
Vol. 23 - Num. 92
Originales
Encuesta sobre el manejo diagnóstico y el uso racional de los antibióticos en patología respiratoria pediátrica en Atención Primaria
Verónica Fernández Romeroa, M.ª Elena Cabezas Tapiab
aPediatra. CS Vélez Málaga-Sur. Vélez-Málaga. Málaga. España.
bPediatra. CS de Villaviciosa de Odón. Villaviciosa de Odón. Madrid. España.
Correspondencia: V Fernández. Correo electrónico: veronicafernandez565@gmail.com
Cómo citar este artículo: Fernández Romero V, Cabezas Tapia ME. Encuesta sobre el manejo diagnóstico y el uso racional de los antibióticos en patología respiratoria pediátrica en Atención Primaria. Rev Pediatr Aten Primaria. 2021;23:353-64.
Publicado en Internet: 12-11-2021 - Número de visitas: 16575
Resumen
Introducción: las infecciones respiratorias constituyen el principal motivo de consulta y de prescripción de antibióticos en Pediatría. La resistencia antibiótica es un problema de salud pública. Objetivo: conocer los hábitos de prescripción antibiótica en patología respiratoria pediátrica a nivel nacional.
Material y métodos: encuesta distribuida por correo electrónico a pediatras españoles y análisis estadístico realizado con el programa SPSS 20.0.
Resultados: se obtuvieron 362 encuestas. El 53,1% de los encuestados atiende de 25-35 pacientes al día. La puntuación media de respuestas correctas es de 18,8/23. En otitis media aguda, la indicación de antibioterapia y su duración se realiza según distintos criterios con porcentajes variables, el 98,6% usa amoxicilina, el 97,2% a dosis correctas. En faringoamigdalitis realiza test microbiológico el 79,1%, trata con amoxicilina 50,8% o penicilina 48,6%, durante 10 días el 84%. En patologías respiratorias de etiología vírica (broncoespasmo, catarro y bronquiolitis), más del 90% no indica antibióticos; sin embargo, la presencia de fiebre alta o secreciones verdosas aumenta su prescripción. En neumonía típica, hasta el 59,6% no realiza radiografía, recetan amoxicilina el 94,1%, durante 7 días el 68,3%. En neumonías atípicas el 97,8% prescribe macrólidos. Se observa relación estadísticamente significativa entre: experiencia laboral y puntuación en la encuesta y realización de radiografía; especialidad y calificación del cuestionario, y presión asistencial con realización de test microbiológico en faringoamigdalitis.
Conclusiones: observamos errores en el manejo de antibioterapia en Pediatría. Es necesario diseñar estrategias para la educación de la población y los profesionales sanitarios para realizar un uso juicioso de antibióticos.
Palabras clave
● Antibióticos ● Infección respiratoria ● Pediatría ● Uso apropiado de medicamentosINTRODUCCIÓN
Las infecciones respiratorias son el principal motivo de consulta en Pediatría de Atención Primaria1-3 y la causa más frecuente por la cual se prescriben antibióticos. Decidir si un antimicrobiano es necesario, cuándo iniciar dicho tratamiento y seleccionar el más apropiado, con la dosis y duración correctas, supone un reto en la práctica clínica.
España es uno de los países con mayor consumo de antibióticos en humanos sin justificación epidemiológica y es uno de los primeros estados europeos con mayor tasa de resistencia a antimicrobianos, siendo las infecciones por gérmenes resistentes un problema sanitario importante4-6.
Entre las principales razones que favorecen el desarrollo y la diseminación de las bacterias multirresistentes se encuentran el uso injustificado e inadecuado de antibióticos. Según el documento de consenso SEIMC-SEFH-SEMPSPH sobre resistencias bacterianas existe un déficit de formación del profesional y de los ciudadanos sobre la prevención, el diagnóstico y el tratamiento de las enfermedades infecciosas en nuestro país lo que justifica la variabilidad de la actuación y el aumento de las resistencias4-6.
El objetivo de nuestro trabajo es conocer los hábitos de prescripción antibiótica en patología respiratoria infantil en el ámbito de Atención Primaria, y relacionar dichos hábitos con las variables años de experiencia laboral, ámbito de trabajo urbano frente a rural, especialidad médica (Pediatría frente a otro) y presión asistencial. Así cómo evaluar si en una misma patología, la presencia de fiebre alta o secreciones verdosas motiva más la indicación de antibioterapia. La finalidad última del estudio es adquirir conocimientos que sustenten el diseño de estrategias efectivas que promuevan al uso racional de antibióticos.
MATERIAL Y MÉTODOS
Se trata de un estudio observacional descriptivo y analítico. Se diseñó un cuestionario semiestructurado y anónimo con 33 preguntas: cuatro sobre datos del profesional y puesto de trabajo; uno sobre la presión asistencial a la que se ve sometida el médico; 16 cuestiones directas sobre criterios clínicos de indicación de antibioterapia, elección de antibiótico, dosis y duración; dos sobre la realización de pruebas complementarias diagnósticas (test microbiológico en faringoamigdalitis y radiografía simple de tórax en neumonía); siete sobre casos clínicos ficticios de niños que representan motivos de consulta habituales, pero sin aportar el diagnóstico; tres sobre la creencia e influencia de los padres o cuidadores en la prescripción y dos sobre los factores que el profesional cree que influyen más en el uso inadecuado de antibióticos.
La idoneidad de la prescripción se evaluó en base a la evidencia científica existente en nuestro país, basándonos en: la Guía ABE, los Protocolos diagnósticos y terapéuticos de la Asociación Española de Pediatría (AEP), los Algoritmos de la Asociación Española de Pediatría de Atención Primaria (AEPap) y los Documentos de consenso nacionales4-23.
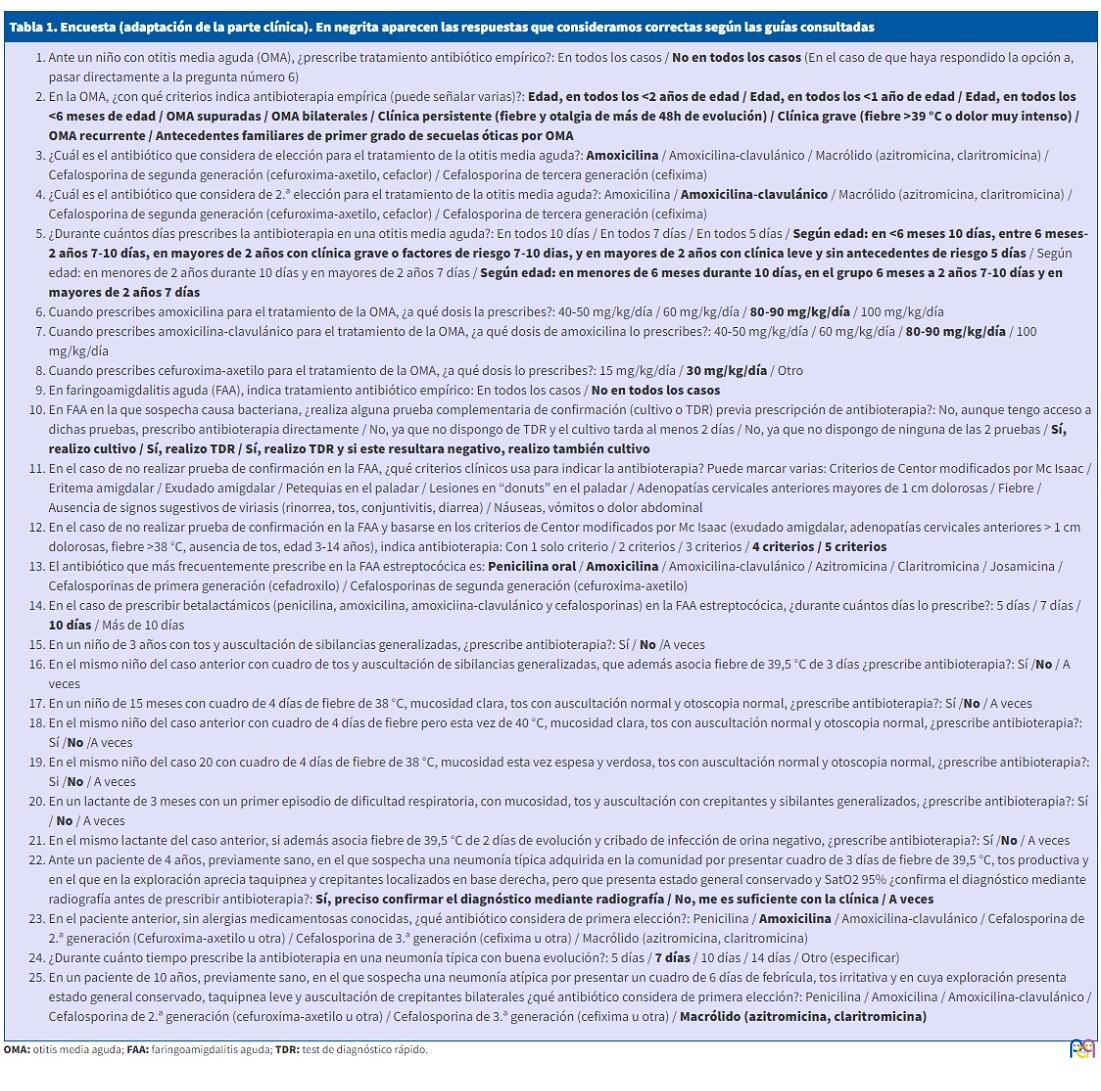
En la Tabla 1 se recoge la encuesta adaptada con los apartados clínicos y las opciones de respuesta, mostrando sombreadas las contestaciones consideradas correctas.
| Tabla 1. Encuesta (adaptación de la parte clínica). En negrita aparecen las respuestas que consideramos correctas según las guías consultadas |
|---|
|
Se envió por correo electrónico el cuestionario a médicos españoles que trabajan en puestos de Pediatría, usando como métodos de difusión: la Lista de Distribución PEDIAP y el contacto con cada una de las federadas autonómicas de la AEPap para que reenviaran el correo a sus socios. Se eligieron estos canales que permitían llegar al mayor número de profesionales dedicados a la Pediatría de Atención Primaria.
La base de datos se diseñó en Microsoft Excel. El estudio estadístico se realizó con el programa SPSS 20.0 para Windows. Se relacionaron con los resultados de la encuesta las siguientes variables: experiencia laboral (en años), especialidad médica (Pediatría vía MIR frente a otras formaciones), área de trabajo (urbana frente a rural frente a mixta) y presión asistencial (número de pacientes atendidos al día).
RESULTADOS
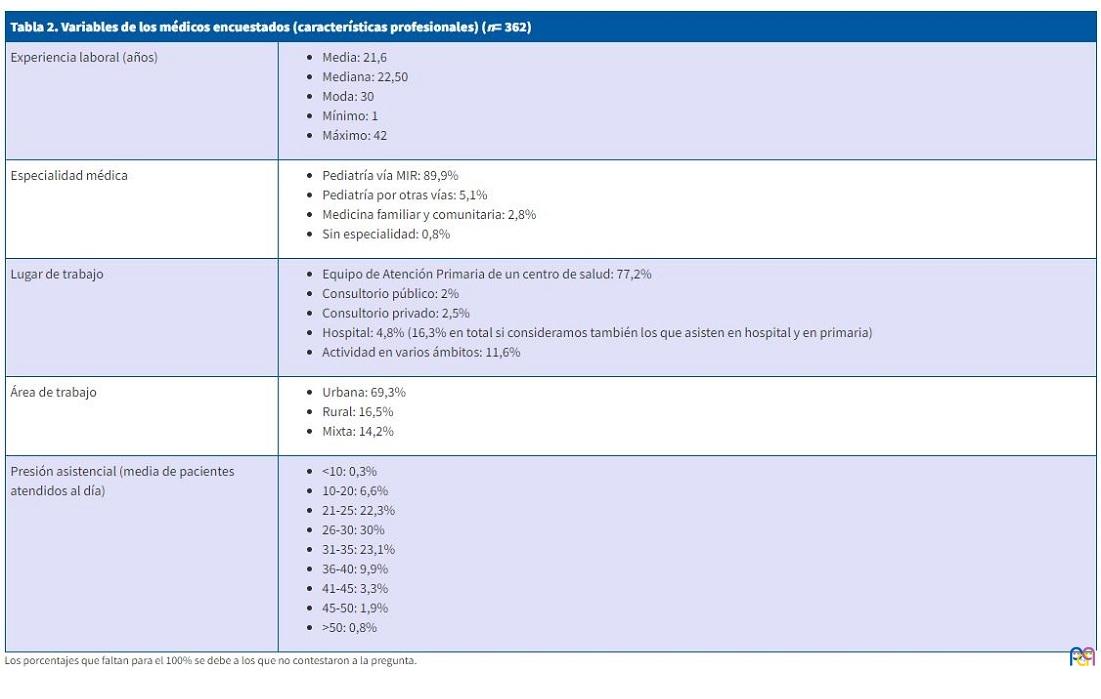
Se obtuvieron 362 cuestionarios cumplimentados. En la Tabla 2 se resumen los datos correspondientes a la formación y los aspectos laborales de los médicos. El manejo diagnóstico-terapéutico de las patologías por parte de los encuestados se resume en la Tabla 3.
| Tabla 2. Variables de los médicos encuestados (características profesionales) (n= 362) | |
|---|---|
| Experiencia laboral (años) |
|
| Especialidad médica |
|
| Lugar de trabajo |
|
| Área de trabajo |
|
| Presión asistencial (media de pacientes atendidos al día) |
|
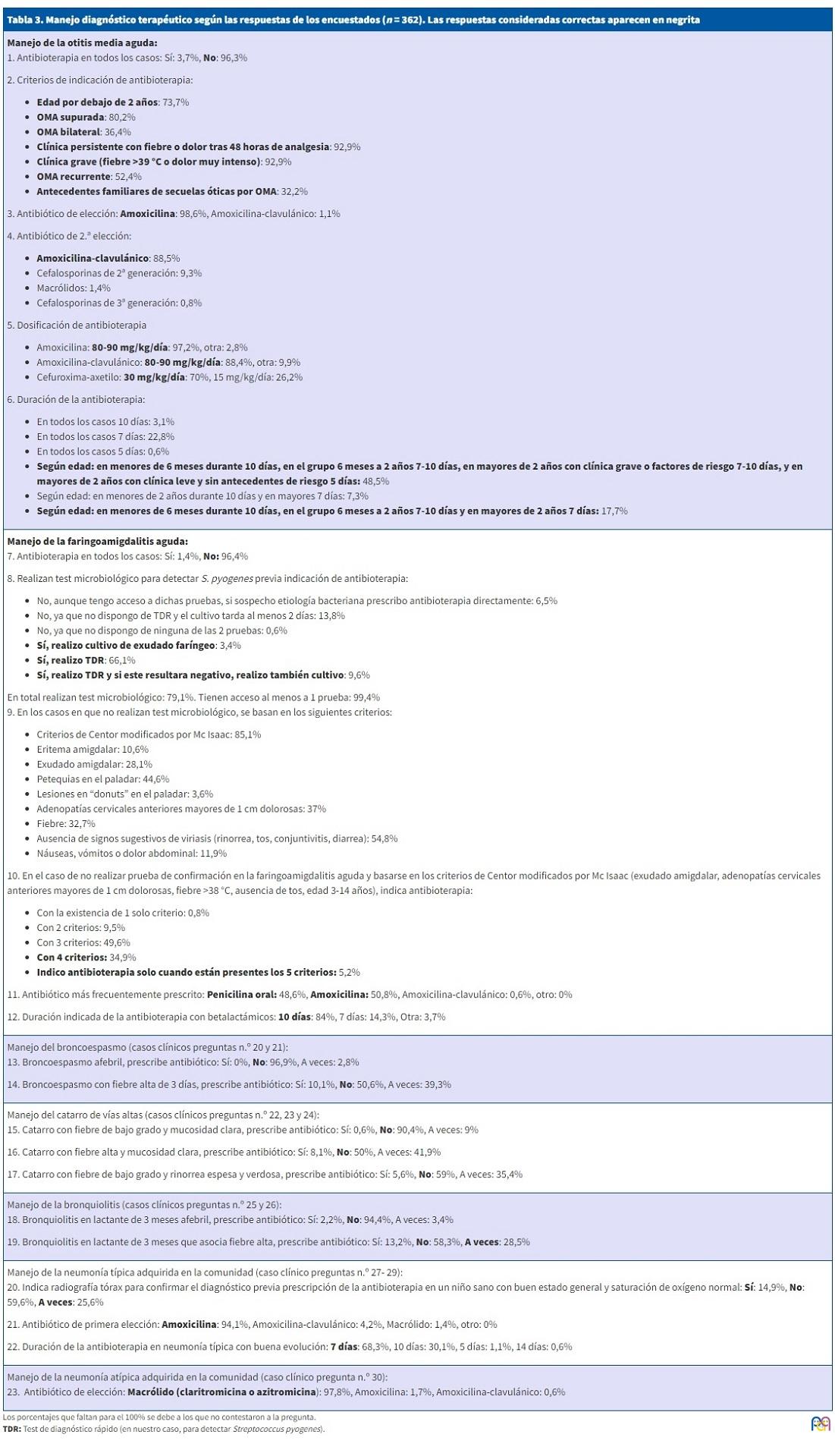
| Tabla 3. Manejo diagnóstico terapéutico según las respuestas de los encuestados (n = 362). Las respuestas consideradas correctas aparecen en negrita |
|---|
| Manejo de la otitis media aguda:
1. Antibioterapia en todos los casos: Sí: 3,7%, No: 96,3% 2. Criterios de indicación de antibioterapia:
3. Antibiótico de elección: Amoxicilina: 98,6%, Amoxicilina-clavulánico: 1,1% 4. Antibiótico de 2.ª elección:
5. Dosificación de antibioterapia
6. Duración de la antibioterapia:
|
| Manejo de la faringoamigdalitis aguda:
7. Antibioterapia en todos los casos: Sí: 1,4%, No: 96,4% 8. Realizan test microbiológico para detectar S. pyogenes previa indicación de antibioterapia:
9. En los casos en que no realizan test microbiológico, se basan en los siguientes criterios:
10. En el caso de no realizar prueba de confirmación en la faringoamigdalitis aguda y basarse en los criterios de Centor modificados por Mc Isaac (exudado amigdalar, adenopatías cervicales anteriores mayores de 1 cm dolorosas, fiebre >38 °C, ausencia de tos, edad 3-14 años), indica antibioterapia:
11. Antibiótico más frecuentemente prescrito: Penicilina oral: 48,6%, Amoxicilina: 50,8%, Amoxicilina-clavulánico: 0,6%, otro: 0% 12. Duración indicada de la antibioterapia con betalactámicos: 10 días: 84%, 7 días: 14,3%, Otra: 3,7% |
| Manejo del broncoespasmo (casos clínicos preguntas n.º 20 y 21):
13. Broncoespasmo afebril, prescribe antibiótico: Sí: 0%, No: 96,9%, A veces: 2,8% 14. Broncoespasmo con fiebre alta de 3 días, prescribe antibiótico: Sí: 10,1%, No: 50,6%, A veces: 39,3% |
| Manejo del catarro de vías altas (casos clínicos preguntas n.º 22, 23 y 24):
15. Catarro con fiebre de bajo grado y mucosidad clara, prescribe antibiótico: Sí: 0,6%, No: 90,4%, A veces: 9% 16. Catarro con fiebre alta y mucosidad clara, prescribe antibiótico: Sí: 8,1%, No: 50%, A veces: 41,9% 17. Catarro con fiebre de bajo grado y rinorrea espesa y verdosa, prescribe antibiótico: Sí: 5,6%, No: 59%, A veces: 35,4% |
| Manejo de la bronquiolitis (casos clínicos preguntas n.º 25 y 26):
18. Bronquiolitis en lactante de 3 meses afebril, prescribe antibiótico: Sí: 2,2%, No: 94,4%, A veces: 3,4% 19. Bronquiolitis en lactante de 3 meses que asocia fiebre alta, prescribe antibiótico: Sí: 13,2%, No: 58,3%, A veces: 28,5% |
| Manejo de la neumonía típica adquirida en la comunidad (caso clínico preguntas n.º 27- 29):
20. Indica radiografía tórax para confirmar el diagnóstico previa prescripción de la antibioterapia en un niño sano con buen estado general y saturación de oxígeno normal: Sí: 14,9%, No: 59,6%, A veces: 25,6% 21. Antibiótico de primera elección: Amoxicilina: 94,1%, Amoxicilina-clavulánico: 4,2%, Macrólido: 1,4%, otro: 0% 22. Duración de la antibioterapia en neumonía típica con buena evolución: 7 días: 68,3%, 10 días: 30,1%, 5 días: 1,1%, 14 días: 0,6% |
| Manejo de la neumonía atípica adquirida en la comunidad (caso clínico pregunta n.º 30):
23. Antibiótico de elección: Macrólido (claritromicina o azitromicina): 97,8%, Amoxicilina: 1,7%, Amoxicilina-clavulánico: 0,6% |
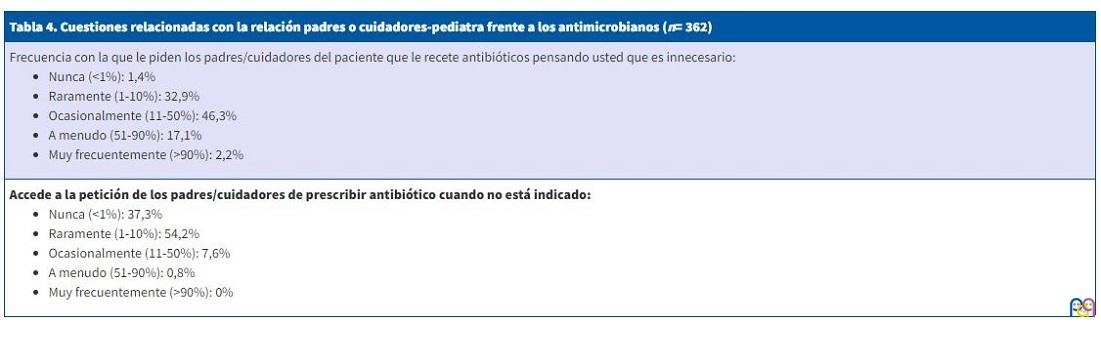
En la Tabla 4 se presentan las respuestas a las cuestiones relacionadas con la impresión por parte de los padres o cuidadores acerca del uso de antibióticos y la presión que ejercen sobre los profesionales.
| Tabla 4. Cuestiones relacionadas con la relación padres o cuidadores-pediatra frente a los antimicrobianos (n= 362) |
|---|
Frecuencia con la que le piden los padres/cuidadores del paciente que le recete antibióticos pensando usted que es innecesario:
|
Accede a la petición de los padres/cuidadores de prescribir antibiótico cuando no está indicado:
|
A la pregunta de qué factor cree que influye más en el uso inapropiado de antibióticos: el 43,1% responde la presión asistencial, el 18,6% la presión de los padres/cuidadores, el 16% la necesidad de ser “eficientes” en la consulta (evitar nuevas citas y revisiones), el 11,7% el miedo a las reclamaciones judiciales debido a la mala evolución clínica de algún caso y el 10,6% otros motivos.
A la cuestión de qué cree más determinante para disminuir el uso inapropiado de antibióticos: el 39,7% responde educar a la población, el 38,3% disponer en la consulta de material que nos facilite el diagnóstico más preciso de los procesos más comunes (otoscopia neumática para el diagnóstico de otitis media aguda [OMA], test de detección rápida de estreptococo para la faringoamigdalitis aguda [FAA], test de detección rápida de virus…), el 15,2% reducir la presión asistencial, el 0,6% todos los anteriores y el resto otros motivos.
Se obtiene una relación estadísticamente significativa e inversa, aunque de escasa magnitud, entre las variables experiencia laboral en años y puntuación en la encuesta, de modo que los profesionales con mayor experiencia laboral lograron calificaciones menores. Asimismo, existe relación estadísticamente significativa entre experiencia laboral y realización de radiografía de tórax cuando se sospecha una neumonía típica en niños sanos: a más años de experiencia, se realizan menos solicitudes de radiografías. Al comparar la formación médica con la calificación del cuestionario se observa que los especialistas en Pediatría puntuaron más alto que otros médicos de forma estadísticamente significativa. Finalmente, también encontramos significación estadística entre la presión asistencial a la que se ve sometida el profesional y la realización de un test microbiológico para el diagnóstico de faringoamigdalitis previa prescripción de antibioterapia, afectando de forma negativa en esta: los sanitarios con mayor presión asistencial realizan en menos ocasiones el test de confirmación diagnóstica. En el resto del análisis estadístico no encontramos asociaciones estadísticamente significativas con las variables estudiadas
DISCUSIÓN
Entre las limitaciones de este estudio se encuentra que, a pesar de ser una encuesta difundida a nivel nacional, solo ha respondido un 5,65% (362 médicos de 6402 plazas de Pediatría de Atención Primaria), lo que implica un sesgo de selección debido a la necesidad de estar suscritos a las listas de distribución, el manejo de los programas informáticos y la voluntariedad de la participación. Probablemente los profesionales menos concienciados con el uso racional de los antibióticos no hayan respondido a este cuestionario24. Es por ello por lo que nuestra encuesta aporta información sobre las tendencias actuales de prescripción de los médicos encuestados, pero no es adecuado extrapolar los resultados a la totalidad de profesionales que trabajan en Pediatría en nuestro país. Por otra parte, se confía en la propia notificación del médico y es posible que existan diferencias entre sus respuestas a la encuesta y lo que realmente aplican en su práctica clínica diaria.
Las resistencias bacterianas suponen un problema de salud púbica. Dichas resistencias aparecen por sobreprescripción antibiótica, por elección errónea sin ajustarse al perfil del antimicrobiano o por su utilización a dosis o duración inadecuados.
Para un tratamiento empírico adecuado deben considerarse:
- Proceso de alta probabilidad de causa bacteriana por su epidemiología y clínica, y si es factible, con el apoyo de pruebas de diagnóstico rápido u otros recursos.
- Conocer los microorganismos que con mayor probabilidad causan cada infección y las resistencias en el medio en el que se trabaja.
- Toxicidad y efectos secundarios comparativos de los antibióticos disponibles.
- Asegurar el cumplimiento mediante dosificación conveniente, palatabilidad y duración idónea.
Según una revisión Cochrane de 2015 los antibióticos producen un beneficio limitado en la OMA en edad pediátrica, siendo este mayor en niños menores de 2 años con OMA bilateral o supuración26. Como más del 80% se resuelve espontáneamente, este beneficio debe ser sopesado ante la posible toxicidad de los antimicrobianos. El 96,3% de los médicos encuestados selecciona los casos de OMA susceptibles de antibioterapia no prescribiéndola en todos los casos. Los criterios de selección más frecuentemente usados son: edad por debajo de dos años, supuración, clínica grave (fiebre >39 °C o dolor muy intenso) y persistencia de los síntomas tras 48 h de analgesia pautada. De acuerdo con las guías clínicas consultadas, la gran mayoría de los encuestados elige la amoxicilina como primera opción de tratamiento y la amoxicilina-clavulánico como segunda, con una posología correcta de dosis elevadas de amoxicilina (80-90 mg/kg/día) debido a las resistencias que el Streptococcus pneumoniae ha desarrollado en nuestro medio4-7. La variabilidad en cuanto a la duración de la antibioterapia se puede justificar por la indicación de esta en diferentes guías4-7 (Tabla 1).
La FAA es de etiología vírica en su mayoría. Entre las bacterias, la principal es Streptococcus pyogenes o estreptococo betahemolitico del grupo A (EBHGA), responsable del 30-40% de las FAA que se observan en niños de 3-13 años, del 5-10% en niños entre los 2 y 3 años y solo el 3-7% en menores de 2 años9,10. De acuerdo con esto, el 96% de los encuestados no pauta tratamiento antibiótico en la FAA de forma sistemática.
En la mayoría de los casos, es difícil diferenciar, basándose exclusivamente en la clínica, entre etiología vírica y estreptocócica de FAA. Hubo disparidad de respuesta en los encuestados acerca de los criterios clínicos en los que basaban su decisión. Son sugestivos de origen estreptocócico el dolor de garganta de comienzo brusco, la fiebre (aunque esta, y también de alto grado aparece frecuentemente en viriasis), el malestar general y la cefalea; también lo son el dolor abdominal, las náuseas y vómitos, sobre todo en niños pequeños. La existencia de petequias en el paladar no es exclusiva de la FAA por EBHGA, pues también aparecen en infecciones virales, sin embargo, casi el 45% de los encuestados lo perciben como un criterio de etiología bacteriana10. Es patognomónica la presencia en el paladar de las denominadas lesiones “donuts” correspondientes a pequeñas pápulas eritematosas con centro pálido cuya presencia solo se ha descrito en la FAA por EBHGA, y solo el 3.6% lo seleccionó para discriminar la etiología de la FAA10. La ausencia de signos sugestivos de viriasis (rinorrea, tos, conjuntivitis o diarrea) es un criterio elegido por más del 50% de los profesionales. El exudado amigdalar es frecuente encontrarlo en infecciones virales (adenovirus, mononucleosis infecciosa), por lo que, en ausencia de otros signos y síntomas, no debería ser un aspecto considerable en el diagnóstico diferencial, como cree más del 70% de encuestados10. El uso de los criterios de Centor modificados por McIsaac de forma exclusiva no es adecuado, ya que solo del 38-63% de las FAA con 4 o 5 puntos son estreptocócicas, por lo que con ellos se tiende al sobrediagnóstico con la consiguiente prescripción innecesaria de antibioterapia10.
Por tanto, dada la inespecificidad de la clínica para discernir la etiología de una FAA, es necesario la realización de pruebas microbiológicas de detección de EBHGA en pacientes bien seleccionados, con signos de infección estreptocócica probable, evitándolas cuando se sospeche un origen vírico8-11. La selección de pacientes susceptibles se hace necesaria no solo por motivos económicos, sino porque estas pruebas no disciernen entre la infección activa y el estado de portador10.
Existen dos tipos de pruebas complementarias para la detección del EBHGA: técnicas de detección rápida de antígeno estreptocócico (TDR) y cultivo de muestra faringoamigdalar8-11. Basándose en su alta especificidad, si el TDR es positivo, se acepta que el paciente presenta una FAA por EBHGA, no siendo precisa la confirmación mediante cultivo. En cambio, ante un resultado negativo algunos expertos sugieren realizar siempre cultivo, cuya sensibilidad es del 90-95% y especificidad hasta el 99%. El mayor inconveniente del cultivo es que los resultados se obtienen, en el mejor de los casos, en un plazo de 24-48 horas10. Casi la totalidad de los profesionales encuestados (99.4%) tienen acceso a un TDR para detectar el Streptococcus pyogenes, pero solo hacen uso de ellos el 79%, motivado por la presión asistencial (a mayor presión asistencial se realizan menos pruebas diagnósticas en faringoamigdalitis, probablemente por el tiempo que ha de invertirse).
El tratamiento antibiótico de la FAA estreptocócica está indicado y justificado, ya que permite una resolución más rápida de los síntomas, reduce el tiempo de contagio y previene las complicaciones supurativas locales y no supurativas9,10.
El tratamiento de elección de la FAA estreptocócica es la penicilina, dado que no se ha documentado ningún aislamiento de EBHGA resistente a la misma. La amoxicilina se considera actualmente también de primera elección en algunas guías debido a su mayor absorción gastrointestinal y tolerancia de la suspensión. En nuestra muestra, prescriben amoxicilina más del 50%. Estos hallazgos podrían deberse a varios motivos: mayor familiaridad del uso de amoxicilina; la penicilina potásica se presenta en sobres con mala palatabilidad y cuya absorción se interfiere por los alimentos; y al posible desconocimiento de los encuestados de la existencia de penicilina benzatina disponible en suspensión oral, con mejor sabor y cuya absorción no precisa de ayuno. De acuerdo con la evidencia científica disponible, el ácido clavulánico no aporta beneficio al tratamiento ya que el EBHGA no produce betalactamasas; su prescripción en la encuesta resulta minoritaria, ya que solo el 0,6% indica amoxicilina-clavulánico8-11. La pauta prescrita debe ser aquella eficaz que facilite la adherencia al tratamiento: penicilina oral debe dosificarse cada 12 h y la amoxicilina puede hacerse cada 12 o 24 horas8-11. La duración recomendada del tratamiento con betalactámicos sigue siendo actualmente de diez días, ya que pautas inferiores presentan menor porcentaje de erradicación del EBHGA8-11; llama la atención que casi el 20% de los encuestados indica otra duración.
En las preguntas presentadas en forma de caso clínico no se aportó el diagnóstico porque se pretendía reproducir una consulta real. La faceta de la prescripción que evalúan dichas cuestiones de la encuesta es la misma que valoran los estudios sobre prescripción real sin diagnóstico microbiológico.
Los primeros dos casos describen un broncoespasmo o bronquitis aguda de corta evolución con dos variantes: sin fiebre y con fiebre, considerándose lo correcto no prescribir antibioterapia en ambas. Estuvieron de acuerdo con esto casi el 97% de los médicos cuando había ausencia de fiebre, pero cuando se asociaba fiebre alta durante tres días solo el 50% se abstuvo de indicar tratamiento antibiótico.
Los siguientes tres casos describen un catarro de vías altas, en tres versiones: con fiebre de bajo grado y rinorrea clara, con fiebre alta y mucosidad clara y con fiebre escasa y secreciones verdosas y espesas. Se consideró en las tres opciones que la opción correcta era no usar antibióticos. El 90,4% coincidió con este criterio cuando no había fiebre alta ni secreciones verdosas, pero con fiebre alta el porcentaje bajó al 50% y con presencia de rinorrea verdosa al 59%.
Las preguntas número 25 y 26 se refieren a casos de bronquiolitis en un lactante de tres meses, afebril y con fiebre alta respectivamente. Sin fiebre, casi el 95% refiere no indicar antibioterapia de acuerdo a la respuesta considerada correcta, pero la aparición de fiebre de alto grado, a pesar de cribado de infección urinaria negativo, disminuye dicha abstención al 58%. En este segundo caso de bronquiolitis consideramos correcta cualquiera de las opciones (no tratar con antibióticos/sí/o hacerlo a veces), debido a que la edad del lactante propuesto de tan solo 3 meses expone una situación de inmunodeficiencia fisiológica y estado vacunal deficiente que predispone a infecciones bacterianas, y a que una neumonía intersticial puede ser indistinguible con la misma clínica.
Así pues, en infecciones de etiología eminentemente viral como el catarro de vías altas, el broncoespasmo y la bronquiolitis, se ha observado una tendencia a la prescripción incorrecta de antibióticos, que se relaciona de forma importante con la presencia de fiebre alta o de secreciones verdosas. Hay que recordar que muchas infecciones virales cursan con fiebre de alto grado y que las elevadas temperaturas no siempre se relacionan con mayor gravedad del proceso. Muchos usuarios y sanitarios creen que las secreciones verdosas y espesas indican sobreinfección bacteriana, cuando realmente se deben a la liberación de peroxidasa por parte de los leucocitos presentes en el moco.
En el manejo de las neumonías adquiridas en la comunidad (NAC), muchas guías actuales proponen en el ámbito de la Atención Primaria no realizar de rutina la radiografía de tórax, basándose su diagnóstico exclusivamente en la clínica22,23. Estaría indicado realizar una radiografía en los siguientes casos: dudas en el diagnóstico, afectación general grave o sospecha de complicaciones (derrame pleural…), episodios previos de neumonías, proceso prolongado y escasa respuesta al tratamiento y cuando exista interés para estudios epidemiológicos. Aunque pudiera parecer que no realizar una radiografía podría predisponer a un sobreuso de antibióticos por diagnóstico incorrecto, hay estudios que demuestran justo lo contrario, ya que la visualización de imágenes de atelectasias o infiltrados de etiología viral podrían motivar el inicio de una antibioterapia indebida23. En nuestra encuesta, casi el 60% respondió no realizar radiografía y ello estuvo relacionado de forma estadísticamente significativa e inversa con los años de experiencia laboral, de modo que, a mayor experiencia, menor indicación de prueba radiológica. Para nuestro estudio, consideramos correctas cualquiera de las 3 opciones (sí/no/a veces) debido a que algunas guías aún proponen su utilización para el diagnóstico de confirmación y a que hubo médicos encuestados que asistían en el ámbito hospitalario (16,3%). El 94% prescribe amoxicilina como primera opción en concordancia con la evidencia científica actual. La duración del tratamiento en una NAC de características típicas es de siete a diez días, debiéndolo acortar a 7 días en los casos con buena evolución. La estrategia de acortar los tratamientos en diversas enfermedades infecciosas, entre ellas neumonía y otitis media aguda, es una de las propuestas por la Organización Mundial de la Salud para contener las resistencias bacterianas. Aunque hay algunos estudios en neumonías típicas cuyos resultados son favorables con tratamientos de tan solo cinco días, no hay suficiente evidencia al respecto.
En neumonías atípicas adquiridas en la comunidad, casi el 98% eligió la opción de tratamiento correcto con macrólidos como la claritromicina y azitromicina.
Para todas las patologías estudiadas, la prescripción de los encuestados de amoxicilina-clavulánico, cefalosporinas y macrólidos, fue baja y, por tanto, adecuada.
Según nuestra encuesta los profesionales están sometidos a peticiones de los cuidadores para que receten antibióticos a los niños ante procesos que no lo precisan y solo ocasionalmente los médicos ceden a estas peticiones. Esto demuestra la falta de concienciación de la población en cuanto a las necesidades de tratamientos antibióticos en procesos infecciosos infantiles y la necesidad de una adecuada educación sanitaria al respecto.
Una estrategia fundamental para la mejora del uso de antimicrobianos es la educación de la población con programas sobre el uso e indicación de los antibióticos, especialmente en aquellas regiones donde haya más falta de información. Además de posibles campañas de divulgación, también hay que contar con que la actitud del propio pediatra a lo largo de repetidas consultas forma un criterio en los cuidadores de nuestros pacientes.
Para la realización de un uso racional de antibióticos en Pediatría, especialmente en el ámbito de la Atención Primaria, es necesario disponer de herramientas para realizar un diagnóstico lo más preciso posible, rápido y de bajo coste. Hemos visto que en nuestro medio existe amplia disponibilidad de test microbiológicos de faringoamigdalitis, siendo de elección en Atención Primaria el TDR. Probablemente sería recomendable introducir la neumatoscopia para evaluar mejor las otitis medias, tanto agudas como serosas, ya que es una técnica que se realiza durante la otoscopia convencional, en poco tiempo y con un equipamiento muy barato. También sería deseable poder disponer en nuestras consultas de test de diagnóstico rápido de virus (virus respiratorio sincitial e influenza preferentemente), así como de técnicas de determinación rápida de la proteína C reactiva (PCR) en sangre capilar, cuyo coste sería mayor28.
En cuanto a los factores considerados como más influyentes en el uso inapropiado de antibióticos, más del 40% contestó la presión asistencial. En el análisis estadístico, la presión asistencial influía en la falta de realización del test microbiológico en faringoamigdalitis, pudiendo aumentar el uso de antimicrobianos en esta patología; sin embargo, no se observó relación con la puntuación total de la encuesta que muestra la adherencia general a las guías clínicas actuales. Otros motivos que consideraron determinantes fueron la presión que ejercen los padres o cuidadores, la necesidad de ser eficiente en la práctica diaria evitando nuevas consultas y revisiones y a la práctica de una medicina defensiva por el miedo a las reclamaciones judiciales en casos de mala evolución.
Existen tres publicaciones relativamente recientes acerca de encuestas sobre prescripción antibiótica en Pediatría en el ámbito español29-31. Una de ellas expone el estudio ABES realizado por el Comité de Medicamentos de la AEP a nivel nacional con una muestra muy amplia de más de 1200 encuestas cumplimentadas que pretendía evaluar la selección del antibiótico de primera elección en la mayoría de las infecciones pediátricas tratadas tanto en el ámbito domiciliario como hospitalario30. En este estudio los pediatras con mayor experiencia laboral obtuvieron mejores puntuaciones, a diferencia de lo observado en el nuestro, que cuenta con una muestra mucho menor. Este hallazgo podría explicarse por la formación más reciente y actualizada de los pediatras encuestados más jóvenes.
Otra de las publicaciones versa sobre los hábitos de prescripción de los pediatras de la Comunidad Valenciana en la otitis media aguda y faringoamigdalitis aguda31. Comparativamente a esta, publicada en 2003, observamos una clara mejora en la indicación de antimicrobianos en la otitis media aguda: más del 48% refería prescribir antibioterapia en todos los casos frente nuestro 3,7% y en muchos casos se indicaba amoxicilina-clavulánico 63,6% frente a 1,1% de nuestro estudio.
Respecto a otro artículo publicado en 2005 sobre la utilización de antimicrobianos en patología respiratoria pediátrica en la Comunidad de Madrid, observamos una prescripción mejorada respecto al escaso uso de amoxicilina-clavulánico en nuestro caso y una presión similar por parte de los padres hacia el pediatra para recetar antibióticos en contra de su criterio29.
CONCLUSIONES
- Se prescriben antibióticos de forma innecesaria especialmente en los casos de catarro de vías altas, bronquiolitis y bronquitis que asocian fiebre alta o secreciones verdosas.
- El antibiótico de elección en cada una de las patologías encuestadas es correcto en un alto porcentaje de respuestas adhiriéndose a las guías clínicas actualizadas, con una prescripción de amoxicilina-clavulánico, cefalosporinas y macrólidos baja y adecuada.
- Se constató una gran disparidad de criterios en el tratamiento de una faringitis probablemente estreptocócica cuando no se realiza test microbiológico de confirmación. A mayor presión asistencial se realizan menos TRD lo que implica sobretratamiento con antimicrobianos en procesos que no lo precisan. La disminución de la presión asistencial mejoraría la aplicación de las guías clínicas de diagnóstico y tratamiento.
- Médicos con mayor experiencia laboral puntuaron peor en la encuesta, lo que podría implicar que conforme aumenta la edad disminuye la actualización de los profesionales y se ajustan menos a las guías con mayor evidencia. Los médicos más jóvenes se ajustan más a la evidencia y a las guías clínicas actualizadas.
- A mayor experiencia laboral menor indicación de radiografía de tórax en sospecha de neumonía típica en niños sanos, disminuyendo la radiación de estos y el uso inadecuado de antibióticos.
- La especialización en Pediatría implica un mayor conocimiento de los protocolos con un mayor número de respuestas correctas frente a los médicos que atienden niños y carecen de dicha formación.
- Es necesario la implantación de vías de formación de los profesionales para mejorar la prescripción de antibióticos y de educación para la salud de la población para no solicitar dichos tratamientos en procesos para los que no son necesarios.
CONFLICTO DE INTERESES
Las autoras declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
AEP: Asociación Española de Pediatría · AEPap: Asociación Española de Pediatría de Atención Primaria · EBHGA: estreptococo betahemolitico del grupo A · FAA: faringoamigdalitis aguda · NAC: neumonía adquirida en la comunidad · OMA: otitis media aguda · PCR: proteína C reactiva · TDR: técnicas de detección rápida.
BIBLIOGRAFÍA
- De la Flor i Brú J. ¿Dónde estamos 30 años después? Análisis descriptivo de un año en una consulta pública de Pediatría de Atención Primaria. Pediatr Integral. 2012; XVI:180-2.
- SEIMC, SEFH y Sociedad Española de Medicina Preventiva, Salud Pública e Higiene. Documento de consenso - Acciones y medidas para combatir las resistencias bacterianas en España, una de las mayores amenazas para la salud pública. En: Asociación Española de Pediatría [en línea] [consultado el 03/11/2021]. Disponible en www.aeped.es/sites/default/files/documento_de_consenso_seimc-sefh-sempsph_sobre_resistencias_bacterianas.pdf
- ECDC country visit to Spain to discuss antimicrobial resistance issues. En: European Centre for Disease Prevention and Control [en línea] [consultado el 03/11/2021]. Disponible en https://www.ecdc.europa.eu/en/publications-data/ecdc-country-visit-spain-discuss-antimicrobial-resistance-issues
- López González G, Martínez Antón A, Ruiz Contreras J. Otitis media aguda (v.2/2008). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en https://www.guia-abe.es/gestion/includes/html4pdf.php?id=otitis-media-aguda
- Del Castillo Martín F, Baquero Artigao F, García Migue MJ, Méndez Echevarría A. Otitis media aguda. Protoc Diagn Ter Pediatr. 2011;1:67-76.
- Del Castillo Martín F, Baquero Artigao F, de la Calle Cabrera T, López Robles MV, Ruiz Canela J, Alfayate Miguelez S, et al. Documento de consenso sobre etiología, diagnóstico y tratamiento de la otitis media aguda. An Pediatr (Barc). 2012;77:345.e1-345.e8.
- Cubero Santos A, García Vera C, Lupiani Castellanos P. Otitis media aguda. En: Guía de Algoritmos en Pediatría de Atención Primaria [en línea] [consultado el 03/11/2021]. Disponible en https://algoritmos.aepap.org/algoritmo/37/otitis-media-aguda
- Fernández-Cuesta Valcarce MA, Benedicto Subirá C. Faringitis aguda (v.3/2011). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en www.guia-abe.es/temas-clinicos-faringitis-aguda
- Álvez González F, Sánchez Lastres JM. Faringoamigdalitis aguda. Protoc diagn ter pediatr. 2011;1:25-36.
- Piñeiro Pérez R, Hijano Bandera F, Álvez González F, Fernández Landaluce A, Silva Rico JC, Pérez Cánovas C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75:342.e1-342.e13
- Cubero Santos A, García Vera C, Lupiani Castellanos P. Faringoamigdalitis. En: Guía de Algoritmos en Pediatría de Atención Primaria [en línea] [consultado el 03/11/2021]. Disponible en https://algoritmos.aepap.org/algoritmo/13/faringoamigdalitis
- Albi Rodríguez MS, Reig Rincón de Arellano I. Bronquitis (traqueobronquitis) aguda (v.2.0/2019). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en www.guia-abe.es/temas-clinicos-bronquitis-(traqueobronquitis)-aguda
- Calvo Rey C, García García ML, Casas Flecha I, Pérez Breña P. Infecciones respiratorias virales. Protoc Diagn Ter Pediatr. 2011;1:189-204.
- Castillo Laita JA, de Benito Fernández J, Escribano Montaner A, Fernández Benítez M, García de la Rubia S, Garde Garde J, et al. Consenso sobre tratamiento del asma. An Pediatr (Barc). 2007;67:253-73.
- Cortés Rico O, Rodríguez Fernández-Oliva CR. Crisis de asma. En: Guía de Algoritmos en Pediatría de Atención Primaria [en línea] [consultado el 03/11/2021]. Disponible en https://algoritmos.aepap.org/algoritmo/35/crisis-de-asma
- González Requejo A. Catarro de vías altas (v.3/2015). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en www.guia-abe.es/gestion/includes/html4pdf.php?id=catarro-de-vias-altas
- Pavo García MR, Rojo Conejo P, Baro Fernández M. Bronquiolitis (v.3/2014). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en www.guia-abe.es/
- García García ML, Korta Murua J, Callejón Callejón A. Bronquiolitis aguda viral. Protoc Diagn Ter Pediatr. 2017;1:85-102.
- Cano Garcinuño A, Mora Gandarillas I, García Merino A. Bronquiolitis. En: Guía de Algoritmos en Pediatría de Atención Primaria [en línea] [consultado el 03/11/2021]. Disponible en https://algoritmos.aepap.org/
- Hernández Merino A, Guerra García F. Neumonía (v.2/2008). En: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [en línea] [consultado el 03/11/2021]. Disponible en www.guia-abe.es
- Méndez Echevarría A, García Miguel MJ, Baquero Artigao F, Del Castillo Martín F. Neumonía adquirida en la comunidad. Protoc diagn ter pediatr. 2011;1:59-66.
- Úbeda Sansano MI, Murcia García J, Asensi Monzó MT; Grupo de Vías Respiratorias. Neumonía adquirida en la comunidad. El pediatra de Atención Primaria y la Neumonía. En: Respirar.org [consultado el 03/11/2021]. Disponible en www.respirar.org/index.php/grupo-vias-respiratorias/protocolos
- Úbeda Sansano MI, Murcia García J. Guía de Algoritmos en Pediatría de Atención Primaria. Neumonía adquirida en la comunidad. AEPap. 2017 (en línea) consultado el 02/01/2019. Disponible en https://algoritmos.aepap.org/
- Gorrotxategi Gorrotxategi P, García Vera C, Graffigna Lojendio A, Sánchez Pina C, Palomino Urda N, Rodríguez Fernández-Oliva CR, et al. Situación de la Pediatría de Atención Primaria en España en 2018. Rev Pediatr Aten Primaria. 2018;20:e89-e104.
- Grupo de Patología Infecciosa, AEPap. Uso racional de antibióticos y Resistencias bacterianas. [en línea] [consultado el 01/03/2020]. Disponible en www.aepap.org/grupos/grupo-de-patologia-infecciosa/uso-racional-de-antibioticos-y-resistencias-bacterianas
- Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2013;(1):CD000219.
- Álvez F. Uso racional de antibióticos en las infecciones más comunes de los niños. An Pediatr Contin. 2010;8:221-30.
- De la Flor i Brú J, Marés Bermúdez J. Test de diagnóstico microbiológico rápido en la consulta de Pediatría de Atención Primaria. Pediatr Integral. 2018;XXII:246.e1-246.e9.
- Herranz Jordán B, Pérez Martín C. Encuesta sobre prescripción de antibióticos en infecciones respiratorias pediátricas. Rev Pediatr Aten Primaria. 2005;7:557-78.
- Piñeiro Pérez R, Calvo Rey C, Medina Claros A.F, Bravo Acuña J, Cabrera García l, Fernández-Llamazares CM, et al. Uso empírico de antibióticos en niños en España. Resultados de una Encuesta Pediátrica Nacional 2012 (Estudio ABES). An Pediatr (Barc). 2013;79:32-41.
- Casaní Martínez C, Calvo Rigual F, Peris Vidal A, Álvarez de Lavida Mulero T, Díez Domingo J, Graullera Millas M, et al. Encuesta sobre el uso racional de antibióticos en Atención Primaria. An Pediatr (Barc). 2003;58:10-6.