

Test para la detección temprana de las dificultades en el aprendizaje de la lectura y escritura
Fernando Cuetosa, P Suárez-Coallab, M. I Molinac, M. C Llenderrozasd
aDepartamento de Psicología. Universidad de Oviedo. España.
bDepartamento de Psicología, Universidad de Oviedo. España.
cPediatra. CS de Durango. Vizcaya. España.
dEnfermera Pediátrica. CS de Durango. Vizcaya. España.
Correspondencia: F Cuetos. Correo electrónico: fcuetos@uniovi.es
Cómo citar este artículo: Cuetos F, Suárez-Coalla P, Molina MI, Llenderrozas MC. Test para la detección temprana de las dificultades en el aprendizaje de la lectura y escritura. Rev Pediatr Aten Primaria. 2015;17:e99-e107.
Publicado en Internet: 18-06-2015 - Número de visitas: 201685
Resumen
Introducción: el diagnóstico de la dislexia se suele producir varios años después de que se inicie el aprendizaje de la lectoescritura. Para entonces muchos niños disléxicos ya saben lo que es el fracaso escolar y la pérdida de autoestima. Con un diagnóstico temprano se pueden evitar muchos de esos problemas. Además los programas de intervención son mucho más eficaces cuanto más tempranamente se apliquen.
Objetivos: el objetivo de este estudio fue elaborar una prueba de diagnóstico precoz de la dislexia, basada en los déficits de procesamiento fonológico que presentan estos niños, aplicable a los cuatro años de edad, antes de que se enfrenten a la lectura.
Material y métodos: la prueba consta de seis subtareas con cinco ítems cada una que se puede pasar entre seis y diez minutos. Las seis subtareas evalúan los principales componentes del procesamiento fonológico: discriminación de fonemas, segmentación de sílabas, identificación de fonemas, repetición de pseudopalabras, memoria verbal a corto plazo y fluidez verbal.
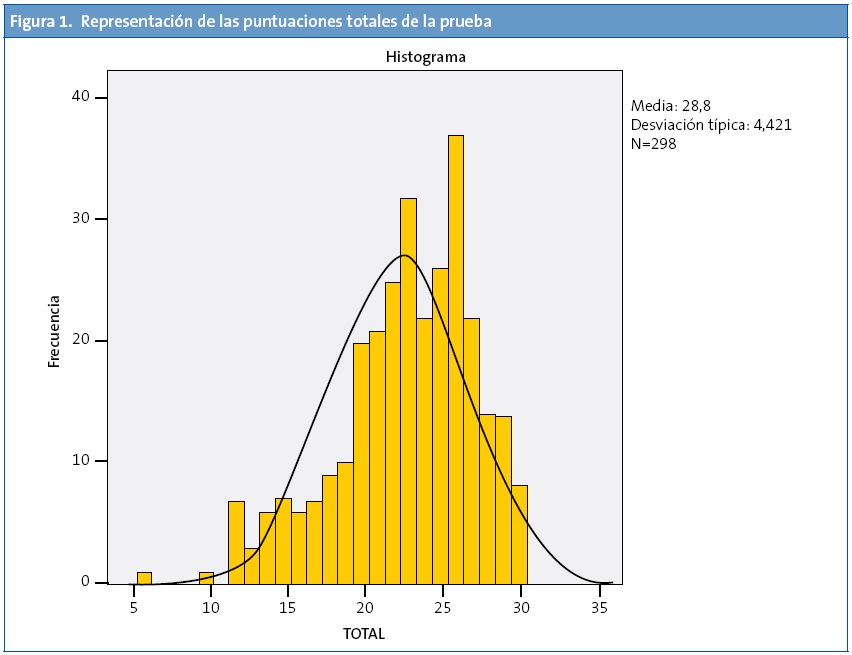
Resultados: los datos obtenidos de una muestra de 298 niños de cuatro años muestran una buena fiabilidad y una alta validez de constructo de la prueba. Se proporcionan valores normativos en percentiles y puntos de corte por debajo de los cuales se consideran niños de riesgo de sufrir una dislexia.
Conclusiones: la aplicación de esta sencilla prueba en las consultas pediátricas y en las clases de Educación infantil a los niños de cuatro años de edad permitirá detectar aquellos con riesgo de sufrir dislexia para poder intervenir lo más tempranamente posible, antes de se enfrenten al aprendizaje de la lectorescritura.
Palabras clave
● Dislexia ● Procesamiento Fonológico ● Test de prevenciónINTRODUCCIÓN
El aprendizaje de la lectoescritura es uno de los principales retos a los que se tienen que enfrentar los niños durante los primeros años de la escolaridad. La mayor parte logran superarlo sin demasiadas dificultades, pero hay un porcentaje importante que presentan serios problemas de aprendizaje, lo que probablemente les conduzca al fracaso escolar, ya que la mayor parte de los contenidos escolares se aprenden a través de la lectura1. En algunos casos se trata de un simple retraso lector producido por problemas familiares, escasa motivación, etc., en otros de un trastorno disléxico de origen neurobiológico. Aunque se han dado estimaciones muy variables de los porcentajes de dislexia, algunos autores hablan de un 17% de casos2. En español, por tener un sistema ortográfico muy transparente, se estima que los porcentajes se encuentran entre el 3 y el 4%3,4.
Generalmente la dislexia se detecta varios años después de iniciado el aprendizaje de la lectura y escritura, cuando los niños, a pesar de tener capacidades cognitivas normales, un entorno familiar y escolar favorables, además de esforzarse por aprender, no terminan de adquirir esas destrezas. Eso conlleva un retraso en el desarrollo escolar con respecto a sus compañeros, y lo que es peor, una pérdida considerable de autoestima. Cuanto más tiempo pasa para ponerle remedio más difícil es la recuperación, ya que por una parte los niños van perdiendo motivación y cada vez sienten menos atracción por la lectura, y por otra el cerebro va perdiendo plasticidad. De hecho, cuando se detectan tempranamente los trastornos disléxicos los resultados de la intervención son mucho más efectivos5,6.
La cuestión es cómo se puede predecir la posible existencia de trastornos de lectura lo más temprano posible, pues obviamente, hasta que el niño no ha iniciado el aprendizaje y hayan pasado varios años sin conseguirlo no se puede hablar de dislexia. Pero para entonces ya se ha perdido un tiempo precioso en el que los tratamientos hubiesen sido muy efectivos. Lo ideal sería comenzar a una edad temprana, antes incluso del inicio del proceso de enseñanza sistemática de la lectura. En ese caso sería necesario conocer los factores predictores de la lectura, es decir, saber si los niños disléxicos presentan alguna alteración responsable de sus problemas para aprender a leer y escribir.
Numerosos estudios realizados en las últimas décadas apuntan, sin ninguna duda, hacia el procesamiento fonológico7-9. Contar con un buen procesamiento fonológico es fundamental para aprender a leer y escribir, ya que la lectura consiste en transformar grafemas o letras en fonemas y la escritura en transformar fonemas en letras. De manera que si un niño no discrimina bien los fonemas, no es capaz de segmentar el habla en unidades menores como las sílabas y fonemas, o no es capaz de retener varios fonemas en su memoria mientras lee o escribe una palabra, sin duda tendrá dificultades para aprender a leer y escribir. De hecho, todos los niños disléxicos tienen dificultades en el procesamiento fonológico. De acuerdo con esto, la definición aportada por la Asociación Internacional de Dislexia (2002) dice textualmente que "la dislexia es una dificultad específica de aprendizaje, de origen neurobiológico, que se caracteriza por dificultades en el reconocimiento preciso y fluido de las palabras y por problemas de ortografía y descodificación. Esas dificultades resultan de un déficit en el componente fonológico"10.
En este sentido, hay varios tipos de evidencias empíricas que apoyan la relación causal entre conciencia fonológica y lectoescritura. Las más importantes son:
- Los estudios longitudinales que muestran que los niños con mejores habilidades fonológicas aprenden antes a leer y escribir. En inglés se han realizado numerosos estudios que prueban esa relación11-13. En español se ha hecho un estudio14 en el que a 50 preescolares se les pasaron varias pruebas de procesamiento fonológico antes iniciar el aprendizaje de la lectoescritura, concretamente al comenzar segundo de preescolar, con una edad media cuatro años y tres meses. Las tareas eran de discriminación de fonemas, repetición de palabras inventadas (pseudopalabras) de memoria a corto plazo y de denominación de rápida de objetos. Dos años y medio después, al finalizar tercero de preescolar, con una edad media de cinco años y diez meses, se les pasaron varias tareas del test de lectura PROLEC-R15 y del test de escritura PROESC16. Se encontró una alta correlación entre los resultados en las tareas de procesamiento fonológico y las tareas de lectura, en el sentido de que los niños que puntuaron alto en esas pruebas puntuaron también alto en las de lectura y escritura, y los que obtuvieron bajas puntuaciones en las tareas fonológicas presentaban mayores dificultades en lectoescritura dos años y medio después.
- Los estudios de intervención que muestran que el entrenamiento en habilidades fonológicas mejora la lectoescritura. Numerosos estudios17-22 han demostrado que solo con realizar actividades de conciencia fonológica, los niños de los primeros cursos de escolaridad mejoran automáticamente sus destrezas de lectura y escritura.
- Los estudios que muestran que los niños con déficits fonológicos tienen posteriormente dificultades en lectoescritura23-25. Lyytinen et al.26 hicieron un seguimiento de varios años a un grupo de niños de riesgo en finlandés haciéndoles evaluaciones cada seis meses. Se consideraban de riesgo porque pertenecían a familias con historial de dislexia. Cuando desarrollaron el lenguaje los empezaron a evaluar en tareas fonológicas, por ejemplo distinguir entre “ata” con una consonante corta y “atta” con consonante larga. Los niños de riesgo presentaban más dificultades con este tipo de tareas. Y al comenzar el aprendizaje de la lectura muchos de estos niños presentaron serias dificultades lectoras.
En consecuencia, dada la estrecha relación entre procesamiento fonológico y lectura y escritura, el procesamiento fonológico es, sin duda, el mejor predictor del aprendizaje lectoescritor. Además, el entrenamiento en habilidades fonológicas mejora considerablemente el aprendizaje de la lectura y escritura. De hecho, es el tipo de intervención más adecuado y más exitoso con los niños disléxicos especialmente cuando se realiza a una edad muy temprana6,21,27. Simos et al.6 obtuvieron imágenes cerebrales, mediante magnetoencefalografía, de un grupo de niños de riesgo de cuatro años y comprobaron una menor activación en la zona temporal superior del hemisferio izquierdo, área del procesamiento fonológico, respecto a otro grupo de niños control de la misma edad. Después, con los niños de riesgo realizaron un programa de intervención, dos veces por semana. Al cabo de cuatro meses, comprobaron que los niños habían mejorado notablemente el procesamiento fonológico, pero lo más interesante fue que al observarles de nuevo mediante neuroimagen comprobaron que en la zona temporal superior del hemisferio izquierdo ahora se producía una activación similar a la de los controles. Esto parece indicar que a la edad de cuatro años, dada la plasticidad cerebral, las intervenciones logopédicas son mucho más exitosas.
A la vista de estos resultados parece fundamental poder detectar tempranamente a los niños de riesgo de sufrir alteraciones en el aprendizaje de la lectura, antes incluso de que se comience la enseñanza formal de la misma. Si los pediatras en la revisión de los cuatro años y/o los profesores de segundo de Educación infantil dispusiesen de una prueba sencilla y rápida de aplicar podrían detectar muchos de los llamados niños de riesgo y alertar sobre la necesidad de intervención logopédica con estos niños. Sin duda, se evitarían muchos trastornos en la lectoescritura.
El objetivo de este estudio fue elaborar una prueba de este tipo, es decir, de aplicación rápida pero sensible a los trastornos fonológicos. Para ello se han utilizado varias tareas cortas, pero que miden diferentes aspectos del procesamiento fonológico, como son la discriminación de fonemas, la conciencia fonológica, la repetición de palabras desconocidas, la memoria a corto plazo y la fluidez verbal. Se trata de actividades relacionadas, pero que exigen procesos distintos y que dependen de zonas cerebrales distintas28. Por tanto, la finalidad sería detectar a los niños de riesgo de sufrir trastornos en el aprendizaje de la lectoescritura para poder intervenir sobre ellos y evitar justamente que presenten esos trastornos.
MATERIAL Y MÉTODOS
Participantes
Un total de 298 niños y niñas de cuatro años participaron en el estudio; 122 fueron evaluados en consulta pediátrica, en varios centros de salud del área de Bilbao y de la Comarca Interior de Vizcaya, en el momento en que acudían para la revisión de cuatro años. Los 176 restantes fueron evaluados en colegios de Educación infantil de Amorebieta, Donostia y Oviedo. Todas las pruebas fueron llevadas a cabo de manera individual.
Materiales
Tal como se puede ver en el Anexo 1, la prueba estaba formada por seis subtareas de procesamiento fonológico, la primera de discriminación de fonemas, la segunda de segmentación en sílabas, la tercera de identificación de fonemas, la cuarta de repetición de pseudopalabras, la quinta de amplitud de memoria a través de dígitos y la sexta de fluidez verbal. Cada subtarea se puntúa de 0 a 5 por lo que la puntuación total va de 0 a 30.
Tarea
A cada niño se le pasaban las subtareas que componen la prueba en el mismo orden en que aparecen y siguiendo las instrucción que se encuentran en el apéndice. Antes de comenzar con los ítems puntuables, hay varios de ensayo para asegurarse de que el niño ha comprendido las instrucciones.
RESULTADOS
Tal como se puede ver en la Tabla 1, la puntuación promedio conseguida fue de 22,80 sobre 30. La puntuación media en cada subtarea va de 3,29 en la de fluidez a 4,25 en la de discriminación de fonemas.

En la Fig. 1 se puede ver la distribución de las puntuaciones que se ajustan a la curva normal con un pequeño incremento en la cola de la izquierda como consecuencia del grupo de niños que tienen dificultades en el procesamiento fonológico.
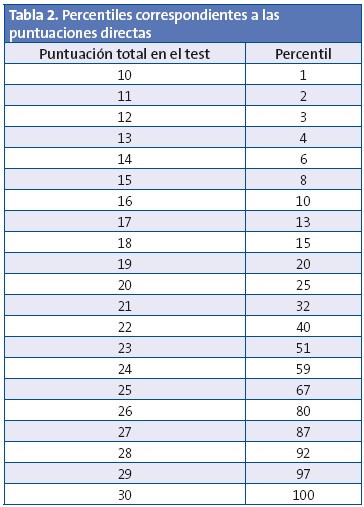
Con las puntuaciones de todos los participantes se calcularon los percentiles (Tabla 2).
Además, con el fin de proporcionar categorías cualitativas a partir de los datos cuantitativos, se consideraron, como se hace usualmente, puntuaciones normales los valores comprendidos entre una desviación por encima y por debajo de la media. Esto es, los valores entre 18,38 (22,80 -4,42) y 27,22 (22,80 +4,42) se consideran puntuaciones normales. Por encima de 27 se sitúan los niños con buenas puntuaciones y por debajo de 18 se encuentran los niños de riesgo. Si en vez de una desviación de la media se resta una desviación y media, la puntuación de corte está en 16,17. Este valor indica que se pueden considerar casos graves todos los que tengan una puntuación por debajo de 16. En total son 31 niños los que obtienen una puntuación de 16 o menos, lo que supone un 10,4% del total.
En definitiva, en base a los datos obtenidos por esta muestra se pueden establecer estas cuatro categorías: a) entre 27 y 30 puntos: buen rendimiento; b) entre 18 y 27 puntos: normal; c) entre 16 y 18 puntos: dificultades leves, y d) menos de 16 puntos: dificultades severas.
Fiabilidad
Para el cálculo de fiabilidad se utilizó el coeficiente α de Cronbach con el número de aciertos en todas las pruebas. El valor de este coeficiente es de 0,73, realmente alto, lo que le confiere una alta fiabilidad a la prueba.
Validez
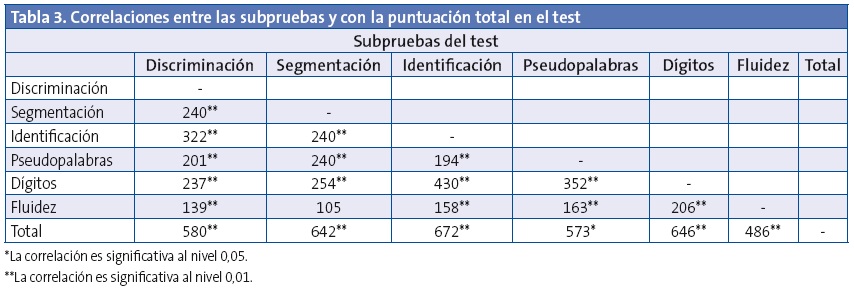
En cuanto a la validez, se utilizó la validez de constructo a través de las correlaciones entre las seis subpruebas que componen el test y con la puntuación total en la prueba. Tal como se puede ver en la Tabla 3, las correlaciones entre las subpruebas son altas, y en todos los casos, excepto entre fluidez y segmentación, son estadísticamente significativas. En cuanto a las correlaciones con el total de la prueba son todas muy altas, siendo la más alta de todas la identificación de fonemas y la más baja la fluidez verbal.
DISCUSIÓN
El objetivo de este estudio ha sido elaborar un test breve de detección temprana de las dificultades en el aprendizaje de la lectura y escritura. La detección temprana de esas dificultades, antes incluso de comenzar el proceso de aprendizaje sistemático de la lectoescritura, puede evitar el fracaso escolar y sufrimiento de muchos niños y familias. Los resultados de las investigaciones de los últimos años muestran, de manera clara, que a través de la evaluación del procesamiento fonológico se puede detectar a los niños con riesgo de presentar dificultades en ese aprendizaje11,14,29.
En consecuencia, para la construcción de este test se tuvieron en cuenta distintos aspectos del procesamiento fonológico, pero todos ellos relacionados con la lectura y escritura, como son la discriminación de fonemas, la conciencia fonológica, la memoria a corto plazo y el acceso al léxico. La discriminación de fonemas permite la escritura al dictado; la conciencia fonológica necesaria para descomponer el habla en sus unidades menores (sílabas y fonemas) para conectarlas posteriormente con los grafemas correspondientes; la memoria a corto plazo, imprescindible para retener información verbal mientras se leen o escriben palabras o frases, y el acceso al léxico que permite desarrollar una lectura fluida.
Todos estos componentes están estrechamente relacionados y prueba de ello es que cuando hay déficit en alguno de ellos suele haberlo en todos, como ocurre con los niños disléxicos30,31. También en niños normales se encuentra correlación en cuando se evalúan esos componentes28.
De acuerdo con estos datos, en este estudio, con una muestra de casi 300 niños hemos encontrado unas correlaciones altas entre todos los componentes y con el total de la prueba, lo que le confiere una buena validez de constructo. También tiene una alta fiabilidad, según la prueba de Cronbach, lo que significa que es una prueba útil para detectar problemas en el procesamiento fonológico y en consecuencia, predecir las dificultades en el aprendizaje de la lectoescritura. Los niños con una puntuación baja en esta prueba posiblemente, si no se hace nada para remediarlo, tendrán dificultades para aprender a leer y escribir. El objetivo de la prueba es justamente evitar que se produzcan esas dificultades, ya que la intervención temprana sobre los niños de riesgo es mucho más efectiva.
La prueba es de fácil y rápida aplicación en niños de cuatro años. Se tarda un promedio de seis a diez minutos y con la puntuación obtenida se puede ver si el niño necesita intervención logopédica para evitar problemas de lectura y escritura. De hecho en la propia prueba se indican los valores por debajo de los cuales se consideran casos de riesgo. Está pensada para los pediatras en la revisión de los cuatro años y para los profesores de Educación infantil que trabajan con niños de esta edad. Sin duda su aplicación, y posterior intervención logopédica, evitará el fracaso escolar y la pérdida de autoestima de muchos niños.
CONFLICTO DE INTERESES
Este estudio ha sido realizado dentro del proyecto PSI2012-31913 del Ministerio de Economía y Competitividad.
BIBLIOGRAFÍA
- Cuetos F. Psicología de la lectura. Madrid: Wolters-Kluwer; 2008.
- Shaywitz SE, Shaywitz BA, Fletcher JM, Escobar MD. Prevalence of reading disability in boys and girls. Results of the Connecticut Longitudinal Study. JAMA. 1990;264:998-1002.
- Cuetos F. Dislexias evolutivas: un puzzle por resolver. Revista de Logopedia, Foniatría y Audiología. 2009;29:78-84.
- Jiménez JE, Rodríguez C, Ramírez G. Spanish developmental dyslexia: prevalence, cognitive profile, and home literacy experiences. J Exp Child Psychol. 2009;103:167-85.
- Papanicolaou AC, Simos PG, Breier JI, Fletcher JM, Foorman BR, Francis D, et al. Brain mechanisms for reading in children with and without dyslexia: a review of studies of normal development and plasticity. Dev Neuropsychol. 2003;24:593-612.
- Simos PG, Fletcher JM, Bergman E, Breier JI, Foorman BR, Castillo EM, et al. Dyslexia-specific brain activation profile becomes normal following successful remedial training. Neurology. 2002;58:1203-13.
- Snowling MJ. From language to reading and dyslexia. Dyslexia. 2001;7:37-46.
- Ramus F. Outstanding questions about phonological processing in dyslexia. Dyslexia. 2001;7:197-216.
- Ramus F. Dyslexia. Talk of two theories. Nature. 2001;412:393-5.
- Lyon GR, Shaywitz SE, Shaywitz BA. Defining dyslexia, comorbidity, teachers’ knowledge of language and reading: a definition of dyslexia. Ann Dyslexia. 2003;53:1-14.
- Caravolas M, Volin J, Hulme C. Phoneme awareness is a key component of alphabetic literacy skills in consistent and inconsistent orthographies: evidence from Czech and English children. J Exp Child Psychol. 2005;92:107-39.
- Parrila RK, Kirby JR, McQuarrie L. Articulation rate, naming speed, verbal short-term memory, and phonological awareness: Longitudinal predictors of early reading development? Scientific Studies Reading. 2004;8:3-26.
- Wagner R, Torgesen J, Rashotte C, Hecht S, Barker T, Burgess S, et al. Changing relations between phonological processing abilities and word-level reading as children develop from beginning to skilled readers: a 5 year longitudinal study. Dev Psychol. 1997;33:468-79.
- Suárez-Coalla P, García de Castro M, Cuetos F. Variables predictoras de la lectura y la escritura en castellano. Infancia y Aprendizaje. 2013;36:77-89.
- Cuetos F, Rodríguez B, Ruano E. Evaluación de los procesos lectores. PROLEC-R. Madrid: Ediciones TEA; 2007.
- Cuetos F, Ramos JL, Ruano E. Evaluación de los procesos de escritura. PROESC. Madrid: Ediciones TEA; 2002.
- Brady S, Fowler A, Stone B, Winbury N. Training phonological awareness: a study with inner-city kindergarten children. Ann Dyslexia. 1994;44:26-59.
- Ehri L, Nunes S, Willows D, Schuster B. Phonemic awareness instruction helps children learn to read: Evidence from the National Reading Panel’s metaanalysis. Reading Research Quarterly. 2001;36:250-87.
- Foorman BR, Breier JI, Fletcher JM. Interventions aimed at improving reading success: an evidence-based approach. Dev Neuropsychol. 2003;24:613-39.
- Hatcher PJ, Hulme C, Snowling MJ. Explicit phoneme training combined with phonic reading instruction helps young children at risk of reading failure. J Child Psychol Psychiatry. 2004;45:338-58.
- Temple E, Deutsch GK, Poldrack RA, Miller SL, Tallal P, Merzenich MM, et al. Neural deficits in children with dyslexia ameliorated by behavioral remediation: evidence from functional MRI. Proc Natl Acad Sci USA. 2003;100:2860-5.
- Torgesen JK, Alexander AW, Wagner RK, Rashotte CA, Voeller KK, Conway T. Intensive remedial instruction for children with severe reading disabilities: immediate and long-term outcomes from two instructional approaches. J Learn Disabil. 2001;34:33-58.
- Bruck M. Persistence of dyslexics’ phonological awareness deficits. Dev Psychol. 1992;26:874-88.
- Swan D, Goswami U. Phonological awareness deficits in developmental dyslexia and the phonological representations hypothesis. J Exp Child Psychol. 1997;66:18-41.
- Vellutino FR, Fletcher JM, Snowling MJ, Scanlon DM. Specific reading disability (dyslexia): what have we learned in the past four decades? J Child Psychol Psychiatry. 2004;45:2-40.
- Lyytinen H, Ahonen T, Eklund K, Guttorm T, Laakso M, Leinonen S, et al. Developmental pathways of children with and without familial risk for dyslexia during the first years of life. Dev Neuropsychol. 2001;20:535-54.
- Suárez-Coalla P. Intervención en dislexia evolutiva. Revista Logopedia, Foniatría y Audiología. 2009;29:131-7.
- Turkeltaub PE, Gareau L, Flowers DL, Zeffiro TA, Eden GF. Development of neural mechanisms for reading. Nat Neurosci. 2003;6:767-73.
- Défior S. ¿Cómo facilitar el aprendizaje inicial de la lectoescritura? Papel de las habilidades fonológicas. Infancia y Aprendizaje. 2008;31:333-45.
- De Jong PF, van der Leij A. Specific contributions of phonological abilities to early reading acquisition: results from a Dutch latent variable longitudinal study. J Educ Psychol. 1999;91:450-76.
- Wagner RK, Torgesen JK. The nature of phonological processing and its causal role in the acquisition of reading skills. Psychological Bull. 1987;101:192-212.
ANEXO 1
Test predictivo de dificultades en la lectoescritura
Nombre y apellidos / Fecha de nacimiento / Fecha de aplicación de la prueba
Discriminación de fonemas (pares mínimos). “Vamos a hacer un juego. Te voy a decir dos palabras y tienes que decirme si son iguales o diferentes, si las dos palabras son la misma o no. Fíjate bien: Gol-gol (son iguales), dar-bar (son muy parecidas, pero no son iguales, son diferentes). Ahora te toca a ti: coz-coz..., mil-mis... ¡Muy bien, seguimos!”.
pan-paz • luz-luz • pez-tez • cal-col • fin-fin
Total:
Segmentación de sílabas. “Ahora tienes que dar palmas. Mira cómo hago yo: casa ca-sa; ahora una más larga: ventana: ven-ta-na. Ahora te toca a ti, dedo: ....... vaso:..... ¡Muy bien!”.
pera • lazo • cometa • oveja • mariposa
Total:
Identificación de fonema. “Voy a decirte un sonido /r/, repítelo conmigo. Ahora dime si lo oyes en estas palabras. ¿Está /r/ en zorro? (sí); ¿Oyes /r/ en la palabra pelo? (no). Seguimos con otras palabras...”.
carro • sillón • ratón • rojo • piña
Total:
Repetición de pseudopalabras. “Este juego consiste en repetir. Tienes que repetir unas palabras que no existen, porque me las he inventado. ¿Vale? Repite lo que yo digo: jepo, socata... ¡Muy bien, ¿estás listo para continuar?".
nigo • muspe • diplo • tingano • pelagro
Total:
Repetición de dígitos. “Te voy a decir unos números y tienes que repetírmelos. Presta mucha atención para no fallar”.
8 5
1-6 7-2
5-2-1 6-4-8
5-3-1-8 3-7-4-1
4-1-8-3-9 6-3-2-5-8
Total:
Fluidez verbal. Nombres de animales. “¿Cuál es tu animal favorito?... Perfecto, pues ahora dime todos los animales que se te ocurran”.
Número de animales
Total:
Puntuación total (sobre 30):
Instrucciones para la aplicación y puntuación de las tareas predictoras de la lectura
Esta prueba evalúa una serie de habilidades relacionadas con la adquisición de la lectura: conciencia silábica, discriminación de fonemas, memoria fonológica, fluidez verbal. La prueba consta de seis tareas; cada una de ellas tendrá una puntuación máxima de 5 puntos, con lo cual el total de la prueba serán 30 puntos. El tiempo de administración es de aproximadamente cinco minutos.
Cada tarea tiene unas instrucciones orientativas, pero a veces se requieren explicaciones complementarias para que el niño comprenda lo que se le pide.
- Discriminación de fonemas. El niño tiene que decir si dos palabras son iguales o diferentes, para ello se le ponen ejemplos de dos palabras iguales (mano-mano) y de dos palabras diferentes (mano-león). Es una tarea que no les resulta difícil de entender. Puntuación: se pone un punto por cada par bien realizado.
- Segmentación de sílabas. En esta tarea se mide la conciencia de sílaba y el niño tiene que segmentar la palabra en sílabas, dando palmas o golpes en la mesa. Se le pondrán varios ejemplos, los que vienen en las explicaciones, su nombre, el nombre de su madre... y se continúa con los ítems del test. Puntuación: se pone un punto por cada palabra bien segmentada.
- Identificación de fonemas. Se valora la capacidad de discriminar fonemas dentro de una palabra. Al niño se le indica que tiene que decirnos si oye un sonido (fonema /r/) dentro de una palabra. Se le dice el fonema aislado y se le manda que lo reproduzca él (en algunos casos el niño no tendrá una pronunciación perfecta del fonema), luego se le ponen ejemplos de palabras que llevan ese fonema: arrrrroz, Rrrramón, rrrrío,... Luego se pasa a la tarea. Puntuación: se pone un punto por cada palabra.
- Repetición de pseudopalabras. Esta tarea es muy sencilla. El niño tiene que repetir sin más. Puntuación: se pondrá un punto por cada pseudopalabra correctamente repetida.
- Repetición de dígitos. Se trata de medir la memoria fonológica. El niño tiene que repetir series de números; se comienza con un número, si lo repite bien se pasa a dos, después a tres... Si falla se le da otra oportunidad con la serie de la segunda columna. Si fracasa en los dos intentos se interrumpe la prueba y se anota el número de dígitos que ha conseguido repetir. Se presentan al ritmo de un número por segundo. Puntuación: la puntuación se corresponderá con el mayor número de dígitos repetido correctamente.
- Fluidez verbal. En un minuto el niño debe nombrar todos los animales que se le ocurran. Se anotará el número de animales dichos. Puntuación: se puntuará según el número de animales. 0-1: 0 puntos; 2-3: 1 punto; 4-5: 2 puntos; 6-7: 3 puntos; 8-9: 4 puntos; 10 o más: 5 puntos.
La puntuación total se obtiene sumando las puntuaciones parciales de las seis tareas:
- Entre 27 y 30 puntos: buen rendimiento.
- Entre 18 y 27 puntos: normal.
- Entre 16 y 18 puntos: dificultades leves.
- Menos de 16 puntos: dificultades severas.