paciente, duración de la prescripción antibiótica, adecuación terapéutica a guías tomadas como referencia de buena práctica clínica, realización o no de test de diagnóstico rápido (TDRA) para estreptococo betahemolítico del grupo A (EbhGA) en el caso de FAA estreptocócica, realización o no de toma de exudado y aislamiento de germen.
Para analizar si la variable edad presentaba o no una distribución normal, se realizó el test de Kolmogorov-Smirnov tanto en el grupo de pacientes con OMA supurada como en el de FAA estreptocócica, obteniendo como resultado que en ambos grupos la edad no seguía una distribución normal.
RESULTADOS
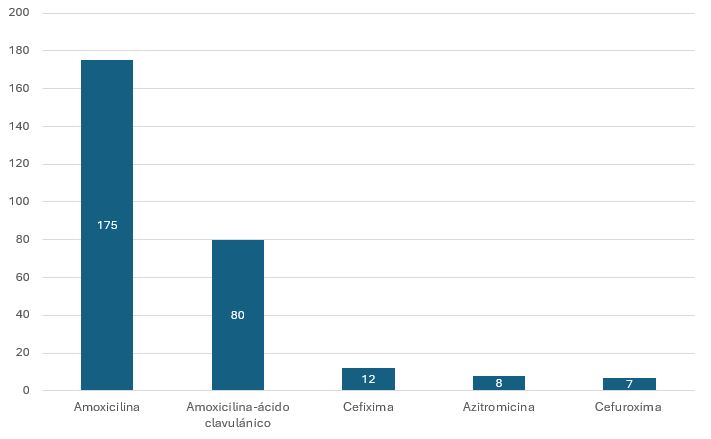
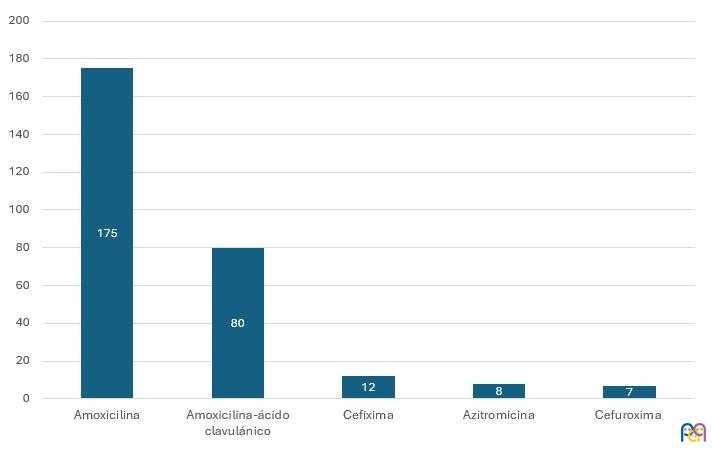
El número de OMA supuradas incluido en el estudio ha sido 353, de las cuales 115 han tenido que ser descartadas del análisis de datos por no disponer de suficiente información. La mediana de edad ha sido de 4 años (rango intercuartílico: 2 a 6), con una discreta prevalencia en hombres (relación hombre/mujer de 1,11). El antibiótico oral más frecuentemente prescrito ha sido amoxicilina (n = 175) seguido por amoxicilina-ácido clavulánico (n = 80) (Figura 1). Un 56,7% de los procesos ha presentado una correcta adecuación del tratamiento antibiótico a las guías terapéuticas de referencia (135 de un total de 238 OMA supuradas). El principal fallo en la adecuación terapéutica ha sido la infradosificación (82,5%). En 145 OMA supuradas se solicitó cultivo de exudado ótico con una tasa de positividad del 88,2% (n = 128), siendo el germen más frecuentemente aislado Haemophilus influenzae en 61 ocasiones (47,6% del total de exudados positivos), seguido de Staphylococcus aureus (n = 21; 16,4% del total de exudados positivos). En la Tabla 1 se exponen los principales resultados del análisis de adecuación terapéutica en OMA supurada.
| Figura 1. Número total de antibióticos prescritos en casos de otitis media aguda supurada (n = 238) |
|---|
 |
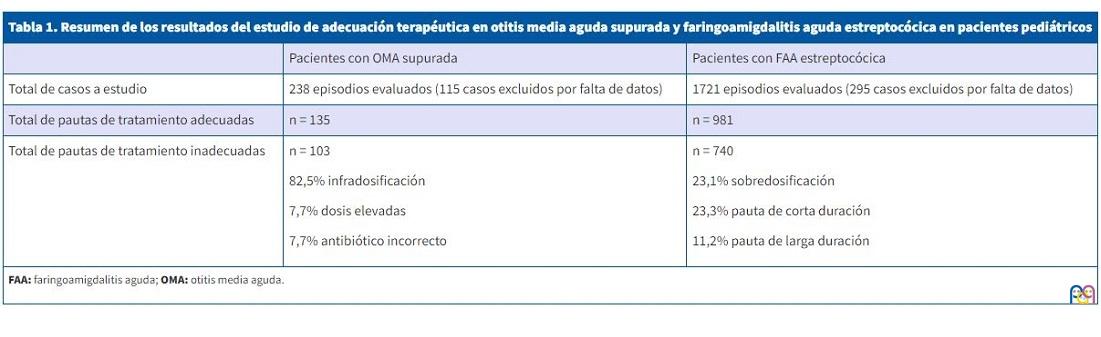
| Tabla 1. Resumen de los resultados del estudio de adecuación terapéutica en otitis media aguda supurada y faringoamigdalitis aguda estreptocócica en pacientes pediátricos | ||
|---|---|---|
| Pacientes con OMA supurada | Pacientes con FAA estreptocócica | |
| Total de casos a estudio | 238 episodios evaluados (115 casos excluidos por falta de datos) | 1721 episodios evaluados (295 casos excluidos por falta de datos) |
| Total de pautas de tratamiento adecuadas | n = 135 | n = 981 |
| Total de pautas de tratamiento inadecuadas |
n = 103 82,5% infradosificación 7,7% dosis elevadas 7,7% antibiótico incorrecto |
n = 740 23,1% sobredosificación 23,3% pauta de corta duración 11,2% pauta de larga duración |
|
FAA: faringoamigdalitis aguda; OMA: otitis media aguda. |
||
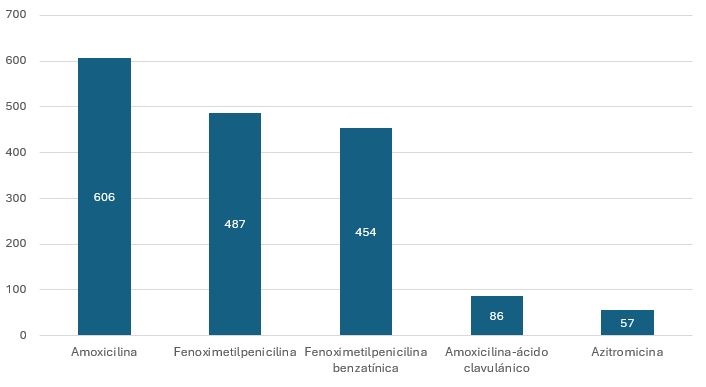
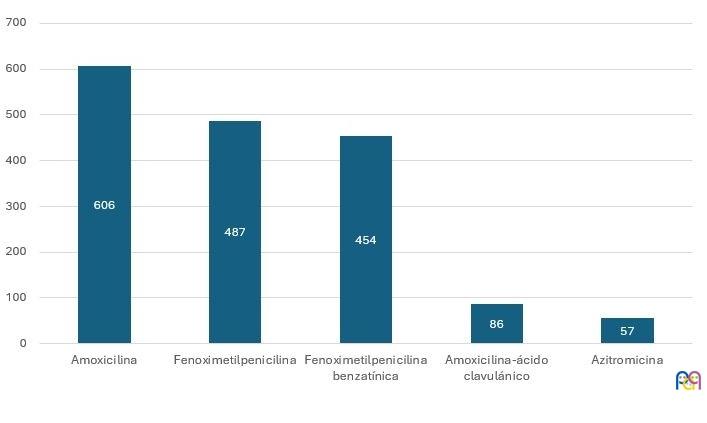
En cuanto a los datos obtenidos del análisis de los pacientes con diagnóstico de FAA estreptocócicas, 1721 han sido incluidas finalmente en este estudio, sin apenas diferencias por sexo (relación hombre/mujer de 1,08). La mediana de edad ha sido de 6 años (rango intercuartílico: 5 a 9). El antibiótico más frecuentemente prescrito ha sido amoxicilina (n = 606; 35% de los episodios), siendo utilizado a dosis recomendadas en el 74,2% de los episodios. Fenoximetilpenicilina (n = 487; 28,2%) y fenoximetilpenicilina benzatínica (n = 454; 26,3%) han sido los antibióticos prescritos en segundo lugar (Figura 2). La utilización a dosis adecuada de fenoximetilpenicilina ha sido del 99%, y la de fenoximetilpenicilina benzatínica del 81,4%. En un total de 1123 episodios se realizaron TDRA para EbhGA, siendo positivos un total de 729 (64,3%). Los cultivos faríngeos han sido realizados en 833 pacientes (llamativamente solo en 166 pacientes con TDRA negativo), siendo positivos para EbhGA en 495 episodios (59,4%). El número de episodios de FAA estreptocócicas adecuadamente tratados ha sido de 981 (57%), siendo los principales motivos de incorrecta adecuación terapéutica la sobredosificación del principio activo (23,1%), así como la duración más corta de la indicada (23,3%). En la Tabla 1 se exponen los principales resultados del análisis de adecuación terapéutica en FAA estreptocócica.
| Figura 2. Número total de antibiótico prescrito en casos de faringoamigdalitis aguda estreptocócica (n = 1721) |
|---|
 |
DISCUSIÓN
La FAA es un proceso infeccioso de diagnóstico frecuente tanto para el pediatra de AP como para el de urgencias hospitalarias. Su etiología en la población pediátrica es principalmente vírica, pero el impacto de la FAA estreptocócica tiene particular interés por sus potenciales complicaciones a corto y largo plazo en caso de no ser tratadas correctamente4,5.
En cuanto al manejo clínico se recomienda la aplicación de una escala clínica para determinar la necesidad o no de realizar un TDRA para EbhGA. En el caso de la escala de McIsaac, tiene un valor predictivo positivo de 28-35% con 3 puntos y de 51-53% con 4 puntos6,7. El documento de consenso de FAA de la AEP del año 2011 recomienda la realización de un TDRA para EbhGA cuando la puntuación de McIsaac es igual o superior a 2 puntos en ausencia de sintomatología viral. En caso de alta sospecha con TDRA negativo o no disponible, recomiendan la realización de cultivo faríngeo1,8. Por su parte, la Asociación Española de Pediatría de Atención Primaria (AEPap) recomienda la realización de un TDRA en caso de 3 o 4 puntos en la escala de Centor9. En cuanto al tratamiento, la penicilina V (fenoximetilpenicilina potásica o benzatina) y la amoxicilina continúan siendo los antibióticos de primera elección con una pauta de 10 días de duración, esta última pudiéndose administrar en una dosis diaria o repartida en dos tomas diarias sin alterar la tasa de erradicación de EbhGA al finalizar el tratamiento2,10. En caso de mal cumplimiento por vía oral o vómitos, la mejor opción sería penicilina G benzatina en dosis única intramuscular (esta pauta es primera elección en algunos países para mejorar el cumplimiento)1,11.
Los estudios publicados de adecuación de la prescripción antibiótica de FAA han arrojado resultados dispares. Una evaluación de la prescripción antibiótica, realizada en AP en Aragón en pacientes de 0 a 14 años con diagnóstico de infección de vías respiratorias altas publicado en 2014, determinó que los pacientes con FAA (75%) han sido los que con mayor proporción recibieron tratamiento antibiótico12. Piñeiro13 evaluó en el año 2015 todos los informes de alta y pruebas complementarias realizadas en los niños menores de 14 años diagnosticados de FAA en un servicio de urgencias pediátricas, concluyendo que la prescripción antibiótica fue del 46,3%. En el 100% de los tratados se realizó estudio microbiológico y correcta selección antimicrobiana, y la duración e intervalo entre dosis tuvo una adecuación mayor del 85%. Ochoa14 realizó un estudio prospectivo multicéntrico en 11 hospitales españoles publicado en 2003, demostrando una baja utilización de antibióticos de primera elección para FAA estreptocócica.
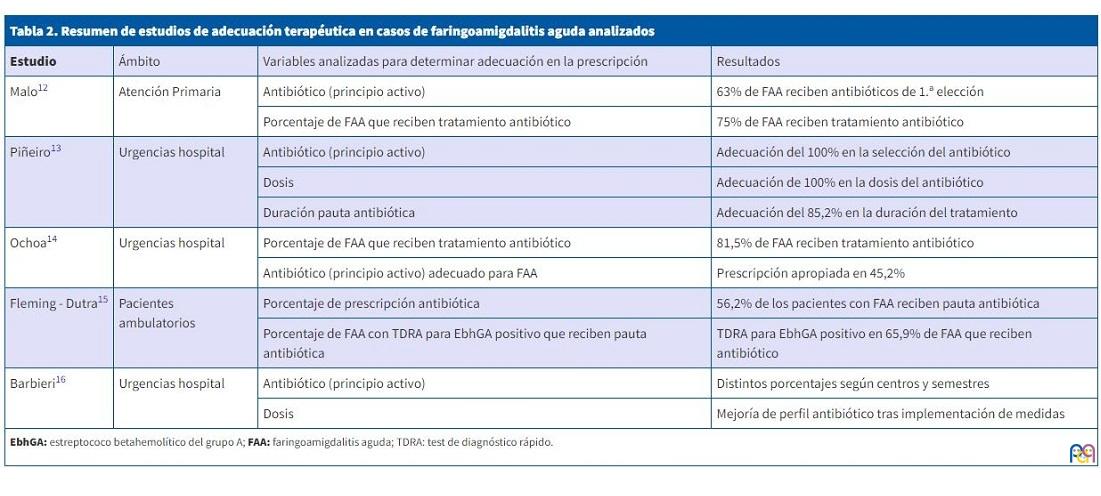
En los años 2010 y 2011 fueron evaluadas 184 032 visitas ambulatorias en Estados Unidos a través de los datos aportados por los CDC, obteniendo que en el 12,6% de las visitas se prescribió tratamiento antibiótico. Las FAA ocuparon el tercer lugar en frecuencia y su adecuación terapéutica fue del 65,9%15. Entre los años 2014 y 2019 fue evaluada la adecuación de prescripción antibiótica en FAA en 3 departamentos de emergencias pediátricas en Italia, demostrando una reducción en la utilización innecesaria de antibióticos de amplio espectro tras implementar ciertas medidas16. En la Tabla 2 se exponen los principales resultados de estos estudios de FAA.
| Tabla 2. Resumen de estudios de adecuación terapéutica en casos de faringoamigdalitis aguda analizados | |||
|---|---|---|---|
| Estudio | Ámbito | Variables analizadas para determinar adecuación en la prescripción | Resultados |
| Malo12 | Atención Primaria | Antibiótico (principio activo) | 63% de FAA reciben antibióticos de 1.ª elección |
| Porcentaje de FAA que reciben tratamiento antibiótico | 75% de FAA reciben tratamiento antibiótico | ||
| Piñeiro13 | Urgencias hospital | Antibiótico (principio activo) | Adecuación del 100% en la selección del antibiótico |
| Dosis | Adecuación de 100% en la dosis del antibiótico | ||
| Duración pauta antibiótica | Adecuación del 85,2% en la duración del tratamiento | ||
| Ochoa14 | Urgencias hospital | Porcentaje de FAA que reciben tratamiento antibiótico | 81,5% de FAA reciben tratamiento antibiótico |
| Antibiótico (principio activo) adecuado para FAA | Prescripción apropiada en 45,2% | ||
| Fleming - Dutra15 | Pacientes ambulatorios | Porcentaje de prescripción antibiótica | 56,2% de los pacientes con FAA reciben pauta antibiótica |
| Porcentaje de FAA con TDRA para EbhGA positivo que reciben pauta antibiótica | TDRA para EbhGA positivo en 65,9% de FAA que reciben antibiótico | ||
| Barbieri16 | Urgencias hospital | Antibiótico (principio activo) | Distintos porcentajes según centros y semestres |
| Dosis | Mejoría de perfil antibiótico tras implementación de medidas | ||
|
EbhGA: estreptococo betahemolítico del grupo A; FAA: faringoamigdalitis aguda; TDRA: test de diagnóstico rápido. |
|||
Si comparamos los resultados de los estudios mencionados en adecuación en la prescripción antibiótica con nuestro estudio en FAA estreptocócica, hemos obtenido resultados algo más bajos que el resto (teniendo en cuenta la disparidad de resultados de los estudios mencionados anteriormente). Un factor determinante en la valoración de la adecuación en la prescripción antibiótica es el correcto registro del peso del paciente y que este no sea muy distante en tiempo respecto a la prescripción antibiótica. A raíz de la situación de pandemia por COVID-19, muchas revisiones del programa de salud infantil han sido retrasadas con sus registros antropométricos. A su vez, la alta presión asistencial con la que lidian los pediatras de AP no permite el correcto registro en la historia clínica del paciente del peso utilizado para la prescripción antibiótica. Teniendo en cuenta esto, posiblemente el grado de adecuación terapéutica sea superior a los datos obtenidos. Claramente, los errores en la duración de la pauta antibiótica no tienen una justificación más que una mala adecuación a las recomendaciones de las guías actuales.
La otitis media (OM) es otro proceso infeccioso de frecuente diagnóstico en la consulta de Pediatría de AP17,18. Afecta principalmente a niños menores de 5 años y su incidencia es más alta en países menos desarrollados19. En cuanto a su etiología, cabe recalcar la reducción de Streptococcus pneumoniae como germen habitual a raíz de la inclusión en el calendario vacunal de la vacuna antineumocócica conjugada20. La OM engloba 3 procesos: OMA, OMA supurativa y OM con supuración crónica21. El diagnóstico depende de la aparición de signos y síntomas típicos (otalgia, alteración en la otoscopia y fiebre o mal estado general), clasificando la OMA en confirmada o posible según la presencia de todos los criterios o parte de ellos22. La indicación de tratamiento antibiótico depende de la edad del paciente, sus antecedentes personales y el grado de afectación, siendo en la actualidad la amoxicilina la primera opción terapéutica23. En las últimas recomendaciones de la AEP publicadas en 2023, se amplía el grupo de pacientes en quienes está indicado una actitud expectante con un tratamiento analgésico como primera opción y su revaloración clínica posterior en el corto plazo24.
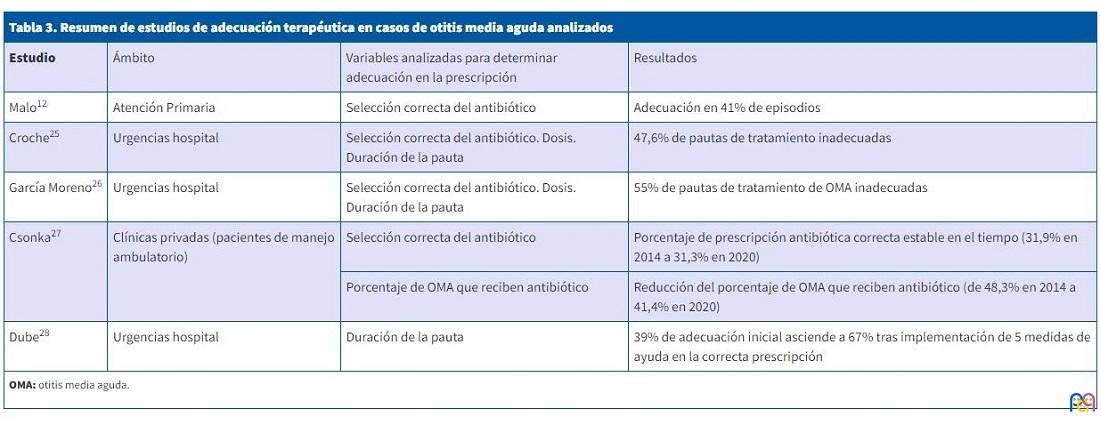
En cuanto a los datos publicados de prescripción antibiótica adecuada en OMA en Pediatría existe también una variación en los resultados de los distintos estudios. Malo12 analizó la prescripción antibiótica en AP en Aragón durante un año para los pacientes diagnosticados de OMA, concluyendo que el porcentaje de prescripción antibiótica era del 72% y que el grado de adecuación terapéutica era bajo. Croche25 evaluó en el año 2013 el grado de adecuación de la prescripción antibiótica en urgencias de un hospital comarcal, concluyendo que el grado de inadecuación fue del 51,9% y la principal enfermedad en la que se produjo prescripción inadecuada fue OMA (47,6%). García-Moreno26 analizó el grado de adecuación de la prescripción antibiótica en un servicio de urgencias pediátricas durante un año en pacientes con diagnóstico de proceso infeccioso. Concluyó que la adecuación terapéutica fue del 49,3%, siendo los fallos más frecuentes en pacientes con diagnóstico de OMA (especialmente en menores de 2 años), infección urinaria y conjuntivitis aguda. Csonka27 analizó la prescripción ambulatoria de antibióticos en pacientes pediátricos con OMA entre 2014 y 2020 en Finlandia, concluyendo que la selección del antibiótico fue adecuada en el 80,1% cuando el prescriptor era pediatra, 67% cuando era médico generalista y, llamativamente, del 55,1% cuando era otorrinolaringólogo. Dube28 analizó el impacto de 5 medidas para mejorar la adecuación en la duración de la prescripción antibiótica en pacientes con OMA en urgencias, detectando una mejora del 39% hasta 67% en las variables analizadas. En la Tabla 3 se exponen los principales resultados de estos estudios en OMA.
| Tabla 3. Resumen de estudios de adecuación terapéutica en casos de otitis media aguda analizados | |||
|---|---|---|---|
| Estudio | Ámbito | Variables analizadas para determinar adecuación en la prescripción | Resultados |
| Malo12 | Atención Primaria | Selección correcta del antibiótico | Adecuación en 41% de episodios |
| Croche25 | Urgencias hospital | Selección correcta del antibiótico. Dosis. Duración de la pauta | 47,6% de pautas de tratamiento inadecuadas |
| García Moreno26 | Urgencias hospital | Selección correcta del antibiótico. Dosis. Duración de la pauta | 55% de pautas de tratamiento de OMA inadecuadas |
| Csonka27 | Clínicas privadas (pacientes de manejo ambulatorio) | Selección correcta del antibiótico | Porcentaje de prescripción antibiótica correcta estable en el tiempo (31,9% en 2014 a 31,3% en 2020) |
| Porcentaje de OMA que reciben antibiótico | Reducción del porcentaje de OMA que reciben antibiótico (de 48,3% en 2014 a 41,4% en 2020) | ||
| Dube28 | Urgencias hospital | Duración de la pauta | 39% de adecuación inicial asciende a 67% tras implementación de 5 medidas de ayuda en la correcta prescripción |
|
OMA: otitis media aguda. |
|||
Al comparar nuestros datos de adecuación terapéutica con el resto de los estudios publicados, el resultado se asemeja a la media, pero es bastante mejorable. Las principales limitaciones a la hora de valorar la adecuación terapéutica en la dosificación es el correcto registro del peso del paciente, lo cual posiblemente hubiese mejorado nuestros resultados. Otro punto limitante es el correcto diagnóstico y la complejidad de ello (sobre todo en la valoración de la otoscopia). Para no incurrir en el error de incluir otitis serosas mal catalogadas como OMA, se decidió incluir solo en el estudio a los pacientes con OMA supurada. Por último, otras limitaciones a destacar son la falta de comprobación de que la administración del antibiótico fue correcta (en cuanto a la toma del mismo y a la duración prescrita), la naturaleza retrospectiva del estudio y los posibles errores de registro de datos en la historia clínica. A pesar de sus limitaciones, hay que destacar el amplio número de episodios evaluados y su realización a través del registro electrónico, lo cual disminuye la variabilidad en la recogida de datos, obteniendo mayor objetividad.
Finalmente, hay que recalcar que este estudio ha sido realizado en AP de Álava, por lo cual su resultado no puede extrapolarse a otras zonas geográficas ni al ámbito hospitalario.
CONCLUSIONES
Es de máxima importancia analizar el grado de adecuación terapéutica a los actuales documentos de consenso en Pediatría de AP, ya que es el primer eslabón de contacto de la población infantil con el sistema sanitario. Detectar un bajo grado de adecuación en el tratamiento para procesos en los cuales está demostrado que la prescripción antibiótica es elevada como son FAA y OMA tendrá un impacto negativo a futuro en la resistencia antibiótica bacteriana.
Más allá de las limitaciones que pueda presentar este estudio y de los datos mejorables detectados, es un punto de partida sobre el cual trabajar. Hay que destacar por último la gran importancia que tiene un correcto registro electrónico en la historia clínica de los pacientes en AP, para lo cual hay que dotar al pediatra de herramientas que faciliten ese objetivo, teniendo en cuenta la presión asistencial con la que lidia en el día a día, lo cual permitirá en un futuro proveer de datos más certeros para realizar estudios a gran escala de este tipo.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: diseño y realización del estudio, análisis de datos, redacción y corrección del artículo (MVM, JTRA), redacción y corrección del artículo, traducción de título, resumen y palabras claves (BBS), obtención y análisis de datos, realización de análisis estadísticos (SGGD).
ABREVIATURAS
AEP: Asociación Española de Pediatría · AEPap: Asociación Española de Pediatría de Atención Primaria · AP: Atención Primaria · CIE-10: Clasificación Internacional de Enfermedades y Problemas Relacionados con la Salud, décima edición · EbhGA: estreptococo betahemolítico del grupo A · FAA: faringitis o faringoamigdalitis aguda · OM: otitis media · OMA: otitis media aguda · TDRA: test de diagnóstico rápido.
BIBLIOGRAFÍA
- Piñeiro Pérez R, Hijano Bandera F, Álvez González F, Fernández Landaluce A, Silva Rico JC, Pérez Cánovas C, et al. Consensus document on the diagnosis and treatment of acute tonsillopharyngitis. An Pediatr (Barc). 2011;75(5):342.e1-13. https://doi.org/10.1016/j.anpedi.2011.07.015
- Piñeiro Pérez R, Álvez González F, Baquero-Artigao F, Cruz Cañete M, De la Flor I Bru J, Fernández Landaluce A, et al; Grupo Colaborador de Faringoamigdalitis Aguda en Pediatría. Diagnosis and treatment of acute tonsillopharyngitis. Consensus document update. An Pediatr (Barc). 2020;93(3):206.e1-206.e8. https://doi.org/10.1016/j.anpedi.2020.05.004
- Del Castillo F, Baquero Artigao F, De la Calle Cabrera T, López RoblesMV, Ruiz Canela J, Alfayate Miguelez S, et al. Consensus document on the aetiology, diagnosis and treatment of acute otitis media. An Pediatr (Barc). 2012;77(5):345-8. https://doi.org/10.1016/j.anpedi.2012.05.026
- Esposito S, Blasi F, Bosis S, Droghetti R, Faelli N, Lastrico A, et al. Aetiology of acute pharyngitis: the role of atypical bacteria. J Med Microbiol. 2004;53:645-51. https://doi.org/10.1099/jmm.0.05487-0
- Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL, Schwartz RH. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis. 2002;35(2):113-25. https://doi.org/10.1086/340949
- Pérez R, Pavez D, Rodríguez J, Cofré J. Recommendations for diagnosis and etiological treatment of acute streptococcal pharyngotonsilitis in pediatrics. Rev Chilena Infectol. 2019;36(1):69-77. https://doi.org/10.4067/S0716-10182019000100069
- Engel ME, Cohen K, Gounden R, Kengne AP, Barth DD, Whitelaw AC, et al. The Cape Town Clinical Decision Rule for Streptococcal Pharyngitis in Children. Pediatr Infect Dis J. 2017;36(3):250-5. https://doi.org/10.1097/INF.0000000000001413
- Kalra MG, Higgins KE, Perez ED. Common Questions About Streptococcal Pharyngitis. Am Fam Physician. 2016;94(1):24-31.
- Cubero Santos A, García Vera C, Lupiani Castellanos P. Guía de Algoritmos en Pediatría de Atención Primaria. Faringoamigdalitis. AEPap. 2015 [en línea] [consultado el 31/01/2024]. Disponible en https://algoritmos.aepap.org/algoritmo/13/faringoamigdalitis
- Nakao A, Hisata K, Fujimori M, Matsunaga N, Komatsu M, Shimizu T. Amoxicillin effect on bacterial load in group A streptococcal pharyngitis: comparison of single and multiple daily dosage regimens. BMC Pediatr. 2019;19(1):205. https://doi.org/10.1186/s12887-019-1582-8
- Martins Moreira Anjos l, Barros Marcondes M, Ferreira Lima M, Lia Mondelli A, Politi Okoshi M. S. Streptococcal acute pharyngitis. Rev Soc Bras Med Trop. 2014;47(4):409-13. https://doi.org/10.1590/0037-8682-0265-2013
- Malo S, Bjerrum l, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Antibiotic prescribing in acute respiratory tract infections in general practice. An Pediatr (Barc). 2015;82(6):412-6. https://doi.org/10.1016/j.anpedi.2014.07.016
- Piñeiro Pérez R, Hernández Martín D, Carro Rodriguez MA, Casado Verrier E, Reques Cosme R, Carbaño Aguado I. Adecuación del diagnóstico y tratamiento de la faringoamigdalitis aguda a las guías actuales. Rev Pediatr Aten Primaria. 2016;18:317-24.
- Ochoa C, Inglada l, Eiros JM, Solís G, Vallano A, Guerra l. Spanish Study Group on Antibiotic Treatments. Appropriateness of antibiotic prescriptions in community-acquired acute pediatric respiratory infections in Spanish emergency rooms. Pediatr Infect Dis J. 2001;20(8):751-8. https://doi.org/10.1097/00006454-200108000-00007
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, Bartoces M, Enns EA, File Jr TM, et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010-2011. JAMA. 2016;315(17):1864-73. https://doi.org/10.1001/jama.2016.4151
- Barbieri E, De Luca M, Minute M, D´Amore C, Ciofi Degli Atti ML, Martelossi S,et al. Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success. Antibiotics (Basel). 2020;9(12):867. https://doi.org/10.3390/antibiotics9120867
- Blanco MV, Hamdy RF, Liu CM, Jones H, Montalbano A, Nedved A. Antibiotic Prescribing Patterns for Pediatric Urgent Care Clinicians. Pediatr Emerg Care. 2022;38(9):1538-40. https://doi.org/10.1097/PEC.0000000000002809
- Messina F, Clavenna A, Cartabia M, Piovani D, Bortolotti A, Fortino I, et al. Antibiotic prescription in the outpatient paediatric population attending emergency departments in Lombardy, Italy: a retrospective database review. BMJ Paediatr Open. 2019;3(1):000546. https://doi.org/10.1136/bmjpo-2019-000546
- Monasta l, Ronfani l, Marchetti F, Montico M, Vecchi Brumatti l, Bavcar A, et al. Burden of disease caused by otitis media: systematic review and global estimates. PLoS One. 2012;7(4):36226. https://doi.org/10.1371/journal.pone.0036226
- Ubukata K, Morozumi M, Sakuma M, Takata M, Mokuno E, Tajima T, et al. Etiology of Acute Otitis Media and Characterization of Pneumococcal Isolates After Introduction of 13-Valent Pneumococcal Conjugate Vaccine in Japanese Children. Pediatr Infect Dis J. 2018;37(6):598-604. https://doi.org/10.1097/INF.0000000000001956
- Schilder AG, Chonmaitree T, Cripps AW, Rosenfeld RM, Casselbrant ML, Haggard MP, et al. Otitis media. Nat Rev Dis Primers. 2016;2(1):16063. https://doi.org/10.1038/nrdp.2016.63
- American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113(5):1451-65. https://doi.org/10.1542/peds.113.5.1451
- Lieberthal AS, Carroll AE, Chonmaitree T, Ganiats TG, Hoberman A, Jackson MA, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):964-99. https://doi.org/10.1542/peds.2012-3488
- López Martín D, Piñeiro Pérez R, Martínez Campos l, Ares Álvarez J, De la Calle Cabrera T, Jiménez Huerta I, et al. Actualización del documento de consenso sobre etiología, diagnóstico y tratamiento de la otitis media aguda y sinusitis. An Pediatr (Barc).2023;28(5):362-72. https://doi.org/10.1016/j.anpedi.2023.03.003
- Croche Santander B, Campos Alonso E, Sánchez Carrión A, Marcos Fuentes l, Diaz Flores I, Vargas JC, et al. Adecuación de la prescripción de antimicrobianos en población pediátrica en un servicio de urgencias hospitalario. An Pediatr (Barc). 2018;88(5):259-65. https://doi.org/10.1016/j.anpedi.2017.06.001
- García-Moreno FJ, Escobar-Castellanos M, Marañón R, Rivas-García A, Manrique-Rodríguez S, Mora-Capín A, et al. Adecuación de la prescripción de antimicrobianos en procesos ambulatorios atendidos en Urgencias. An Pediatr (Barc). 2022;96(3):179-89. https://doi.org/10.1016/j.anpedi.2020.11.019
- Csonka P, Palmu S, Paula Heikkilä P, Huhtala H, Korppi M. Outpatient Antibiotic Prescribing for 357,390 Children With Otitis Media. Pediatr Infect Dis J. 2022;41(12):947-52. https://doi.org/10.1097/INF.0000000000003693
- Dube AR, Zhao AR, Odozor CU, Jordan K, Garuba FO, Kennedy A, et al. Improving Prescribing for Otitis Media in a Pediatric Emergency Unit: A Quality Improvement Initiative. Pediatr Qual Saf. 2023;8(1):625. https://doi.org/10.1097/pq9.0000000000000625