
Vol. 21 - Num. 84
Originales
Patrones de sueño de los niños sanos a los cuatro años: factores sociales y estilos de crianza
Clara M.ª Aymerich de Franchescia, Clara Miguel Miguelb, M.ª Luisa Arroba Basantac, Celina Arana Cañedo-Argüellesd, Luisa Cabello Ballesterose
aSección de Gastroenterología, Hepatología y Nutrición Pediátrica. Hospital Universitario 12 de Octubre. Madrid. España.
bEstudiante de Medicina. Universidad Complutense de Madrid. Madrid. España.
cDepartamento de Salud Pública y Materno-Infantil. Universidad Complutense de Madrid. Pediatra. CS Pozuelo-Emisora. Pozuelo de Alarcón. Madrid. España.
dPediatra. CS Paseo Imperial. Madrid. España.
eTécnico de Salud. Unidad Docente Multiprofesional de Atención Familiar y Comunitaria Noroeste. Madrid. España.
Correspondencia: ML Arroba. Correo electrónico: mlarroba@ucm.es
Cómo citar este artículo: Aymerich de Franchesci CM, Miguel Miguel C, Arroba Basanta ML, Arana Cañedo-Argüelles C, Cabello Ballesteros L. Patrones de sueño de los niños sanos a los cuatro años: factores sociales y estilos de crianza. Rev Pediatr Aten Primaria. 2019;21:343-56.
Publicado en Internet: 31-10-2019 - Número de visitas: 30688
Resumen
Introducción: estudio descriptivo transversal mediante un cuestionario en las consultas de Pediatría de Atención Primaria en centros de salud, cuyo objetivo es describir el patrón de sueño en los niños de cuatro años, nacidos a término, en dos zonas urbanas de la Comunidad de Madrid, y estudiar posibles asociaciones con diversas variables: antecedentes de crianza y hábitos del sueño, factores socioeconómicos y familiares.
Material y métodos: se ha estudiado a 193 niños, de los cuales 111 (57,8%) presentaron un test de cribado alterado. Un 94,9% duerme nueve o más horas nocturnas. Dentro de los antecedentes de crianza, un 89,6% ha recibido lactancia materna y el 51,8% la ha mantenido más de seis meses. El 28,5% de los padres realizó colecho. En el momento actual, el 51% comparte habitación con hermanos, mientras que el 9,9% duerme con los padres. El 57,8% utiliza aparatos electrónicos como inductores del sueño.
Resultados: se ha encontrado un mayor porcentaje de posibles alteraciones del sueño en niños que son hijos únicos, no asistieron a guardería, duermen con los padres en el momento actual, realizan colecho reactivo y utilizan aparatos electrónicos después de cenar.
Conclusiones: se concluye que la prevalencia de signos de alarma de un trastorno del sueño es alta, y dadas las implicaciones a largo plazo de estos problemas, es importante tener un protocolo de cribado adecuado para identificar a los niños con posibles alteraciones. Conocer las asociaciones estudiadas podría permitir al pediatra realizar una labor educativa con las familias susceptibles, para prevenir o solucionar estas alteraciones.
Palabras clave
● Crianza ● Encuestas y cuestionarios ● SueñoINTRODUCCIÓN
Las dificultades para dormir de los niños son motivo de consulta frecuente en las consultas de Pediatría de Atención Primaria, y generan angustia en los padres. Entre los tres y cinco años, los niños duermen entre 10 y 12 horas diarias y se consideran normales las siestas hasta los 3-4 años1. Se calcula que el 30% de los niños menores de cinco años tienen algún tipo de alteración del sueño1. Esta gran prevalencia se explica porque incluye tanto las patologías como los problemas del sueño1, patrones de sueño insatisfactorios para los padres, el niño o el pediatra, sin que haya alteración de la función fisiológica que controla el sueño1 y por tanto, apreciaciones subjetivas influidas por la cultura2,3: un estudio de 2010 refleja que los padres de niños asiáticos son más propensos a pensar que sus hijos tienen dificultades a la hora de irse a la cama y que duermen peor en comparación con familias caucásicas4.
La falta de sueño afecta al comportamiento, el estado de ánimo y las funciones cognitivas1. Se ha estimado que el 10% de las dificultades de aprendizaje en la infancia se deben a la fatiga diurna5,6. También se relaciona con obesidad y resistencia a la insulina7; cambios de 30 minutos en la duración del sueño pueden tener impacto sobre la salud8.
Múltiples artículos analizan las alteraciones del sueño, pero son escasos los estudios que valoran el sueño en niños sanos y los factores relacionados9. Se han realizado estudios en gemelos, donde se observa una mayor influencia de los factores ambientales que de los genéticos1,2. Se han sugerido como factores determinantes que facilitan la adquisición de malos hábitos actitudes demasiado permisivas o estrictas de los padres, el amamantamiento prolongado como inductor del sueño o el colecho reactivo1,10. Parece que los niños a los que se les permite realizar un colecho reactivo se van a la cama más tarde, tienen despertares nocturnos más tardíos y una menor duración del sueño que los niños que duermen solos1,10. Otro factor que se debe tener en cuenta es el uso de dispositivos electrónicos: en Italia se realizó un estudio que estimaba que el 39,1% de los niños de entre uno y tres años los utilizan antes de ir a dormir1,5. Este tipo de uso reduce la duración total del sueño unas 0,25 horas, debido a una disminución de los niveles de melatonina por la exposición a la luz que estos generan5; también se relacionan con irregularidad en la hora de acostarse11.
Respecto a la relación con el contexto sociocultural, un estudio en niños británicos de tres años observó mejor higiene y horarios de sueño en familias de clase social alta2. Estas medidas repercuten en una mayor duración del sueño nocturno, pero no en su duración total, ya que puede compensarse con la siesta2,5. Un estudio realizado con 29 287 niños asiáticos y caucásicos describe diferencias en los hábitos de sueño y en la percepción parental de los problemas, según la procedencia4. Si se compara población blanca y negra en el mismo lugar de residencia (sur de Misisipí), parece que la duración del sueño nocturno es menor en los niños de raza negra que en los de raza blanca, pero que los primeros duermen más durante el día12.
La zona de residencia es otro factor que hay que considerar. En un estudio realizado en EE. UU. se vio que la duración del sueño de los niños de áreas urbanas era menor que los de áreas no urbanas13.
La cultura y el ambiente son importantes para poder comprender y evaluar la duración y el patrón del sueño14, pero hay pocos estudios realizados en población residente en España.
En cuanto a los trastornos del sueño, la influencia ambiental destaca como causa del insomnio conductual o por higiene de sueño inadecuada. En él influye en gran medida el modelo familiar, como por ejemplo la falta continua de uno de los progenitores, relaciones maternofiliales conflictivas y madres jóvenes con síntomas depresivos1,2,15. Existen otros trastornos de sueño cuya etiopatogenia es más compleja, con menor influencia ambiental y mayor influencia de factores biológicos como la carga genética, las alteraciones del ritmo circadiano y otros factores asociados al sexo y la edad1.
El objetivo principal de este estudio es describir el patrón de sueño en los niños de cuatro años, nacidos a término, en dos zonas urbanas de la Comunidad de Madrid, y estudiar posibles asociaciones con diversas variables: antecedentes de crianza y hábitos del sueño, factores socioeconómicos y familiares.
Este trabajo se justifica por la ausencia de datos globales y bibliográficos sobre los temas objeto de estudio, además de la importante prevalencia de las alteraciones de sueño y su gran impacto sobre la población pediátrica y sus familias. Conocer los factores asociados a las alteraciones de sueño puede permitir identificar los grupos de riesgo y realizar una prevención eficaz.
MATERIAL Y MÉTODOS
Estudio observacional descriptivo en el ámbito de Atención Primaria: centros de salud (CS) Paseo Imperial y Pozuelo Estación de la Comunidad de Madrid (España).
La población de estudio fueron los niños, de cuatro años cumplidos y menores de cinco, que acudieron a las consultas de dichos centros, cumplían los criterios de inclusión y no los de exclusión, y aceptaron participar hasta completar el tamaño muestral.
Se definieron como:
- Criterios de inclusión: niños de ambos sexos nacidos a término pertenecientes a los CS Pozuelo Estación y Paseo Imperial; menores de cinco años, que tengan cuatro años cumplidos en el momento del estudio y que acudan a las consultas de Pediatría por cualquier motivo; que cualquiera de los padres acepte participar en el estudio.
- Criterios de exclusión: antecedentes de prematuridad; niños con alteración del neurodesarrollo; necesidad de medicación que pueda alterar o interferir con la maduración normal del sueño (antiepilépticos y melatonina); niños adoptados; niño que acuda a consulta con una persona distinta a su padre o su madre; dificultad idiomática.
El tamaño de la muestra se decidió en función de un nivel de confianza del 95%, una precisión del 7% y una prevalencia esperada de algún signo de alteración de sueño del 50% (asumiendo el peor caso posible: p = 0,5), se precisan para ello 196 pacientes aproximadamente.
Se recogieron las siguientes variables:
- Universales y relacionadas con el nivel socioeconómico de la familia: sexo del niño; zona geográfica de procedencia de la madre y del padre; edad de la madre y del padre en el momento actual (en años); nivel de estudios de la madre y del padre; situación laboral de la madre y del padre en el momento actual; estructura familiar; número de hijos en el momento actual; características de la fratria y posición en ella.
- Variables relacionadas con los antecedentes personales, de crianza y hábitos de sueño: lactancia materna; duración de la lactancia materna (en meses); hasta qué edad ha dormido en la habitación de los padres; en qué lugar dormía en la habitación de los padres; tipo de habitación del niño en el momento actual; método para dormir cuando era bebé; edad hasta la que ha dormido siestas (en años); asistencia a guardería; duerme en la cama de los padres al menos una parte de la noche; utilización de aparatos electrónicos (televisión, tableta, móvil…) después de cenar; lectura antes de dormir; necesidad de compañía de padres para dormirse.
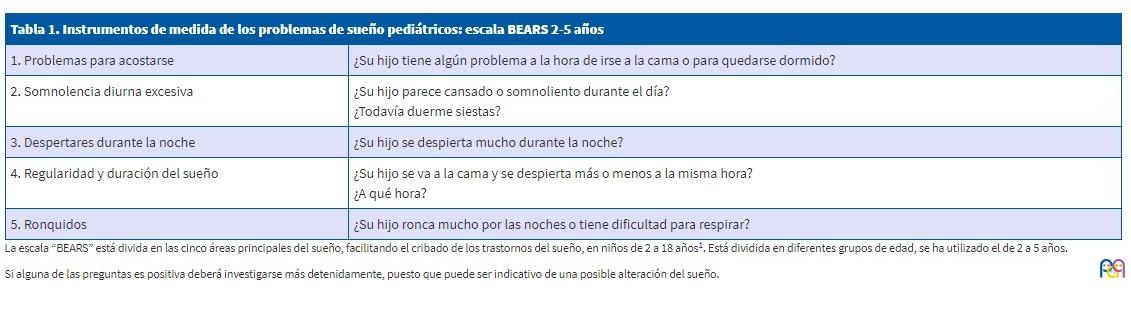
- Variables principales: cribado de alteraciones de sueño mediante el cuestionario Bedtime problems, Excessive daytime sleepiness, Awakenings during the night, Regularity and duration of sleep, Snoring (BEARS), validado en castellano (Tabla 1); duración del sueño nocturno actual.
| Tabla 1. Instrumentos de medida de los problemas de sueño pediátricos: escala BEARS 2-5 años | |
|---|---|
| 1. Problemas para acostarse | ¿Su hijo tiene algún problema a la hora de irse a la cama o para quedarse dormido? |
| 2. Somnolencia diurna excesiva | ¿Su hijo parece cansado o somnoliento durante el día? ¿Todavía duerme siestas? |
| 3. Despertares durante la noche | ¿Su hijo se despierta mucho durante la noche? |
| 4. Regularidad y duración del sueño | ¿Su hijo se va a la cama y se despierta más o menos a la misma hora? ¿A qué hora? |
| 5. Ronquidos | ¿Su hijo ronca mucho por las noches o tiene dificultad para respirar? |
Previamente a la recogida de datos se realizó un cuestionario piloto para valorar su compresibilidad y adecuación.
Las variables se almacenaron en una base de datos y se han analizado mediante el paquete estadístico SPSS versión 21. Se ha realizado el estudio descriptivo de todas las variables para detectar valores anómalos u otras inconsistencias. Las variables se describen mediante los estadísticos más apropiados a su naturaleza, tipo y escala de medida: análisis porcentual para las variables cualitativas, mientras que las variables cuantitativas se presentan a través de medidas de centralización y dispersión según proceda. Para el análisis bivariable se ha utilizado la prueba de χ2 o el test exacto de Fisher para las variables cualitativas y comparación de medianas para las variables cuantitativas. Para todas las pruebas se ha aceptado un valor de significación del 5%.
Aspectos éticos. Consentimiento informado
En las bases de datos no se ha incluido información que pueda identificar directa o indirectamente a los participantes en el estudio.
A todos los participantes se les informó sobre los objetivos del proyecto y la identidad de los investigadores (estudiantes de medicina) y se les solicitó su participación. El cuestionario era anónimo y en ningún momento se accedió a la historia clínica para recoger datos personales o clínicos.
Las estudiantes estuvieron en todo momento tutorizadas por el médico pediatra responsable de la consulta (Orden SSI/81/2017 de 19 de enero: asegurar y proteger el derecho a la intimidad del paciente por los alumnos y residentes en ciencias de la salud). Los cuestionarios fueron entregados y revisados por el propio pediatra del niño.
Se han respetado las normas internacionales de protección de datos, así como la legislación española vigente (Ley Orgánica 15/1999 del 13/12/99 de Protección de Datos de Carácter Personal, BOE 298 de 14/12/99). Este trabajo cuenta con el informe favorable del Comité Ético de Investigación Clínica del Hospital Clínico San Carlos (código interno: 17/450-E_TFG) y de la Comisión Local de Investigación Noroeste de la Gerencia Asistencial de Atención Primaria del Servicio Madrileño de Salud (código de proyecto: 06/2017).
RESULTADOS
Análisis descriptivo de la muestra estudiada
Se ha estudiado a 193 niños (100 hombres y 92 mujeres) pertenecientes a los CS Paseo Imperial (52,3%) y Pozuelo Estación (47,7%).
La mediana de edad de las madres es de 39 años (23-49 años) y la de los padres de 40 años (24-61 años), sin que se observen diferencias estadísticamente significativas entre la población de ambos CS.
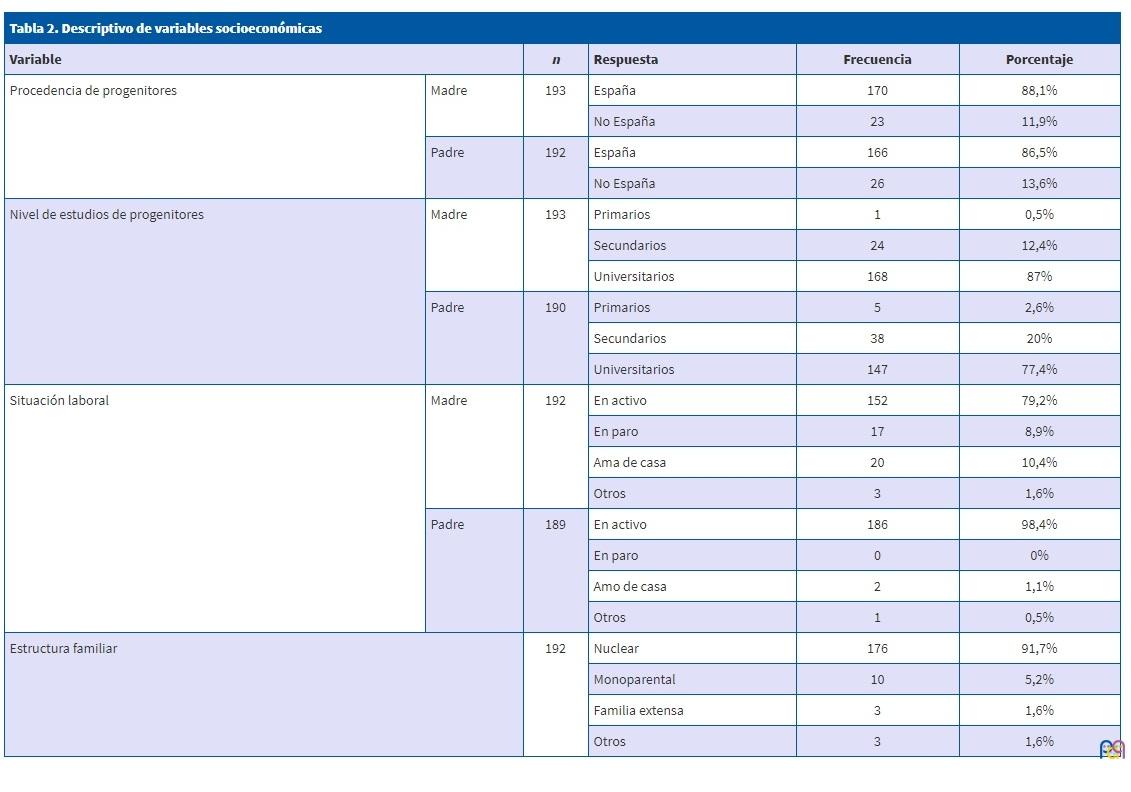
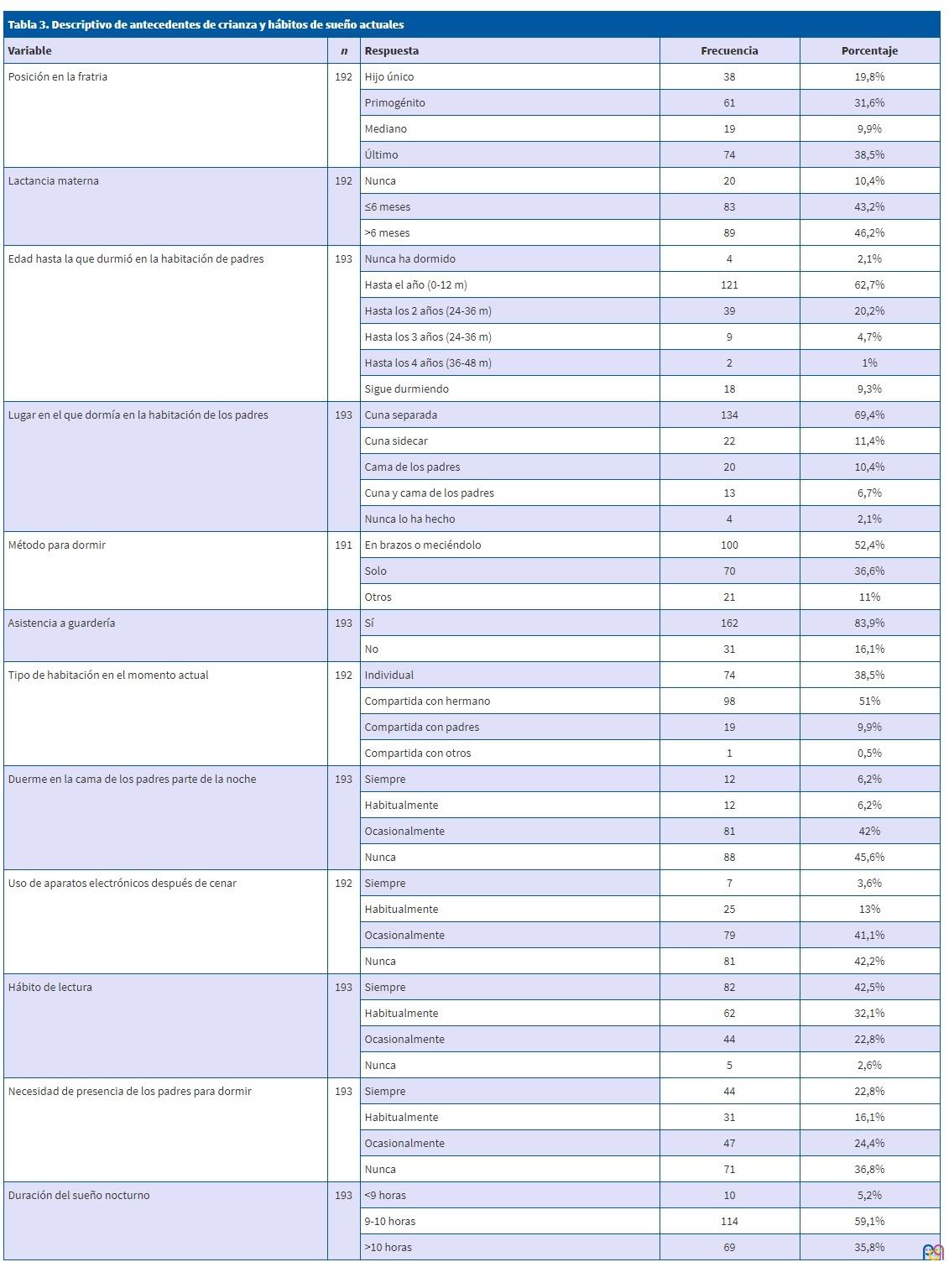
Los resultados de las variables cualitativas se recogen en las Tablas 2 y 3.
| Tabla 2. Descriptivo de variables socioeconómicas | |||||
|---|---|---|---|---|---|
| Variable | n | Respuesta | Frecuencia | Porcentaje | |
| Procedencia de progenitores | Madre | 193 | España | 170 | 88,1% |
| No España | 23 | 11,9% | |||
| Padre | 192 | España | 166 | 86,5% | |
| No España | 26 | 13,6% | |||
| Nivel de estudios de progenitores | Madre | 193 | Primarios | 1 | 0,5% |
| Secundarios | 24 | 12,4% | |||
| Universitarios | 168 | 87% | |||
| Padre | 190 | Primarios | 5 | 2,6% | |
| Secundarios | 38 | 20% | |||
| Universitarios | 147 | 77,4% | |||
| Situación laboral | Madre | 192 | En activo | 152 | 79,2% |
| En paro | 17 | 8,9% | |||
| Ama de casa | 20 | 10,4% | |||
| Otros | 3 | 1,6% | |||
| Padre | 189 | En activo | 186 | 98,4% | |
| En paro | 0 | 0% | |||
| Amo de casa | 2 | 1,1% | |||
| Otros | 1 | 0,5% | |||
| Estructura familiar | 192 | Nuclear | 176 | 91,7% | |
| Monoparental | 10 | 5,2% | |||
| Familia extensa | 3 | 1,6% | |||
| Otros | 3 | 1,6% | |||
| Tabla 3. Descriptivo de antecedentes de crianza y hábitos de sueño actuales | ||||
|---|---|---|---|---|
| Variable | n | Respuesta | Frecuencia | Porcentaje |
| Posición en la fratria | 192 | Hijo único | 38 | 19,8% |
| Primogénito | 61 | 31,6% | ||
| Mediano | 19 | 9,9% | ||
| Último | 74 | 38,5% | ||
| Lactancia materna | 192 | Nunca | 20 | 10,4% |
| ≤6 meses | 83 | 43,2% | ||
| >6 meses | 89 | 46,2% | ||
| Edad hasta la que durmió en la habitación de padres | 193 | Nunca ha dormido | 4 | 2,1% |
| Hasta el año (0-12 m) | 121 | 62,7% | ||
| Hasta los 2 años (24-36 m) | 39 | 20,2% | ||
| Hasta los 3 años (24-36 m) | 9 | 4,7% | ||
| Hasta los 4 años (36-48 m) | 2 | 1% | ||
| Sigue durmiendo | 18 | 9,3% | ||
| Lugar en el que dormía en la habitación de los padres | 193 | Cuna separada | 134 | 69,4% |
| Cuna sidecar | 22 | 11,4% | ||
| Cama de los padres | 20 | 10,4% | ||
| Cuna y cama de los padres | 13 | 6,7% | ||
| Nunca lo ha hecho | 4 | 2,1% | ||
| Método para dormir | 191 | En brazos o meciéndolo | 100 | 52,4% |
| Solo | 70 | 36,6% | ||
| Otros | 21 | 11% | ||
| Asistencia a guardería | 193 | Sí | 162 | 83,9% |
| No | 31 | 16,1% | ||
| Tipo de habitación en el momento actual | 192 | Individual | 74 | 38,5% |
| Compartida con hermano | 98 | 51% | ||
| Compartida con padres | 19 | 9,9% | ||
| Compartida con otros | 1 | 0,5% | ||
| Duerme en la cama de los padres parte de la noche | 193 | Siempre | 12 | 6,2% |
| Habitualmente | 12 | 6,2% | ||
| Ocasionalmente | 81 | 42% | ||
| Nunca | 88 | 45,6% | ||
| Uso de aparatos electrónicos después de cenar | 192 | Siempre | 7 | 3,6% |
| Habitualmente | 25 | 13% | ||
| Ocasionalmente | 79 | 41,1% | ||
| Nunca | 81 | 42,2% | ||
| Hábito de lectura | 193 | Siempre | 82 | 42,5% |
| Habitualmente | 62 | 32,1% | ||
| Ocasionalmente | 44 | 22,8% | ||
| Nunca | 5 | 2,6% | ||
| Necesidad de presencia de los padres para dormir | 193 | Siempre | 44 | 22,8% |
| Habitualmente | 31 | 16,1% | ||
| Ocasionalmente | 47 | 24,4% | ||
| Nunca | 71 | 36,8% | ||
| Duración del sueño nocturno | 193 | <9 horas | 10 | 5,2% |
| 9-10 horas | 114 | 59,1% | ||
| >10 horas | 69 | 35,8% | ||
Respecto a las características socioeconómicas, la población es mayoritariamente española (87,3%), con estudios universitarios y en activo. La estructura familiar más común es la nuclear (91,7%). El 20,7% de las familias tienen un único hijo, el 53,4% dos hijos, el 18,1% tres hijos, y el 6,4% tienen cuatro o más.
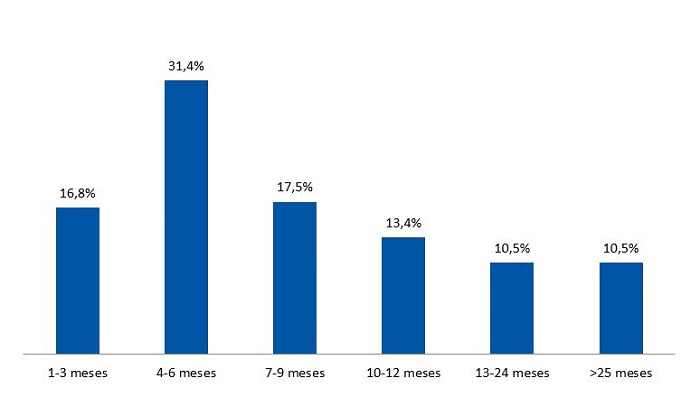
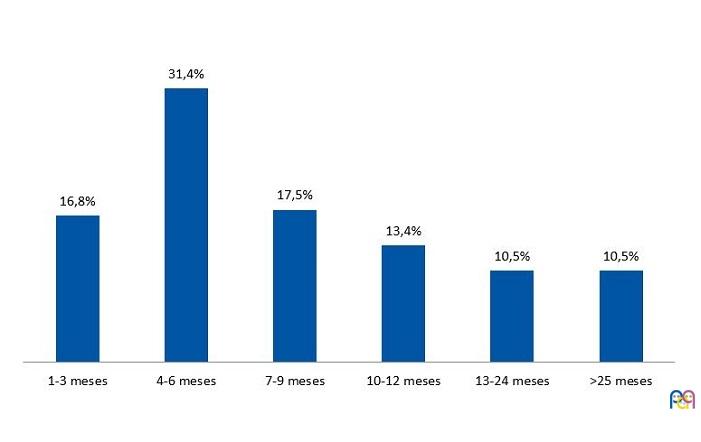
En relación con los antecedentes de crianza, el 89,6% ha recibido lactancia materna; y el 51,8% la ha mantenido más de seis meses (Fig. 1). La mayoría de los niños ha dormido en cuna separada dentro de la habitación de los padres los primeros años (69,4%), y el 28,5% de los padres realizó colecho. En cuanto al método empleado para dormir, el 52,2% de los niños se dormían en brazos o mecidos, mientras que el 36,6% se dormían solos. El 83,9% ha asistido a guardería.
| Figura 1. Duración de la lactancia materna |
|---|
 |
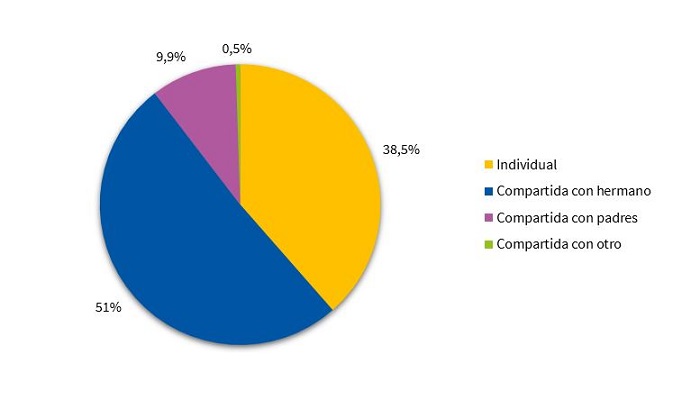
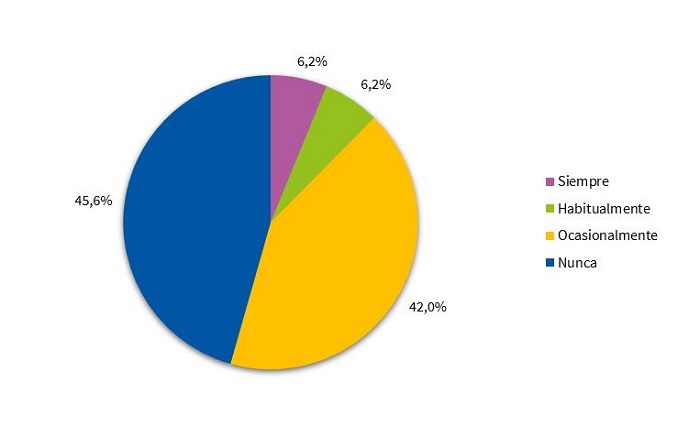
Si se analizan los hábitos de sueño actuales, la mayoría de los niños comparte habitación con algún hermano (51%). Un 9,9% sigue durmiendo en la habitación de los padres (Fig. 2). El 45,6% nunca va a la cama de los padres durante la noche, mientras que el 42% lo hace ocasionalmente (Fig. 3).
| Figura 2. Habitación actual |
|---|
 |

| Figura 3. Duermen en la cama de los padres parte de la noche |
|---|
 |
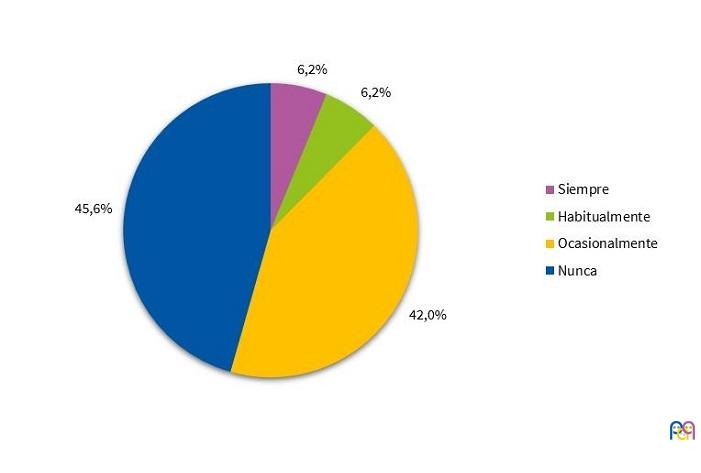
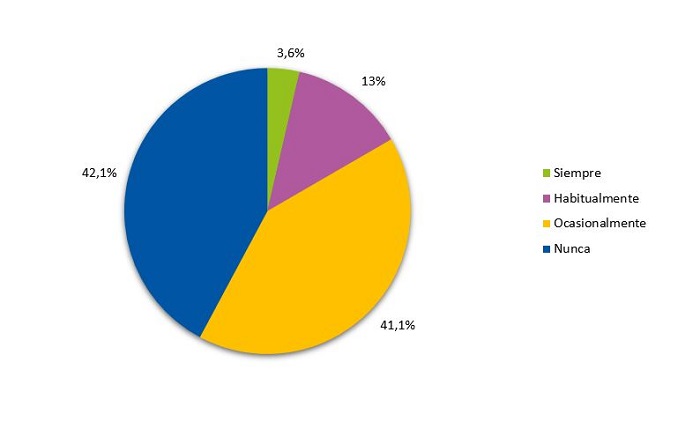
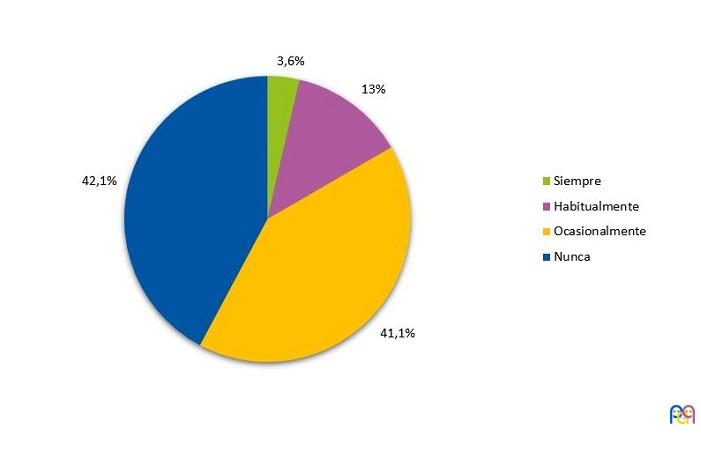
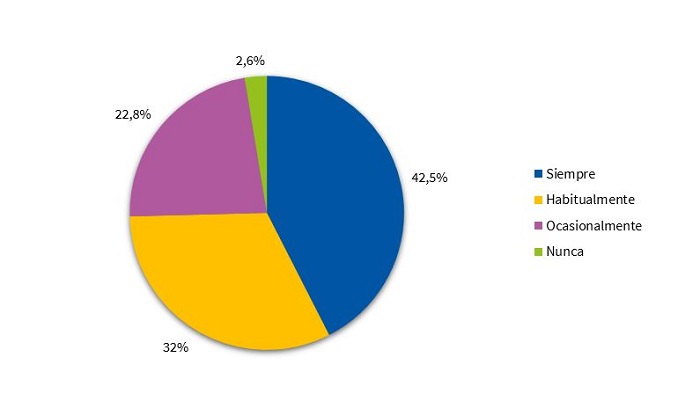
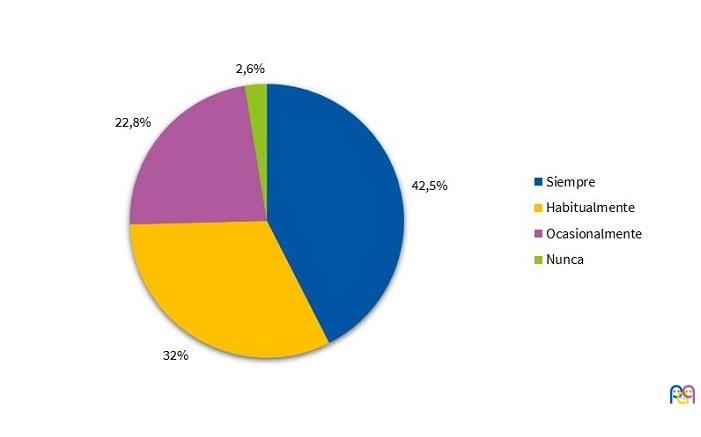
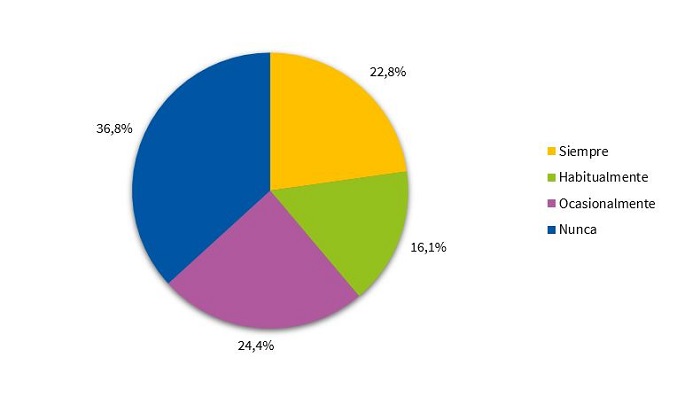
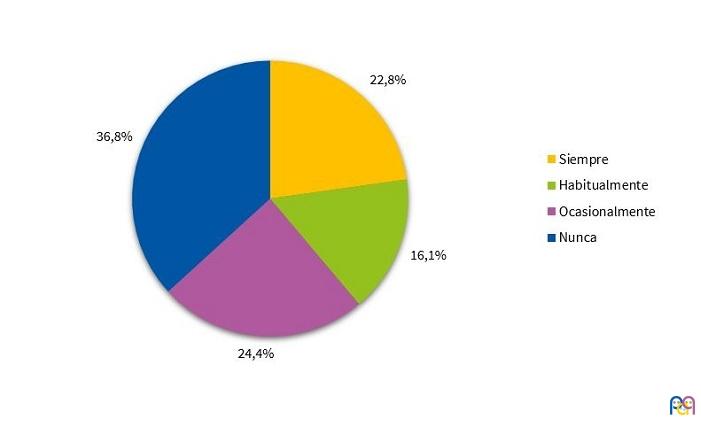
En lo relativo a la inducción del sueño, el 57,8% de los niños utiliza aparatos electrónicos después de cenar de forma ocasional, habitual o siempre (Fig. 4). La mayoría de los niños lee siempre antes de dormir (42,5%) (Fig. 5). El 36,8% no necesita la presencia de los padres para dormir (Fig. 6). El 37,5% de los niños sigue durmiendo siestas.
| Figura 4. Uso de aparatos electrónicos |
|---|
 |
| Figura 5. Hábito de lectura |
|---|
 |
| Figura 6. Necesidad de la presencia de los padres para dormir |
|---|
 |
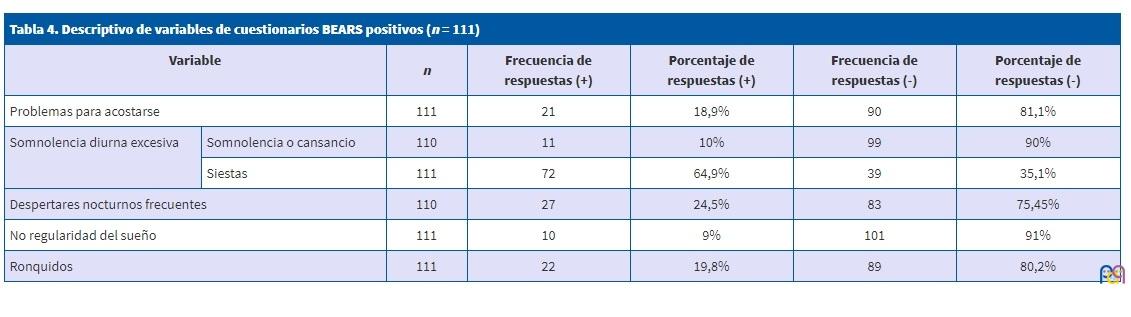
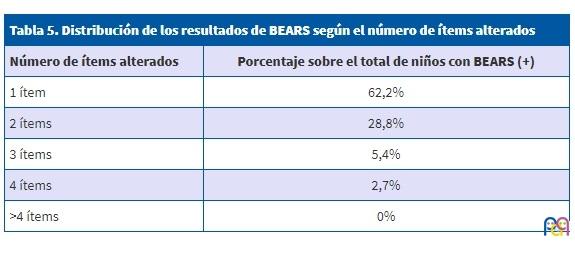
En cuanto al patrón de sueño en el momento actual, el 57,8% de los niños estudiados tienen un BEARS positivo, indicativo de una posible alteración del sueño. Se han recogido las frecuencias de respuestas positivas en cada ámbito en la Tabla 4. De los niños con BEARS positivo, tienen un único ítem alterado el 62,2%, debido mayoritariamente a la persistencia de siestas (Tabla 5). Se ha observado que la prevalencia de BEARS positivos si se excluyen los casos que se deben únicamente a la persistencia de siestas, es de un 37,71%.
| Tabla 4. Descriptivo de variables de cuestionarios BEARS positivos (n = 111) | ||||||
|---|---|---|---|---|---|---|
| Variable | n | Frecuencia de respuestas (+) | Porcentaje de respuestas (+) | Frecuencia de respuestas (-) | Porcentaje de respuestas (-) | |
| Problemas para acostarse | 111 | 21 | 18,9% | 90 | 81,1% | |
| Somnolencia diurna excesiva | Somnolencia o cansancio | 110 | 11 | 10% | 99 | 90% |
| Siestas | 111 | 72 | 64,9% | 39 | 35,1% | |
| Despertares nocturnos frecuentes | 110 | 27 | 24,5% | 83 | 75,45% | |
| No regularidad del sueño | 111 | 10 | 9% | 101 | 91% | |
| Ronquidos | 111 | 22 | 19,8% | 89 | 80,2% | |
| Tabla 5. Distribución de los resultados de BEARS según el número de ítems alterados | |
|---|---|
| Número de ítems alterados | Porcentaje sobre el total de niños con BEARS (+) |
| 1 ítem | 62,2% |
| 2 ítems | 28,8% |
| 3 ítems | 5,4% |
| 4 ítems | 2,7% |
| >4 ítems | 0% |
Respecto a la duración del sueño nocturno, el 59,1% duerme entre nueve y diez horas; el 35,8% duerme más de diez, y el 5,2% duerme menos de nueve.
Análisis de las variables en función del BEARS
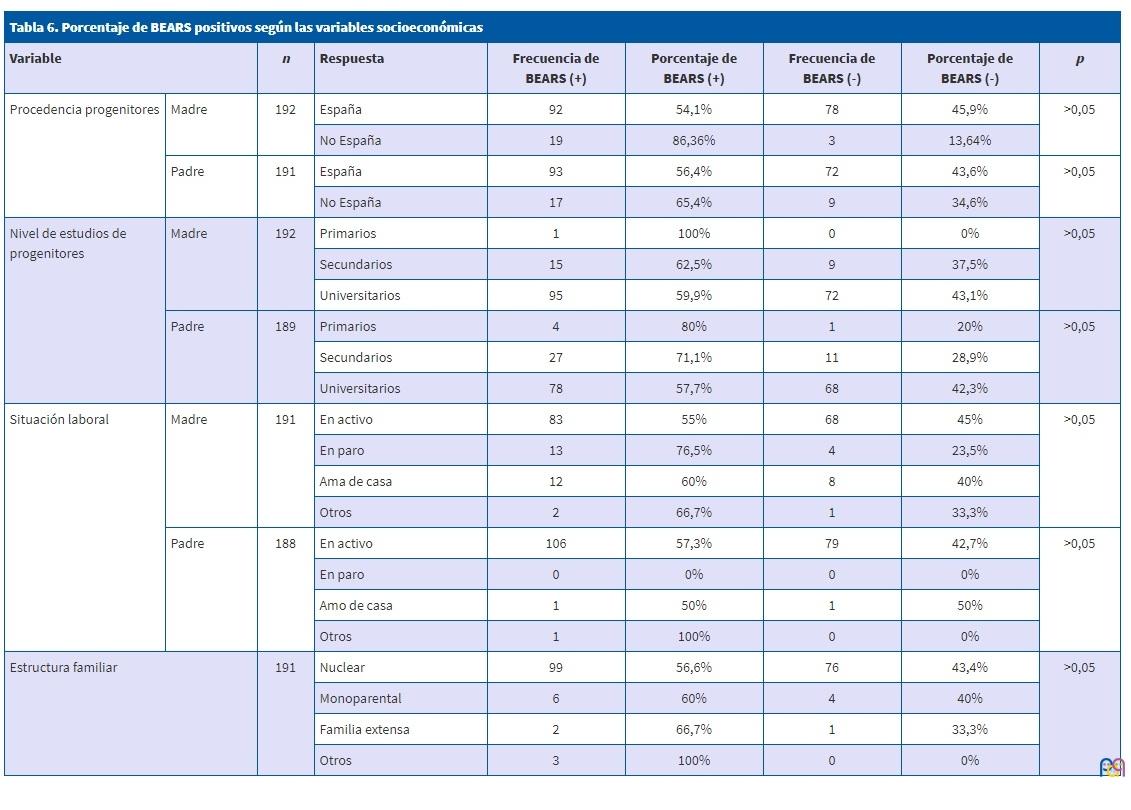
Al analizar la relación entre las distintas variables y el sueño de los niños a los cuatro años, se ha observado que existe mayor porcentaje de niños con BEARS positivo entre aquellos que: son hijos únicos (84,2%); siguen durmiendo en la habitación de los padres (70,6%); no asistieron a guardería (67,7%); comparten actualmente habitación con los padres (73,7%) o duermen en habitación individual (65,8%); duermen habitualmente en la cama de los padres (75%); utilizan siempre aparatos electrónicos después de cenar (85,7%); necesitan siempre la compañía de los padres para dormir (68,2%); tienen progenitores con menor nivel de estudios; tienen madres en paro (76,5%) (Tablas 6 y 7).
| Tabla 6. Porcentaje de BEARS positivos según las variables socioeconómicas | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variable | n | Respuesta | Frecuencia de BEARS (+) | Porcentaje de BEARS (+) | Frecuencia de BEARS (-) | Porcentaje de BEARS (-) | p | |
| Procedencia progenitores | Madre | 192 | España | 92 | 54,1% | 78 | 45,9% | >0,05 |
| No España | 19 | 86,36% | 3 | 13,64% | ||||
| Padre | 191 | España | 93 | 56,4% | 72 | 43,6% | >0,05 | |
| No España | 17 | 65,4% | 9 | 34,6% | ||||
| Nivel de estudios de progenitores | Madre | 192 | Primarios | 1 | 100% | 0 | 0% | >0,05 |
| Secundarios | 15 | 62,5% | 9 | 37,5% | ||||
| Universitarios | 95 | 59,9% | 72 | 43,1% | ||||
| Padre | 189 | Primarios | 4 | 80% | 1 | 20% | >0,05 | |
| Secundarios | 27 | 71,1% | 11 | 28,9% | ||||
| Universitarios | 78 | 57,7% | 68 | 42,3% | ||||
| Situación laboral | Madre | 191 | En activo | 83 | 55% | 68 | 45% | >0,05 |
| En paro | 13 | 76,5% | 4 | 23,5% | ||||
| Ama de casa | 12 | 60% | 8 | 40% | ||||
| Otros | 2 | 66,7% | 1 | 33,3% | ||||
| Padre | 188 | En activo | 106 | 57,3% | 79 | 42,7% | >0,05 | |
| En paro | 0 | 0% | 0 | 0% | ||||
| Amo de casa | 1 | 50% | 1 | 50% | ||||
| Otros | 1 | 100% | 0 | 0% | ||||
| Estructura familiar | 191 | Nuclear | 99 | 56,6% | 76 | 43,4% | >0,05 | |
| Monoparental | 6 | 60% | 4 | 40% | ||||
| Familia extensa | 2 | 66,7% | 1 | 33,3% | ||||
| Otros | 3 | 100% | 0 | 0% | ||||
| Tabla 7. Porcentaje de BEARS positivo según los antecedentes de crianza y hábitos de sueño | |||||||
|---|---|---|---|---|---|---|---|
| Variable | n | Respuesta | Frecuencia de BEARS (+) | Porcentaje de BEARS (+) | Frecuencia de BEARS (-) | Porcentaje de BEARS (-) | P |
| Posición en la fratria | 191 | Hijo único | 32 | 84,2% | 6 | 15,8% | 0,002 |
| Primogénito | 33 | 54,1% | 28 | 45,9% | |||
| Mediano | 11 | 57,9% | 8 | 42,1% | |||
| Último | 34 | 46,6% | 39 | 53,4% | |||
| Lactancia materna | 191 | Nunca | 12 | 60% | 8 | 40% | >0,05 |
| ≤6 meses | 48 | 57,8% | 35 | 42,2% | |||
| >6 meses | 50 | 56,8% | 38 | 43,2% | |||
| Edad hasta la que durmió en la habitación de padres | 192 | Nunca ha dormido | 1 | 25% | 3 | 75 | >0,05 |
| Hasta el año | 70 | 57,9% | 51 | 42,1% | |||
| Hasta los 2 años | 20 | 51,3% | 19 | 48,7% | |||
| Hasta los 3 años | 6 | 66,7% | 3 | 33,3% | |||
| Hasta los 4 años | 2 | 100% | 0 | 0% | |||
| Sigue durmiendo | 12 | 70,6% | 5 | 29,4% | |||
| Lugar en el que dormía en la habitación de los padres | 192 | Cuna separada | 77 | 57,5% | 57 | 42,5% | >0,05 |
| Cuna sidecar | 14 | 66,7% | 4 | 33,3% | |||
| Cama de los padres | 12 | 60% | 8 | 40% | |||
| Cuna y cama de los padres | 7 | 53,8% | 6 | 46,2% | |||
| Nunca lo ha hecho | 1 | 25% | 3 | 75% | |||
| Método para dormir | 190 | En brazos o meciéndolo | 56 | 56,6% | 43 | 43,4% | >0,05 |
| Solo | 43 | 61,4% | 27 | 38,6% | |||
| Otros | 10 | 47,6% | 11 | 52,4% | |||
| Asistencia a guardería | 192 | Sí | 90 | 55,9% | 71 | 44,1% | >0,05 |
| No | 21 | 67,7% | 10 | 32,3% | |||
| Tipo de habitación en el momento actual | 191 | Individual | 48 | 65,8% | 25 | 34,2% | 0,052 |
| Compartida con hermano | 48 | 49% | 50 | 51% | |||
| Compartida con padres | 14 | 73,7% | 5 | 26,3% | |||
| Compartida con otros | 1 | 100% | 0 | 0% | |||
| Duerme en la cama de los padres parte de la noche | 192 | Siempre | 7 | 58,3% | 5 | 41,7% | >0,05 |
| Habitualmente | 9 | 75% | 3 | 25% | |||
| Ocasionalmente | 51 | 63% | 30 | 37% | |||
| Nunca | 44 | 50,6% | 43 | 49,4% | |||
| Uso de aparatos electrónicos | 191 | Siempre | 6 | 85,7% | 1 | 14,3% | >0,05 |
| Habitualmente | 15 | 60% | 10 | 40% | |||
| Ocasionalmente | 46 | 58,2% | 33 | 41,8% | |||
| Nunca | 44 | 55% | 36 | 45% | |||
| Hábito de lectura | 192 | Siempre | 46 | 56,8% | 35 | 43,2% | >0,05 |
| Habitualmente | 37 | 59,7% | 25 | 40,3% | |||
| Ocasionalmente | 25 | 56,8% | 19 | 43,2% | |||
| Nunca | 3 | 60% | 2 | 40% | |||
| Necesidad de presencia de los padres para dormir | 192 | Siempre | 30 | 68,2% | 14 | 31,8% | >0,05 |
| Habitualmente | 15 | 48,4% | 16 | 51,6% | |||
| Ocasionalmente | 24 | 52,2% | 22 | 47,8% | |||
| Nunca | 42 | 59,2% | 29 | 40,8% | |||
| Duración del sueño nocturno | 192 | <9 horas | 7 | 70% | 3 | 30% | 0,051 |
| 9-10 horas | 72 | 63,7% | 41 | 36,3% | |||
| >10 horas | 32 | 46,4% | 37 | 53,6% | |||
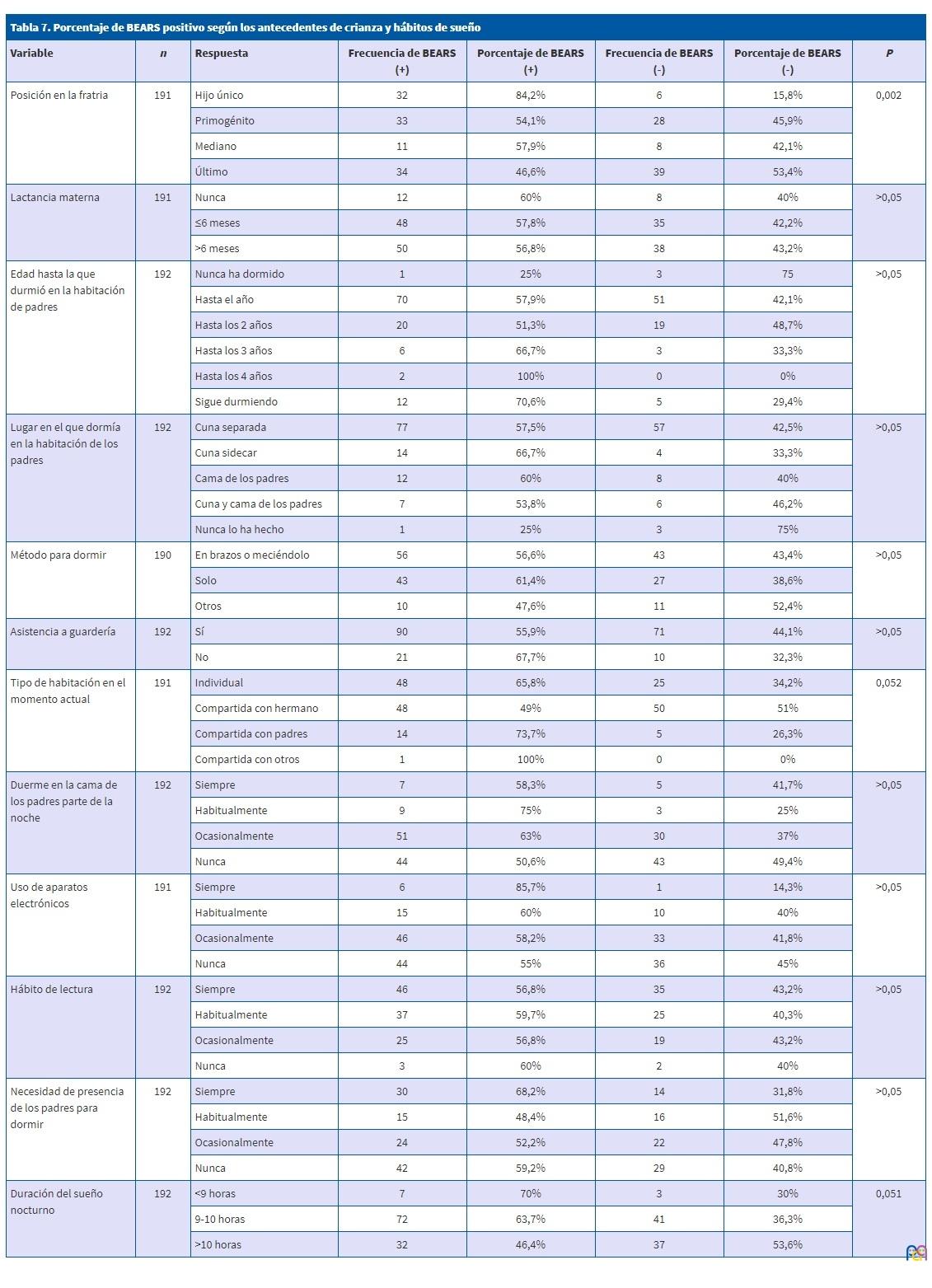
Se han encontrado diferencias estadísticamente significativas entre los niños que son hijos únicos y aquellos que tienen hermanos respecto al número de resultados positivos en el BEARS (p = 0,002).
En cuanto a la duración del sueño nocturno, tienen BEARS positivo el 70% de los niños que duermen menos de nueve horas; el 63,7% de los que duermen de nueve a diez horas y el 46,4% de los que duermen más de diez horas (p = 0,05).
No se ha observado asociación entre la duración de lactancia materna, el lugar donde dormían los primeros meses de vida, el método utilizado para dormir, el hábito de lectura, la estructura familiar o la edad de los padres, y los resultados del BEARS.
DISCUSIÓN
El sueño normal en niños sanos de cuatro años se compone de un periodo nocturno de aproximadamente diez horas, que se pueden complementar con siestas diurnas. Según estudios previos, el 10% de los niños duerme más de 12 horas, y un 10% menos de 9,5 horas16. Este trabajo estudia el patrón de sueño habitual en niños de cuatro años de dos CS de Madrid mediante una prueba de cribado validada. Se ha elegido el cuestionario BEARS por ser breve, amplio y fácil de usar en el contexto de Atención Primaria. Ha sido utilizado en numerosos estudios e investigaciones en lengua inglesa, pero hay pocos trabajos publicados que utilicen la traducción española, recomendada por las guías1,17. Bastida-Pozuelo y Sánchez-Ortuño realizaron un estudio para comprobar su validez comparándola con el Children’s Sleep Habits Questionnaire (CSHQ), que es el test de referencia; concluyeron que la traducción española del BEARS es un test válido para detectar los problemas de sueño en niños y adolescentes18. Se ha descartado el uso del CSHQ por su excesiva duración y complejidad, y la falta de puntos de corte entre lo patológico y lo normal.
Según la Guía de Práctica Clínica, las alteraciones del sueño tienen una prevalencia del 30%1, y su importancia radica en sus consecuencias sobre el niño y su familia a largo plazo. En este estudio se ha observado una prevalencia del 57,8% de resultados positivos en el BEARS, que constituyen un signo de alarma por tratarse de una prueba de cribado, pero no significan necesariamente la presencia de alteraciones de sueño. Así, un resultado positivo se debe individualizar en la consulta, mediante una valoración integral del niño y su familia.
En cuanto a la población estudiada, es en su mayoría española con nivel sociocultural alto, con estructura familiar nuclear y tienen dos o más hijos. Esto es ligeramente superior a los datos de natalidad y fecundidad del Instituto Nacional de Estadística19 (número medio de hijos por mujer: 1,33).
Se trata de una muestra homogénea, por lo que los resultados se pueden aplicar principalmente a grupos poblacionales con características socioculturales similares. Se ha observado una asociación inversa entre el nivel de estudios alcanzado por los progenitores y las alteraciones del sueño. La situación laboral precaria, considerando el paro como un agente estresante en la familia, también se relaciona con un mayor porcentaje de alteraciones. Estos resultados se asemejan a los obtenidos en estudios previos2.
Llama la atención la alta prevalencia de lactancia materna en la muestra (89,6% globalmente y 51,8% con una duración superior a seis meses) en contraposición con los datos que refleja la ENSE 2011/12 (72,2% a las seis semanas y 46,9% a los seis meses)20. En estudios previos se ha relacionado el amamantamiento de larga duración con un aumento en las alteraciones del sueño1, pero los resultados obtenidos no muestran diferencias significativas en función de la presencia o no de lactancia materna, ni según su duración mayor o menor de seis meses.
Otro dato que destaca es que el 28,5% de las familias ha realizado colecho espontáneo, no secundario a problemas socioeconómicos o de la vivienda. Se entiende por colecho que el niño duerma habitualmente en la misma superficie que sus padres. No existen datos oficiales sobre su prevalencia en España, pero en un estudio reciente en dos CS de Madrid con 317 niños, se ha obtenido una prevalencia de colecho del 31,86%21. Es importante remarcar que no se ha observado asociación entre el colecho espontáneo durante los primeros meses de vida y alteraciones de sueño a los cuatro años.
En cuanto a la evolución del sueño desde esos primeros años de vida hasta los cuatro años, la mayoría de los niños abandonan la habitación de los padres, y pasan a compartir habitación con hermanos o a una individual. Llama la atención que un 9,9% de los niños continúa durmiendo en la habitación de los padres a los cuatro años. Esto tiene especial relevancia, ya que se ha observado un mayor porcentaje de BEARS positivos en este grupo de niños (73,7%) y en aquellos que están solos en la habitación (65,8%), en contraste con aquellos que duermen con hermanos (49%). Estos datos podrían aplicarse desde las consultas de Atención Primaria, para fomentar el traslado de los niños a habitaciones con hermanos si es posible, tanto para prevenir como para intentar solucionar patrones del sueño alterados.
Se ha observado una mayor prevalencia de alteraciones en niños que van habitualmente a la cama de los padres durante la noche y que necesitan su compañía para dormir; ambos hechos pueden considerarse indicadores de colecho reactivo. Estos resultados son acordes a los obtenidos en estudios previos1,10.
Se ha encontrado que los hijos únicos tienen más alteraciones del sueño (p = 0,002). A pesar de que es un factor aparentemente no modificable, conocer su relación con las alteraciones del sueño permite al pediatra identificar estas familias, fomentar en ellas un estilo educativo favorecedor de la autonomía del niño y reforzar a los padres para que se sientan seguros en la crianza.
Uno de los aspectos más estudiados previamente es el uso de aparatos electrónicos en la infancia, por la alarma social que genera la adicción a las pantallas. Se ha observado que el 57,8% de la muestra los utiliza como inductor del sueño, en contraposición al 39,1% de prevalencia que señalan estudios en otros países5. Las sociedades científicas pediátricas22 recomiendan limitar el uso de pantallas a menos de una hora diaria en niños mayores de dos años, y evitarlas en la hora previa a acostarse. La alta prevalencia encontrada en la muestra debe ser motivo de intervención por parte de los pediatras, ya que se ha encontrado un mayor porcentaje de pruebas de cribado patológicas en aquellos niños que los utilizan de forma habitual (85,7%), de forma similar a estudios existentes5,11.
En cuanto a la duración del sueño nocturno, se aconseja que los niños de cuatro años duerman de 10 a 12 horas diarias1. Lo más habitual es que el periodo nocturno sea de aproximadamente diez horas. complementadas con siestas diurnas16. Las horas de sueño nocturno de los niños del estudio están en el límite inferior de las recomendaciones: el 94,9% duerme nueve o más horas nocturnas. La duración total del sueño diario sin embargo puede estar compensada por la persistencia de siestas en el 37,5%.
A pesar de que el cuestionario empleado (BEARS) considera indicativo de alteración la presencia de siestas en este grupo de edad, se consideran recomendables hasta los cinco años1. En los casos en los que el BEARS positivo se deba únicamente a las siestas, el pediatra debe averiguar mediante la anamnesis si estas siestas se integran adecuadamente en la rutina del niño o si generan problemas en el colegio o la familia, distinguiendo así los casos que sean realmente patológicos. Se ha analizado la prevalencia de alteraciones de sueño excluyendo los casos que se deben exclusivamente a la persistencia de siestas y se observa un 37,71% de niños con BEARS positivo, lo cual se asemeja a estudios previos1.
La relevancia de este estudio se basa en poder identificar tanto factores ambientales sobre los que actuar como aquellos que, siendo no modificables, se asocian a alteraciones de sueño. Actualmente, las familias muestran una gran preocupación en cuanto a utilizar el mejor modo de crianza posible con sus hijos, y transmiten estas dudas a sus pediatras. Los resultados de este estudio apoyan la utilidad para el pediatra del cribado de los signos de alarma de los problemas de sueño como herramienta para establecer medidas preventivas (orientar a los padres en sus decisiones sobre la crianza, fomentar que los niños tengan un horario de sueño regular y suficiente, evitar el uso de aparatos electrónicos en edades tan tempranas, etc.).
Es importante recalcar que el resto de los factores modificables parecen tener una menor influencia en el patrón de sueño, como son la lectura o el método usado para dormir.
A la hora de plantear nuevos estudios sobre este tema, se deben valorar las limitaciones que se han encontrado en este trabajo. En primer lugar, a pesar de tratarse de una muestra de 193 pacientes de dos áreas sanitarias distintas, la población es homogénea en ciertos aspectos (estructura familiar, procedencia, situación laboral, edad de los progenitores, etc.), por lo que no se han podido estudiar ciertas asociaciones con el patrón del sueño. También se ha de valorar la existencia de sesgo de memoria, ya que en el cuestionario se incluyen aspectos de los primeros años de vida, que pueden recordar mejor los padres de hijos con problemas de sueño.
CONCLUSIÓN
Se ha observado una alta prevalencia de niños con una prueba de cribado BEARS positiva, lo que tiene gran importancia durante la práctica pediátrica en Atención Primaria por las implicaciones que puede tener un trastorno de sueño en el niño a largo plazo. Es recomendable plantear el desarrollo de protocolos de cribado adecuados para identificar a los niños susceptibles.
Se han observado escasas relaciones entre los antecedentes de crianza y el patrón de sueño a los cuatro años. No se han observado diferencias según el tipo y duración de la lactancia y el colecho espontáneo.
El pediatra debe respetar el estilo de crianza de los padres y fomentar las medidas educativas que favorezcan la autonomía del niño, pero evitar hacer recomendaciones sobre modificar el tiempo de lactancia o el colecho espontáneo con el objetivo de mejorar el patrón de sueño futuro del niño. Se debe sin embargo desaconsejar el uso de aparatos electrónicos en la infancia, ya que se ha observado que su uso es muy superior a los límites recomendados por las asociaciones pediátricas.
CONFLICTO DE INTERESES
Las autoras declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
BEARS: Bedtime problems, Excessive daytime sleepiness, Awakenings during the night, Regularity and duration of sleep, Snoring · CS: centro de salud · CSHQ: Children’s Sleep Habits Questionnaire.
BIBLIOGRAFÍA
- Grupo de trabajo de la Guía de Práctica Clínica sobre Trastornos del Sueño en la Infancia y Adolescencia en Atención Primaria. Guía de Práctica Clínica sobre Trastornos del Sueño en la Infancia y Adolescencia en Atención Primaria. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad. Unidad de Evaluación de Tecnologías Sanitarias de la Agencia Laín Entralgo; 2011. Guías de Práctica Clínica en el SNS: UETS n.º 2009/8. Disponible en https://portal.guiasalud.es/wp-content/uploads/2018/12/GPC_489_Trastorno_sue%D0%B4o_infadol_Lain_Entr_compl.pdf
- Jones C, Ball H. Exploring socioeconomic differences in bedtime behaviours and sleep duration in English preschool children. Inf Child Dev. 2014;23:518-31.
- Owens JA. Behavioral sleep problems in children. En: UpToDate [en línea] [consultado el 29/10/2019]. Disponible en www.uptodate.com/contents/behavioral-sleep-problems-in-children
- Mindell JA, Sadeh A, Kwon R, Goh DYT. Cross-cultural differences in sleep of preschool children. Sleep Med. 2013;14:1283-9.
- Brambilla P, Giussani M, Pasinato A, Venturelli L, Privitera F, Miraglia Del Giudice E, et al. Sleep habits and pattern in 1-14 years old children and relationship with video devices use and evening and night child activities. Ital J Pediatr. 2017;43:7.
- Pin Arboledas G, Cubel Alarcon M, Martín González G, Lluch Rosello A, Morell Salort M. Hábitos y problemas con el sueño de los 6 a los 14 años en la Comunidad Valenciana. Opinión de los propios niños. An Pediatr (Barc). 2011;74:103-15.
- Matthews KA, Pantesco EJM. Sleep characteristics and cardiovascular risk in children and adolescents: an enumerative review. Sleep Med. 2016;18:36-49.
- Sadeh A, Gruber R, Raviv A. The effects of sleep restriction and extension on school-age children: what a difference an hour makes. Child Dev. 2003;74:444-55.
- Galland BC, Mitchell EA. Helping children sleep. Arch Dis Child. 2010;95:850-3.
- Li S, Jin X, Yan C, Wu S, Jiang F, Shen X. Bed- and room-sharing in Chinese school-aged children: Prevalence and association with sleep behaviors. Sleep Med. 2008;9:555-63.
- Magee CA, Lee JK, Vella SA. Bidirectional relationships between sleep duration and screen time in early childhood. JAMA Pediatr. 2014;168:465-70.
- Crosby B, LeBourgeois MK, Harsh J. Racial differences in reported napping and nocturnal sleep in 2-to 8-year-old children. Pediatrics. 2005;115:225-32.
- Botino CJ, Rifas-Shiman SL, Kleinman KP, Oken E, Redline S, Gold D, et al. The association of urbanicity with infant sleep duration. Health Place. 2012;18:1000-5.
- Bathory E, Tomopoulos S. Sleep regulation, physiology and development, sleep duration and patterns, and sleep hygiene in infants, toddlers, and preschool-age children. Curr Probl Pediatr Adolesc Health Care. 2017;47:29-42.
- Pascual M, Estivill E, Albares J. Trastornos del sueño en la infancia. An Pediatr Contin. 2007;5:302-7.
- Pin G, Ugarte R. Lo que el pediatra de Atención Primaria debería saber sobre el sueño. Rev Pediatr Aten Primaria. 2010;12:s219-s230.
- Pin G, Ugarte R. Taller de sueño infantil. Herramientas para su interpretación por el pediatra de Atención Primaria. Rev Pediatr Aten Primaria. 2009;11:s399-s404.
- Bastida-Pozuelo MF, Sánchez-Ortuño MM. Preliminary analysis of the concurrent validity of the Spanish translation of the BEARS sleep screening tool for children. J Psychiatr Ment Health Nurs. 2016;23:513-20.
- España en cifras 2017. En: Instituto Nacional de Estadística [en línea] [consultado el 29/10/2019]. Disponible en www.ine.es/prodyser/espa_cifras/2017/index.html#1
- Encuesta Nacional de Salud de España 2011/12. Resultados detallados nacionales y por comunidades autónomas. En: Ministerio de Sanidad, Servicios Sociales e Igualdad. Portal Estadístico del SNS [en línea] [consultado el 29/10/2019]. Disponible en www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2011/encuestaResDetall2011.htm
- Martín Martín R, Sánchez Bayle M, Teruel de Francisco MC. El colecho en nuestro medio: estudio de casos y controles en las consultas pediátricas de Atención Primaria. Rev Pediatr Aten Primaria. 2017;19:15-21.
- AAP Council on Communications and Media. Media and young minds. Pediatrics. 2016;138:e20162591.