
Vol. 25 - Num. 99
Originales
¿Cómo usan el teléfono móvil los niños de Castilla y León?
M.ª Cristina García de Riberaa, María Alfaro Gonzálezb, María Tríguez Garcíac, Ana Fierro Urturid, Marta Esther Vázquez Fernándeze, Franco Sorgef, Eva M.ª Dulce Lafuenteg, Elena Santamaría Marcosh, M.ª Fe Muñoz Morenoi
aPediatra. CS Tórtola. Valladolid. España.
bServicio de Pediatría. Hospital Medina del Campo. Valladolid. España.
cPediatra. CS Eras del Bosque. Palencia. España.
dPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
ePediatra. CS Circunvalación. Valladolid. España .
fPediatra. CS Aranda Norte. Aranda de Duero. Burgos. España.
gPediatra. CS Aranda Sur. Aranda de Duero . Burgos. España.
hPediatra. CS López Saiz. Burgos. España.
iBioestadístico. Unidad de Apoyo a la Investigación. Hospital Clínico Universitario de Valladolid. España.
Correspondencia: MC García. Correo electrónico: cristinaderibera@hotmail.com
Cómo citar este artículo: García de Ribera MC, Alfaro González M, Tríguez García M, Fierro Urturi A, Vázquez Fernández ME, Sorge F, et al. ¿Cómo usan el teléfono móvil los niños de Castilla y León? . Rev Pediatr Aten Primaria. 2023;25:251-60. https://doi.org/10.60147/d3636814
Publicado en Internet: 13-09-2023 - Número de visitas: 12655
Resumen
Introducción: los teléfonos móviles suponen una gran herramienta de comunicación entre iguales, pero un uso inapropiado puede repercutir en las relaciones familiares, sociales y en el rendimiento escolar.
Objetivos: el objetivo principal del trabajo fue estudiar el uso del teléfono móvil en la población pediátrica de varias áreas de salud de Castilla y León.
Material y métodos: estudio multicéntrico prospectivo en varios centros de salud y un hospital comarcal. Se pasó una encuesta a padres de niños que acudían a consulta y a los adolescentes que lo desearon, quienes también respondieron a un test de dependencia (TDM).
Resultados: el móvil es el dispositivo electrónico que más usaban los niños para navegar por Internet. La media de edad en la que tuvieron el primer móvil propio fue de 10,35 años; la mayoría, con acceso a Internet.
El 68% de ellos accedía sin ningún control parental. El 70% de padres establecieron unas normas al proporcionárselo. Un tercio reconocían que estas no se cumplían.
El número de horas diarias de uso aumentaba según la edad de los niños. De los adolescentes, más del 50% lo usaba más de dos horas al día. Los más pequeños lo utilizaban para ver vídeos y los mayores para chatear y redes sociales.
El uso del móvil se relacionaba con el uso de gafas, pero no con el rendimiento académico, problemas de sueño ni práctica de deporte.
En el TDM se observaron muchas respuestas positivas en los ítems de los cuatro apartados en los que se divide el test, especialmente en el de falta de control.
Conclusiones: la media de edad de adquisición del primer teléfono móvil propio es menor de la recomendada. Su abuso puede generar conductas con rasgos de adicción.
Palabras clave
● Adicción ● Internet ● Tecnología ● Teléfono inteligenteINTRODUCCIÓN
Gracias a los teléfonos móviles o smartphones podemos acceder a Internet de manera constante. La mayoría de la población, de hecho, accede a esta red a través de su teléfono.
Supone una gran herramienta para facilitar la comunicación entre iguales, pero un uso excesivo o inapropiado puede repercutir en las relaciones familiares, sociales y en el rendimiento escolar1.
El uso problemático del teléfono móvil (PMPU) generalmente se conceptualiza como un comportamiento adictivo2, porque presenta los rasgos centrales de las adicciones, como la prominencia cognitiva, pérdida de control, modificación del estado de ánimo, tolerancia, retraimiento, conflicto y recaída3.
En estudios previos se revela una amplia variabilidad en las tasas de prevalencia, que oscilan entre el 2,4 y el 31,3%4,5.
Sucesivas investigaciones han demostrado que el PMPU se asocia con comportamiento sedentario, peor salud física, peor capacidad de atención y rendimiento escolar6 y finalmente, peor calidad de vida, vinculados a los entornos escolar y familiar. Además, hay evidencia de un vínculo entre PMPU y comportamientos disfuncionales y síntomas psicopatológicos tales como miedo a perderse algo (FoMO), hiperactividad, mala conducta prosocial, baja autoestima, estrés, ansiedad y depresión e ideación suicida.
Así mismo, se ha demostrado la potencial interferencia del uso de teléfonos móviles en la calidad del sueño y la relación de problemas del sueño con el uso de teléfonos inteligentes y PMPU7. Su uso, especialmente a la hora de dormir, se asocia negativamente con diferentes características del sueño entre niños y adolescentes, como cantidad inadecuada, peor calidad y alta somnolencia diurna8.
Ciertos adolescentes pueden ser más susceptibles a los efectos de PMPU. Los rasgos patológicos de la personalidad están relacionados con deterioro tanto en el contexto interpersonal como personal, así como con adicciones y uso problemático de la tecnología9.
A la luz de lo anterior, el presente estudio tiene como objetivo realizar un estudio en la población pediátrica de varias áreas de salud de Castilla y León sobre el uso del teléfono móvil.
MATERIAL Y MÉTODOS
Se llevó a cabo un estudio multicéntrico prospectivo, observacional, transversal, descriptivo. La muestra fue recogida en las consultas de Pediatría de Atención Primaria de un centro de salud de Burgos, dos de Aranda de Duero, dos de Valladolid, uno de Palencia y en consultas externas del Hospital de Medina del Campo, de julio a octubre de 2022.
En ese periodo temporal se pasó una encuesta a padres de niños que acudían a consulta sobre el uso del teléfono móvil que hacían sus hijos. En paralelo, se pasó otra encuesta a los adolescentes de 11 a 14 años que lo desearon. Se excluyó a los menores de un año y a los niños con patología neurológica o mental grave.
Las encuestas recogían variables sociodemográfricas, de salud y datos sobre el uso habitual que hacían de este dispositivo. A los niños a partir de 11 años se les pasó el test de dependencia al móvil (TDM), que está validado a partir de esa edad. Consta de 12 de preguntas que se agrupan en 4 apartados: Abstinencia/ Abuso/ Tolerancia/ Falta de control (Tabla 1).
| Tabla 1. Test de dependencia al móvil (TDM) de Choliz (versión breve) | ||
|---|---|---|
| Preguntas de la encuesta | Sí | No |
| Abstinencia | ||
| 1. Dedico más tiempo del que me gustaría a hablar por teléfono móvil, jugar, chatear o estar en redes sociales | ||
| 2. Me he acostado más tarde o he dormido menos porque estaba usando mi teléfono móvil | ||
| 3. Utilizo mi teléfono móvil en situaciones en las que, aunque no sea peligroso, no es adecuado hacerlo (comiendo, mientras otras personas me hablan, etc.) | ||
| Abuso | ||
| 4. Si mi teléfono móvil se estropeara durante un periodo prolongado de tiempo y tardara mucho en arreglarse, me sentiría muy mal | ||
| 5. Necesito usar mi móvil cada vez con más frecuencia | ||
| 6. Si no tengo mi teléfono móvil, me siento mal | ||
| Tolerancia | ||
| 7. Cuando tengo mi teléfono móvil conmigo, no puedo dejar de usarlo | ||
| 8. Desde que tengo mi teléfono móvil, he aumentado la cantidad de WhatsApp que envío | ||
| 9. Nada más levantarme por la mañana, lo primero que hago es ver quién me ha llamado al móvil o si alguien me ha enviado un mensaje | ||
| Falta de control | ||
| 10. Creo que para mí sería insoportable pasar una semana sin teléfono móvil | ||
| 11. Cuando me siento solo, uso mi teléfono móvil (llamadas, WhatsApp, jugar, ver RRSS...) | ||
| 12. Cogería mi teléfono móvil y enviaría un mensaje o navegaría por Internet ahora mismo | ||

Se obtuvo el consentimiento para participar en el estudio tanto del menor como de los padres tutores. El presente trabajo contó con la autorización de cada centro, así como con la aprobación del Comité Ético de Investigación Clínica (CEIC) de cada área de salud.
Los datos obtenidos fueron analizados con el programa estadístico IBM SPSS Statistics versión 24.0 para Windows. Aquellos valores de p <0,05 se consideraron estadísticamente significativos.
RESULTADOS
Rellenaron la encuesta 227 adultos, acompañantes de niños que acudían a consultas de Pediatría, en su mayor parte la madre (79,9%), en menor porcentaje por el padre (16,4%). La mayoría (47,6%) de los adultos tenía entre 41 y 50 años, seguidos de 38,8% que tenían entre 31 y 40 años. La media de edad de los niños fue de 6,92 años (Tabla 2). La mayoría eran de nacionalidad española (88,6%) y tenían un único hermano (49,3%); el 26,4% eran hijos únicos.
| Tabla 2. Resultados principales obtenidos de las encuestas | ||
|---|---|---|
| Muestra | Adultos acompañantes de niños de 1 a 14 años | Adolescentes de 11 a 14 años |
| Media de edad de cada muestra | 6,92 años | 12,58 años |
| Número de niños | 227 niños | 55 adolescentes |
| Media de edad para la adquisición del primer smartphone | 10,35 años | 11,14 años |
|
Niños sin móvil propio Media de edad |
164 (72%) 5,25 años |
7 (13%) 12 años |
|
Niños con móvil Media de edad Sin Internet Media de edad Conexión:
|
63 niños (28%) 11,24 años 3 niños (5%) 6,67 años
|
48 (87%) 12,67 años Ninguno
|
| Control parental | 32% | 19% |
| Contrato/normas de uso | 70% | 65% |
| Se cumplen normas | 67,8% | 51,4% |
Además, 55 adolescentes de entre 11 y 14 años contestaron otra encuesta específica para ellos. La media de edad fue de 12,58 años.
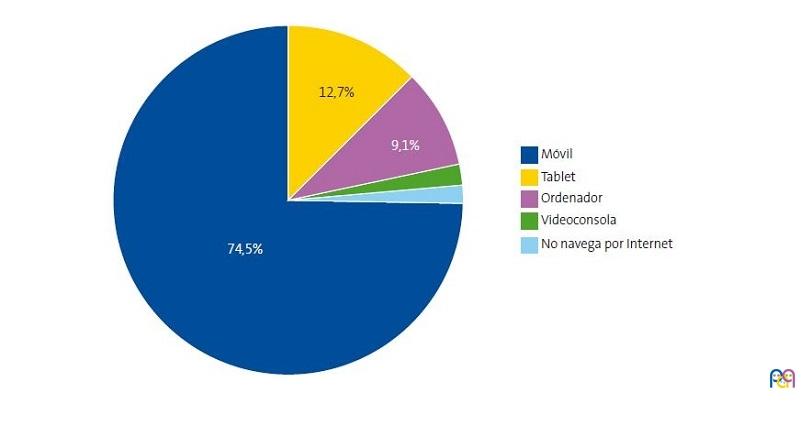
El teléfono móvil era el dispositivo electrónico que más usaban los niños de nuestro estudio para navegar por Internet (45,7%), seguido por la tableta electrónica (24,7%) (Fig. 1), como ocurre con los adolescentes (Fig. 2). Más de la mitad (50,7%) lo usaba preferentemente por la tarde.
| Figura 1. Dispositivo que más usan para navegar por internet |
|---|
 |
| Figura 2. Dispositivo que más usan para navegar por internet de 11 a 14 años |
|---|
 |
La edad media de los que más usaban el smartphone fue de 7,6 años, similar a la de los que usaban tableta. Sin embargo, los que usaban más el ordenador y la videoconsola eran significativamente mayores, siendo la edad media de 10,14 y 9,4 años, respectivamente.
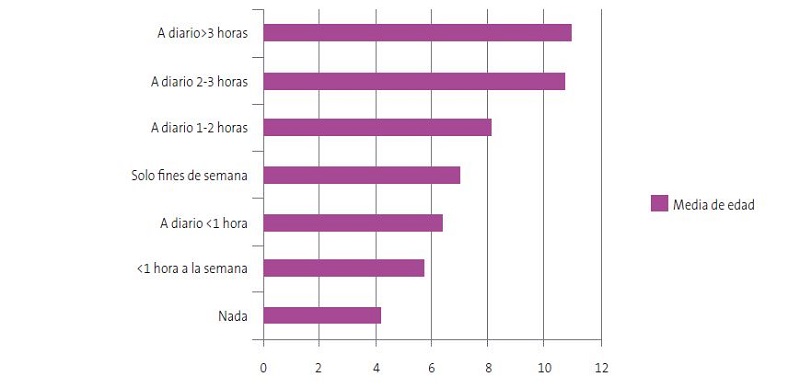
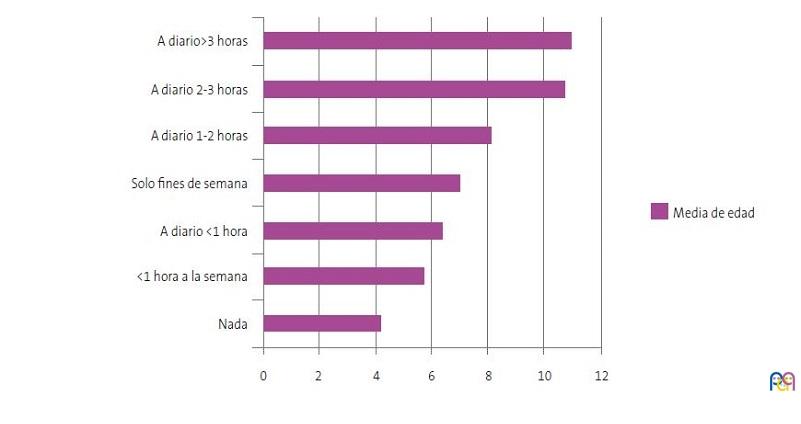
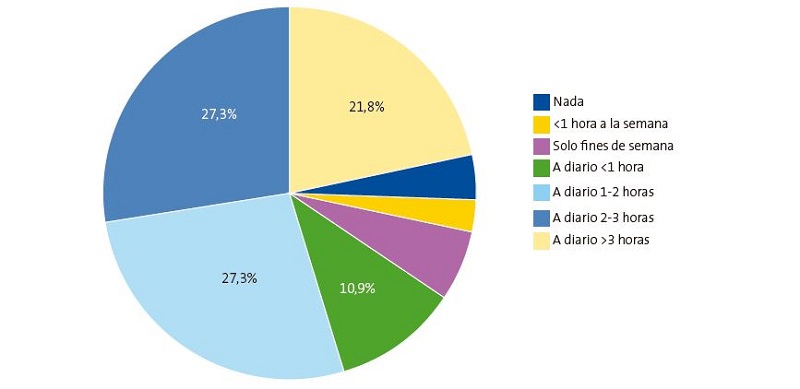
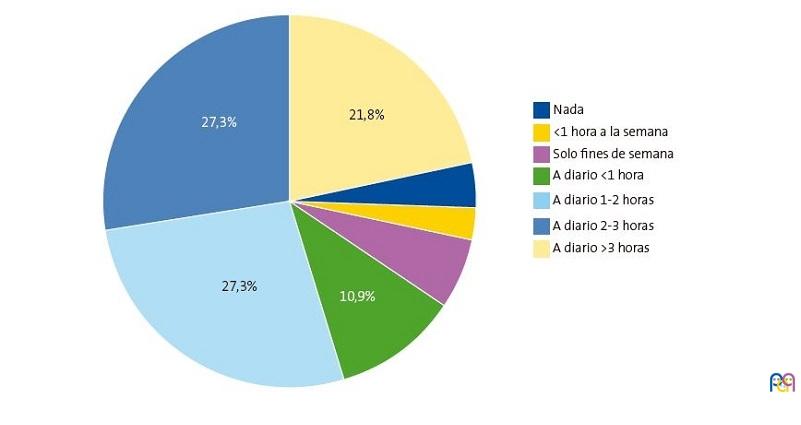
También, el número de horas diarias de uso del smartphone aumentaba significativamente según la edad de los niños (Fig. 3). La media de edad de los que no lo usaban a diario fue de 5,48 años versus a los 8,3 años de los que lo hacían a diario. En la Figura 4 aparece el uso del móvil por parte de los adolescentes: la mitad lo usa más de dos horas al día.
| Figura 3. Número de horas de uso diario según la edad |
|---|
 |
| Figura 4. Número de horas de uso de móvil entre los adolescentes |
|---|
 |
Además, si comparamos las opciones para las que lo utilizan con la edad, hallamos importantes diferencias significativas. Los niños más pequeños lo utilizaban para ver vídeos, con una media de edad de 6,09 años, y los más mayores para hablar (9,89 años), hacer fotos o vídeos (8,56 años), chatear por WhatsApp (10,58 años), redes sociales (RRSS) (10,76 años) y videojuegos (8,5 años).
Entre los adolescentes, un 65,5% lo usaba más en horario de tarde y un 63,6% refería utilizarlo para tareas escolares. La mayoría (67%) lo apagaba en clase. Algo más de la mitad (54%) lo apagaban para dormir y 45% lo hacían para estudiar.
La aplicación más utilizada por ellos era TikTok, seguida de WhatsApp y YouTube. La media de edad de los que utilizaban redes sociales (12,73 años) era mayor que la de los que decían no usarlas (12,14 años). De estos, es significativo cómo los usuarios de Instagram eran mayores (13,12 años) que el resto (12,13 años).
Solo 2 adolescentes referían haber visto algo inapropiado en Internet, 6 preferían no decirlo. Únicamente uno reconoció que se había sentido acosado, dos habían sentido que se habían burlado de ellos en RRSS y otros dos preferían no contestar. El 41,8% pensaban que usaban el móvil más de lo que deberían y 25,5% opinaban que tal vez lo hacían.
En relación con el género, entre los adolescentes, no se encontraron diferencias significativas de las chicas frente a los chicos respecto al dispositivo que más utilizaban para navegar por Internet, el tener o no teléfono móvil propio, el tiempo de uso y las opciones para las que lo utilizaban, salvo los videojuegos, que los varones usaban más que las mujeres: un 79% frente a un 41% de ellas. Tampoco había diferencias de género respecto a tener control parental, tener o no conexión a Internet, ni haber visto algo vergonzante o haberse sentido acosado o que se hubieran burlado de ellos.
Respecto a la edad para la adquisición del primer smartphone se situó en 10,35 años, con una desviación típica (DT) de 2,08. Tenían móvil propio el 28% de los niños. A más de la mitad se lo habían comprado nuevo, los otros lo habían “heredado”. No había diferencias significativas entre la media de edad de un grupo frente a otro.
La mayoría de los niños con teléfono en exclusiva para ellos tenían conexión a Internet. Solo el 5% no disponían de ella. Si comparamos la media de edad de los niños que no tenían conexión a Internet en su teléfono o la tenían solo con WiFi frente al grupo que tenía conexión por datos limitados o ilimitados, también encontramos diferencias significativas: 9,58 años (sin conexión o WiFi), 12,95 (datos limitados) y 11,88 años (datos ilimitados). En la Tabla 2 vemos también cómo se distribuía entre los adolescentes.
Respecto al control del uso, un 78% de los adultos afirmaba que revisaban las aplicaciones que el menor se instalaba: un 70% mediante unas normas de uso o la firma de un “contrato” con el niño antes de proporcionárselo y un 32% mediante programa de control parental. La mayoría usaban Family Link®, de Google, y un 32,2% reconocía que los acuerdos no se estaban cumpliendo. Un 28,8% de los adultos no supervisaba el móvil de los menores para ver lo que escribía o buscaba. Un 50,8% afirmaba que lo revisaba de vez en cuando, y un 28,8% lo hacía casi a diario. El 50,8% tenía establecido un horario de uso de móvil. Un 47,5% lo tenía en su habitación mientras dormía. El 57,6% tenía establecido un límite de gasto.
Un 40% de los adultos estaba preocupado por el uso del teléfono del menor. La media de edad de los niños cuyos padres estaban preocupados (8,73 años) era significativamente mayor que la de los que no (5,63). El 33,3% creían que ellos no eran un buen ejemplo del uso de este dispositivo de cara a los niños.
Hemos encontrado diferencias significativas al analizar el nivel de estudios de los progenitores relacionado con el tipo de conexión Internet y con el control de uso. De tal manera, que los hijos de padres con estudios básicos tenían más conexión por WiFi o no tenían Internet y eran los que en mayor porcentaje instalaban control parental y más supervisaban la descarga de aplicaciones. Mientras que los de padres con estudios de Bachillerato, FP o universitarios accedían a Internet, la mayoría con datos limitados y menor control parental. Pero no hemos encontrado diferencias significativas al relacionar la edad de los padres con al tiempo de uso del móvil que hacen los niños, la posesión o no de uno propio, ni las características de uso y conexión a Internet.
Otros aspectos analizados en el uso del móvil han sido la influencia del modelo familiar, el uso de gafas, los problemas de sueño y la práctica de deporte extraescolar.
Teníamos un 11% de padres separados y aparecieron diferencias respecto a la posesión de móvil propio y el tipo. De los niños cuyos padres vivían juntos, un 74,5% no tenían teléfono móvil, frente a las familias separadas, en los que el 53,8% no lo tenían. La adquisición de un móvil nuevo era significativamente mayor en los hijos de padres que vivían juntos (68,6%). Los separados, en su mayoría (66,7%) le habían dado uno ya usado. Sin embargo, no vimos diferencias significativas con las familias cuyos progenitores vivían juntos, respecto a las horas de uso de móvil de los niños, la conexión a Internet, la supervisión ni el control parental. Tampoco hemos encontrado relación entre la nacionalidad de la familia ni entre el número de hermanos con la posesión o no del móvil y el uso que los niños hacían de él.
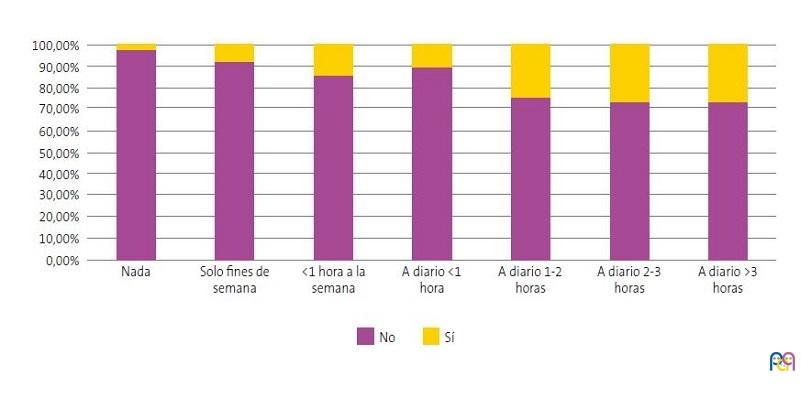
Entre los que no tenían móvil, solo un 8,6% era usuario de gafas, mientras que el porcentaje de usuarios de lentes correctoras era significativamente mayor entre los que sí tenían teléfono móvil propio, siendo un 28,6% de ellos. También se ha visto cómo el porcentaje de usuarios de lentes aumentaba proporcionalmente a las horas de uso del dispositivo (Fig. 5).
| Figura 5. Usuarios de lentes correctoras en relación con horas de uso de smartphone |
|---|
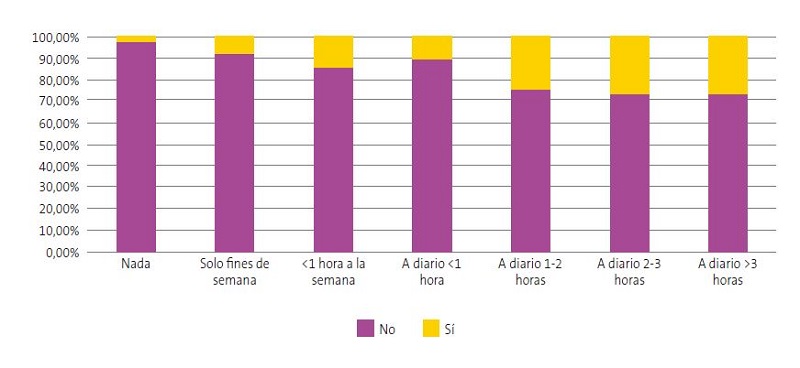 |
Y el último aspecto, aunque el porcentaje de los que tenían problemas para dormir era algo mayor entre los propietarios de teléfono móvil propio, no se ha encontrado significación estadística al respecto. Tampoco la hemos hallado al relacionar las horas de deporte extraescolar que hacían a la semana con el hecho de tener o no móvil propio. Ni al comparar el índice de masa corporal (IMC) con el tiempo de uso.
La mayoría pensaba que las notas del niño no habían disminuido desde que tenía móvil propio, frente a un 16,9% que pensaba que sí habían descendido por esta causa. Un 70,3% de los adolescentes afirmaba que la posesión de teléfono móvil propio no había repercutido en sus calificaciones. No hemos visto relación significativa entre el grado de rendimiento académico con los momentos en los que tenían apagado el móvil, ni con el tener un contrato o normas, se cumplieran o no.
Finalmente, estudiamos la dependencia al móvil mediante el test TDM (test de dependencia al móvil) que consta de 12 de preguntas que se agrupan en 4 apartados: Abstinencia / Abuso / Tolerancia / Falta de control (Tabla 2). La respuesta que más adolescentes han marcado afirmativamente, 56% de ellos, ha sido “Cuando me siento solo, uso mi teléfono móvil (llamadas, WhatsApp, jugar, RRSS…)”, que está dentro del apartado de Falta de control. Dentro del apartado de Abstinencia: el 52% afirma que “Paso más tiempo del que yo quisiera con mi teléfono móvil” y el 42% que “Me he ido a la cama más tarde o dormí menos porque estaba usando mi teléfono”. Del apartado de Tolerancia, el 44% afirma que “Tan pronto como me levanto por la mañana, lo primero que hago es ver quién me ha llamado al móvil o si alguien me ha enviado un mensaje”. El apartado cuyos ítems tienen menos respuestas positivas es el de Abuso.
Se ha encontrado una relación significativa entre la falta de control y el mayor número de horas de uso del móvil de los encuestados. Y entre la abstinencia, abuso, tolerancia y falta de control y el grupo de adolescentes que piensa que usa más el móvil de lo que debería.
No se ha encontrado relación con el grupo que afirma que tiene peores resultados académicos desde que tiene móvil propio.
DISCUSIÓN
El uso del teléfono móvil está muy extendido en la población pediátrica, como se refleja en nuestro estudio, al igual que en la literatura al respecto10.
En el mundo desarrollado, el acceso a Internet forma parte de nuestras vidas. Un estudio europeo muestra que casi la mitad de la población de 9 a 16 años usa su propio smartphone para acceder diariamente a Internet11. Que el teléfono móvil sea el dispositivo más utilizado entre nuestros niños para este acceso es comprensible, ya que la mayoría de los progenitores suelen llevarlo consigo, así como muchos de los adolescentes1.
No existe un consenso sobre la edad recomendada para adquirir un smartphone propio, aunque cada vez los expertos insisten en retrasarlo lo máximo posible12. Sin embargo, la edad media de adquisición de este dispositivo es menor de lo aceptable, como queda reflejado en nuestra muestra, en la que la media de edad del primer móvil (10,35 años) es similar a la de otros estudios, como el de Unicef13.
Son numerosos los peligros a los que se exponen los menores al navegar por la red. Gracias a las campañas que se realizan desde el ámbito educativo y sanitario, cada vez son más conocidos por los niños y sus tutores, que instalan controles parentales y supervisan la actividad de sus hijos por Internet. En nuestro estudio llama la atención que los que más lo hagan sean los padres con menor nivel académico. No podemos dar una explicación. Pero en otros estudios, como en el de Jiménez Morales14, ocurre al contrario.
Otros autores han documentado la relación del abuso del móvil con problemas de comportamiento, del sueño, obesidad y miopía15,16. Se están estudiando mucho sus repercusiones en la salud17 y en el rendimiento académico18. En nuestro trabajo solo se ha objetivado significación estadística con problemas visuales. Como limitación de ese resultado debemos decir que la prevalencia de los defectos de refracción aumenta proporcionalmente al aumento de edad de los niños, al igual que en nuestro estudio aumentan proporcionalmente las horas de uso del teléfono.
La edad de acceso que WhatsApp establece en sus términos de uso es de 16 años. Las de otras redes sociales como Instagram y TikTok es de 13 años. A pesar de esto, su uso está muy extendido en niños de menor edad, como vemos en la población encuestada.
Cada vez son más los autores que defienden que el uso problemático del móvil tiene características de conducta adictiva3.
De acuerdo con la definición de dependencia de Chóliz4, el PMPU representa una condición caracterizada por:
- Uso excesivo, tanto en términos de alto costo económico como en el número de llamadas y mensajes.
- Problemas interpersonales asociados con el uso excesivo.
- Interferencia con actividades académicas o de la vida diaria.
- Tolerancia, es decir, un aumento gradual en la cantidad de uso necesario para obtener el mismo nivel de satisfacción, así como la necesidad de sustituir dispositivos operativos con nuevos modelos que aparecen en el mercado.
- Síntomas de abstinencia, es decir, una necesidad urgente de usar un teléfono móvil después de que haya transcurrido un tiempo desde su último uso, así como alteraciones emocionales cuando se impida o dificulte su uso.
- Falta de control, es decir, incapacidad para detener el comportamiento adictivo.
En este trabajo hemos realizado el TDM abreviado de Choliz a los niños mayores de 11 años, en los que estaba validado19, observándose muchas respuestas positivas en ítems de los cuatro apartados en los que se divide el test, especialmente en el de falta de control. Ellos mismos eran conscientes de este uso problemático, ya que estas respuestas positivas se correlacionaban con el mayor número de horas de uso y con haber afirmado que creían que usaban el móvil más de lo que deberían.
CONCLUSIONES
Los hábitos de uso del teléfono móvil influyen de manera importante en la vida de los niños. Hemos comprobado que es el dispositivo que más utilizan para navegar por Internet.
La media de edad de adquisición del primer teléfono móvil propio es menor de la recomendada, en nuestro estudio es de 10,35 años. Las redes sociales se usan antes de la edad aconsejada por las plataformas digitales.
Su abuso puede generar conductas con rasgos de adicción, que hemos constatado en nuestro estudio. La percepción de dependencia al móvil aparece en edades tempranas.
Los pediatras necesitamos estar formados en el consumo de nuevas tecnologías para poder ayudar a las familias a tener un uso racional de este dispositivo. En nuestros controles de salud programados deberíamos incluir aspectos relativos a la salud digital, proporcionando herramientas que faciliten un uso adecuado de Internet y redes sociales.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este proyecto ha sido financiado con la Beca AEPap–FPS para la investigación en Pediatría de Atención Primaria 2022, que agradecemos enormemente.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del manuscrito publicado.
ABREVIATURAS
DT: desviación típica · FoMO: miedo a perderse algo · IMC: índice de masa corporal · PMPU: uso problemático del teléfono móvil · RRSS: redes sociales · TDM: test de dependencia al móvil.
BIBLIOGRAFÍA
- Fischer Grote l, Kothgassner OD, Felnhofer A. The impact of problematic smartphone use on children's and adolescents' quality of life: A systematic review. Acta Paediatr. 2021;110:1417-24.
- De Sola J, Talledo H, Rodríguez de Fonseca F, Rubio G. Prevalence of problematic cell phone use in an adult population in Spain as assessed by the Mobile Phone Problem Use Scale (MPPUS). PLoS One. 2017; 12(8): e0181184.
- Billieux J, Maurage P, López Fernández O, Kuss,DJ, Griffiths MD. Can Disordered Mobile Phone Use Be Considered a Behavioral Addiction? An Update on Current Evidence and a Comprehensive Model for Future Research. Curr. Addict. Rep. 2015;2:156-62.
- Chóliz M. Mobile phone addiction in adolescence: evaluation and prevention of mobile addiction in teenagers. LAP, Lambert Academic Publishing. 2010.
- Thapa K, Lama S, Pokharel R, Sigdel R, Rimal SP. Mobile phone dependence among undergraduate students of a medical college of Eastern Nepal: A Descriptive Cross-sectional Study. JNMA J Nepal Med Assoc. 2020;58:234-9.
- Alavi SS, Ghanizadeh M, Mohammadi MR, Jannatifard F, Salehi M, Farahani M, et al. Psychometric Properties of Mobile Phone Abuse (MPA): Exploratory and Confirmatory Factor Analysis in Student Mobile Users. Iran J Psychiatry. 2021 (2):187-97.
- Zhang J, Zhang X, Zhang K, Lu X, Yuan G, Yang H, et al. An updated of meta-analysis on the relationship between mobile phone addiction and sleep disorder. J Affect Disord. 2022;305:94-101.
- Dibben GO, Martin A, Shore CB, Johnstone A, McMellon C, Palmer V, et al. Adolescents' interactive electronic device use, sleep and mental health: a systematic review of prospective studies. J Sleep Res. 2023:e13899.
- Sohn S, Rees P, Wildridge B, Kalk NJ, Carter B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: A systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019;19:1-10.
- Mascheroni G, Ólafsson K. The mobile Internet: Access, use, opportunities and divides among European children. New Media & Society 2016;18:1657-79.
- Smahel D, Machackova H, Mascheroni G, Dedkova l, Staksrud E, Ólafsson K, et al. EU Kids Online 2020: Survey results from 19 countries. EU Kids Online. (2020) [en línea] [consultado el 05/09/2023]. Disponible en www.lse.ac.uk/media-and-communications/research/research-projects/eu-kids-online/eu-kids-online-2020
- Dienlin T, Johannes N. The impact of digital technology use on adolescent well-being. Dialogues Clin Neurosci. 2020;22:135-42.
- Andrade B, Guadix I, Rial A, Suárez F. Impacto de la tecnología en la adolescencia. Relaciones, riesgos y oportunidades. (2021). Madrid: UNICEF España [en línea] [consultado el 05/09/2023]. Disponible en www.unicef.es/publicacion/impacto-de-la-tecnologia-en-la-adolescencia
- Jiménez Morales M, Montaña M, Medina Bravo P. Childhood use of mobile devices: Influence of mothers’ socio-educational level. Rev Comunicar 2020 64 XXVIII.
- Álvarez Peregrina C, Sánchez Tena MÁ, Martínez Pérez C, Villa Collar C. The Relationship Between Screen and Outdoor Time With Rates of Myopia in Spanish Children. Front Public Health. 2020;8:560378.
- Wang J, Li M, Zhu D, Cao Y. Smartphone Overuse and Visual Impairment in Children and Young Adults: Systematic Review and Meta-Analysis. J Med Internet Res. 2020;22:e21923.
- Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9:e023191.
- Yadav MS, Kodi SM, Deol R. Impact of mobile phone dependence on behavior and academic performance of adolescents in selected schools of Uttarakhand, India. J Educ Health Promot. 2021;10:327.
- Cerutti R, Presaghi F, Spensieri V, Fontana A, Amendola S. Adaptation and Psychometric Analysis of the Test of Mobile Phone Dependence-Brief Version in Italian Adolescents. Int J Environ Res Public Health. 2021;18:2612.