Estado nutricional de la población infantil en Asturias (Estudio ESNUPI-AS): delgadez, sobrepeso, obesidad y talla baja
Begoña Domínguez Aurrecoecheaa, Manuela Sánchez Echeniqueb, M.ª Ángeles Ordóñez Alonsoc, José Ignacio Pérez Candásd, J Delfrade Osinagae
aPediatra. Instituto de Investigación Sanitaria del Principado de Asturias (ISPA). Asturias. España.
bPediatra. Servicio de Planificación y Gestión de Atención Primaria. Navarra. España.
cPediatra. CS La Corredoria. Instituto de Investigación Sanitaria del Principado de Asturias (ISPA). Oviedo. Asturias. España.
dPediatra. CS de Sabugo. Avilés. Asturias. España.
eTécnico del CIBER. Instituto de Salud Pública Navarra. Navarra. España.
Correspondencia: B Domínguez. Correo electrónico: begoa.dominguez@gmail.com
Cómo citar este artículo: Domínguez Aurrecoechea B, Sánchez Echenique M, Ordóñez Alonso MA, Pérez Candás JI, Delfrade Osinaga J. Estado nutricional de la población infantil en Asturias (Estudio ESNUPI-AS): delgadez, sobrepeso, obesidad y talla baja. Rev Pediatr Aten Primaria. 2015;17:e21-e31.
Publicado en Internet: 18-03-2015 - Número de visitas: 73680
Resumen
Objetivos: valorar el estado de nutrición de los niños menores de quince años del Principado de Asturias, identificando los que tienen parámetros alterados, por exceso o defecto, y devolver la información obtenida a pediatras y gestores.
Métodos: estudio descriptivo transversal retrospectivo. Población diana: menores de 15 años de Asturias nacidos entre 1995 y 2012. Fuente de datos: historia clínica informatizada de Atención Primaria. Variables: último peso y talla registrados, fecha de medida y de nacimiento, sexo, y códigos de área, zona básica y pediatra del niño. Indicadores calculados: peso/edad; talla/edad; índice de masa corporal (IMC)/edad y peso/longitud (< cinco años). Patrones de comparación utilizados: estándares de la Organización Mundial de la Salud (OMS) y se han utilizado los softwares ANTHRO y ANTHRO PLUS. Se calcularon para cada niño la desviación estándar (DE) según edad y sexo para el IMC/edad, talla/edad y peso/edad; (Z-standard) y las prevalencias de cada variable ajustadas por edad y sexo.
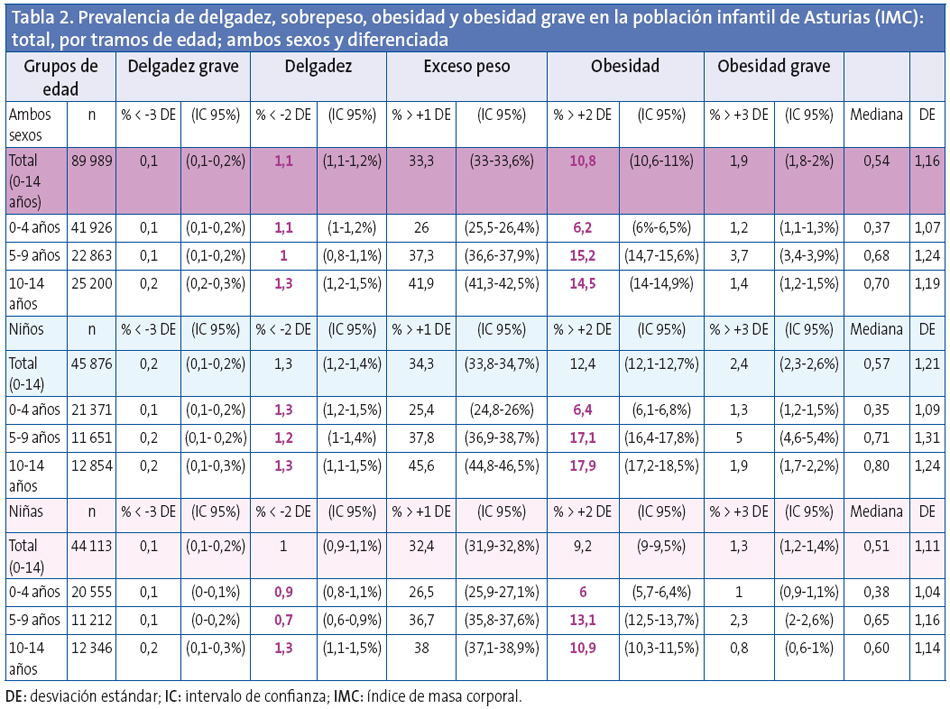
Resultados y conclusiones: se obtuvo una base neta con 89 989 registros: el 50,98% niños y el 49,02% niñas. Presentaron baja talla el 1,8%, normopeso el 66,56%, sobrepeso el 22,5%, obesidad el 10,9%, obesidad grave el 1,9% y delgadez el 1,1%. Por sexos, la tasa de obesidad es mayor en niños (12,4) que en niñas (9,2). Por edades, la tasa de exceso de peso fue mayor en los niños de entre 10 y 14 años (41,9). Los niños de entre cinco y nueve años presentaron las mayores tasas de obesidad (15,1) y obesidad grave (3,7). Las diferencias de prevalencia de exceso de peso entre las 68 zonas básicas estudiadas llegan hasta 20 puntos; su conocimiento permitirá establecer las zonas prioritarias de intervención.
Palabras clave
● Asturias ● España ● Infantil ● Nutrición ● Obesidad ● Sobrepeso ● Talla bajaINTRODUCCIÓN
Son muchas las investigaciones que muestran la importancia de una correcta nutrición para el buen desarrollo y la salud del niño y adolescente y el impacto que tiene para el futuro, tanto a nivel personal como comunitario. Los impactos de la nutrición en la salud pueden llegar incluso a las siguientes generaciones, como muestran las investigaciones de epigenética de Pembrey y M. Sjöström1,2.
Aunque en los países desarrollados la alteración más preocupante en estos momentos es la prevalencia de las alteraciones por exceso, en sus grados de sobrepeso y obesidad, es importante también detectar si existen zonas que puedan tener alteraciones por defecto causadas por factores personales, del entorno sociocultural y de la crisis económica.
Se consideró oportuno realizar un estudio de la situación para obtener información de las zonas prioritarias que precisen intervenciones especiales, máxime en este momento en el que, debido a la crisis, se debe de extremar la vigilancia para detectar también focos de desnutrición.
Los informes publicados por la International Association for the Study of Obesity (IASO)3 en 2007 indican que los países con más alto índice de sobrepeso en la edad infanto-juvenil son España (35% y32% para niños y niñas respectivamente), seguidos por Malta (30,9% y 20,1%), Portugal (25,9% y 34,3%), Escocia (29,8% y 32,9%) e Inglaterra (29% y 29,3%).
Sin embargo, la diversidad de criterios que se usan para la definición de sobrepeso y obesidad y debido a que cada país ha diseñado sus propias tablas, tanto de tipo longitudinales4,5como transversales, hacen difícil la comparación de los datos.
Con el fin de resolver estos problemas, la Organización Mundial de la Salud (OMS) lideró la construcción de unas gráficas con un enfoque prescriptivo, que muestran cómo los niños deberían crecer cuando el entorno permite que su potencial genético se desarrolle óptimamente; la OMS6 presentó el año 2006 estas gráficas para los niños menores de cinco años,adoptadas ya oficialmente por más de 125 países. En 2007, la OMS, como continuación a dichas gráficas, presentó las referencias para escolares de 5-19 años7, lo que permitirá poder tener unos criterios homogéneos a la hora de efectuar los cálculos y comparaciones. La OMS ha editado asimismo un software de apoyo, ANTHRO (de 0 a 60 meses) y ANTHRO PLUS (mayores de cinco años) que permite realizar el estudio nutricional individual y de grupo, de manera que los resultados sean fácilmente obtenibles y así poder realizar comparaciones de datos a nivel mundial8,9.
En Navarra se ha realizado un estudio con la totalidad de los niños menores de 15 años los años 2007, 2009, 2011 y 2013, que permite apreciar las tendencias.
Pocos son los estudios que se centran en la Atención Primaria (AP) y su importancia en el diagnóstico precoz de las alteraciones de nutrición. Teniendo en cuenta el seguimiento completo, desde el nacimiento hasta los 14 años, que se realiza a los niños en nuestro sistema público de salud, debe de considerarse la plataforma perfecta para estos objetivos.
OBJETIVOS
El objetivo general es valorar el estado de nutrición de la población menor de 15 años del Principado de Asturias atendida en los centros de salud, estudiando la prevalencia de la baja talla, el sobrepeso, la obesidad, la obesidad mórbida y la delgadez según los criterios de la OMS.
Los objetivos específicos son devolver la información detallada obtenida a los profesionales y aportar a los gestores una visión general con las zonas que presentan mayores o menores prevalencias, lo que será de utilidad para planificar y priorizar estrategias de intervención.
MATERIAL Y MÉTODOS
Es un estudio descriptivo retrospectivo transversal. Se extrajo, por parte del servicio responsable del Servicio de Salud del Principado de Asturias (SESPA) a partir de la historia clínica informatizada, una base de datos con las siguientes características.
Universo muestral: todos los niños menores de 15 años nacidos desde el 1 de enero de 1995 hasta marzo del 2012 que acuden a las consultas de los centros de salud de Asturias. Se incluyeron los datos de todos los niños en dicha franja de edad, inclusive los que no tenían datos de peso y talla, con el fin de valorar también la cobertura en relación al universo total.
Variables obtenidas a partir de la historia clínica de cada niño: fecha de nacimiento, sexo, último peso y talla (cuando ambos se hubieran obtenido el mismo día), fecha de la medida del peso y talla, número de Tarjeta Individual Sanitaria (TIS), país de nacimiento, zona básica o centro de salud y código de identificación (CIAS) del médico responsable.
Para garantizar la confidencialidad de los datos se disoció el número de TIS, dándole otro valor que imposibilita al investigador la identificación del niño. El servicio de obtención de datos se queda con el fichero que vincula el número real de TIS con el disociado. Una vez procesados y obtenidos los datos del estudio, el recorrido inverso es realizado antes de enviar al profesional los datos de sus pacientes.
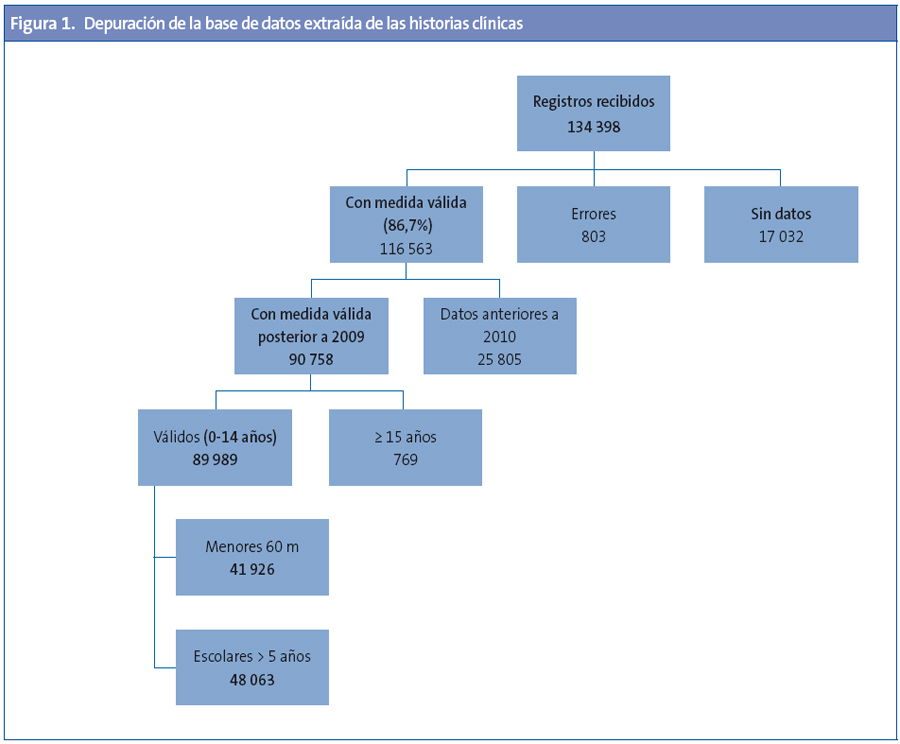
Obtenida la base bruta, se eliminaron las mediciones erróneas, los mayores de 14 años y los registros con medidas anteriores al 2010, incluyendo tan solo los datos registrados con posterioridad a enero 2010 (Anexo 1, Fig. 1).
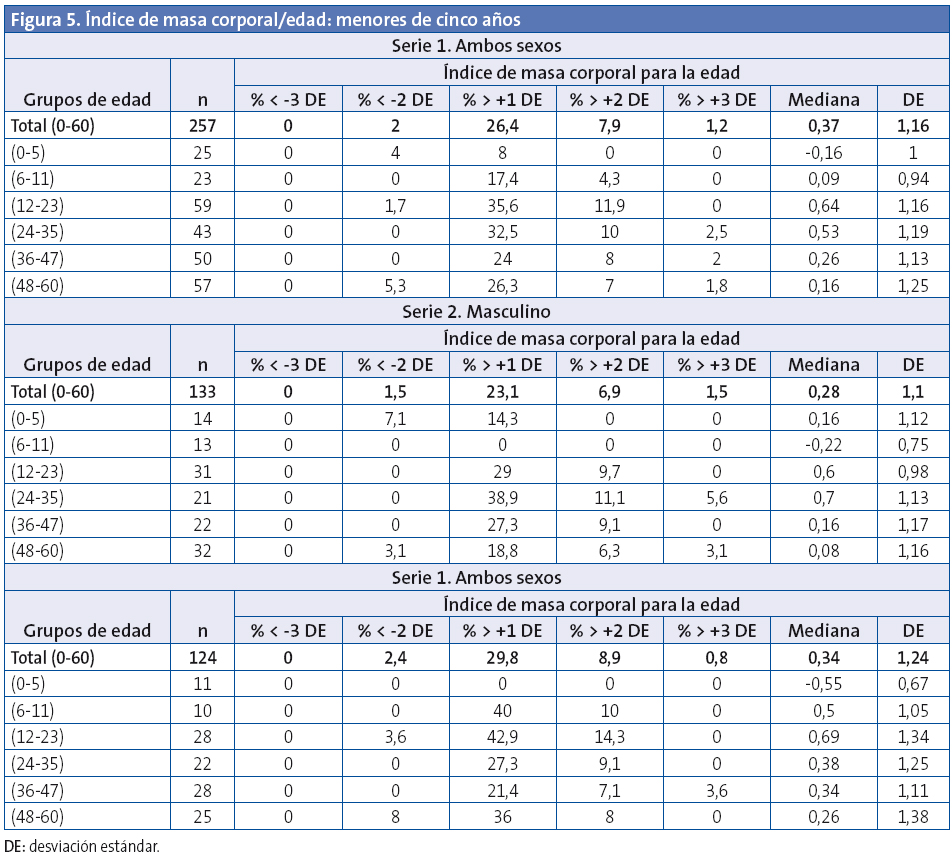
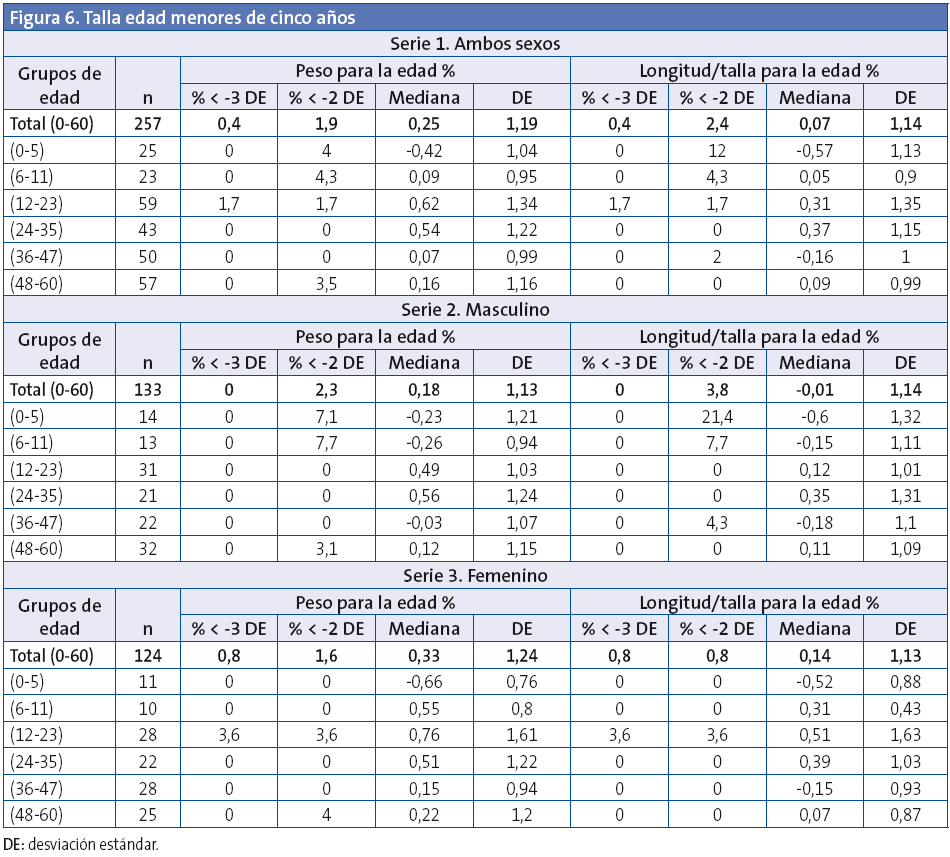
Indicadores calculados: peso/edad, talla/edad, índice de masa corporal (IMC)/edad y peso/longitud (< cinco años).
Patrones de comparación utilizados: estándares de la OMS, y obtenida la base neta, con 89 989 registros, mediante el software de la OMS, ANTHRO y ANTHRO PLUS, en su sección de “Encuesta nutricional”, se calculó para cada niño la desviación estándar (DE) según edad y sexo para el IMC/edad, talla/edad y peso/edad.
Asimismo se obtuvieron mediante el programa los siguientes datos: porcentaje de niños con IMC/edad (> +1 DE): exceso peso: incluye sobrepeso y obesidad; porcentaje de niños con IMC/edad (> +2 DE): obesidad; porcentaje de niños con IMC/edad (> +3 DE): obesidad grave; porcentaje de niños con bajo IMC/edad (< -2D E): delgadez; porcentaje de niños con bajo IMC/edad (< -3 DE): delgadez grave; porcentaje de niños con bajo peso/edad (< -2 DE); porcentaje de niños con baja talla/edad (< -2 DE).
En los menores de cinco años (60 meses), la OMS recomienda el término sobrepeso para IMC > +2 DE para evitar que se utilicen dietas restrictivas en época de crecimiento importante10.
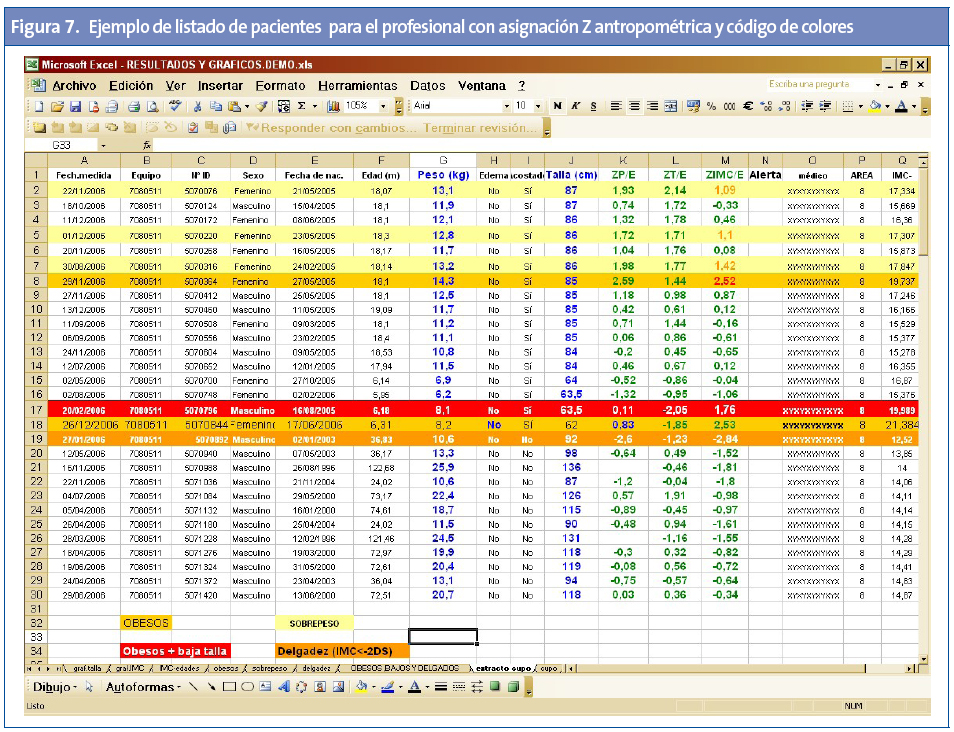
A todos los niños se les ha calculado su puntuación Z antropométrica.
La prevalencia de cada variable es presentada de forma gráfica y numérica tanto del conjunto global como por tramos de edad y por sexos y para los diferentes niveles: cupos; las 68 zonas básicas; las ocho áreas sanitarias y la comunidad autónoma (CC. AA.).
Los resultados se presentan con sus intervalos de confianza, mediana y desviación estándar.
Para comparar la prevalencia por zonas entre sí, se calculó la prevalencia ajustada por edad y sexo (método directo). Para el cálculo de la población total de las diferentes zonas básicas de salud estudiadas se utilizaron los datos de la Consejería de Salud del Principado de Asturias (año 2012).
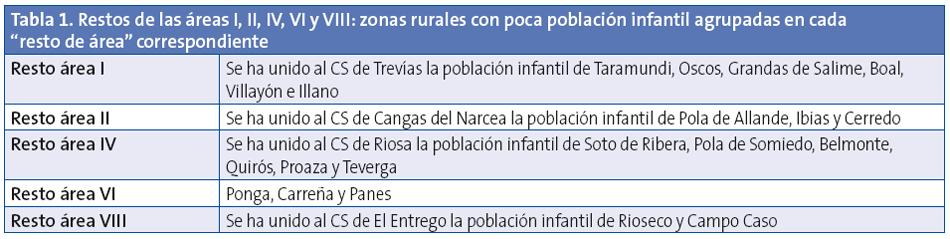
Algunas zonas con baja población infantil se agruparon bajo el concepto “Resto de áreas” (Anexo 1, Tabla 1).
Se elaboró una clasificación (ranking) con las zonas básicas de salud, clasificándolas según su prevalencia ajustada de sobrepeso y obesidad y se comprobó además para cada una de ellas si existen diferencias significativas respecto a la media de la prevalencia de sobrepeso y obesidad de Asturias.
RESULTADOS
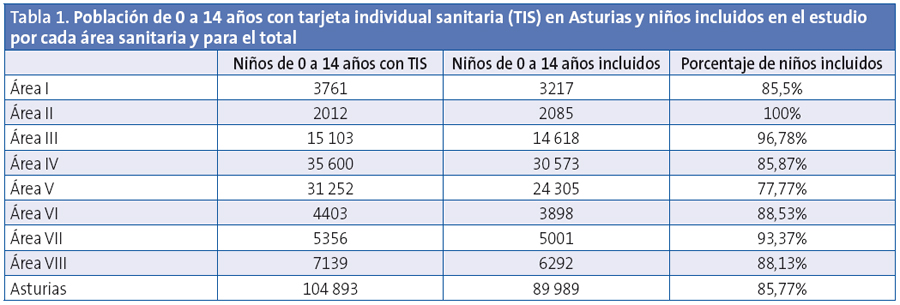
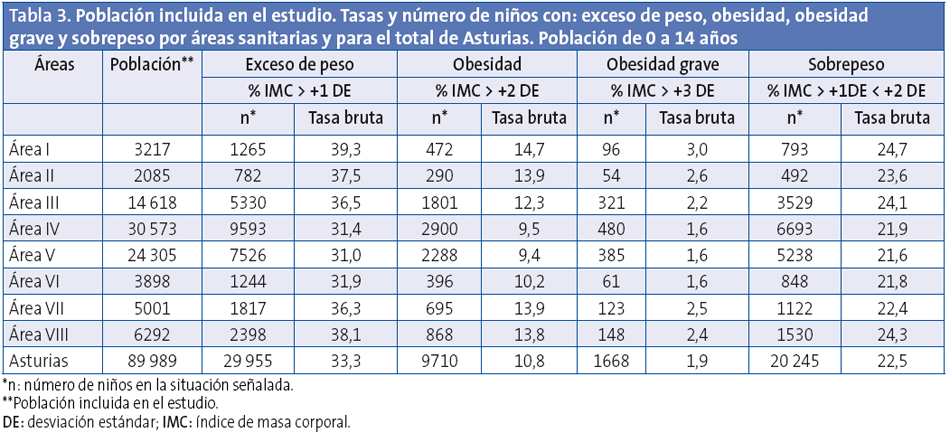
Se incluyeron en el estudio 89 989 niños de los que el 49,02% son niñas y el 50,98% niños. Los niños incluidos son el 85,77% de la población de 0 a 14 años con TIS del Principado de Asturias en el año 2012, que son un total de 104 893 (Tabla 1).
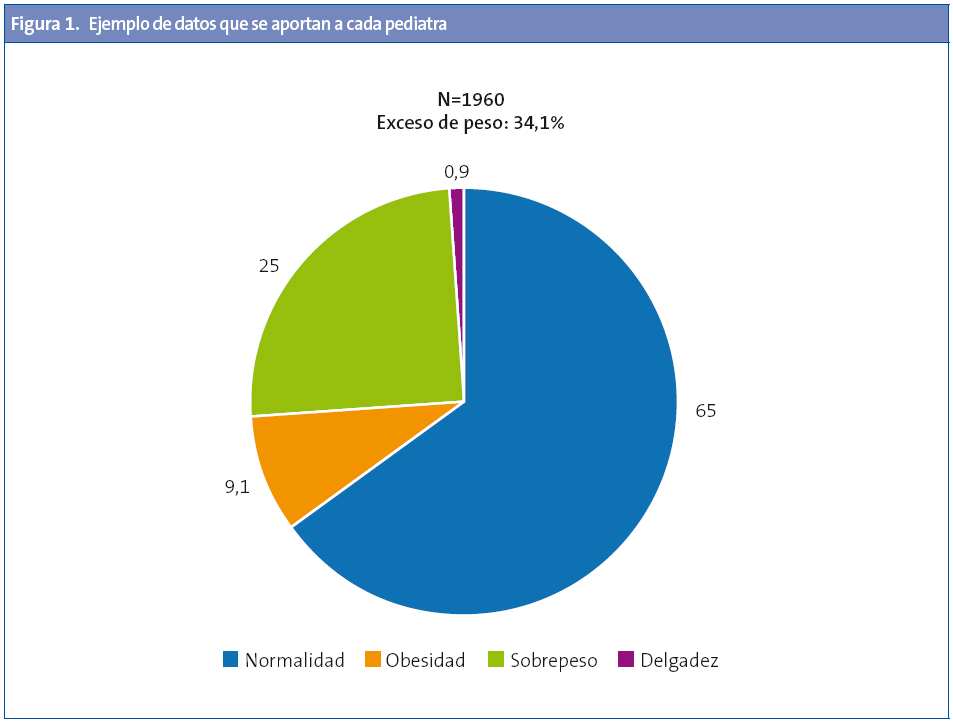
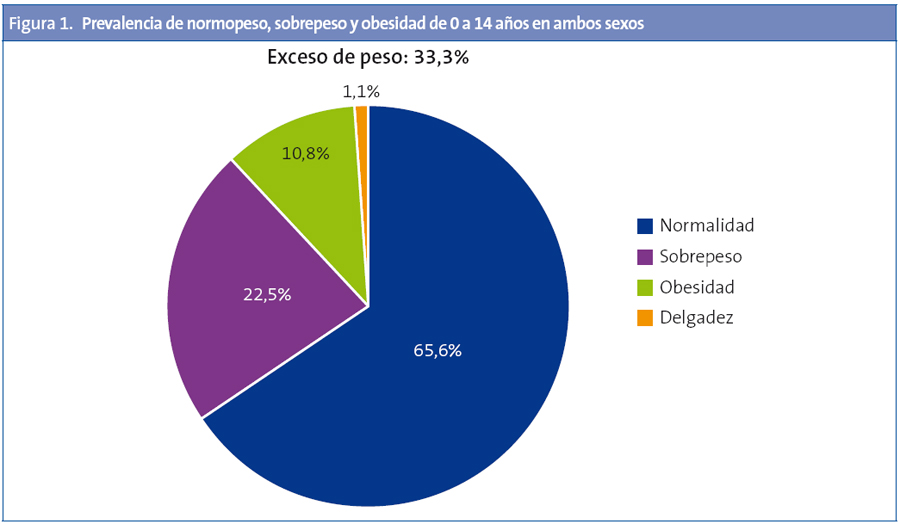
La prevalencia de la delgadez es del 1,1% y la de talla baja del 1,8%. La prevalencia de normopeso es del 65,6%; la de sobrepeso del 22,5% y la obesidad del 10,8% (Fig. 1).
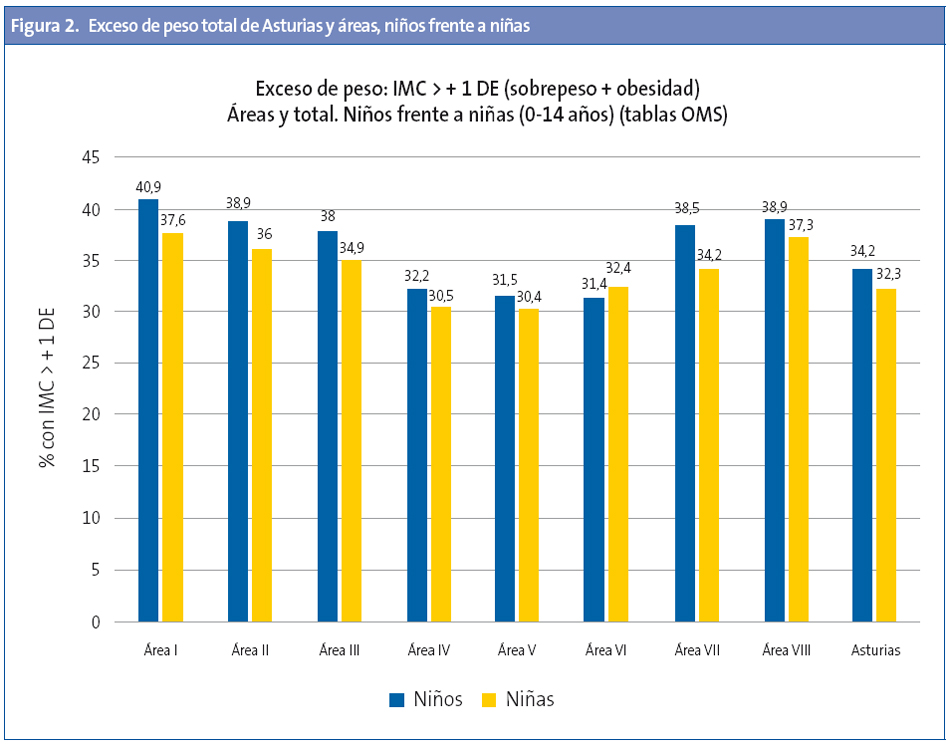
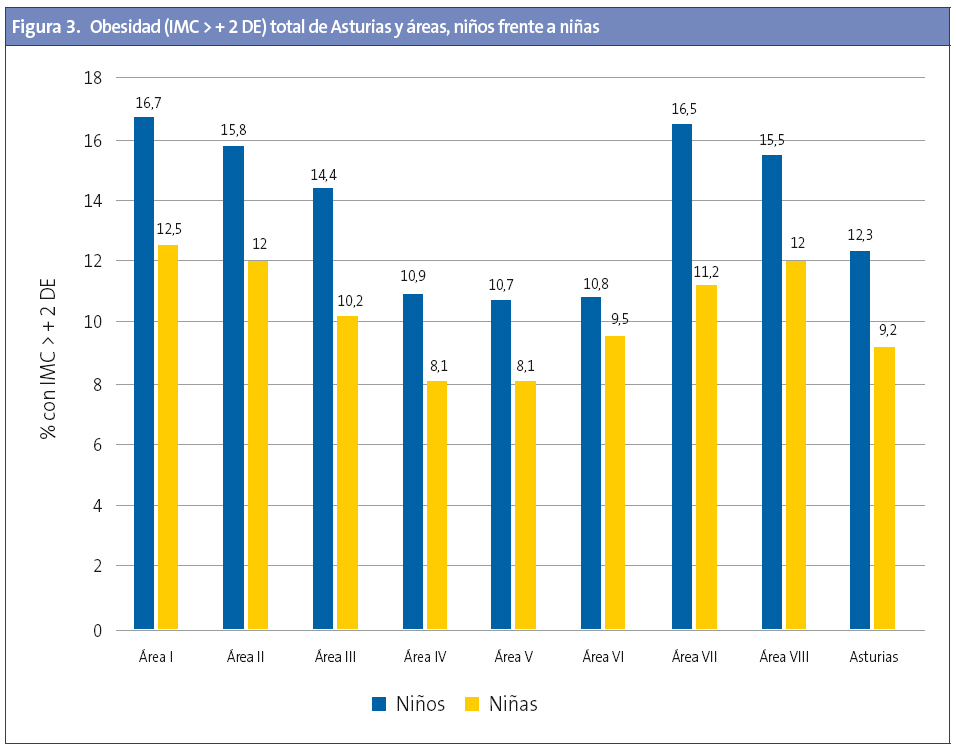
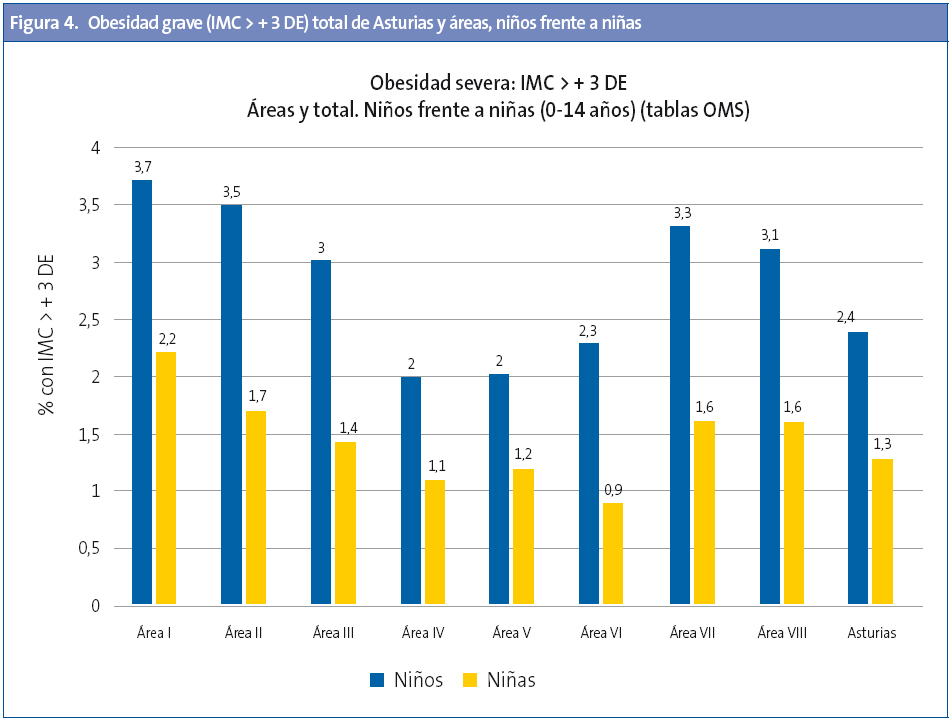
Por sexos, para el total de Asturias, la tasa de exceso de peso (sobrepeso + obesidad) es mayor en niños (34,3) que en niñas (32,4); lo mismo ocurre para la obesidad (niños 12,4; niñas 9,2) y obesidad grave (tasa de 2,4 en niños y 1,3 niñas). En la Tabla 2 se exponen los datos para Asturias y por tramos de edad con IC, mediana y DE.
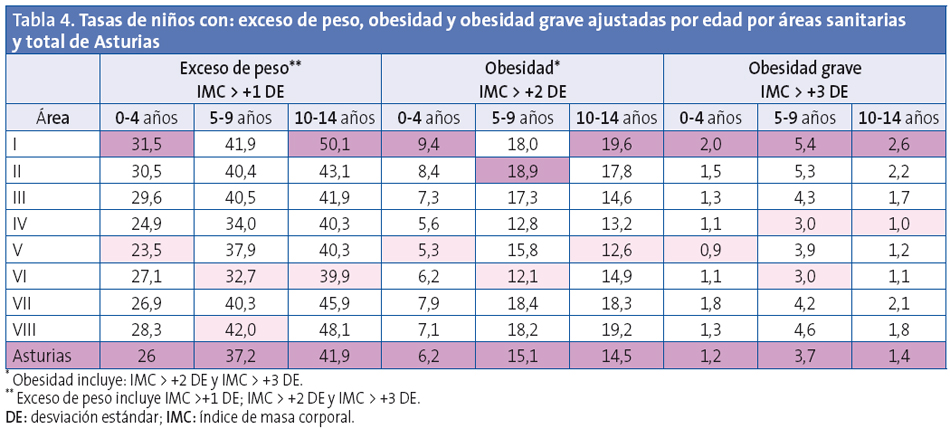
Por edades, el exceso de peso es mayor en los niños de entre 10 y 14 años; la obesidad y la obesidad grave, en el tramo de entre cinco y nueve años (Tabla 2).
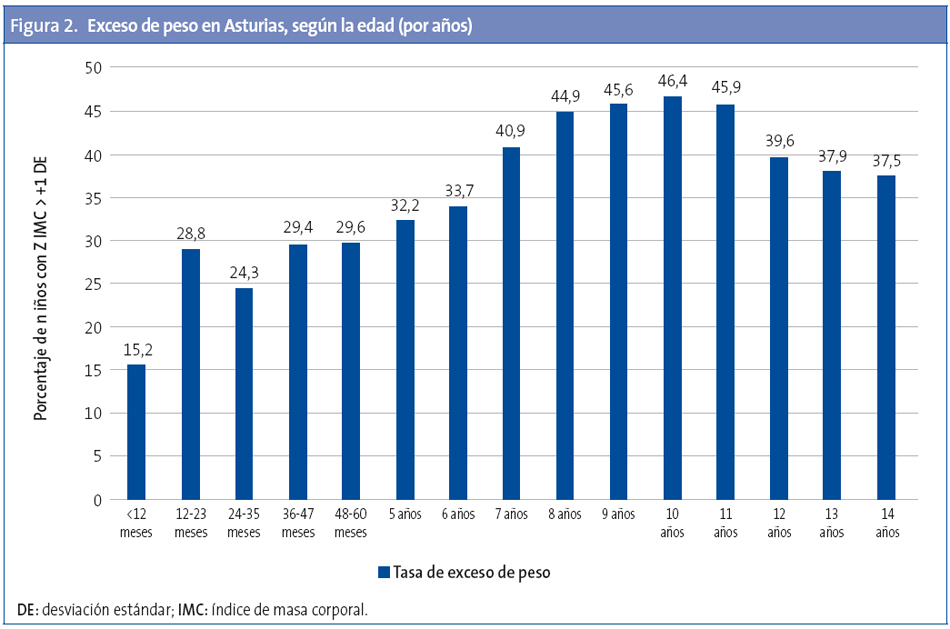
El estudio pormenorizado año a año demuestra que entre el primer y segundo año de vida se produce un aumento importante del exceso de peso (28,8%), que se mantiene hasta el quinto año (29,6%); se observa después un nuevo pico entre los 7 y 11 años, que desciende posteriormente hasta los 14 años (Fig. 2).
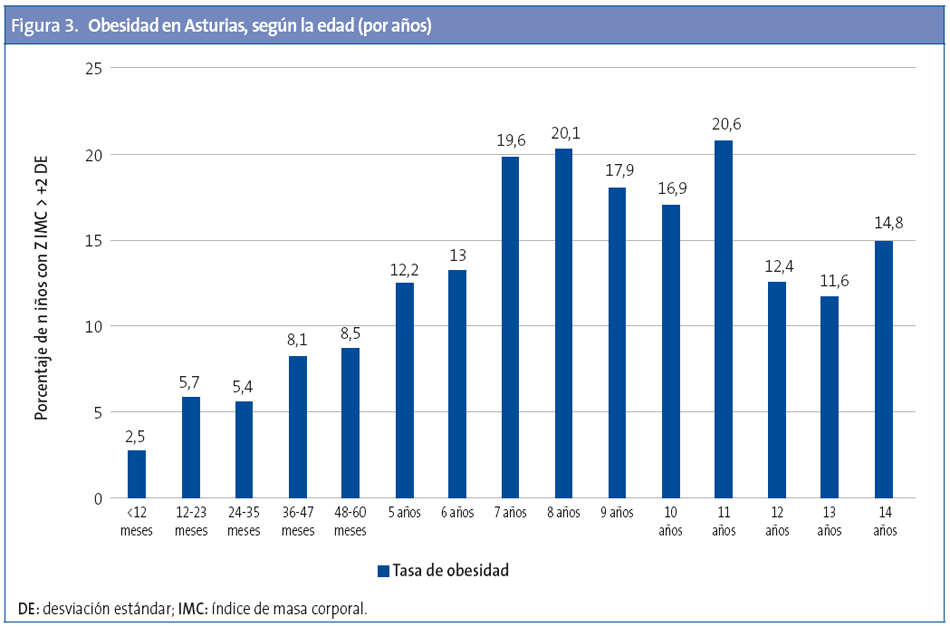
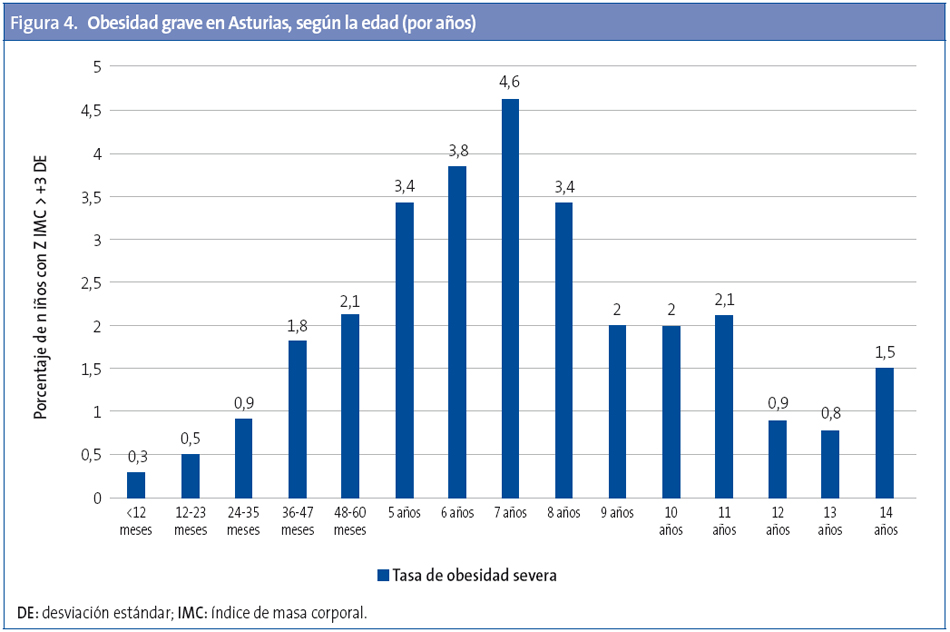
Las tasas mayores de obesidad se producen entre los 7 y 11 años (Fig. 3) y la de obesidad grave a los siete y ocho años (Fig. 4).
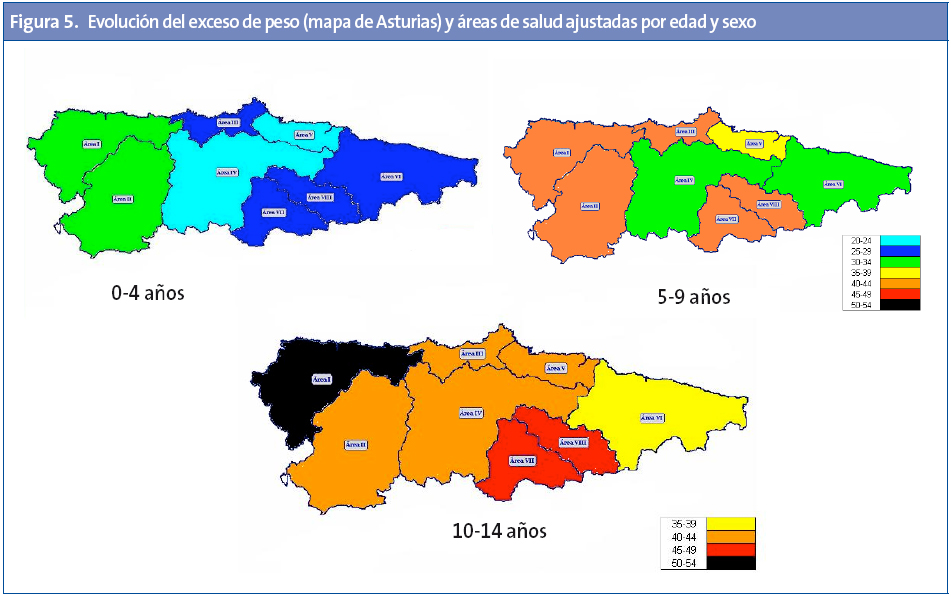
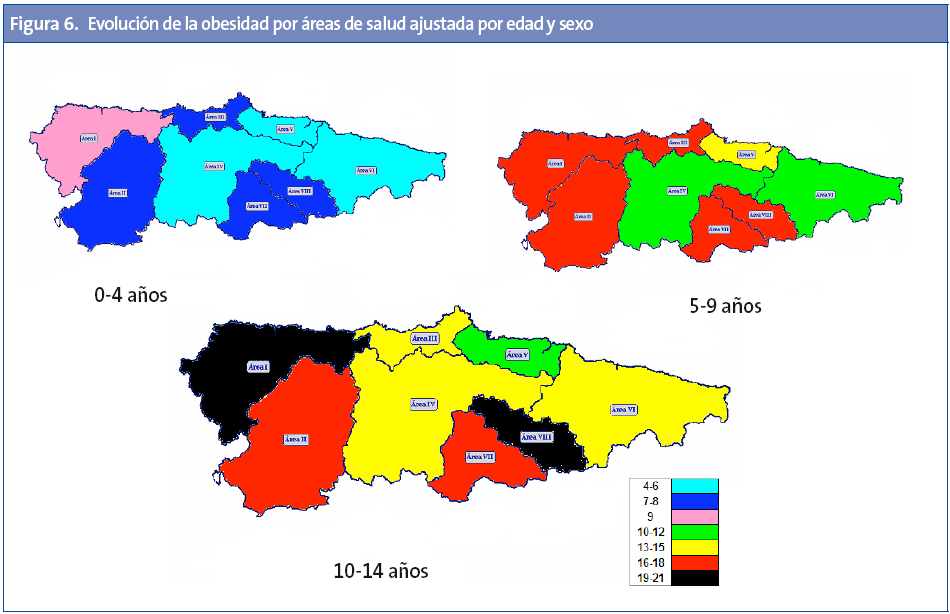
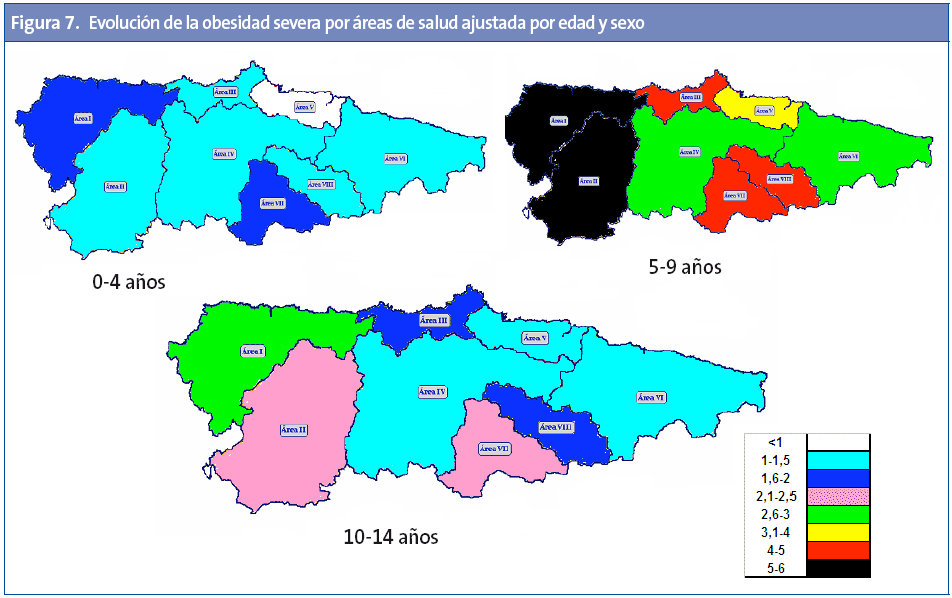
Las diferencias entre las áreas sanitarias son importantes (Tabla 3), presentando el área I las tasas más altas de exceso de peso, obesidad y obesidad grave. Las áreas IV, V y VI son las de menores prevalencias en todos los parámetros. Por tramos de edad, el área I presenta las mayores tasas para todas las edades excepto la mayor tasa de obesidad entre cinco y nueve años, que corresponde al área II, y el mayor exceso de peso para esta misma edad al área VIII (Tabla 3). De manera detallada y para las diferentes áreas, se exponen en el mapa sanitario de Asturias (Anexo 1) los resultados de la evolución por tramos de edad de las tasas de exceso de peso (Figura 5), obesidad (Figura 6) y obesidad severa (Figura 7).
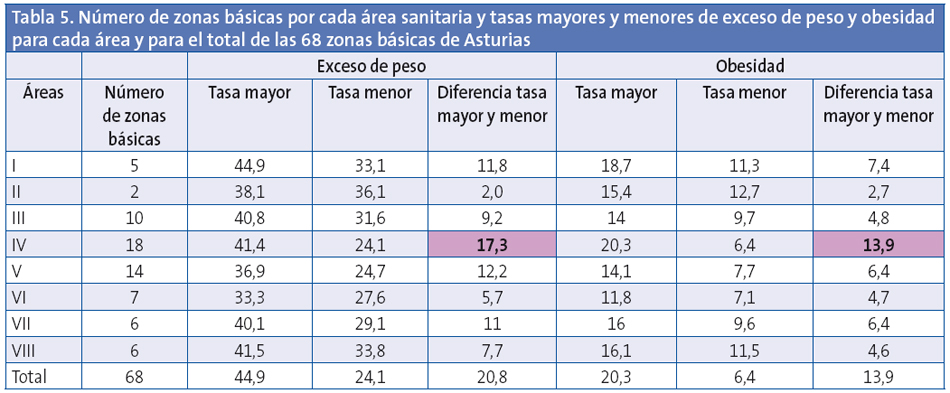
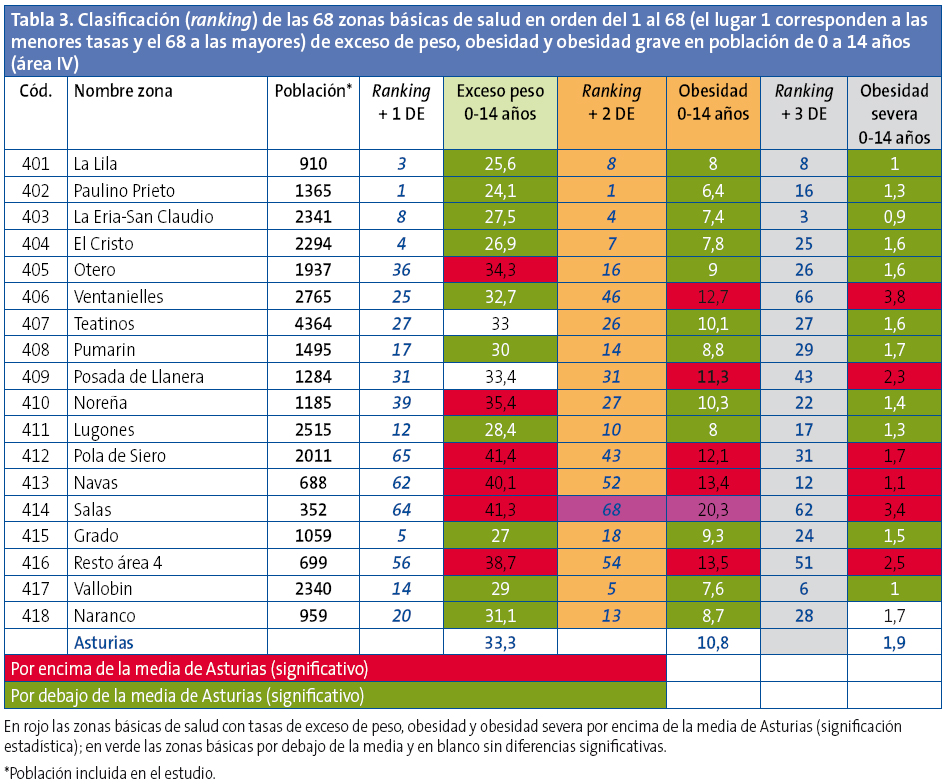
Las diferencias de prevalencia de exceso de peso y obesidad son muy importantes entre las zonas básicas de salud aún dentro de una misma área sanitaria. Las menores diferencias (dos puntos) se observan en el área II, con tan solo dos zonas básicas de salud. Las mayores diferencias se observan en el área IV, con 18 zonas básicas de salud, donde la diferencia es de 17,3 puntos (tasas entre 41,4 y 24,1) (Tabla 4).
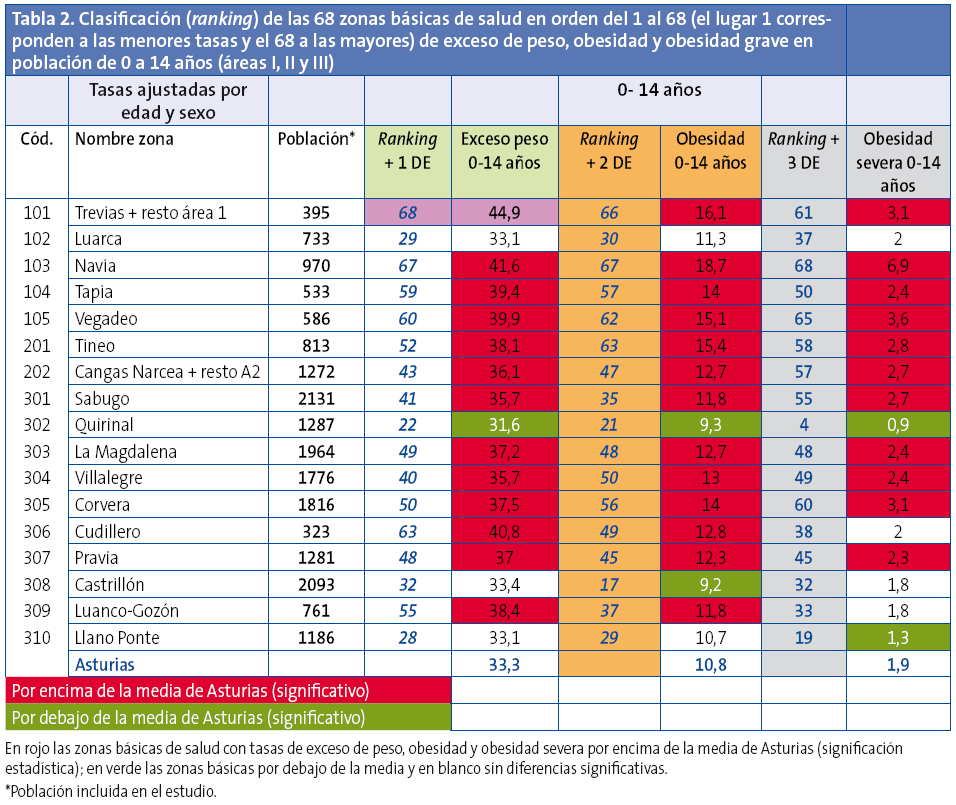
Las diferencias entre las 68 zonas básicas estudiadasllegan, para el exceso de peso, a 20,8 puntos (tasas entre 44,9 y 24,1) y para la obesidad, a 13,9 puntos (tasas entre 20,3 y 6,4).
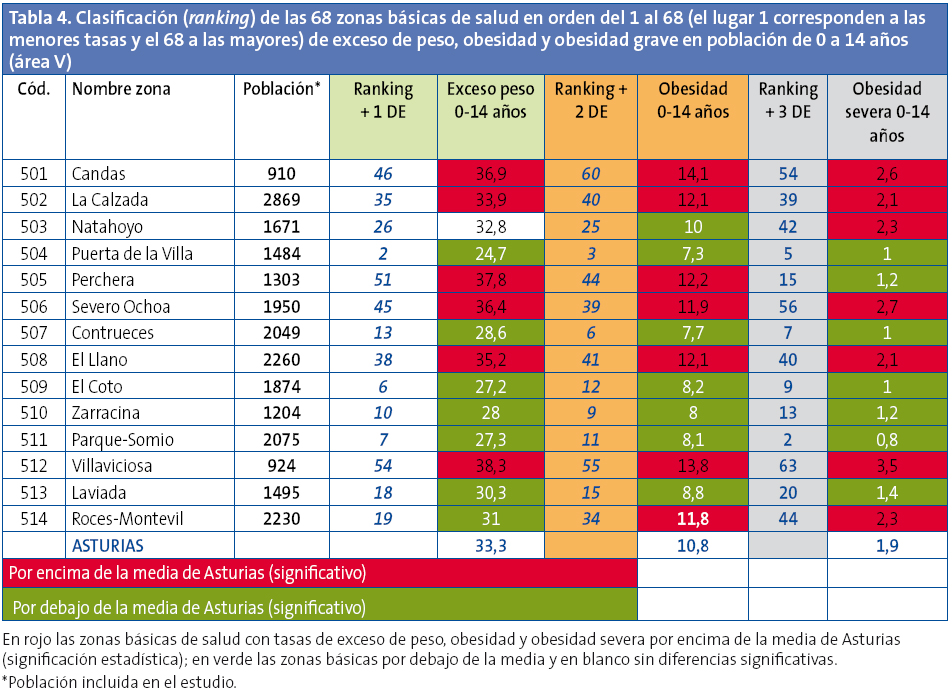
Se elaboró una clasificación con las zonas básicas de salud, clasificándolas según sus prevalencias ajustadas de sobrepeso, obesidad y obesidad grave; se exponen además para cada una de ellas: en color rojo las que presentan diferencias significativas por encima de la medias de Asturias, en color verde las prevalencias por debajo de la media y en blanco las que no presentan diferencias significativas (Anexo 1, Tablas 2, 3, 4 y 5).
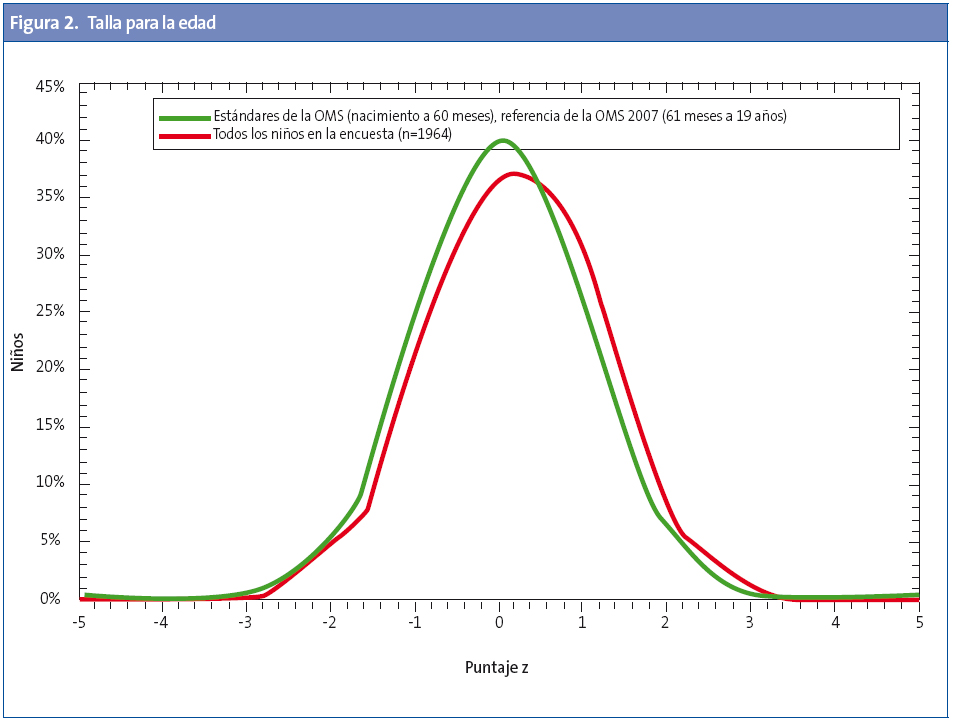
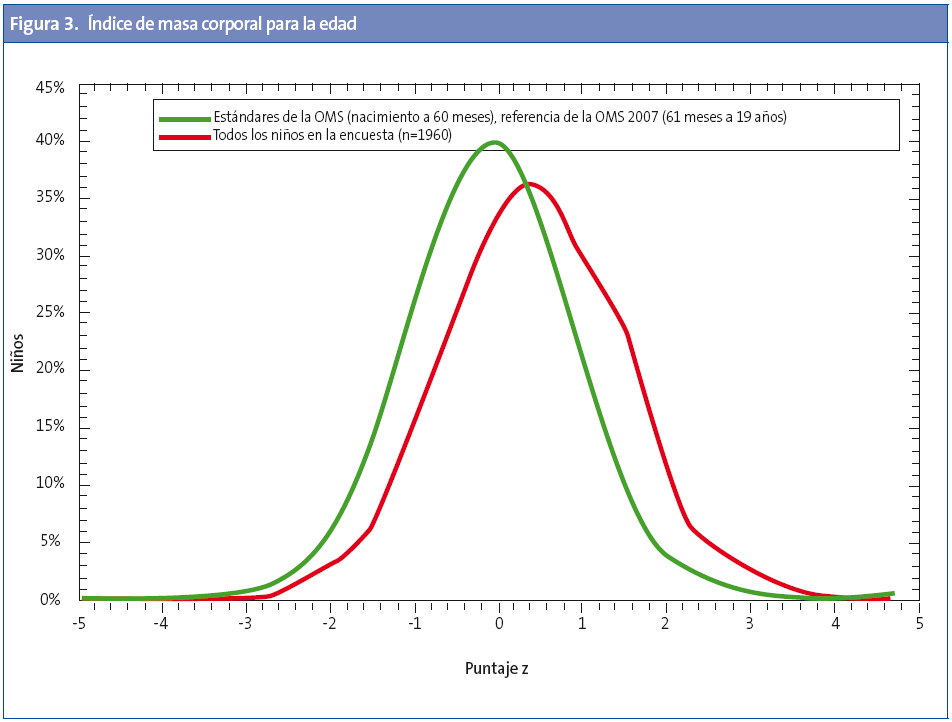
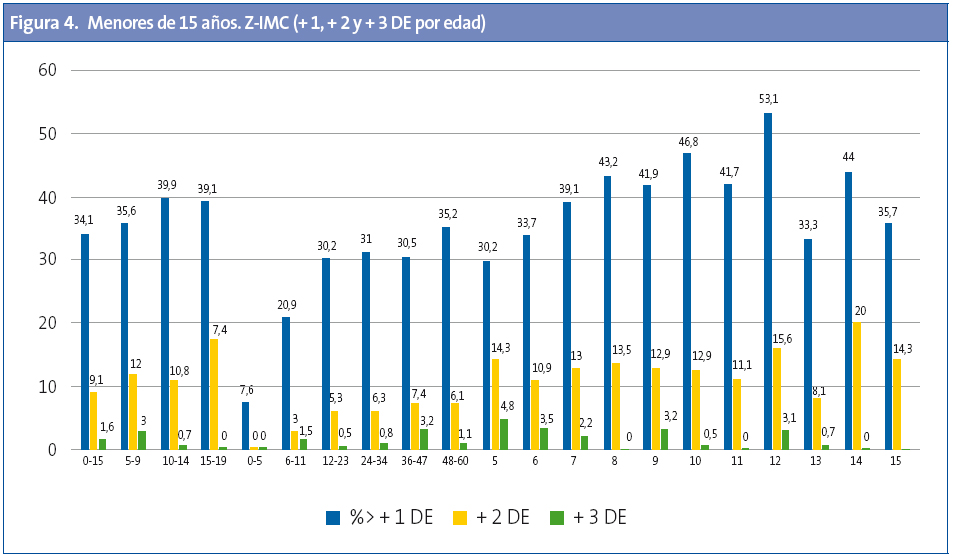
Para cada profesional (Anexo 2) se obtienen los siguientes datos del conjunto de sus pacientes: 1) prevalencias de baja talla, delgadez, sobrepeso, obesidad y obesidad grave; 2) comparativa de sus pacientes con el patrón de gráficas de la OMS para la talla/edad y el IMC para la edad, y 3) el listado de sus pacientes con la asignación de Z-standard para la talla/edad, peso/edad e IMC/edad (Z-antropométrica).
DISCUSIÓN Y CONCLUSIONES
Este estudio, por su diseño, presenta varias ventajas para los clínicos con respecto a otros publicados; en primer lugar se han utilizado criterios y parámetros de comparación internacionales propuestos por la OMS, que presentan modelos saludables que tienen validez para uso clínico y epidemiólogo, lo que evita las cifras diferentes de otros trabajos que utilizan criterios epidemiológicos distintos de los utilizados en la práctica clínica.
En segundo lugar el estudio ha utilizado todos los registros de las tarjetas sanitarias de los menores de 15 años. En España todos los niños tienen, por ley, derecho a la asistencia sanitaria sin tener en cuenta la situación administrativa regular o irregular. Ello ha permitido que todos los niños puedan tener calculado su Z-standard antropométrico y ofrecer una radiografía del estado de nutrición de la población infantil asturiana desde el nivel individual al de los cupos pediátricos, zonas básicas de salud, áreas sanitarias y la comunidad autónoma.
Otra ventaja añadida es que no ha sido necesario realizar ninguna inversión extraordinaria para obtener la fuente de datos; habitualmente, la recogida de datos suele ser una de las tareas con mayor dificultad y que requiere mayor inversión.
Limitaciones
Este estudio tiene varias limitaciones:
- Cada niño tiene un registro, el de su última medida; por lo que las fluctuaciones que haya podido tener a lo largo del tiempo no son detectadas. Dado que la mayoría de los niños son valorados antropométricamente durante las consultas del programa de salud infantil, los niños mayores tienen las medidas concentradas en determinados años de edad (6, 10-11 y 13-14) de manera que en años donde no estaba previsto que hubiera revisión el número “n” de los registros difiere de los años adyacentes. Por este motivo, sobre todo en zonas con poca población, donde el número de niños correspondientes a cada año de edad es bajo, recomendamos contemplar los datos con cautela y hacerlo por tramos etarios más amplios.
- Aunque en todos los centros de salud los materiales de medición antropométrica son homologados y las medidas son tomadas por enfermeras y pediatras con formación específica, existe la posibilidad de que las medidas, tomadas por muchos actores, puedan tener errores de ejecución o registro. Sin embargo, puesto que las decisiones clínicas son tomadas en base a estos resultados, consideramos que las ventajas superan con creces el posible margen de error, que en todo caso sería muy inferior al existente en otros estudios basados en cuestionarios a padres o a resultados basados en muestras que, extrapoladas, tendrían representatividad tan solo a nivel autonómico, pero no local. Es preciso además considerar el valor de este estudio que devuelve los datos de sus propios pacientes al pediatra lo que no se cumple en otro tipo de trabajos.
- Se desconocen datos socioeconómicos o familiares que permitan efectuar un análisis de las causas, si bien la localización geográfica permite intuir que las zonas rurales y más aisladas presentan unas cifras claramente peores, lo que sugiere la existencia de causas multifactoriales sobre todo en el tema del sobrepeso y obesidad ya que en el resto de parámetros (bajas tallas y bajo peso e IMC), no se han registrado diferencias a destacar.
Resultados
Lo primero a destacar del estudio es que no hay indicios de patología por desnutrición en la población infantil asturiana, en estos momentos de crisis en los que se barajan cifras en España de pobreza infantil elevadas, ya que el 1,1% de bajo peso y bajo IMC está dentro de lo esperable y atribuible a patologías crónicas, antecedentes de prematuridad, etc. La baja talla (1,8%), que puede detectar desnutrición también, está dentro de márgenes normales.
Los resultados mostraron la existencia de prevalencia alta de exceso de peso, con distribución muy heterogénea entre áreas sanitarias y zonas básicas de salud.
Es importante señalar que la obesidad alcanza tasas cercanas a la media de Asturias a edades tempranas: a los tres años de edad es ya de 8,1 (media de 10,8).
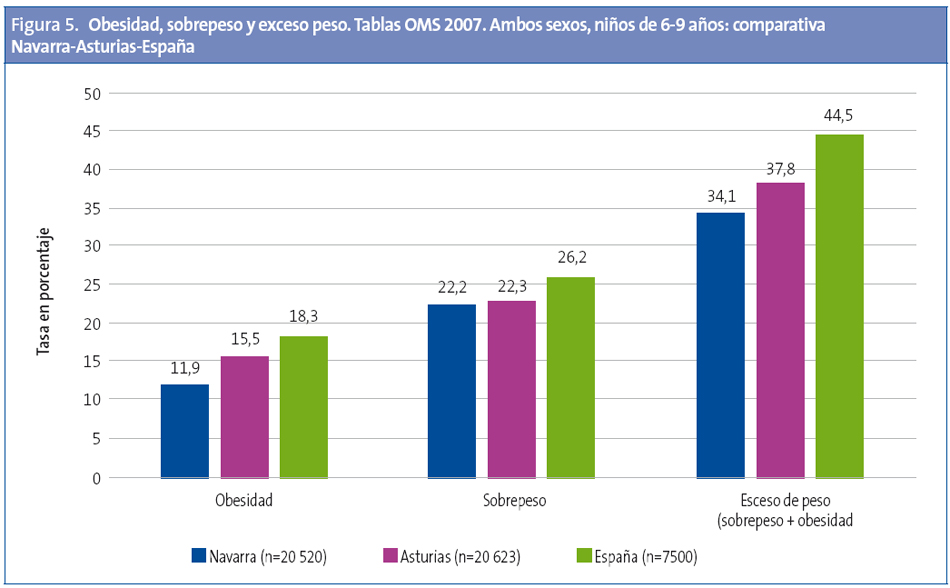
En el tramo de 6-9 años, la prevalencia de sobrepeso y obesidad en Asturias a partir del presente estudio, realizado con los mismos criterios que el estudio nacional ALADINO11, es menor que en aquel y mayor que en el efectuado en Navarra (Fig. 5)
En cuanto a la tendencia, aunque los estudios no son homogéneos, no se observan diferencias significativas entre el actual y el realizado en Asturias en el año 2006.
Estudios a partir de encuestas a la población presentan sesgos importantes12, como el realizado también en Asturias con 291 niños de entre nueve y diez años, en el que el porcentaje de obesidad es del 6,02% a partir de los datos de los encuestados y del 15,06% con los datos de los evaluadores, cifra más próxima a nuestro estudio con un 16,9% de obesidad a los diez años.
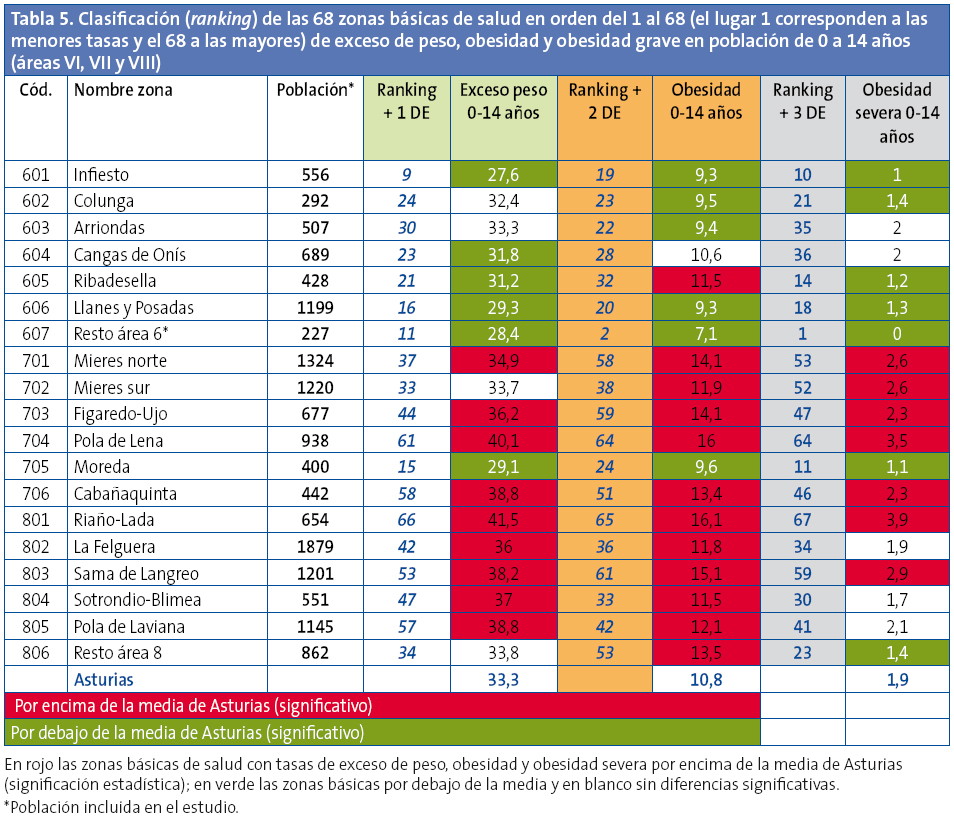
Hay que destacar las diferencias tan importantes observadas no solo en las distintas áreas sanitarias sino entre las zonas básicas de una misma área, a excepción de las áreas I (con las tasas más altas) y VI (con tasas bajas y homogéneas) (Tabla 5).
En la clasificación en orden a las mayores prevalencias de las 68 zonas básicas de salud estudiadas para el exceso de peso, la obesidad y la obesidad grave, se observa que ocho centros de salud presentan las mayores prevalencias para todos los parámetros estudiados y algunos centros de salud presentan, de manera aislada, peores resultados en tan solo uno de los parámetros medidos, posiblemente en relación con bolsas de población de características específicas.
De las 68 zonas básicasestudiadas, 34 presentan un exceso de peso por encima de la media de Asturias (significación estadística), 38 se sitúan por encima de la media en obesidad y 31 en obesidad grave; 24 zonas básicas están por debajo de la media de Asturias en la prevalencia de exceso de peso, 27 en obesidad y 25 en obesidad grave. Queda pendiente investigar las causas de estas grandes diferencias.
Conclusiones
El registro electrónico de la información clínica (OMI-AP) permite estimar la prevalencia de obesidad infantil y otras alteraciones del desarrollo en Asturias.
Las altas prevalencias de sobrepeso y obesidad comienzan a edades tempranas (en el tercer año de vida). Las diferencias en sobrepeso y obesidad son importantes no solo entre las diferentes áreas sanitarias sino también entre las zonas básicas de una misma área, algunas de las cuales presentan tasas menores o iguales a las de los países de menores prevalencias del estudio COSI14. El conocimiento de esta diversidad permitirá diseñar y priorizar de manera específica las intervenciones destinadas a la población infantil de Asturias.
Los datos correspondientes a cada pediatra y su comparación con los globales serán una ayuda para ellos y las enfermeras en el abordaje de los trastornos nutricionales de sus poblaciones asignadas.
AGRADECIMIENTOS
A todos los pediatras y enfermeras de los centros de salud de Asturias por la calidad de sus registros y las altas coberturas de atención a la población infantil. A los Servicios Centrales del SESPA por aportar la base de datos. A la Asociación Española de Pediatría de Atención Primaria por apoyar estos trabajos. A la Asociación Asturiana de Pediatría de Atención Primaria por su ayuda.
CONFLICTO DE INTERESES
Este trabajo ha sido auspiciado por la Asociación Española de Pediatría de Atención Primaria (AEPap) y no ha recibido ningún otro tipo de financiación. Los autores declaran no tener conflicto de intereses.
ABREVIATURAS: AP: Atención Primaria; CC. AA.: comunidades autónomas; CIAS: código de identificación del médico; DE: desviación estándar; IASO: International Association for the Study of Obesity; IC: intervalo de confianza, IMC: índice de masa corporal; OMS: Organización Mundial de la Salud; SESPA: Servicio de Salud del Principado de Asturias; TIS: tarjeta individual sanitaria.
BIBLIOGRAFÍA
- Pembrey ME. Time to take epigenetic inheritance seriously. Eur J Human Genet. 2002;10:669-71.
- Kaati G, Bygren LO, Pembrey ME, Sjöström M. Transgenerational response to nutrition, early life circumstances and longevity. Eur J Human Genet. 2007;15:784-90.
- Currie C, Roberts C, Morgan A, Smith R, Settertobulte W, Samdal O, et al. (eds.). Young people’s health in context. Health behavior in school-aged children (HBSC) study: international report from the 2001/2002 survey.En: Organización Mundial de la Salud [en línea] [consultado el 11/03/2015]. Disponible en www.euro.who.int/__data/assets/pdf_file/0008/110231/e82923.pdf
- Ferrández A, Baguer L, Labarta Jl, Labena C, Mayayo E, Puba B, et al. Longitudinal study of normal Spanish children from birth to adulthood (anthropometric, pubertal, radiological and intellectual data. Pediatr Endocr Rev. 2005;2:423-559.
- Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index to define thinness in children and adolescent: International survey. BJM. 2007;335:194.
- WHO multicentre growth reference study group. The WHO child growth standards, length/height-for-age, weight-for-age, weight-for length, weight for height, body mass index-for-age: Methods and development. Ginebra: Organización Mundial de la Salud; 2006.
- De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull WHO. 2007;85:660-7.
- De Onis M, Blössner M, Borghin E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257-64.
- Shields M, Tremblay MS. Canadian childhood obesity estimates based on WHO, IOTF and CDC cut-points. Int J Pediatr Obes. 2010;5:265-73.
- De Onis M, Lobstein T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Inter J Pediatr Obes. 2010;5:458-60.
- AESAN. Estudio de prevalencia de la obesidad infantil – Estudio ALADINO (Alimentación, Actividad física, Desarrollo Infantil y Obesidad). En: Ministerio de Sanidad, Servicios Sociales e Igualdad [en línea] [actualizado el 18/06/2013, consultado el 11/03/2015]. Disponible en www.naos.aesan.msps.es/naos/investigacion/aladino/
- Amigo I, Busto R, Pena E, Fernández C. Prevalencia de sobrepeso y obesidad en los niños de 9 y 10 años del Principado de Asturias: el sesgo de la valoración de los padres. An Pediatr (Barc). 2013;79:307-11.
- Wijnhoven TMA. WHO European Childhood Obesity Surveillance Initiative 2008: weight, height and body mass index in 6-9-year-old children. Pediatr Obes. 2013;8:79-97.
ANEXO 1
ANEXO 2