

Care plans for children and adolescents with asthma in Spain, an analysis by autonomous community
Natalia Rivas Abraldesa, Águeda García Merinob
aPediatra. CS Mungia. Vizcaya. España.
bPediatra. CS Vallobín-Las Campas. Oviedo. Asturias. España.
Correspondence: N Rivas . E-mail: natalia_take@hotmail.com
Reference of this article: Rivas Abraldes N, García Merino A. Care plans for children and adolescents with asthma in Spain, an analysis by autonomous community. Rev Pediatr Aten Primaria. 2022;24:e11-e25.
Published in Internet: 12-04-2022 - Visits: 17581
Abstract
Introduction and objective: to describe the management of children and adolescents with asthma by primary care paediatricians (PCPs) in Spain.
Materials and methods: we conducted a cross-sectional descriptive study to assess the paediatric asthma care plans/guidelines of the autonomous communities (ACs) of Spain and Ceuta and Melilla, the inclusion of an asthma care pathway in the list of services covered by regional health systems and the documentation of asthma care in health records. The study was performed through an online survey of regional primary care paediatrics associations and by telephone for the autonomous cities of Ceuta and Melilla. We evaluated the identified documents using a reference protocol that we developed based on current clinical practice guidelines and included items pertaining to asthma diagnosis, treatment, and monitoring, available resources and care quality indicators, and assessed the differences in these documents.
Results: We found that 50% of ACs in Spain have care plans/guidelines for the management of asthma in children and adolescents. In 10 ACs, asthma care is included in the official list of health care services, and in 11, the electronic health records included a specific module devoted to asthma. Of the 9 asthma care documents identified in the survey, 3 were care plans and 6 were guidelines. The former achieved higher global scores in the comparison with the reference. Of all parameters under study, the only 2 fulfilled by all the plans/guidelines were the existence of a print asthma management document and the classification of the severity of asthma at diagnosis.
Conclusion: In Spain, there is significant variability in the management of asthma in children and adolescents, and not all ACs have established care plans or guidelines for it or integrated specific modules for documentation of asthma care in the electronic health records. To guarantee equity in the management of patients with asthma, it would be helpful for all regions to introduce an updated and comprehensive care plan.
Keywords
● Asthma ● Clinical practice guidelines ● Health resources ● National Health Programs ● Pediatrics ● Primary health careINTRODUCTION
Asthma is probably the most frequent chronic disease in children and adolescents in many parts of the world, including Spain, where it affects 1 in 10 children, with significant geographical variability. 1,2 It is also an important public health problem, as it decreases the quality of life of children and their families and generates substantial costs for health care systems and society.1-3
In economic terms, asthma is estimated to account for 1 to 2% of total health care expenditures. Most of it involves direct health care costs (60%), with the highest expenditures made at the primary care (PC) level. Most indirect costs (40%) are associated with the care of affected minors at home.1-3
For more than 20 years, consensus guidelines for the management of asthma, in adults and, more recently, in children, have been published and updated domestically and abroad. They are meant to provide uniform guidance based on high-quality evidence and relevant sources with recommendations for diagnosis and treatment, thereby allowing uniform delivery of high-quality care.1
However, management of asthma also requires adequate planning and organization through established programmes, including adaptation and coordination of the necessary human and material resources to implement guidelines and recommendations.4-6 The evaluation of national and regional asthma care programmes for children and adults in Europe has demonstrated that the implementation of integrated care pathways coordinating the activity of all the involved providers facilitates asthma control in the short and long terms, reduces direct and indirect costs associated with asthma and improves the quality of life of patients and families.4,7
In Spain, health care coverage for children is universal and services accessible, and primary care paediatricians (PCPs) are the main point of entry of children to the National Health System (NHS), with the management of a large part of chronic childhood diseases, such as asthma, being one of the responsibilities within their scope of practice. However, the decentralization of health care authority with transfer of administrative management to autonomous communities (ACs) have resulted in heterogeneous approaches in the prioritization of services offered by the public health system. While asthma care for children and adolescents continues to be covered nationwide by the PC level of the NHS under the Section of Child and Adolescent Services, the actual implementation of asthma care has varied significantly between regions, both in the development of care plans and in the inclusion of asthma care in the list of covered services,3,8,9 as well as in the documentation of this activity in electronic health records.
We conducted a study with the aim of describing the care delivered by PCPs to children and adolescents with asthma in the different autonomous communities in Spain and the autonomous cities of Ceuta and Melilla, in terms of the use of asthma care plans/guidelines, their inclusion in the list of covered services of the autonomous community or city (AC) and the documentation in electronic records of data related to asthma control and monitoring. In addition, in the case of ACs with a regional plan/guideline of their own, we analysed the criteria used in the diagnosis and treatment of asthma, the allocated material and human resources, the distribution and organization of resources in the followup of children and adolescents with asthma, the indicators used to assess the quality of asthma care and any implemented interventions.
MATERIAL AND METHODS
Design: we conducted a cross-sectional descriptive study to learn and assess the contents of care plans for management of asthma in children and adolescents in Spain in each AC (including the cities of Ceuta and Melilla), the inclusion of asthma care pathways in the services covered by regional health systems and the documentation of asthma care in electronic health records.
Protocol: we used the following methods to collect data on the asthma care plans in the autonomous communities and the autonomous cities of Ceuta and Melilla.
Literature review:
- Review of the scientific literature, including databases, restricted to publications in English or Spanish through year 2018, using search terms specific to the diagnosis, treatment and followup of asthma in the paediatric population.
- Official publications of the Spanish Ministry of Health, including the official state gazette (Boletín Oficial del Estado, BOE), and publications of the National Health Administration Institute (Instituto Nacional de Gestión Sanitaria, INGESA), an organization dependent on the Ministry of Health that manages public health services in the autonomous cities of Ceuta and Melilla, which are officially considered the 18th AC). Official publications of the different ACs and Ceuta and Melilla, including their official gazettes.
Website review:
- Ministry of Health, Consumption and Social Welfare of Spain: Section corresponding to health care.
- Departments involved in public health and health services in the ACs and the autonomous cities of Ceuta y Melilla.
- Respirar/To Breathe: webpage of the Airway Group of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics) (AEPap).
We conducted an online survey, sending a questionnaire using the mailing lists of the PC paediatrician associations at the AC level affiliated to the AEPap, which exist in every AC with the exception of Ceuta and Melilla, a region that we covered by contacting paediatricians in the area by telephone. The questionnaire had 3 items:
- Management of asthma in children/adolescents by PCPs in the AC according to a predefined care plan/guideline. If this was the case, the respondent was asked about the access to this pathway.
- Care of children and adolescents with asthma included in the health services covered at the AC level.
- Inclusion in the health information system or electronic health record database used to record clinical activity in paediatric clinics in the AC of a specific section in which to document the monitoring and followup of children and adolescents with asthma.
Explanation of dichotomous (yes/no) variables in the questionnaire:
- Asthma care plan: regulatory document developed in a consensus process by health care professionals that managed children and adolescents in the region and adapted to local social and health care characteristics. Its purpose is to guide clinicians in the diagnosis and management of asthma applying criteria endorsed by the global scientific community. It includes planning, logistics, an implementation strategy, allocation of resources and coordination between levels of care (PC and hospital-based care) and it is supported by the regional public health administration.3,7
- Clinical practice guideline (CPG) for the management of asthma: document developed by consensus by experts in the region to standardise diagnostic and therapeutic interventions for asthma based on current scientific knowledge and high-quality evidence and endorsed by the regional public health administration.3,7
Both care plans and guidelines are meant to improve the management of asthma, reduce variability in care delivery between health professionals and have a positive impact on the course of disease, so for the sake of convenience we considered them a single variable in our analysis of the current situation.3
- Definition of the list of services (LS) at the PC level covered by the NHS: set of health care services offered to meet the needs and demand of the population, established based on scientific and technical criteria and public health policy. They are interventions implemented by PC professionals with the aim of managing or preventing a health problem or satisfying a demand in health care and must meet predefined certification criteria. The LS is a tool that is dynamic and flexible tool in both time and geographical setting (AC).9
- Specific asthma module: a distinct form or section in the electronic health records of the AC use to document interventions performed in the monitoring and management of patients with asthma, such as the classification of disease, prescribed treatments, diagnostic tests, educational interventions or scheduled checkups.10
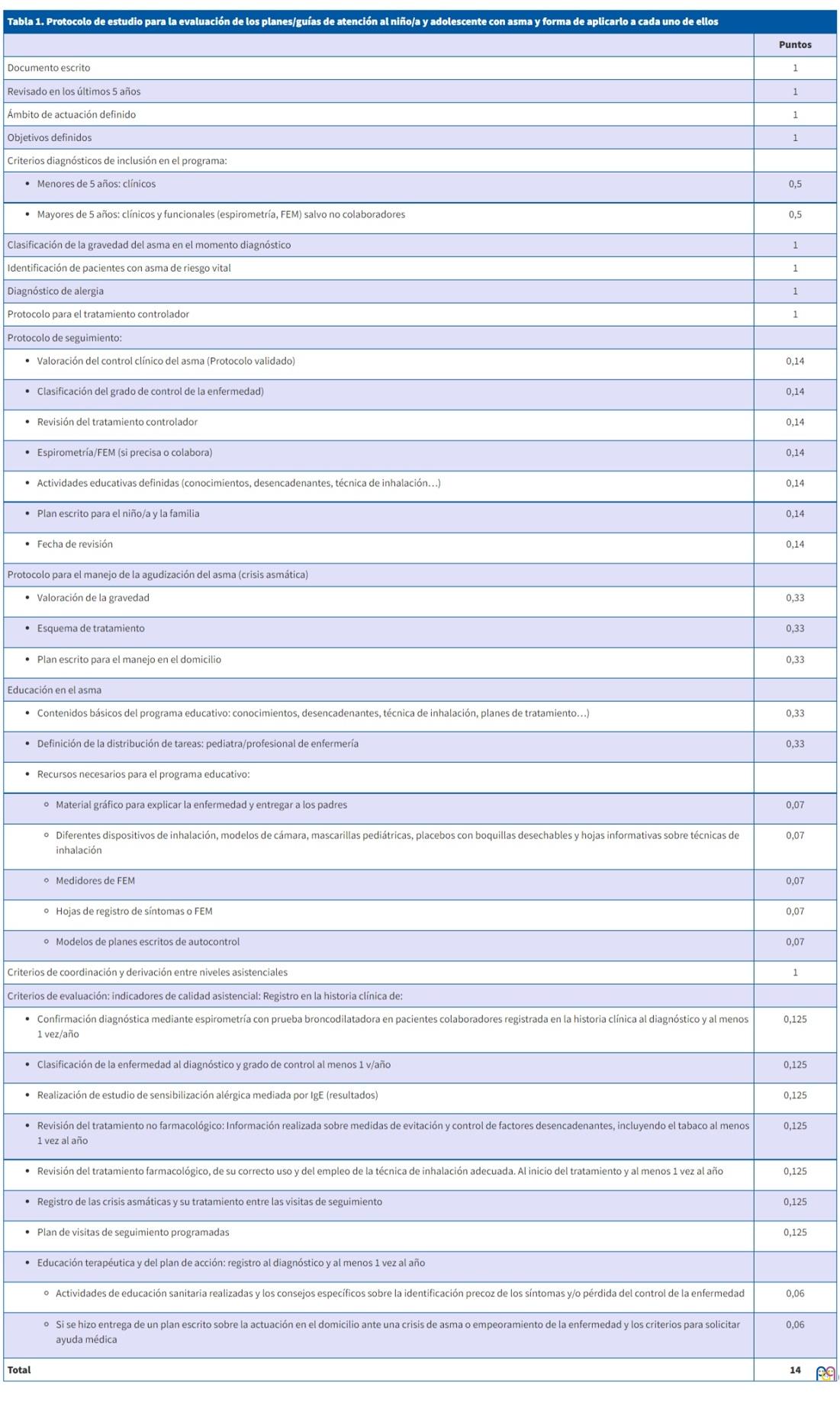
Intervention: we performed a detailed analysis of the contents of asthma care plans in different ACs using as reference a predefined protocol that comprised 14 items and 27 subitems regarding diagnostic and treatment criteria, available resources, the organization and distribution of tasks between professionals, quality indicators to assess delivered care and updates to the care plan/guideline (Table 1). We established this protocol based on the most recent CPGs, the recommendations published by Airway Group of the AEPap, the documents detailing the primary care services covered by the NHS and the health care quality targets recommended for the management of asthma at the PC level in the paediatric population.5,6,9,11-16
| Table 1. Reference protocol for assessment of care plans/guidelines for management of asthma in children and adolescence and scoring scheme | |
|---|---|
| Points | |
| Written document | 1 |
| Updated in past 5 years | 1 |
| Defined scope | 1 |
| Defined targets | 1 |
| Diagnostic criteria for inclusion in the care pathway: | |
|
0.5 |
|
0.5 |
| Classification of asthma severity at the time of diagnosis | 1 |
| Identification of patients with life-threatening asthma | 1 |
| Allergy diagnosis | 1 |
| Treatment protocol for asthma control | 1 |
| Protocol for patient followup: | |
|
0.14 |
|
0.14 |
|
0.14 |
|
0.14 |
|
0.14 |
|
0.14 |
|
0.14 |
| Protocol for management of asthma exacerbations (attacks) | |
|
0.33 |
|
0.33 |
|
0.33 |
| Asthma education | |
|
0.33 |
|
0.33 |
|
|
|
0.07 |
|
0.07 |
|
0.07 |
|
0.07 |
|
0.07 |
| Criteria regarding continuity of care and referrals between care levels | 1 |
| Evaluation criteria: quality indicators: Documentation in health record of: | |
|
0.125 |
|
0.125 |
|
0.125 |
|
0.125 |
|
0.125 |
|
0.125 |
|
0.125 |
|
|
|
0.06 |
|
0.06 |
| Total | 14 |
Statistical analysis: first, we performed a descriptive analysis of the 3 variables contemplated at the outset: existence of an asthma care plan/management guideline, inclusion of the care plan/guideline in the services covered by the regional health system, and presence in the electronic health records of a distinct module to document asthma care, in addition to the distribution of these variables by AC.
Then, we analysed the degree of variation of care plan contents relative to the established protocol as well as variability between ACs. To do so, we assigned 1 point to each item included in the reviewed document. If an item had subitems, we assigned each subitem a proportional value so that the total would add to 1. We expressed the result as the percentage of points obtained of the total possible score of 14 (Table 1).
We also analysed each of the 14 items separately to determine the percentage of adherence to each of them.
RESULTS
All PCP associations affiliated to the AEPap (one per AC, total of 17) responded to the survey, and we obtained responses for the autonomous cities of Ceuta and Melilla separately. The paediatricians surveyed for Ceuta and Melilla answered no to all 3 items, so for the purpose of statistical analysis, and taking into account that both are overseen by the INGESA, we treated them as a single AC, so that the analysis for all of Spain included a total of 18 ACs.
The responses to the first item showed that 9 ACs (50%) had established plans or guidelines for the management of asthma in the paediatric population, which was consistent with the results of a search of the official webpages and publications of the Spanish Ministry of Health and the regional Departments of Health; 3 (33.3%) were considered care plans for asthma in children/adolescents (Andalusia, Asturias and Balearic Islands) and 6 (66.7%) paediatric asthma guidelines (Aragon, Cantabria, Castilla y Leon, Catalonia, Basque Country and Madrid). Respondents in the other 9 ACs (50%) reported that there was no official document at the regional level for the management of asthma (Canary Islands, Castilla-La Mancha, Valencian Community, Extremadura, Galicia, La Rioja, Murcia, Navarre and INGESA [Ceuta and Melilla]).
When it came to the item regarding the inclusion of an asthma care pathway among the services covered by the PC system of the AC, 10 ACs (55.6%) turned out to have it in the LS: Andalusia, Aragon, Asturias, Cantabria, Castilla y Leon, Galicia, Madrid, Murcia, Navarre and Basque Country, while it was not included in the LS of the other 8 ACs (44.4%).
In the third item, concerning the presence of a specific module for documentation of asthma care in paediatric patients in the electronic health record interface, respondents from 11 ACs reported that it was available (61.1%) while it was not available in 7 ACs (38.9%): Andalusia, Castilla-La Mancha, Canary Islands, Valencian Community, Galicia, Extremadura and INGESA.
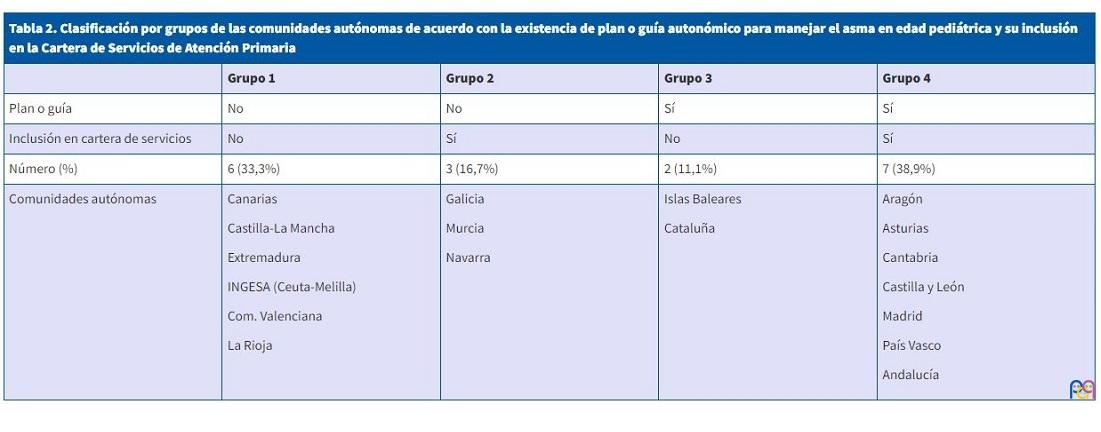
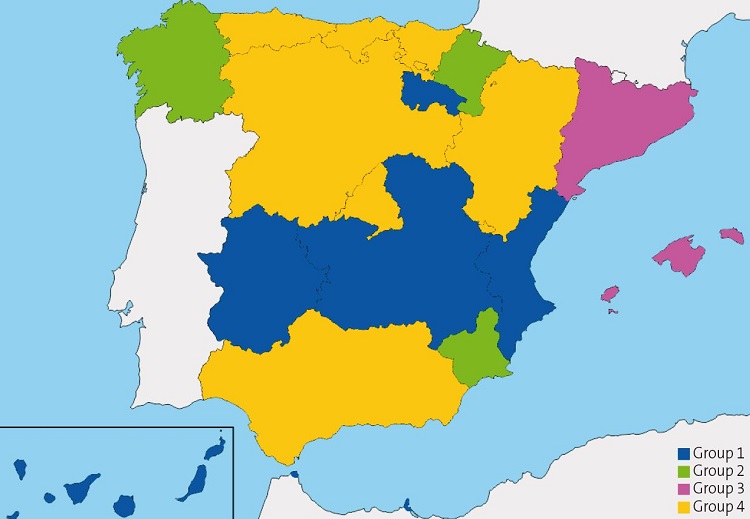
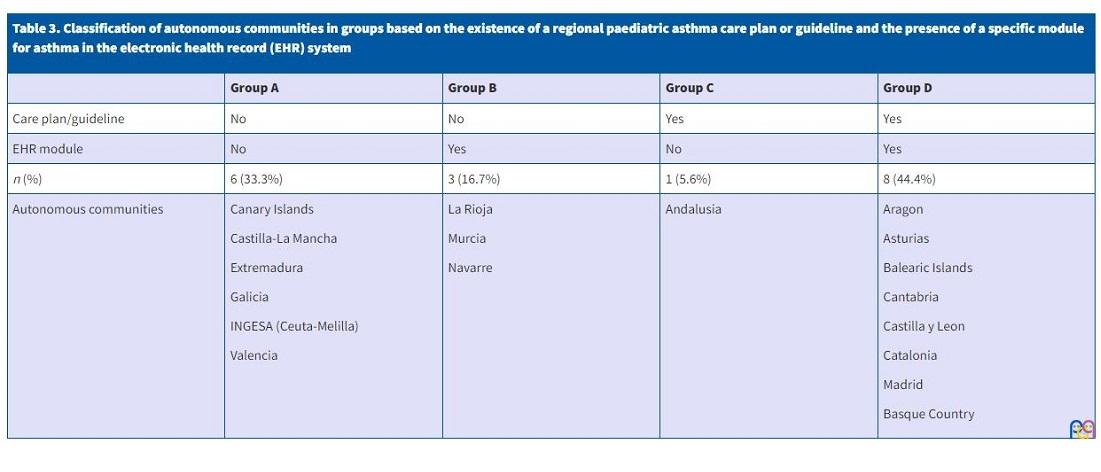
The distribution of the presence of a paediatric asthma care plan/guideline by AC and the inclusion of the asthma care pathway in the PC LS allowed classification of ACs in 4 groups (Table 2, Fig. 1). We used the same approach for the distribution for the variables concerning the presence of a care plan/guideline and the availability of a specific module in the health records, which yielded another 4 groups of ACs (Table 3, Fig.2). Although there were some differences, the ACs included in each of the 4 groups in these 2 distributions were almost the same.
| Table 2. Classification of autonomous communities in groups based on the existence of a regional paediatric asthma care plan and its inclusion in the list of services covered by the primary care system | ||||
|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | Group 4 | |
| Care plan/guideline | No | No | Yes | Yes |
| Inclusion in list of covered services | No | Yes | No | Yes |
| n (%) | 6 (33.3%) | 3 (16.7%) | 2 (11.1%) | 7 (38.9%) |
| Autonomous Communities |
Canary Islands Castilla-La Mancha Extremadura INGESA (Ceuta-Melilla) Valencia La Rioja |
Galicia Murcia Navarre |
Balearic Islands Catalonia |
Aragon Asturias Cantabria Castilla y Leon Madrid Basque Country Andalusia |
| Figure 1. Graphic representation of the 4 groups of autonomous communities based on the existence of a regional paediatric asthma care plan/guideline and its inclusion in the list of services covered by the primary care system |
|---|
 |

|
Table 3. Classification of autonomous communities in groups based on the existence of a regional paediatric asthma care plan or guideline and the presence of a specific module for asthma in the electronic health record (EHR) system |
||||
|---|---|---|---|---|
| Group A | Group B | Group C | Group D | |
| Care plan/guideline | No | No | Yes | Yes |
| EHR module | No | Yes | No | Yes |
| n (%) | 6 (33.3%) | 3 (16.7%) | 1 (5.6%) | 8 (44.4%) |
| Autonomous communities |
Canary Islands Castilla-La Mancha Extremadura Galicia INGESA (Ceuta-Melilla) Valencia |
La Rioja Murcia Navarre |
Andalusia |
Aragon Asturias Balearic Islands Cantabria Castilla y Leon Catalonia Madrid Basque Country |
| Figure 2. Graphic representation of the 4 groups of autonomous communities based on the existence of a regional paediatric asthma care plan or guideline and the presence of a specific module for asthma in the electronic health records system. |
|---|
 |
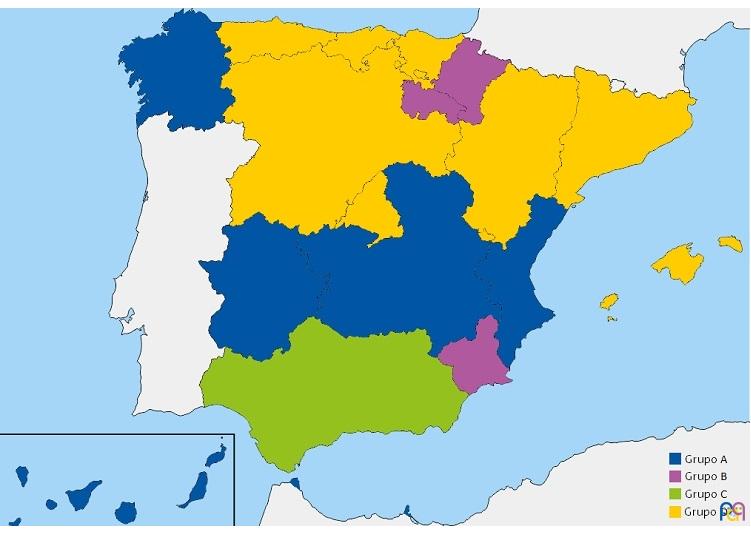
The analysis of the presence of all 3 variables revealed that 6 ACs (33.3%; Asturias, Castilla y Leon, Cantabria, Aragon, Basque Country and Madrid) had a paediatric asthma care plan/guideline, with the asthma care pathway included in the LS, and a specific module in the electronic health records devoted to asthma care. On the other hand, 5 ACs (27.8%; Castilla-La Mancha, Canary Islands, Valencian Community, Extremadura, Ceuta and Melilla) did not have any of these measures in place. In the remaining ACs, the distribution of the 3 variables was heterogeneous (Tables 2 and 3) (Figs. 1 and 2).
Table 4 presents the results of the comparison of the reference protocol (Table 1) to the 9 regional care plans/guidelines established in Spain for management of paediatric asthma at the AC level, expressed as the total points obtained by each AC and the percentage over the total possible points.
| Table 4. Results obtained in the comparison of the reference protocol to the regional care plans for management of asthma in the paediatric age group in the autonomous communities that had them | ||
|---|---|---|
| Autonomous community (plan/guideline) | Total score | Score as % |
| Andalusia (plan) | 13.0 | 92.8% |
| Principality of Asturias (plan) | 12.7 | 90.5% |
| Castilla y Leon (guideline) | 12.5 | 89.5% |
| Balearic Islands (plan) | 11.5 | 81.8% |
| Cantabria (guideline) | 10.7 | 76.6% |
| Basque Country (guideline) | 10.4 | 73.9% |
| Aragon (guideline) | 9.7 | 69.3% |
| Catalonia (guideline) | 9.6 | 68.6% |
| Madrid (guideline) | 5.9 | 42.1% |
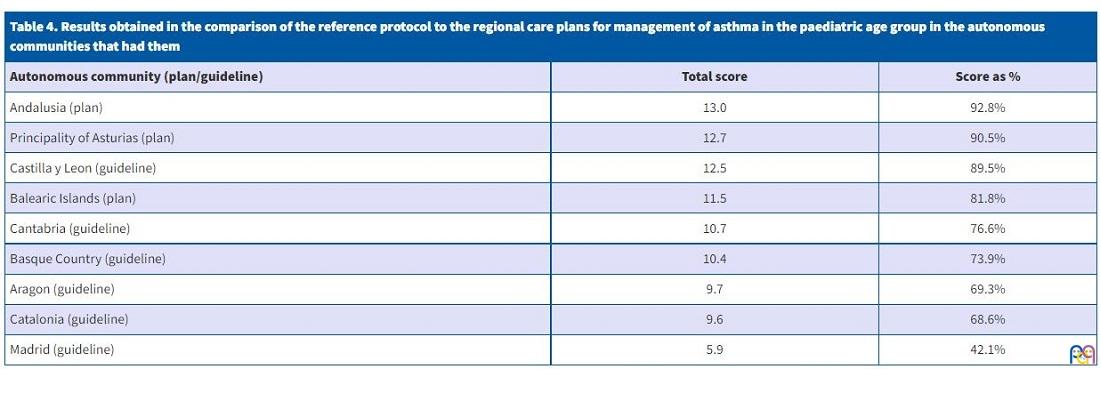
Andalusia has 2 established asthma care plans,17,18 one from 2003 with an exclusively paediatric scope and a subsequent revision from 2012 that merged the paediatric and adult care plans. We considered the 2003 plan the foundation on which updates were made in 2012. With a score of 92.8%, it fulfilled every reference item with the exception of having been updated in the past 5 years.
In the Principality of Asturias, a paediatric asthma care plan was established in 2001 and updated in n 2011.19 With a score of 90.5%, it fulfilled every item with the exception of having been updated in the past 5 years and allocating specific tasks to different health care professionals.
The guideline established in Castilla y Leon in 200420 received a score of 89.5% on account of not having been reviewed in the past 5 years, failing to provide a classification of asthma control, failing to provide a form to document symptoms or peak flow measurements and absence of some quality indicators, such as documentation of asthma exacerbations in the health record and having an established calendar for scheduled follow-up visits.
The care plan established in the Balearic Islands in 200721 received a score of 81.8%, for not having been updated in the past 5 years, like the others, failure to identify patients with life-threatening asthma (LTA), a lack of a validated protocol to assess asthma control and failure to call for documentation of educational interventions.
The 2006 guideline of Cantabria22 received a score of 76.6%, failure to fulfil the criteria of having been reviewed in the past 5 years, having defined targets, adequate coordination between levels of care, a validated protocol to assess asthma control and documentation of educational interventions.
The Basque Country23 has a comprehensive guideline for management of asthma in children, adolescents and adults with a subsequent revision of the recommendations for the paediatric population published in 2015. As we did in Andalusia and Asturias, we considered the 2005 the main guideline later supplemented with the 2015 update. This guideline received a score of 73.9% and did not meet the criteria of having a defined scope of application, defining diagnostic criteria, identifying patients with LTA, having a protocol to assess asthma control, in addition to missing 50% of the quality indicators under consideration.
The guideline of Aragon24 of 2004 had a score of 69.3%, as it was not updated in the past 5 years, did not have defined targets, did not identify patients with LTA, did not have a protocol to assess asthma control, did not specify the need to perform lung function tests for followup, did not have templates for asthma action and was missing some quality indicators, such as the documentation of asthma exacerbation or the provision of written information.
The Catalonia guideline25 of 2008 received a score of 68.6%, as it was not revised in the past 5 years, had no defined scope or targets, did not consider the degree of asthma control or performance of lung function tests for followup, did not allocate specific tasks to paediatricians/nurses, did not specify the educational resources available and was missing more than 50% of the quality indicators.
Lastly, we considered the documents included in the official LS covered by the PC system in Madrid under the title Atención a niños con asma activa (Management of children with active asthma), last updated in 2014,26 a guideline. It received a score of 42.1% of the total possible points. It did not have defined targets, did not identify patients with LTA, did not specify the need to do allergy testing, did not include treatment protocols, had not been updated in the past 5 years and did not establish criteria for continuity of care between care level. On the other hand, the followup protocol was quite adequate and it scored well in the recording of quality indicators.
Table 5 presents the degree of adherence (%) with the reference items under study in the analysed care plans/guidelines.
| Table 5. Percentage of adherence with analysed elements of the care plans for management of asthma in the paediatric age group established at the autonomous community level in Spain | ||
|---|---|---|
| Item | Yes (%) | No (%) |
| Reviewed in the past 5 years | 1 (11.1%) | 8 (88.9%) |
| Criteria for evaluation of care quality indicators (in full) | 2 (22.2%) | 7 (77.8%) |
| Follow-up protocol (in full) | 3 (33.3%) | 6 (66.7%) |
| Defined targets | 5 (55.6%) | 4 (44.4%) |
| Identification of children with life-threatening asthma | 5 (55.6%) | 4 (44.4%) |
| Asthma education (in full) | 5 (55.6%) | 4 (44.4%) |
| Defined scope | 7 (77.8%) | 2 (22.2%) |
| Criteria for continuity of care and referral between levels of care | 7 (77.8%) | 2 (22.2%) |
| Diagnostic criteria for entry to pathway (in full) | 8 (88.9%) | 1 (11.1%) |
| Allergy diagnosis | 8 (88.9%) | 1 (11.1%) |
| Treatment protocol for asthma control | 8 (88.9%) | 1 (11.1%) |
| Protocol for management of asthma exacerbations (in full) | 8 (88.9%) | 1 (11.1%) |
| Written document | 9 (100%) | - |
| Classification of asthma severity at the time of diagnosis | 9 (100%) | - |
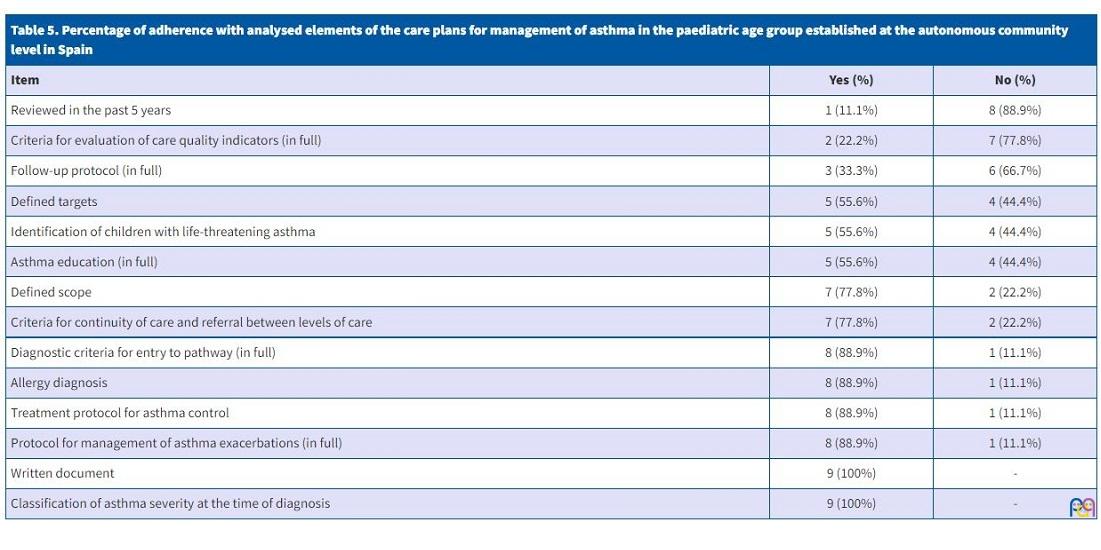
The criteria that had been met least frequently were having been updated in the past 5 years, which was only met by 1 of the 9 plans (11.1%), and the quality indicators, which were only met in full by 2 (22.2%), although another 4 scored above 0.75 on that item. When it came to the quality indicators, the subitems that were met least frequently were the documentation of performed interventions (4), documentation of asthma exacerbations (4), use of spirometry at diagnosis and every year thereafter (3) and the annual monitoring of asthma control (3).
The criteria used to rate the followup protocol item were only met fully by 33.3% of the analysed documents. Most were missing a protocol for assessment of asthma control (55.6%). The other subitems were met by all documents except for 2 that did not include annual performance of spirometry/peak flow measurement or called for providing examples of action plans to families.
Only 55.6% (5) plans/guidelines established criteria for the identification of children with LTA and had defined targets.
When it came to the item on asthma education, while criteria were only met fully by 55.6% (5) documents, another guideline had a score greater than 0.9.
Seven documents (77.8%) defined the scope of application of the plan/guideline and criteria for coordination of care and referral between levels of care.
Eight documents (88.9%) presented clear diagnostic criteria for entry in the asthma care pathway, and all documents but the Madrid guideline mentioned the need of allergy testing as part of the care plan and included protocols for asthma control medication and management of exacerbations.
All the plans/guidelines called for provision of information in print and called for assessment of asthma severity at diagnosis.
DISCUSSION
Asthma is possibly the most frequent chronic disease in the paediatric population of Spain. It is not only important in terms of its prevalence, but also due to its impact on the quality of life of children and families, the national economy, health care expenditure and the use of health care resources.1 The goals of asthma control are to decrease its impact on the population, which requires organization of care delivery with a rational use of human, material and health care resources fitting patient needs and adequate training and involvement of the health professionals that manage these patients.4,11,12
On the other hand, the main asthma CPGs contemplate the need to organise care delivery, but do not address every key element required to structure care, possibly because they are applicable to multiple care settings and cannot touch on the particularities of each health system or define a single model for paediatric asthma care.
In Spain, given the characteristics of the NHS, children and adolescents with asthma enter the health system through PC paediatricians, who are therefore the health professionals best positioned to diagnose and followup these patients. Thus, since the early 1990s different models have been proposed to organise asthma care from the PC setting, involving PC paediatricians and nurses,5,6 with their scope expanding over time to the eventual development of integrated care pathways at the AC level. However, as demonstrated by our findings, the implementation of these care plans varies significantly between ACs, so that while paediatric asthma care is included in the services covered by the public primary care system at the national level,8 the transfer of administrative powers to the different ACs has led to the implementation of different approaches in the services offered by each administration at the regional level.9
Although integrated care plans with ongoing followup and regular monitoring of patients with asthma are clearly cost-effective through the reduction of emergency department visits and hospital admissions and the improvement of the quality of life of patients and their families,1,7 only 50% of the 18 ACs in Spain had a regional care plan or guideline for the management of asthma in the paediatric population. In addition, ACs that have established care pathways allocate more human and material resources for asthma care than those that do not.3 However, there are studies that show that the existence of care plans does not guarantee their knowledge or implementation by the health providers involved.3,15,16 In this case, all the associations in ACs that had asthma care plans were aware of them and were able to provide the document for the study, but since we did not do a survey of their members, we were not able to determine the actual dissemination of the plan among PC paediatricians. Given this, to facilitate the implementation and adherence to care plans, it is not only important to develop a document with recommendations, but also to plan the training of health professionals and allocate human and material resources. It is also essential to establish quality indicators with which to justify the inclusion of the care pathway in the services covered by the PC system of the region and that allow periodic evaluation of the programme.3,9
In most cases, the existence of an asthma care plan or guideline in an AC was associated with the inclusion of this activity in the list of covered services and of a means to document this activity in the electronic health records system. Thus, of the 9 ACs with paediatric asthma care plans, 7 had this activity included in the official PC service list, which reflects the activity developed by PC paediatricians.9 Only 3 of the ACs that did not have a care plan/guideline included this activity in the regional health system LS, which means that it is possible that asthma care in these regions is delivered in adherence with national or international CPGs,11,12 an approach that would partly fulfil the quality criteria established by the NHS of Spain.9
With the exception of Andalusia, the ACs with care plans for management of paediatric asthma (8) also had specific software tools for documentation of asthma care at the PC level integrated in in the electronic health records system. These electronic records facilitate the followup of paediatric patients with asthma, delivery of health education, with the option of providing advice and directions to the patient and family at each visit, and the periodic review and evaluation of established goals. In contrast, only 3 ACs that did not have asthma care plans had a specific software module to document asthma care in paediatric patients integrated in the health record system.
Royal Decree 1030/2006, of 15 September established the list of services covered nationwide by the NHS; both this decree and subsequent revisions8-10 included the detection and followup of chronic diseases in children, including asthma, is included in the basic list of services covered by the PC system, and although the benefits of regional asthma care plans for children and adolescents at the AC level are well established, 50% of ACs do not have a regional consensus-based protocol for health providers involved in paediatric asthma care. While in some of these ACs there are care plans for paediatric asthma of a lesser scope, such as the Protocol for the Management of Asthma of the Complejo Hospitalario Insular Materno-Infantil of Gran Canaria,27 we did not evaluate them in this study because they did not apply to the entire AC.
Of the 9 identified documents included in the analysis, we considered 3 (33.3%) to be care plans while the remaining 6 (66.7%) conformed more to the structure of a guideline. We assigned these categories taking into account that a care plan for a chronic disease, in this case asthma, differs from a guideline in its comprehensive approach to the disease, starting from an overview of the status quo and available resources that provides the foundation to define clear health care targets and quality indicators to allow their evaluation. A care plan includes protocols, all pertinent documents and a plan for implementation. In contrast, a guideline describes the optimal management of asthma based on the most recent and highest-quality scientific evidence, but does not necessary consider available resources or draw a plan for its dissemination and implementation.3,7
Based on the results of assessing the appropriateness of paediatric asthma management documents in each AC, we found that care plans, which existed in Andalusia17,18, Asturias19 and Balearic Islands,21 scored higher overall compared to guidelines and occupied the top spots in the ranking, which indicated greater adherence to published CPGs and recommendations.5,11-14 This superiority may be partly explained by the use in the assessment of a reference protocol developed to evaluate plans that included items (such as the definition of the scope of application, target outcomes and quality indicators) that are contemplated in care plans by definition but not necessarily addressed in guidelines. In addition to achieving higher scores relative to the reference protocol, the evidence to date suggests that the implementation of care plans achieves better outcomes compared to guidelines,7 and a study that assessed the quality of clinical practice guidelines found that adherence to them was generally poor.28 In general, in the process of developing care plans, efforts are made to produce documents that are easy to use for health professionals, facilitating their dissemination and acceptance,5 an aspect that we did not take into account in the reference protocol but that is frequently not prioritised in the development of guidelines; for instance, the guideline of the Basque Country23 was lengthy and organised in a manner that was neither intuitive nor practical, which poses a barrier to its dissemination and its implementation by health care professionals.
The paediatric asthma care plans that scored highest were those of Andalusia and Asturias,17-19 which were very thorough, although it is worth noting that neither had been updated in the past 5 years. On the other hand, they have the benefit of the experience of 15 years since their initial introduction and have served as a model for subsequent care plans and guidelines.20-22,24 A positive aspect worth highlighting is the brief format and high readability of the 2011 update of the Asturias care plan,19 following the proposals of the Airway Group of theAEPap.5 We also ought to note the how clearly organised and well-structured the followup of patients, the allocation of tasks to different professionals and health literacy sections were in the third care plan we analysed, which belonged to Balearic Islands.21
Of the reviewed guidelines, the one from Castilla y Leon20 had an overall score close to those achieved by the care plans of Asturias and Andalusia, and even higher than the score of the care plan of Balearic Islands, as it was thorough, comprehensive, readable and easy to use. Although it did not include forms for the documentation of symptoms or a classification of asthma control and was missing documentation of some health care quality indicators, this was probably a consequence of it being conceived as a guideline rather than an actual care plan. On the other extreme, with the lowest score, was the guideline of the Community of Madrid,26 but it is important to take into account that although we classified it as a guideline, in reality it is a “document for the management of children with active asthma”, developed for the purpose of standardising diagnostic and therapeutic interventions in the management of paediatric asthma in the region included in the list of services of the PC system, which is why it did not get points for many of the items used in the evaluation.
When it came to the individual analysis of each parameter included in the reference protocol, we ought to highlight that of the 9 documents included in the analysis, the only one that had been updated in the past 5 years was the guideline of the Basque Country.23 While the Global Initiative for Asthma (GINA) guideline11 and the Spanish Guideline for Asthma Management (GEMA)12 are updated yearly, the British guideline,29 to put an example, is updated every 2 to 3 years. We did not find any reference to the time interval that would be appropriate to revise and update care plans in the reviewed literature, but it seems reasonable that frequent updating based on the main international guidelines would be appropriate, although it may not be necessary to revise the entire care plan in every single update.
Items that had subitems were also fulfilled completely by fewer plans, as more criteria had to be met to achieve a full point, which complicated the interpretation of the results. This is the case of quality indicators, as only 2 plans achieved a full point for including the 8 indicators considered in the reference protocol, although another 4 documents covered 75% of the indicators. In addition, this low frequency of fulfilment may be partly due to the fact that most of the documents analysed were not care plans but guidelines, a type of document that does not generally contemplate quality indicators.3,7 Another aspect that may contribute to explaining this finding is that until its version 4.2 from 2017, the GEMA guideline did not address care quality criteria,12 and most of the documents in the analysis were published before this year. At present, efforts are underway to develop quality indicators which, once validated, could help measure the correct implementation of care plans and the associated health outcomes. Thus, several authors have been proposing good clinical practice guidelines, usually based on expert consensus,13,14 some of which were included in the reference protocol used in the analysis. The application of these quality indicators in regions with official care plans could help measure their impact on, for instance, the quality of life of patients and families or the consumption of resources resulting from PC and emergency visits and hospital admissions, and to assess the adherence of health care providers and identify opportunities for improvement.3,14
The specification of a followup protocol was another of the aspects fulfilled least frequently, and the criteria were only met in full by 3 documents. Most plans fail to fulfil this aspect by not including a validated protocol for assessment of asthma control (55.6%), an element that has been recommended for years by the GINA11 and GEMA12 guidelines and that should be included in asthma care plans within the health records.
Only 5 of the 9 documents included criteria to identify patients with LTA. The main CPGs11,12,29 recommend assessment of risk factors for LTA, since, while LTA occurs in only a minority of patients (the scarce epidemiological data in Spain suggests that life-threatening episodes amount to 3% of all asthma exacerbations30), these patients are at greater risk of having exacerbations with a sudden onset and fatal outcome. The identification, close monitoring and education on exacerbation prevention and asthma self-management of these patients are associated with improved outcomes, so asthma care plans should include a section on how to identify these patients.30
Another item, fulfilled by 5 of the 9 documents, was the definition of specific care goals, an aspect that may also be influenced by the difference between care plans and guidelines.3,7 Thus, all care plans fulfilled this parameter, compared to only 2 of the 6 guidelines.
Asthma education was another one of the items with several subitems; 5 documents fulfilled it completely and another 2 scored more than 90% on this item, but all documents devoted a substantial section to health literacy, agreeing on the stance that this is a cornerstone of asthma management.20,21
Other parameters, such as assessing asthma severity at diagnosis, having a print document, providing clear criteria for entry in the care pathway, defining the scope of application, establishing criteria for coordination of care and referrals between care levels or protocols for asthma control medication and treatment of exacerbations, were fulfilled by most documents, probably because these were included in the Paediatric Asthma Care Pathway within the section on Paediatric Care of the list of services covered by the PC system of the Ministry of Health of Spain as criteria that must be met to receive accreditation for this care.9
In the past 20 years, ACs in Spain have been publishing regional plans for the management of asthma in the paediatric age group. The few studies that have analysed the impact of their implementation5 have evinced ACs with a paediatric asthma care plan/guideline allocate more resources to asthma care and that a higher proportion of children with asthma in these regions are followed up in PC paediatric clinics, although we do not know the impact of the provided care on the quality of patients and their families or in the consumption of health care resources, or whether there are differences in outcomes between ACs with an established care pathway, an official guideline or neither.3 The experience with the implementation of regional or national asthma care plans described in other countries, such as Finland, Poland, Canada or Australia, clearly demonstrates that these programmes are cost-effective for patients and society overall. In addition, regional/national plans achieve better outcomes compared to conventional asthma care guidelines.7 Thus, the recently published “worldwide charter for all children with asthma”31 proposes a roadmap to improve the quality of life of these patients in which asthma monitoring and management in children is carried out in the framework of a care pathway adapted to local/regional characteristics, rooted in the primary level of care, which requires active involvement of governments, institutions and health care workers to achieve improvements in health care outcomes.
CONCLUSION
Our study evinced that asthma care in the paediatric age group varies significantly within Spain and allowed us to generate an AC map based on the use of specific asthma care plans. To pursue equity in the care delivered to all children and adolescents with the disease, it would be beneficial for all regions to implement an updated integrated care plan adapted to the particular characteristics of each AC, based on the recommendation of the CPGs of highest quality, including every health care professional involved in the management of children and adolescents with asthma and incorporating validated and standardised quality indicators to allow evaluation of the appropriateness of existing care plans, assessment and comparison of care outcomes and identification of opportunities for improvement.
CONFLICTS OF INTEREST
This article has been produced in the framework of the final master’s thesis for the Master of Primary Care Paediatrics programme of the Universidad Complutense de Madrid.
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
ABBREVIATIONS
AC: autonomous community · AEPap: Asociación Española de Pediatría de Atención Primaria · CPG: clinical practice guideline · LS: list of services · LTA: life-threatening asthma · NHS: National Health System · PAP: primary care paediatrician · PC: Primary Care.
REFERENCES
- García Merino A, Praena Crespo M. El impacto del asma en la infancia y la adolescencia. En: AEPap (ed.). Curso de actualización en Pediatría 2013. Madrid: Exlibris Ediciones; 2013. pp. 257-65.
- Blasco Bravo AJ, Pérez Yarza EG, Lázaro y de Mercado P, Bonillo Perales A, Díaz Vázquez CA, Moreno Galdó A. Coste del asma en Pediatría en España: un modelo de evaluación de costes basado en la prevalencia. An Pediatr (Barc). 2011;74:145-53.
- Úbeda Sansano MI, Cano Garcinuño A, Rueda Esteban S, Praena Crespo M. Resources to handle childhood asthma in Spain: The role of plans and guides and the participation of nurses. Allergol Immunopathol. 2018;46:361-9.
- Sordo MA, Alonso JC, Del Ejido J, Díaz CA, Alonso LM, García MT. Evaluación de las actividades y de la efectividad de un programa del niño asmático desarrollado en Atención Primaria. Aten Primaria. 1997;19:199-206.
- Implantación en España de los programas de atención al niño con asma. Situación actual y propuestas del Grupo de Vías Respiratorias. In: Grupo de Vías Respiratorias de la AEPap (GVR-AEPap) [online] [accessed 07/01/2022]. Available at www.respirar.org/index.php/grupo-vias-respiratorias/grupo-vias-respiratorias
- Díaz Vázquez CA. Mesa Redonda. Asma ¿En qué situación estamos? Organización de la asistencia sanitaria a los niños con asma. Bol Pediatr. 2003;43:191-200.
- Selroos O, Kupczyk M, Kuna P, Łacwik P, Bousquet J, Brennan D, et al. National and regional asthma programmes in Europe. Eur Respir Rev. 2015;24:474-83.
- Real Decreto 1030/2006, de 15 de septiembre, por el que se establece la cartera de servicios comunes del Sistema Nacional de Salud y el procedimiento para su actualización. Ministerio de Sanidad y Consumo. BOE-A-2006-16212. In: Boletín Oficial del Estado [online] [accessed 07/01/2022]. Available at www.boe.es/eli/es/rd/2006/09/15/1030/con
- Instituto de Información Sanitaria – Sistema de Información de Atención Primaria (SIAP). Cartera de servicios de Atención Primaria. Desarrollo, organización, usos y contenido. In: Sistema Nacional de Salud [online] [accessed 07/01/2022]. Available at www.mscbs.gob.es/estadEstudios/estadisticas/docs/siap/Cartera_de_Servicios_de_Atencion_Primaria_2010.pdf
- Ministerio de Sanidad, Servicios Sociales e Igualdad, Instituto de Información Sanitaria - Subcomisión de Sistemas de Información del NHS. Oferta de Servicios en Atención Primaria. Servicios asistenciales, procedimientos y acceso a pruebas diagnósticas. In: Ministerio de Sanidad, Servicios Sociales e Igualdad [online] [accessed 07/01/2022]. Available at www.mscbs.gob.es/organizacion/sns/planCalidadNHS/pdf/equidad/informeAnual2008/annualReportNHS2008ING.pdf
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention [Internet]; Updated 2020 [online] [accessed 07/05/2020]. Available at https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report-final-wms.pdf
- Grupo de trabajo de la Guía Española para el Manejo del Asma. In: GEMA 5.0 2020 [online] [accessed 07/01/2022]. Available at www.gemasma.com
- Quirce S, Delgado J, Entrenas LM, Grande M, Llorente C, López Viña A, et al. Quality Indicators of Asthma Care Derived From the Spanish Guidelines for Asthma Management (GEMA 4.0): A Multidisciplinary Team Report. J Investig Allergol Clin Immunol. 2017;27:69-73.
- Ruiz Canela Cáceres J, Aquino Linares N, Sánchez Díaz JM, García Gestoso ML, de Jaime Revuelta ME, Praena Crespo M. Indicators for childhood asthma in Spain, using the Rand method. Allergol Immunopathol. 2015;43:147-56.
- Plaza V, Rodríguez del Río P, Gómez F, López Viña A, Molina J, Quintano JA, et al. Identificación de las carencias asistenciales en la atención clínica del asma en España. Resultados de la encuesta OPTIMA-GEMA. An Sist Sanit Navar. 2016;39:181-201.
- Plaza V, Bolívar I, Giner J, Llauger MA, López Viña A, Quintano JA, et al. Opinión, conocimientos y grado de seguimiento referidos por los profesionales sanitarios españoles de la Guía Española para el Manejo del Asma (GEMA) Proyecto GEMA-TEST. Arch Bronconeumol. 2008;44:245-51.
- Lora Espinosa A, Fernández Carazo C, Jiménez Cortes A, Martín Vázquez C, Pérez Frías J, Pérez Martín AF, et al. Guía de diseño y mejora continua de procesos asistenciales. Asma en la edad pediátrica. In: Consejería de Salud. Junta de Andalucía [online] [accessed 07/01/2022]. Available at www.epes.es/wp-content/uploads/Asma-en-la-edad-pediatrica_definitivo.pdf
- García Polo C, Gómez-Pastrana Duran D. Proceso Asistencial Integrado de Asma. Consejería de Salud. In: Junta Andalucía [online] [accessed 07/01/2022]. Available at www.juntadeandalucia.es/export/drupaljda/salud_5af1956d56097_asma.pdf
- Carvajal Urueña I, García Merino A, García Muñoz M, Díaz Vázquez C, Domínguez Aurrecoechea B. Plan Regional de Atención al Niño y Adolescente con Asma del Principado de Asturias (PRANA). Servicio de publicaciones del Gobierno Principado de Asturias; 2001. Actualización 2011: Carvajal Urueña I, Cobo Ruisánchez A, Mora Gandarillas I, Pérez Vaquero A, Rodríguez García J. Plan Regional de Atención al Niño/a y Adolescente con Asma del Principado de Asturias (PRANA). In: Respirar [online] [accessed 07/01/2022]. Available at www.respirar.org/images/pdf/respirar/prana_2011.pdf
- Asma Infantil: Guía para la atención de los niños y adolescentes con Asma de Castilla y León. In: Junta de Castilla y León [online] [accessed 07/01/2022] Available at www.respirar.org/images/pdf/respirar/asma_sacyl.pdf
- Amengual E, Botey A, Figuerola J, Herreros S, Hervás J, Carrión MT, et al. Plan de Asma Infantil de las Illes Balears. In: Conselleria de Salut i Consum del Govern de Les Illes Balears [online] [accessed 07/01/2022]. Available at www.ibsalut.es/apmallorca/attachments/article/1258/Plan%20de%20asma%20infantil%20de%20las%20Illes%20Balears%202007%20CAST.pdf
- Bercedo Sanz A, Gómez Serrano M, Redondo Figuero C, Martínez Herrera B, Rollán Rollán A. Guía Clínica de Manejo del Asma Bronquial en Niños y Adolescentes de Cantabria en Atención Primaria. In: Servicio Cántabro de Salud [online] [accessed 07/01/2022]. Available at www.respirar.org/images/asma_cantabria.pdf
- Grupo de trabajo de la Guía de Práctica Clínica sobre Asma Infantil. Guía de Práctica Clínica sobre Asma Infantil. Ministerio de Sanidad, Servicios Sociales e Igualdad. 2014. Guías de Práctica Clínica en el NHS. In: Guía Salud [online] [accessed 07/01/2022]. Available at https://portal.guiasalud.es/wp-content/uploads/2018/12/GPC_548_Asma_infantil_Osteba_mat_met.pdf
- Atance Melendo E, Boné Calvo J, Castillo Laita JA, Cenarro Guerrero T, Elfau Mairal M, Forés Calata A, et al. Atención al niño asmático. In: Servicio Aragonés de Salud; Gobierno de Aragón [online] [accessed 20/06/2020]. Available at www.aragon.es/estaticos/GobiernoAragon/Organismos/ServicioAragonesSalud/Documentos/ATENCIoN+NInO+ASMATICO.PDF
- Alba Moreno F, Buñuel Álvarez C, FosEscriva E, Moreno Galdo A, Oms Arias M, Puig Congost M. Asma Infantil. Guies de práctica clínica i material docent, num. 13. Barcelona: Institut Català de la Salut [online] [accessed 07/01/2022]. Available at http://canalsalut.gencat.cat/web/.content/_A-Z/A/asma/enllasos/guia_asma_infantil.pdf
- Cartera de Servicios Estandarizados de Atención Primaria de Madrid. In: Servicio Madrileño de Salud [online] [accessed 07/01/2022]. Available at www.comunidad.madrid/sites/default/files/doc/sanidad/prim/2018_cartera_de_servicios_estandarizados_ap.pdf
- Protocolo para el Manejo del Asma en Atención Primaria Coordinación entre niveles asistenciales de Atención Sanitarias del Área de Salud de Gran Canaria. Complejo Hospitalario Universitario Insular-Materno Infantil. In: Servicio Canario de Salud [online] [accessed 07/01/2022]. Available at www.sepexpal.org/download/protocolos/Protocolo-Manejo-del-Asma-en-Atencion-Primaria.pdf
- Acuňa Izcaray A, Sánchez Angarita E, Plaza V, Rodrigo G, Montes de Oca M, Gich I, et al. Quality assessment of asthma clinical practice guidelines: a systematic appraisal. Chest. 2013;144:390-7.
- Asthma Guidelines. BTS/SIGN Asthma Guideline: 2016. In: British Thoracic Society [online] [accessed 07/01/2022]. Available at www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/
- Pereira Vega A, Muñoz Zara P, Ignacio Barrios VM, Ayerbe-García R. Manejo de la agudización asmática. Asma de riesgo vital. In: Soto-Campos JG (ed.). Manual de diagnóstico y terapéutica en neumología. 3.ª edición. Madrid: Ergon; 2016. p. 389-98.
- Szefler SJ, Fitzgerald DA, Adachi Y, Doull IJ, Fischer GB, Fletcher M, et al. A worldwide charter for all children with asthma. Pediatr Pulmonology. 2020;55:1282-92.