
Vol. 22 - Num. 85
Originales
Características clínicas y evolutivas de la neumonía adquirida en la comunidad en pacientes hospitalarios
Mercedes Cemeli Canoa, Sara Laliena Aznarb, José Valiente Lozanoc, Berta Martínez Ganuzad, Matilde Bustillo Alonsoe, César García Veraf
aPediatra. CS Valdespartera-Montecanal. Zaragoza. España.
bPediatra. CS Cuarte de Huerva. Zaragoza. España.
cEnfermero. CS Valdespartera. Zaragoza. España.
dPediatra. Servicio de Urgencias Extrahospitalario San Martín. Servicio Navarro de Salud-Osasunbidea. Pamplona. Navarra. España.
eUnidad de Infectología Pediátrica. Servicio de Pediatría. Hospital Universitario Miguel Servet. Zaragoza. España.
fPediatra. CS José Ramon Muñoz Fernández. Zaragoza. España.
Correspondencia: M Cemeli. Correo electrónico: cano.mcemeli@salud.aragon.es
Cómo citar este artículo: Cemeli Cano M, Laliena Aznar S, Valiente Lozano J, Martínez Ganuza B, Bustillo Alonso M, García Vera C. Características clínicas y evolutivas de la neumonía adquirida en la comunidad en pacientes hospitalarios. Rev Pediatr Aten Primaria. 2020;22:23-32.
Publicado en Internet: 02-03-2020 - Número de visitas: 26791
Resumen
Introducción: la neumonía adquirida en la comunidad (NAC) sigue siendo una enfermedad frecuente en la edad pediátrica, encontrándose entre las primeras causas de mortalidad. El objetivo del estudio fue conocer la incidencia de las neumonías ingresadas y describir sus características.
Material y métodos: estudio descriptivo y retrospectivo que incluyó a los pacientes ingresados en el Servicio de Pediatría del Hospital Universitario Miguel Servet de Zaragoza (España), con el diagnóstico de NAC durante dos años para describir sus características clínicas, radiológicas, analíticas, demográficas y complicaciones.
Resultados: se registraron 248 casos de neumonía, con una media de edad de 37,60 ± 2,20 meses, siendo significativamente mayor en neumonías bacterianas típicas (41,98 ± 37,46) y atípicas (73,43 ± 41,28) frente a las víricas (23,30 ± 19,07) (p <0,0001 y p = 0,0004 respectivamente). La neumonía más frecuente fue la de probable origen neumocócico (47,6%; intervalo de confianza del 95% [IC 95]: 41,84 a 54,18) mientras que el agente identificado con más frecuencia el virus respiratorio sincitial (34,65%; IC 95: 26,93 a 43,26). La odds ratio de presentar patrón radiológico alveolar en neumonías bacterianas frente a víricas fue de 2,98 (IC 95: 1,50 a 5,91; p = 0,0013). El antibiótico más utilizado fue ampicilina intravenosa (62,87%), siendo la duración mayor en las neumonías típicas bacterianas.
Conclusión: la NAC que precisa ingreso hospitalario es más prevalente en niños menores de cuatro años; con una incidencia y complicaciones similares a las descritas en otras series. El diagnóstico etiológico y el consiguiente tratamiento antibiótico continúa siendo un reto difícil de alcanzar.
Palabras clave
● Hospital ● Neumonía adquirida en la comunidad ● PediatríaINTRODUCCIÓN
La neumonía adquirida en la comunidad (NAC) constituye la principal causa individual de mortalidad infantil en todo el mundo. En países desarrollados, se estima que suceden hasta 2,6 millones de casos anuales de NAC en niños menores de cinco años, causando 1,5 millones de hospitalizaciones y, aproximadamente, 3000 muertes por esta causa1,2.
Por ello, su elevada incidencia anual, con 30-40 casos por 1000 niños menores de cinco años y su potencial gravedad, originan gran preocupación y consumo de recursos. La gran mayoría de los estudios están realizados en el ámbito hospitalario, que con frecuencia engloba los casos de mayor gravedad. Uno de los principales retos en el tratamiento de los niños con NAC es conseguir el diagnóstico etiológico, siendo complicado la detección del germen por muestras habituales de laboratorio. La identificación dependerá de la disponibilidad de las técnicas, por lo que en publicaciones la etiología se puede demostrar en función de estas entre un 40-85%2-4.
Las complicaciones de las neumonías se producen cuando la infección no se limita al parénquima pulmonar, sino que se extiende a áreas vecinas, o cuando el desarrollo de la infección es más complejo de lo habitual por diferentes motivos. Esto modifica el curso clínico de la neumonía inicial constituyendo un reto en su manejo, dado que no existen unos criterios totalmente unificados sobre su tratamiento.
Las principales complicaciones de la NAC son: derrame pleural (DP), empiema pulmonar, neumotórax, fístula broncopleural, absceso pulmonar, neumonía necrosante o necrotizante, pioneumotórax, bacteriemia o septicemia. Estas complicaciones suceden solo en el 1% de las neumonías, aunque este porcentaje aumenta a casi un 40% en caso de precisar ingreso hospitalario5-7.
La neumonía es la causa principal de DP en niños y, aproximadamente, el 20-40% de las que ingresan presentan DP y de ellos, entre un 0,6-2% acaban en empiema. En las últimas décadas se han observado cambios epidemiológicos, con un aumento de la prevalencia de este tipo de complicaciones de las neumonías (la incidencia anual de DP ha pasado de 18 a 42/100 000 niños y la incidencia en niños ingresados de 0,76 a 3,3/100). También se han constatado cambios en la prevalencia de gérmenes y serotipos que se han relacionado con el uso más racional de antibióticos y los cambios en la estrategia vacunal7,8.
Por todo ello, es importante que reconozcamos si la NAC en la edad pediátrica está sufriendo una serie de cambios epidemiológicos, clínicos, etiológicos y de resistencias a antibióticos que obliguen a replantear su abordaje diagnóstico y terapéutico. Por ello, el objetivo de este estudio es conocer las tendencias etiológicas más actuales en nuestro entorno junto a los perfiles clínicos y evolutivos en la población pediátrica hospitalizada por NAC.
MATERIAL Y MÉTODOS
Estudio retrospectivo descriptivo y analítico a través de los registros clínicos de pacientes ingresados en el Hospital Universitario Infantil Miguel Servet de Zaragoza (España). Se incluyeron aquellos pacientes que ingresaron con el diagnóstico clínico y radiológico de neumonía. El periodo de estudio fue de dos años naturales (2017-2018) y se incluyeron los niños a partir de un mes de edad hasta 14 años.
A pesar de no ser siempre necesaria para el diagnóstico de NAC, la radiografía de tórax se consideró como gold standard para establecer el diagnóstico de NAC. Se consideró neumonía la presencia, en un paciente previamente sano, de clínica respiratoria infecciosa compatible (fiebre, tos, dificultad respiratoria, rinitis) sumada a un patrón radiológico alveolar (consolidación lobar o segmentaria con broncograma aéreo o derrame pleural en neumonías con probable etiología bacteriana), o intersticial (infiltrados perihiliares difusos bilaterales, atrapamiento aéreo y atelectasias en el caso de neumonías atípicas o víricas) o mixto o indefinido.
Los criterios de exclusión de pacientes para este estudio fueron: pacientes menores de un mes y mayores de 14 años; inmunodeficiencias primarias o secundarias; enfermedad neoplásica; fibrosis quística; patología pulmonar (secuestros pulmonares, bronquiectasias, displasia broncopulmonar); encefalopatías con posibilidad de broncoaspiración; pacientes positivos a la prueba de la tuberculina o prueba cutánea de derivado proteico purificado; pacientes hospitalizados más de siete días antes del inicio de los síntomas.
Se recogió como variable principal el tipo de neumonía (bacteriana de probable origen neumocócico, atípica bacteriana, vírica y mixta). Variables secundarias incluidas para el estudio fueron de tipo demográfico (edad, sexo), epidemiológico (antecedente personales incluido antecedente de bronquitis o hiperreactividad bronquial (HRB), estado de vacunación, y lactancia materna), clínicas (temperatura máxima y su duración, tos, frecuencia respiratoria (FR) determinada en función de la edad según criterios de la Organización Mundial de la Salud (OMS)9, signos de dificultad respiratoria, saturación de oxígeno y otros síntomas extrapulmonares), radiológicas (patrón, localización y presencia de derrame pleural u otras complicaciones), analíticas (cifra absoluta de leucocitos, neutrófilos, proteína C reactiva [PCR]), serología IgM de M. pneumoniae, resultado del aspirado nasofaríngeo (ANF) para virus y de tratamiento (tipo, vía y duración).
Cuando se detectó S. pneumoniae se hizo mediante cultivo o reacción en cadena de la polimerasa en líquido pleural o hemocultivo. El diagnóstico de neumonía atípica se realizó a través de serología para M. pneumoniae mediante el método ELISA (basado en la reacción de los anticuerpos de la muestra con el antígeno unido a la superficie de poliestireno), que permite la cuantificación de IgM con una sensibilidad de 81-89% en niños1,10.
El diagnóstico de neumonía de origen vírico se realizó a través de ANF mediante inmunofluorescencia (IF), que incluye la determinación de los siguientes virus: virus respiratorio sincitial (VRS), influenza A y B, parainfluenza 1,2,3, metapneumovirus y adenovirus.
Para el análisis de los tipos de neumonía se realizó la siguiente agrupación: bacteriana típica (se incluyeron S. aureus, S. pyogenes, B. pertussis y las supuestamente neumocócicas), atípica bacteriana (M. pneumoniae y Chl. pneumoniae), vírica y mixta.
Toda la información recogida se trató conforme a lo establecido en la Ley Orgánica 15/99, de Protección de Datos de Carácter Personal. En la base de datos del estudio no se incluyeron datos personales de los pacientes, ni ningún dato que permitiera identificarlos. Se le asignó a cada paciente un código que solo el equipo investigador conocía.
Análisis estadístico
En el análisis descriptivo de los datos se calcularon para las variables cuantitativas las medidas de tendencia central y de dispersión (media, mediana y desviación estándar [DE]); para las cualitativas los datos se expresaron en valores de frecuencia absolutas y en porcentajes con sus respectivos IC 95. Para el estudio analítico, las relaciones entre variables se exploraron mediante el cálculo de la odds ratio (OR) y de la diferencia de medias (DM) con sus respectivos IC 95. La significación estadística fue calculada mediante los estadísticos χ2 y t de Student. El valor de p considerado como significativo fue ≤0,05.
RESULTADOS
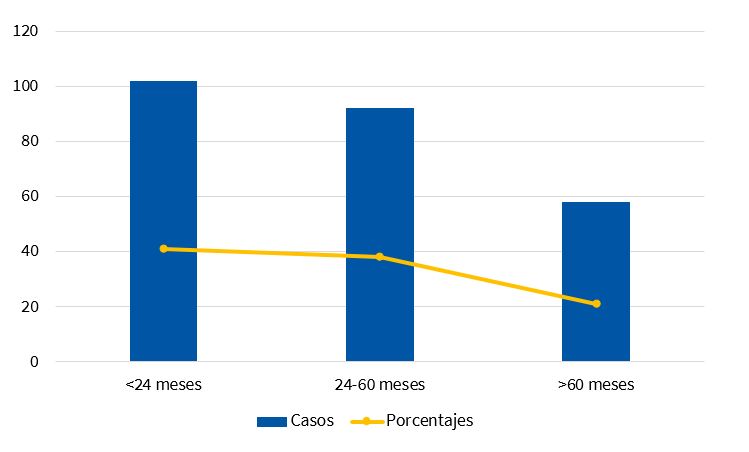
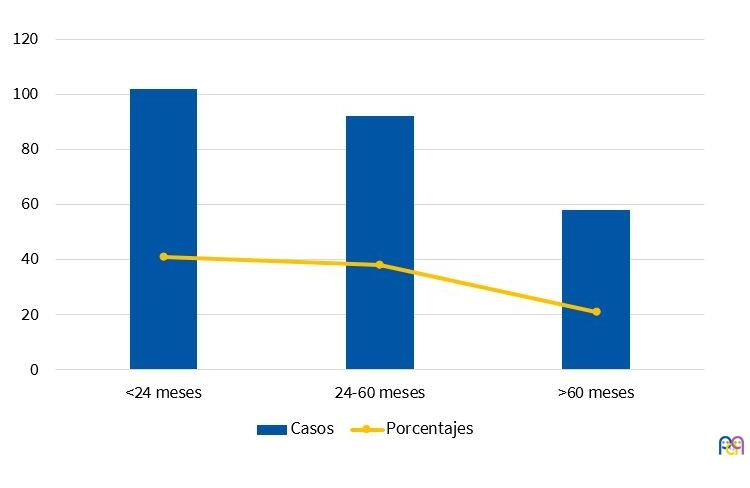
Un total de 248 pacientes pediátricos cumplieron criterios de inclusión, con una media de edad de 37,60 ± 2,20 meses. La distribución por sexos fue muy similar (50,92% mujeres, 49,08% hombres). En la Fig. 1 se muestra la distribución por rangos de edad. La mayoría de los episodios ocurrieron en otoño (36,69%) e invierno (26,61%). Las neumonías bacterianas típicas predominaron en otoño y primavera, mientras que víricas y atípicas lo hicieron en invierno y otoño.
| Figura 1. Distribución de los casos de neumonía por edad (meses) |
|---|
 |
El 42,80% (IC 95: 36,74 a 49,08) de los pacientes presentaron antecedentes de asma o HRB y hasta un 4,84% (IC 95: 2,79 a 8,27) había presentado una neumonía previa. El antecedente de HRB se registró de forma no estadísticamente significativa en mayor número de casos de neumonías víricas (50,50%; IC 95: 40,50 a 60,66) que en bacterianas típicas (38,42%; IC 95: 30,50 a 46,22). De la misma forma, el 52,23% (IC 95: 31,85 a 72,55) de las neumonías bacterianas atípicas tuvieron el antecedente, en proporción no significativamente mayor que en las neumonías típicas.
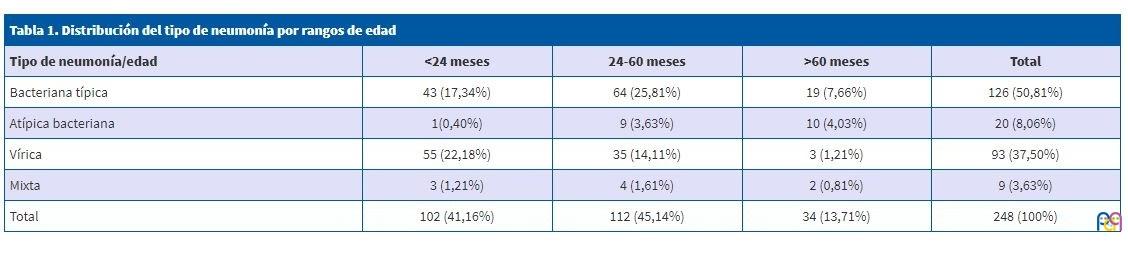
La edad media fue significativamente mayor en el global de neumonías bacterianas (46,86 ± 39,62 meses) frente a las víricas (23,30 ± 19,07 meses): DM 23,56 meses (IC 95:16,10 a 31,02 meses, p <0,0001) (Tabla 1). Del mismo modo, la edad media fue significativamente mayor en los pacientes con neumonía atípica (73,43 ± 41,28 meses) que en los pacientes con neumonía bacteriana de sospecha típica (41,98 ± 37,46 meses) (DM: 31,45 meses; IC 95: 14,38 a 48,51; p = 0,0004), así como entre niños con bacterianas típicas y víricas (DM: 18,68 meses [IC 95: 11,05 a 26,30; p <0,0001]).
| Tabla 1. Distribución del tipo de neumonía por rangos de edad | ||||
|---|---|---|---|---|
| Tipo de neumonía/edad | <24 meses | 24-60 meses | >60 meses | Total |
| Bacteriana típica | 43 (17,34%) | 64 (25,81%) | 19 (7,66%) | 126 (50,81%) |
| Atípica bacteriana | 1(0,40%) | 9 (3,63%) | 10 (4,03%) | 20 (8,06%) |
| Vírica | 55 (22,18%) | 35 (14,11%) | 3 (1,21%) | 93 (37,50%) |
| Mixta | 3 (1,21%) | 4 (1,61%) | 2 (0,81%) | 9 (3,63%) |
| Total | 102 (41,16%) | 112 (45,14%) | 34 (13,71%) | 248 (100%) |
Con respecto a las vacunas, casi la totalidad de los niños de la serie (99%) estaban correctamente vacunados frente a H. influenzae según el calendario vacunal en vigor en Aragón y un 90% frente a neumococo (vacuna no incluida en calendario hasta el año 2016).
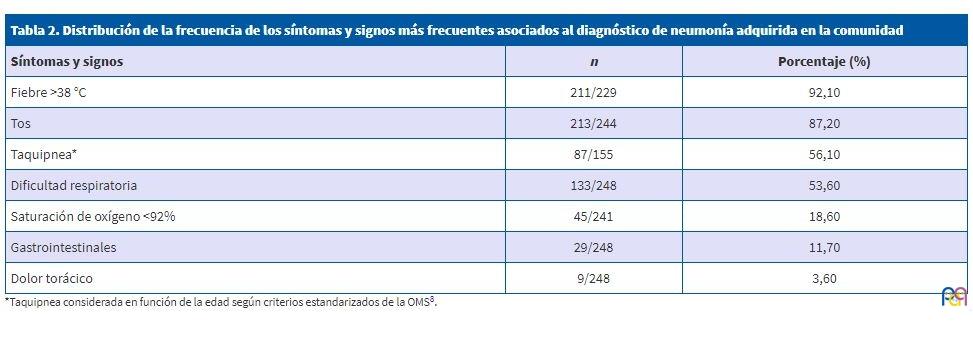
En la Tabla 2 se presentan los síntomas y signos más frecuentes al diagnóstico. El signo más frecuente fue la fiebre, presente en el 85,1% (IC 95: 80,1 a 89,0), con una media de temperaturas máximas de 39,04 ± 0,91 °C y una duración media al diagnóstico de 3,88 ± 2,74 días. La temperatura máxima media fue significativamente mayor en pacientes con neumonía vírica (39,28 ± 0,77 °C) que con neumonía bacteriana típica (38,92 ± 0,96 °C): DM: 0,36 °C; IC 95: 0,12 a 0,59; p = 0,0031, o con neumonía bacteriana atípica (38,55 ± 0,94 °C): DM: 0,73 °C; IC 95: 0,34 a 1,12; p = 0,0004).
| Tabla 2. Distribución de la frecuencia de los síntomas y signos más frecuentes asociados al diagnóstico de neumonía adquirida en la comunidad | ||
|---|---|---|
| Síntomas y signos | n | Porcentaje (%) |
| Fiebre >38 °C | 211/229 | 92,10 |
| Tos | 213/244 | 87,20 |
| Taquipnea* | 87/155 | 56,10 |
| Dificultad respiratoria | 133/248 | 53,60 |
| Saturación de oxígeno <92% | 45/241 | 18,60 |
| Gastrointestinales | 29/248 | 11,70 |
| Dolor torácico | 9/248 | 3,60 |
En relación con la duración de la fiebre, únicamente existieron diferencias significativas entre neumonías bacterianas típicas (3,62 ± 2,56 días) (DM: 2,1 días; IC 95: 0,76 a 3,44; p = 0,0023) y neumonías bacterianas atípicas (5,72 ± 3,30 días) (DM: 2,04 días; IC 95: 0,68 a 3,40; p = 0,0037).
La tos se registró en un 87% (IC 95: 82 a 90%) de los casos. Su ausencia fue mayor en pacientes con neumonía atípica (27%, IC 95: 9 a 46) que con bacteriana típica (13%, IC 95: 7 a 19). La diferencia alcanzó el umbral de significación estadística entre atípicas y víricas (8%; IC 95: 3 a 14) (OR: 4,08; IC 95: 1,25 a 13,34; p = 0,0141).
Analizando los 155 pacientes en los que constaba la FR, el 49,03% (IC 95: 41,28 a 56,83) presentó taquipnea. No fue significativamente más prevalente en ningún tipo concreto de neumonía, aunque se detectó en más casos de neumonía vírica (53,23%; IC 95: 40,98 a 65,09) que bacteriana típica (47,22%; IC 95: 36,13 a 58,60) o atípica (46,67%; IC 95: 24,81 a 69,88).
En lo referido a las cifras de saturación de oxígeno al diagnóstico, no hubo diferencias significativas entre neumonías típicas (95,60 ± 3,12), las atípicas (94,52 ± 2,78), ni víricas (95,05 ± 2,90).
Anomalías en la auscultación pulmonar (AP) hubo en el 81,45% de los casos, siendo la hipoventilación (49,60%) y los crepitantes (40,32%) los hallazgos más frecuentes.
Otros síntomas y signos se presentaron en menor proporción, no menos importantes, como son la clínica digestiva (24,60%) (IC 95: 19,65 a 30,32), y el dolor torácico (4,44%) (IC 95: 2,29 a 7,77), más frecuentes en edades tardías.
Los hallazgos radiológicos están presentados en la Tabla 3. El patrón alveolar fue el que apareció con mayor frecuencia y el DP apareció en un 19,76%. Si separamos por rango de edad y germen, el patrón alveolar fue más frecuente en menores de cuatro años y en neumonías probablemente neumocócicas. En el 73,47% (IC 95: 64,56 a 82,50) de las neumonías víricas el patrón fue alveolar, igual que en el 91,30% (IC 95: 73,20 a 97,50) de las neumonías por M. pneumoniae. La edad media de los pacientes que presentaron patrón alveolar (39,41 ± 35,97 meses) fue significativamente mayor que aquellos que presentaron patrón intersticial (25,71 ± 19,65), DM: 13,70 meses; IC 95: 1,52 a 25,88, p = 0,0295).
| Tabla 3. Distribución por rangos de edad del patrón radiológico. Se muestran otros hallazgos de interés como son atelectasia y neumonía redonda | ||||
|---|---|---|---|---|
| Patrón radiológico/edad | <24 meses | 24-60 meses | >60 meses | Total (n=248) |
| Alveolar | 78 (37,86%) | 98 (47,57%) | 30 (14,56%) | 206 (83,06%) |
| Intersticial | 8 (57,14%) | 5 (35,71%) | 1 (7,14%) | 14 (5,65%) |
| Mixto | 16 (57,14%) | 9 (32,14%) | 3 (10,71%) | 28 (11,29%) |
| Atelectasia | 6 (28,57%) | 11 (52,30%) | 4 (19,05%) | 21 (8,47%) |

No existe una relación significativa entre el patrón alveolar de las bacterianas atípicas (91,30%; IC 95: 79,80 a 102,80) frente a las típicas (88,80%; IC 95: 83,30 a 94,30). Sin embargo, la probabilidad de presentar patrón alveolar es 2,98 veces mayor en el total de bacterianas (89,20%; IC 95: 84,21 a 94,22) que en las víricas (73,50%, IC 95: 64,77 a 82,23) OR: 2,98; IC 95: 1,50 a 5,91; p = 0,0013, y también significativamente mayor en las bacterianas típicas que en las víricas, OR: 2,86 (IC 95: 1,40 a 5,85; p = 0,0031).
Presentaron atelectasias 21 pacientes, un 61,90% fueron de probable origen neumocócico, un 23,81% vírico y el resto por M. pneumoniae. En una de las tres neumonías redondas, se aisló parainfluenza virus 3.
Los motivos de ingreso fueron múltiples, sin embargo, los más frecuentes fueron las neumonías con hipoxemia (28,23%), derrame pleural (19,76%), la afectación multifocal (11,69%) y el fallo del tratamiento antibiótico oral (7,26%).
Se consiguió identificar el germen causal en 139 pacientes (56,05%) (IC 95: 46,61 a 58,95). El microorganismo más frecuentemente encontrado fue el VRS (17,74%) (Tabla 4). S. pneumoniae se detectó en siete casos, mientras el ANF para virus fue positivo en 90 pacientes.
| Tabla 4. Principales agentes etiológicos identificados | ||
|---|---|---|
| Agentes identificados | n | Porcentaje |
| Streptococcus pneumoniae | 7 | 2,82% |
| Streptococcus aureus | 1 | 0,40% |
| Streptococcus pyogenes | 2 | 0,81% |
| Bordetella pertussis | 1 | 0,40% |
| Mycoplasma pneumoniae | 24 | 9,68% |
| Chlamydia pneumoniae | 5 | 2,02% |
| Virus respiratorio sincitial | 44 | 17,74% |
| Influenza A virus | 21 | 8,47% |
| Influenza B virus | 7 | 2,82% |
| Metapneumovirus | 7 | 2,82% |
| Parainfluenza virus 1, 2 y 3 | 5 | 2,02% |
| Adenovirus | 5 | 2,02% |
| Enterovirus | 1 | 0,40% |
| Mixtas | 9 | 3,63% |
| Total | 139 | 56,05% |
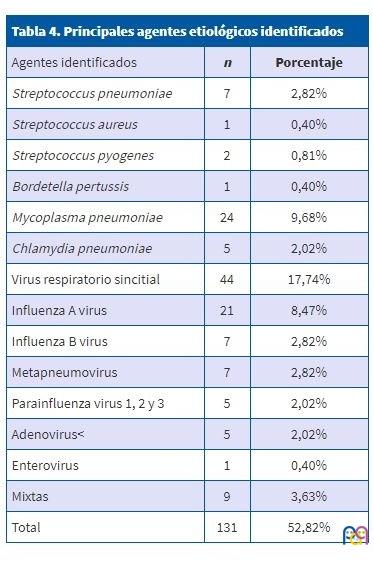
Es importante destacar el gran número de neumonías víricas diagnosticadas en menores de cuatro años (35,08%). También en este rango de edad se diagnosticó un número no desdeñable de neumonías atribuidas a M. pneumoniae (2,42%), siendo casi similar al grupo de mayores de cuatro años (4,03%), a diferencia de los patrones clásicamente descritos sobre la etiología. El germen que con más frecuencia se sospechó asociado a neumonía multifocal fue el neumococo (41,75%), seguido muy de cerca por los virus, con un 39,81%. A DP se asoció fundamentalmente neumococo y en menor proporción los virus. La afectación unifocal (9,03%) fue más frecuente en neumonías por M. pneumoniae que la multifocal (6,80%).
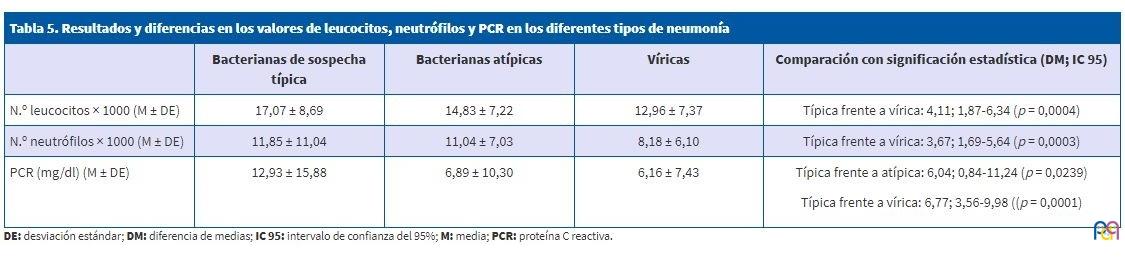
La leucocitosis y neutrofília fueron significativamente mayores en bacterianas típicas que en víricas (Tabla 5), mientras que la PCR fue significativamente más alta en las típicas que en el resto. A su vez, valores superiores a 10 mg/dl, se observaron en un 31,05% (IC 95: 25,62 a 37,06), de los cuales, el 62,34% fueron neumonías de posible origen neumocócico con mayores complicaciones.
| Tabla 5. Resultados y diferencias en los valores de leucocitos, neutrófilos y PCR en los diferentes tipos de neumonía | ||||
|---|---|---|---|---|
| Bacterianas de sospecha típica | Bacterianas atípicas | Víricas | Comparación con significación estadística (DM; IC 95) | |
| N.º leucocitos × 1000 (M ± DE) | 17,07 ± 8,69 | 14,83 ± 7,22 | 12,96 ± 7,37 | Típica frente a vírica: 4,11; 1,87-6,34 (p = 0,0004) |
| N.º neutrófilos × 1000 (M ± DE) | 11,85 ± 11,04 | 11,04 ± 7,03 | 8,18 ± 6,10 | Típica frente a vírica: 3,67; 1,69-5,64 (p = 0,0003) |
| PCR (mg/dl) (M ± DE) | 12,93 ± 15,88 | 6,89 ± 10,30 | 6,16 ± 7,43 |
Típica frente a atípica: 6,04; 0,84-11,24 (p = 0,0239) Típica frente a vírica: 6,77; 3,56-9,98 ((p = 0,0001) |
La mayoría de los pacientes hospitalizados recibieron inicialmente tratamiento antibiótico intravenoso (95,56%) (IC 95: 92,23 a 97,51). El 62,87% recibieron monoterapia con ampicilina, de los cuales un 6,04% no respondieron, teniendo que asociar o cambiar a otro antibiótico como amoxicilina-clavulánico o cefotaxima. Amoxicilina-clavulánico intravenoso se utilizó como primera opción en un 13,50% y cefotaxima en un 6,75%. Un 10,97% precisó asociar dos antibióticos simultáneamente. La duración media del tratamiento intravenoso fue de 4,6 ± 3,6 días. Las neumonías bacterianas típicas (6,30 ± 5,08 días) se relacionaron de forma significativa con más días de ingreso que las atípicas (4,78 ± 2,86 días): DM: 1,52 días; IC 95: 0,58 a 2,46 días; p = 0,0017, y que las víricas (4,97 ± 2,73 días): DM: 1,33 días; IC 95: 0,28 a 2,38 días; p = 0,0132.
Algunos de los ingresados recibieron tratamiento con antibiótico oral, siendo lo más frecuente azitromicina y amoxicilina. Destacamos que hasta un 5,91% (IC 95: 3,55 a 9,67) de los pacientes precisaron tratamiento broncodilatador y corticoideo al asociar bronquitis. El tiempo de hospitalización medio fue de 5,63 ± 4,12 días, con un máximo de hasta 27 días y más prolongado en aquellos pacientes con mayor hipoxemia y que requirieron drenaje quirúrgico del DP.
Al alta la mayoría de ellos continuó tratamiento antibiótico oral, siendo amoxicilina el más frecuente (56,54%), amoxicilina-clavulánico en el 37,97% y azitromicina en el 20,25%; solos o en asociación y una duración media de 5,6 ± 3,2 días.
DISCUSIÓN
Nuestro estudio recoge un total de 248 pacientes, coincidiendo con la mayoría de las publicaciones en que la NAC que precisa ingreso es más prevalente en menores de cinco años5,8, así como el aislamiento de virus en gran número de casos. En los meses de otoño, la mayoría de los casos fueron a expensas fundamentalmente de virus; sin embargo, las neumonías atípicas se diagnosticaron en los meses de invierno y otoño solo o en coinfección. Cabe destacar el porcentaje de pacientes con el antecedente de asma e HRB que precisaron hospitalización por neumonía vírica, del mismo modo que un gran número de pacientes presentaron bronconeumonía al diagnóstico, lo que obligó a asociar tratamiento broncodilatador a la antibioterapia. Estos datos corroboran la especial predisposición que presentan estos pacientes en padecer cuadros respiratorios de mayor gravedad y la mayoría relacionados con la edad menor de dos años.
En nuestro estudio se ha considerado la radiografía de tórax como gold standard para el diagnóstico de NAC, siendo necesario reseñar la dificultad que supone en algunos casos su interpretación en niños que asocian un proceso bronquial. No obstante, sigue siendo en la actualidad el único patrón de referencia para el diagnóstico de NAC admitido como tal.
Un dato importante, es cómo la edad se relacionó con el tipo de neumonía. De este modo, los pacientes de mayor edad se relacionaron más con neumonías bacteriana típicas que con víricas, y a su vez más con neumonías atípicas que típicas, apoyando la edad como mejor factor predictivo del tipo de neumonía.
En cuanto a los síntomas que presentaron los pacientes, los más frecuentes fueron la fiebre y la tos, siendo la duración de 72 horas de fiebre la que con más frecuencia se constató al diagnóstico. La temperatura máxima se dio con más frecuencia en neumonías víricas que en las bacterianas (típicas y atípicas). La duración media de la fiebre fue mayor en neumonías atípicas frente al resto de neumonías, lo que coincide con la mayoría de los estudios6-8.
Por otro lado, la ausencia de tos fue mayor en el grupo de neumonías atípicas, sin llegar a ser estadísticamente significativa, probablemente por el bajo número de casos de en los que se constató serología positiva a M. pneumoniae.
La AP fue normal hasta en un 18,55%, posiblemente esos pacientes llevaban menos tiempo de evolución del proceso infeccioso, siendo un dato concordante con lo publicado en la mayoría de las series6-9. Por otro lado, la taquipnea se ha considerado el signo más sensible y específico de neumonía en niños confirmada radiológicamente. Tal es así que, para algunos autores, la ausencia de taquipnea descarta la neumonía con alta probabilidad en menores de cinco años con fiebre y sobre todo en los menores de dos años1,6,9. En nuestros pacientes, entre aquellos que presentaban criterios de taquipnea (49%), en el 33%, la saturación de oxígeno fue menor o igual a 92% al diagnóstico. No hubo relación estadísticamente significativa con el tipo de neumonía, pero apareció con mayor frecuencia en las víricas y, aunque es un dato que se valora en cada paciente, el hecho de que no se registrase en unos 100 pacientes, limita las conclusiones sobre este dato.
Uno de los puntos de especial relevancia es el patrón radiológico encontrado en función del tipo de neumonía. El patrón intersticial apenas se observó en neumonías atípicas, siendo más frecuente en las neumonías víricas. El patrón alveolar fue el más encontrado y se relacionó con pacientes de mayor edad y con neumonías bacterianas frente al resto, fundamentalmente en las típicas. En cambio, el patrón alveolar no diferenció las neumonías típicas de las atípicas. Los virus presentaron un patrón intersticial y mixto en la mayoría de los pacientes.
Los parámetros analíticos mostraron cómo la PCR fue significativamente mayor en neumonías bacterianas típicas frente a atípicas y víricas, tal y como muestran estudios similares. Las cifras medias de leucocitos y neutrófilos mostraron diferencias relevantes para apoyar el diagnóstico diferencial entre las neumonías típicas bacterianas y las víricas, pero no con las atípicas, dato que apoya la mayor dificultad actual en la diferenciación de la infección por M. pneumoniae.
Cerca de un 96% de los pacientes recibió tratamiento antibiótico intravenoso, siguiendo las recomendaciones habituales de tratamiento de las NAC que requieren ingreso en pediatría1,2,6,7,12,13. El antibiótico inicial más utilizado fue ampicilina, seguido de amoxicilina-clavulánico y cefotaxima, acorde a los últimos protocolos publicados10,12,13. En un 6% de los casos se utilizó una cefalosporina (cefotaxima). Se ha advertido un uso elevado e injustificado de cefalosporinas de tercera generación en niños ingresados con NAC. Así, en un estudio multicéntrico español, se observó que hasta el 34% recibió esta antibioterapia empírica inicialmente13. Por otro lado, amoxicilina-clavulánico estaría indicado en pacientes mal vacunados frente a H. influenzae o en neumonías por gripe o, menos frecuente en niños, en neumonías por sospecha de aspiración, por lo que ha sido utilizado en nuestra serie con mayor frecuencia que la recomendada7 (13,50%). Se observó un mayor tiempo de estancia hospitalaria en pacientes con neumonía bacteriana típica frente al resto, en relación con las mayores complicaciones y edad de los pacientes.
Por otro lado, existen controversias sobre la necesidad de iniciar tratamiento antibiótico en niños pequeños que presentan clínica y exploración compatible con NAC junto a una radiología con patrón no alveolar, analítica inicialmente no sugerente de bacteriana y aislamiento de virus en el ANF. En este caso podría ser válida una actitud expectante sin iniciar tratamiento antibiótico1,6,12, aunque ninguno de los pacientes de nuestra serie siguió esta pauta.
Como ya sabemos, las NAC en los niños pueden estar producidas por un gran número de agentes etiológicos y determinar esos agentes es complicado con las técnicas habituales. En nuestro estudio se intentó determinar el agente etiológico en el caso de virus, bacterias atípicas y en ocasiones neumococo (siendo especialmente complicado en este caso). El más frecuentemente filiado fue VRS, dada la gran prevalencia de este germen en niños más pequeños y la posibilidad de asociar bronquiolitis con neumonías de mayor gravedad. Hubo cinco pacientes en los que detectaron gérmenes menos habituales de NAC, como son H. influenzae, S. aureus, S. pyogenes y Bordetella pertussis.
Estos resultados se encontrarían en la misma línea de diferentes estudios donde las neumonías víricas pueden llegar al 40%12 y entre 20-30% infección mixta bacteriana y viral.
En nuestro estudio, las neumonías mixtas fueron generalmente por coinfección de dos virus y su asociación con M. pneumoniae en tres casos y uno con neumococo. Hasta un 9,68% de los pacientes presentó infección por M. pneumoniae y un 2,02% por Chl. pneumoniae, cifra que está en aumento en la última década, sobre todo en menores de dos años, donde puede alcanzar el 20% en algunas series10. Nuestra cifra no es muy elevada en comparación con otras publicaciones, quizá por tratarse de neumonías con menor tendencia a complicarse e incluso por la dificultad de determinar analíticamente este germen por serología. La serología IgM puede ser negativa en un 50% casos (fundamentalmente en los primeros 10-14 días), teniendo un pico a las tres semanas y pudiendo persistir positiva durante 2-3 meses. En todos los rangos de edad, el neumococo es el germen posible más frecuente, principalmente en el rango de menores de dos años en nuestra serie.
Una de las principales limitaciones que tiene este estudio es la dificultad de determinar la etiología neumocócica en niños, ya que las muestras obtenidas a partir de ANF pueden resultar positivas simplemente por colonización y no por enfermedad, y por los falsos positivos en la prueba de antígeno en orina que en la infancia se dan en portadores sanos en nasofaringe y en niños con vacunación reciente. Cabe recordar que la neumonía neumocócica es en pocos casos responsable de bacteriemia, por lo que el hemocultivo es una herramienta poco útil para perfilar la etiología. Por eso, en este estudio se ha asumido un diagnóstico de probable etiología neumocócica en los de clínica y radiografía compatible negativos a M. pneumoniae y otras bacterias y virus.
En nuestro estudio, la NAC por VRS se produjo en un 17,74% de los casos, siendo el intervalo de edad predominante el de menores de dos años. Sin embargo, dada la limitación de las pruebas diagnósticas disponibles en nuestro medio para niños, fundamentalmente para determinar neumococo, los resultados deben ser interpretados con cautela.
A pesar de incluirse en el estudio un alto número de casos, tiene otras limitaciones, como es la dificultad de conseguir los datos completos, al ser obtenidos de forma retrospectiva a partir de historias clínicas. Una de las más importantes sería la de establecer el diagnóstico etiológico a nivel hospitalario que refleja la realidad diaria, donde se establece el tratamiento inicial empíricamente en función de las recomendaciones y guías más actuales en nuestro entorno, basándose fundamentalmente en la edad del paciente la clínica y la imagen radiológica.
En conclusión, el diagnóstico inicial del tipo de neumonía sigue siendo un reto diagnóstico en Pediatría, tanto en Atención Primaria como en Hospitalaria. No existe un parámetro clínico ni radiológico que nos guíe con precisión hacia el agente etiológico, demostrándose cada vez con más claridad, lo poco ajustados a la realidad que están los clásicos patrones de neumonía neumocócica como típica y prácticamente el resto las atípicas.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
ANF: resultado del aspirado nasofaríngeo · AP: auscultación pulmonar · DE: desviación estándar · DM: diferencia de medias · DP: derrame pleural · FR: frecuencia respiratoria · HRB: hiperreactividad bronquial · IC 95: intervalo de confianza del 95% · IF: inmunofluorescencia · NAC: neumonía adquirida en la comunidad · OMS: Organización Mundial de la Salud · OR: odds ratio · PCR: proteína C reactiva · VRS: virus respiratorio sincitial.
BIBLIOGRAFÍA
- Úbeda Sansano MI, Murcia García J, Asensi Monzó MT; Grupo de Vías Respiratorias. Neumonía adquirida en la comunidad. El pediatra de Atención Primaria y la Neumonía. Protocolo del GVR (publicación P-GVR-8). En: Respirar [consultado el 17/02/2020]. Disponible en www.respirar.org/images/protocolo-neumonia-2017.pdf
- Giménez Sánchez F, Sánchez Marenco A, Battles Garrido JM, López Soler JA, Sánchez-Solís Querol M. Características clínico-epidemiológicas de la neumonía adquirida en la comunidad en niños menores de 6 años. An Pediatr (Barc). 2007;66:578-84.
- Clark JE, Hammal D, Hamptom F, Spencer D, Parker L. Epidemiology of community-acquired pneumonia in children seen in hospital. Epidemiol Infect. 2007;135:262-9.
- Neuman MI, Graham D, Bachur R. Variation in the use of chest radiography for pneumonia in pediatric emergency departments. Pediatr Emerg Care. 2011;27:606-10.
- Rudan I, O'Brien KL, Nair H, Liu L, Theodoratou E, Qazi S, et al. Epidemiology and etiology of childhood pneumonia in 2010: estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J Glob Health. 2013;3:010401.
- Harris M, Clark J, Coote N, Fletcher P, Harnden A, McKean M, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. 2011;66 Suppl 2:ii1-23.
- Andrés Martín A, Asensio de la Cruz O, Pérez Pérez G. Complicaciones de la neumonía adquirida en la comunidad: derrame pleural, neumonía necrotizante, absceso pulmonar y pioneumotórax. Protoc diagn ter pediatr. 2017;1:127-46.
- Andrés Martín A, Moreno-Pérez D, Alfayate Miguélez S, Couceiro Gianzo JA, García García ML, Korta Murua J, et al. Etiología y diagnóstico de la neumonía adquirida en la comunidad y sus formas complicadas. An Pediatr (Barc). 2012;76:162.e1-e18.
- The management of acute respiratory infections in children: practical guidelines for outpatient care. En: Organización Mundial de la Salud [en línea] [consultado el 17/02/2020]. Disponible en https://apps.who.int/iris/handle/10665/41803
- Baer G, Engelcke G, Abele-Horn M, Schaad UB, Heininger U. Role of Chlamydia pneumoniae and Mycoplasma pneumoniae as causative agents of community-acquired pneumonia in hospitalised children and adolescents. Eur J Clin Microbiol Infect Dis. 2003;22:742-5.
- Palafox M, Guiscafre H, Reyes H, Munoz O, Martínez H. Diagnostic value of tachypnoea in pneumonia defined radiologically. Arch Dis Child. 2000;82:41-5.
- Don M, Canciani M, Korppi M. Community-acquired pneumonia in children: what’s old? What’s new? Acta Paediatr. 2010;99:1602-8.
- Borrás C, Novell C, Hernández Bou S, García García JJ. Prescripción antibiótica en los pacientes hospitalizados desde Urgencias. Estudio multicéntrico. An Pediatr (Barc). 2013;79:15-20.