
Vol. 25 - Num. 99
Original Papers
How do children in Castilla y León use their mobile phones?
M.ª Cristina García de Riberaa, María Alfaro Gonzálezb, María Tríguez Garcíac, Ana Fierro Urturid, Marta Esther Vázquez Fernándeze, Franco Sorgef, Eva M.ª Dulce Lafuenteg, Elena Santamaría Marcosh, M.ª Fe Muñoz Morenoi
aPediatra. CS Tórtola. Valladolid. España.
bServicio de Pediatría. Hospital Medina del Campo. Valladolid. España.
cPediatra. CS Eras del Bosque. Palencia. España.
dPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
ePediatra. CS Circunvalación. Valladolid. España .
fPediatra. CS Aranda Norte. Aranda de Duero. Burgos. España.
gPediatra. CS Aranda Sur. Aranda de Duero . Burgos. España.
hPediatra. CS López Saiz. Burgos. España.
iBioestadístico. Unidad de Apoyo a la Investigación. Hospital Clínico Universitario de Valladolid. España.
Correspondence: MC García. E-mail: cristinaderibera@hotmail.com
Reference of this article: García de Ribera MC, Alfaro González M, Tríguez García M, Fierro Urturi A, Vázquez Fernández ME, Sorge F, et al. How do children in Castilla y León use their mobile phones? . Rev Pediatr Aten Primaria. 2023;25:251-60. https://doi.org/10.60147/d3636814
Published in Internet: 13-09-2023 - Visits: 12568
Abstract
Introduction: mobile phones are a great tool for communication between peers, but inappropriate use can affect family and social relationships and school performance.
Objectives: the primary objective of the study was to assess the use of mobile phones in the paediatric population of several health areas in Castilla y León.
Material and methods: prospective multicentre study in several primary care centres and one regional hospital.
We provided a questionnaire to the adults accompanying children to their visits and to the adolescents who agreed to participate, and the latter also completed a test of mobile phone dependence (TMD).
Results: the mobile phone is the electronic device that children used the most to browse the internet. The average age at which they received their first mobile phone was 10.35 years, and most of them had internet access.
Sixty-eight percent of participants access the internet without any form of parental control. Seventy percent of parents had established mobile phone use rules. One third recognized that these rules were not being adhered to.
The daily number of hours of mobile phone use increased with the age of the children. More than 50% of the adolescents used it more than two hours a day. Younger children used the phone mainly to watch videos and older ones to chat and for social media.
The use of mobile phones was associated with to the use of prescription glasses, but not with academic performance, sleep problems or physical activity.
In the TMD, there were many affirmative answers to items in the four sections that the test is structured into, and especially in the section concerning lack of control.
Conclusions: the mean age at which children received their first mobile phone is lower than recommended. Mobile phone abuse can generate behaviours with features characteristic of addiction.
Keywords
● Addiction ● Internet ● Smartphone ● TechnologyINTRODUCTION
Thanks to mobile phones, or smartphones, we now have constant access to the internet. Most people, in fact, access the internet through their phones.
Mobile phones are a great tool that facilitates communication between peers, but excessive or inappropriate use can have a negative impact on family and social relationships and on academic performance.1
Problematic mobile phone use (PMPU) is broadly defined as an addictive behaviour2 because it has the core components of addictive behaviours, such as cognitive salience, lack of control, mood modification, tolerance, withdrawal, conflict and relapse.3
The prevalence reported in previous studies has varied widely, ranging between 2.4 and 31.3%.4,5
A series of studies have found an association of PMPU with sedentary behaviour, decreased physical fitness, poor concentration and academic performance6 and reduced quality of life in the school and home settings. There is also evidence that PMPU is associated with dysfunctional behaviours and psychological symptoms such as fear of missing out (FoMO), hyperactivity, poor prosocial behaviour, low self-esteem, stress, anxiety, depression and suicidal ideation.
In addition, mobile phone use may have an impact on sleep quality, with evidence of an association of sleep disturbances with the use of smartphones and PMPU.7 Use of these devices, especially at bedtime, is associated with poorer outcomes in the assessment of different sleep characteristics in children and adolescents, such as inadequate sleep duration, reduced sleep quality and high daytime somnolence.8
Certain adolescents may be more susceptible to the effects of PMPU. Personality traits in the abnormal range may be associated with impairment, both in the personal and interpersonal spheres, as well as addictive behaviour and problematic use of technology.9
In this context, our aim was to conduct a survey of the paediatric population of several health care areas in the region of Castilla y León, Spain, concerning mobile phone use.
MATERIAL AND METHODS
We conducted a multicentre, prospective, cross-sectional, observational and descriptive study. Participants were recruited from one primary care centre in Burgos, two in Aranda del Duero, two in Valladolid and one in Palencia as well as the outpatient clinics of the Hospital de Medina del Campo during visits made to these centres, between July and October 2022.
During this period, we gave parents of children visiting the hospital or primary care centre a questionnaire regarding mobile phone use in their children. At the same time, we gave another questionnaire to adolescents aged 11 to 14 years who agreed to participate. We excluded patients aged less than 1 year or with severe neurologic or psychiatric disease.
The questionnaires included items for collection of data on sociodemographic and health-related characteristics and on the usual utilization of the mobile phone by the child. Patients aged 11 years or older were also given the test of mobile phone dependence (TMD) questionnaire, which has been validated in children from that age. It comprises 12 items grouped into 4 sections: Withdrawal/ Abuse/ Tolerance/ Loss of control (Table 1).
| Table 1. Test of dependence on the mobile phone (TDM) of Chóliz (brief version) | ||
|---|---|---|
| Items | Yes | No |
| Withdrawal | ||
| 1. I spend more time than I would like to talking on the mobile phone, gaming, chatting or using social media | ||
| 2. I have gone to bed later or slept less because I was using my mobile phone | ||
| 3. I use my mobile phone in situations where, even though not dangerous, it is not appropriate to do so (eating, while other people are talking to me, etc.) | ||
| Abuse | ||
| 4. If my mobile phone were broken for an extended period of time and took a long time to fix, I would feel very bad | ||
| 5. I need to use my mobile phone more and more often | ||
| 6. If I don’t have my mobile phone, I feel bad. | ||
| Tolerance | ||
| 7. When I have my mobile phone with me, I can’t stop using it | ||
| 8. Since I got my mobile phone, I have increased the number of WhatsApp messages I send | ||
| 9. As soon as I get up in the morning, the first thing I do is see who has called me on my mobile phone or if someone has sent me an SMS | ||
| Lack of control | ||
| 10. I don’t think I could stand spending a week without a mobile phone | ||
| 11. When I feel lonely, I use the mobile phone (calls, WhatsApp, games, social media...) | ||
| 12. I would grab my mobile phone and send a message or browse the web right now | ||
We obtained consent for the participation in the study of both the children and their parents or legal guardians. The study was approved by each participating centre as well as the Clinical Research Ethics Committee of each health care area.
The obtained data were analysed with the statistical software IBM SPSS Statistics version 24.0 for Windows. We considered p values of less than 0.05 statistically significant.
RESULTS
The questionnaire was completed by 227 adults who accompanied paediatric patients to their medical visits, who were most frequently the mothers(79.9%), followed by the father (16.4%). Most of the adult participants (47.6%) were aged 41 to 50 years, followed by those aged 31 to 40 years (38.8%). The mean age of the children was 6.92 years (Table 2). Most were Spanish nationals (88.6%) and had a single sibling (49.3%); 26.4% were only children.
| Table 2. Main results of the surveys | ||
|---|---|---|
| Sample | Adults accompanying minors aged 1 to 14 years | Adolescents aged 11 to 14 years |
| Mean age of each sample | 6.92 years | 12.58 years |
| Number of minors | 227 minors | 55 adolescents |
| Mean age at acquisition of first mobile phone | 10.35 years | 11.14 years |
|
Did not have own mobile phone Mean age |
164 (72%) 5.25 years |
7 (13%) 12 years |
|
Had own mobile phone Mean age No internet access Mean age Type of internet access:
|
63 children (28%) 11.24 years 3 children (5%) 6.67 years
|
48 (87%) 12.67 years None
|
| Parental control | 32% | 19% |
| Contract/Usage rules | 70% | 65% |
| Adherence to contract/rules | 67.8% | 51.4% |
In addition, 55 adolescents aged 11 to 14 years completed a different questionnaire. Their mean age was 12.58 years.
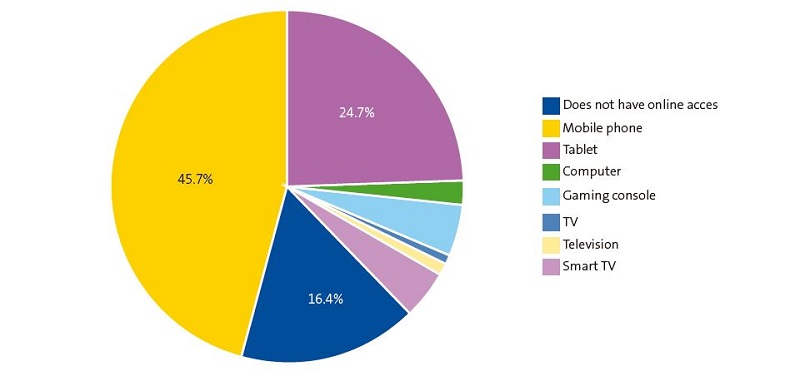
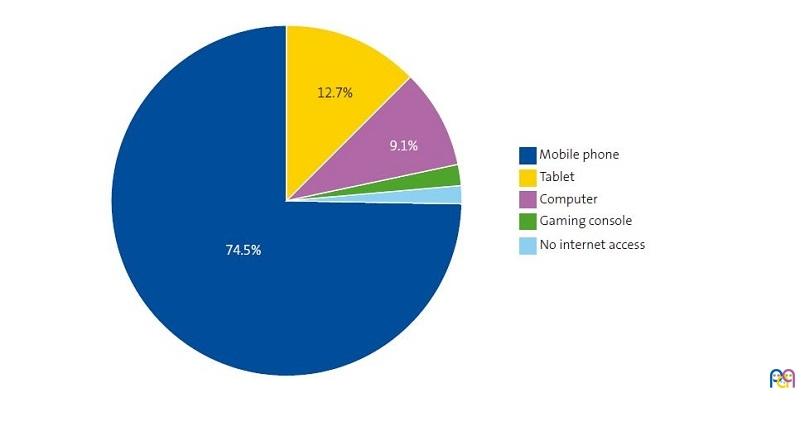
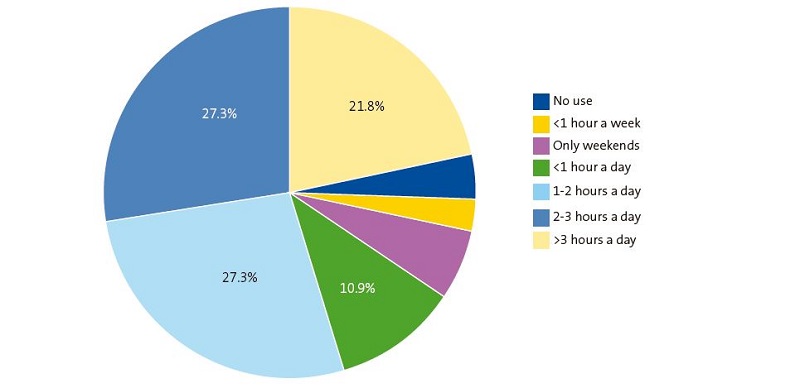
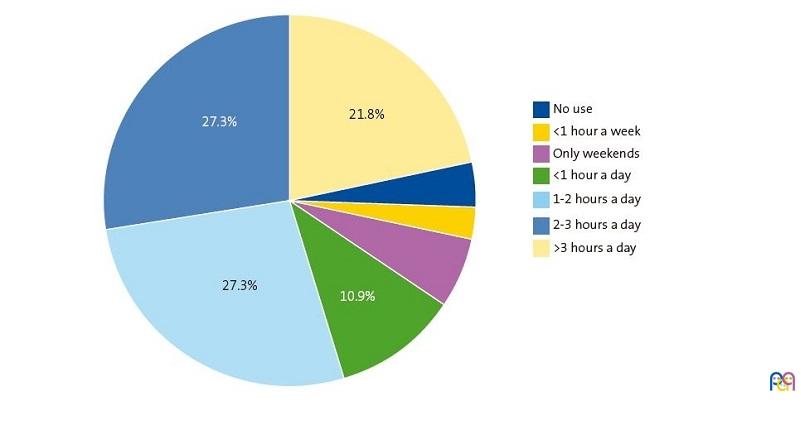
The mobile phone was the electronic device used most frequently by children in our study to access the internet (45.7%), followed by tablets (24.7%) (Fig. 1), which was also the case in adolescents (Fig. 2). More than half (50.7%) used the phone chiefly in the afternoon.
| Figure 1. Device used most frequently to access the internet |
|---|
 |
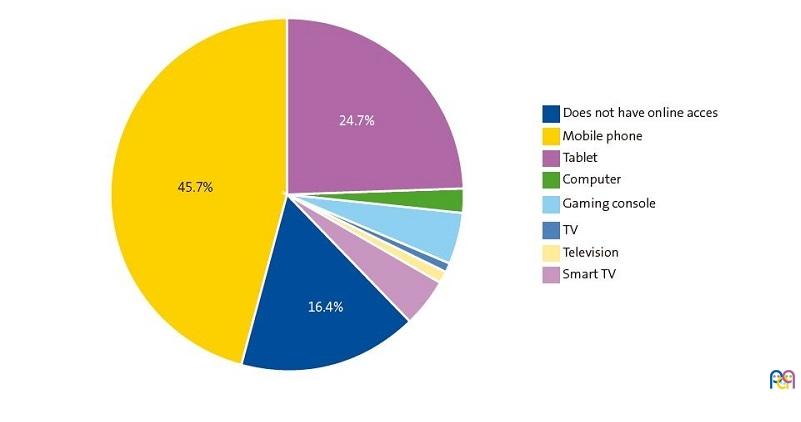
| Figure 2. Device used most frequently to access the internet (age 11 to 14 years) |
|---|
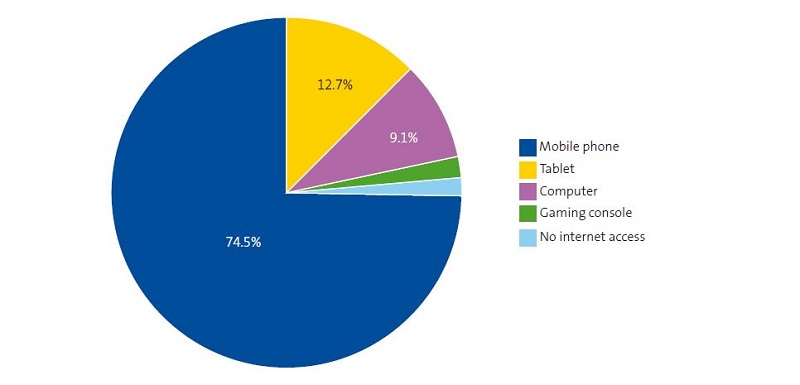 |
The mean age of the participants who used the mobile phone the most was 7.6 years, similar to the mean age of those who used the tablet. In contrast, those who used computers or game consoles more were significantly older, with mean ages of 10.14 and 9.4 years, respectively.
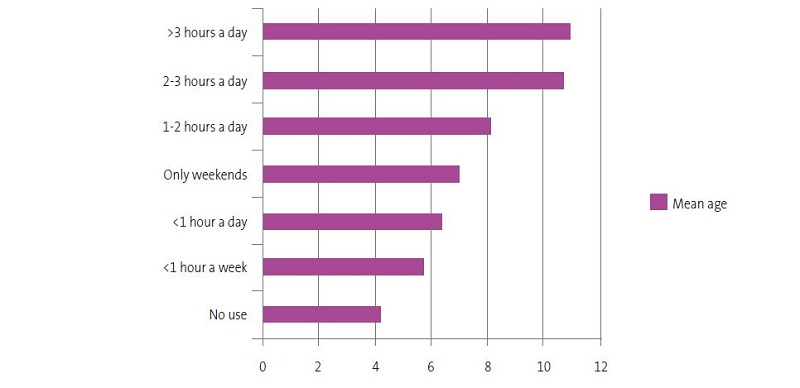
The number of hours of mobile phone use a day also increased significantly with age (Fig. 3). The mean age of the children who did not use the mobile phone every day was 5.48 years compared to the mean age of 8.3 years of children who did. Figure 4 presents the time of mobile phone use in adolescents: more than half used it more than 2 hours a day.
| Figure 3. Number of hours of daily use by age |
|---|
 |
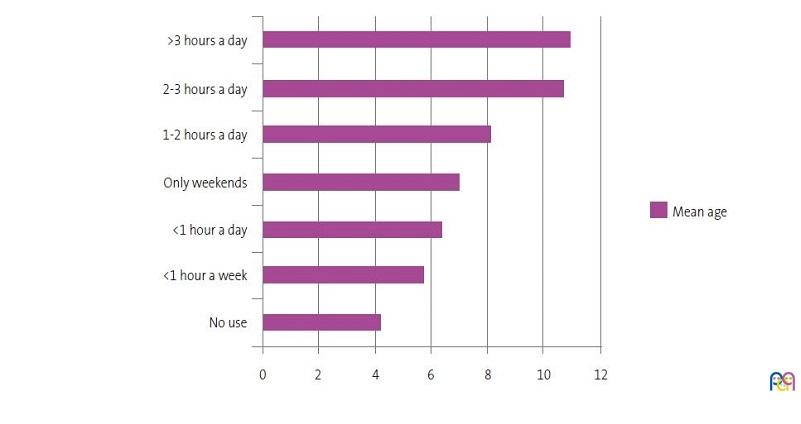
| Figure 4. Number of hours of mobile phone use in adolescents |
|---|
 |
Furthermore, when we compared what the mobile phone was used for in different age groups, we found substantial significant differences. The youngest children used it to watch videos, with a median age of 6.09 years, and older children to make calls (9.89 years), take photos or videos (8.56 years), chat through WhatsApp (10.58 years), use social media (SM) (10.76 years) and for gaming (8.5 years).
In the adolescent subset, 65.5% used the phone more in the afternoon and 63.6% reported using it for schoolwork. Most of them (67%) turned it off during class. A little over a half (54%) turned it off when they went to sleep and 45% turned it off to study.
The application used most frequently by adolescents was TikTok, followed by WhatsApp and YouTube. The mean age of those who used social media (12.73 years) was greater compared to those who reported not using SM applications (12.14 years). Among the SM users, it is worth noting that Instagram users (13.12 years) were older compared to the rest (12.13 years).
Only 2 adolescents reported having watched inappropriate content on the internet, and 6 declined to answer in this regard. Only one reported having felt bullied, 2 felt they had been mocked through SM and another 2 declined to answer. When it came to perceived abuse, 41.8% reported that they used the mobile phone more than they should and 25.5% that they might.
As regards sex/gender, we did not find significant differences between male and female adolescents in the device used most frequently to access the internet, the proportion that owned a mobile phone of their own, the hours of usage and what the phone was used for, except in gaming, which was more frequent in male compared to female adolescents: 79% versus 41%. There were also no differences between the sexes in the setting of parental controls, having or not having access to the internet, having been exposed to inappropriate content or having felt bullied or mocked online.
When it came to the age at which children received their first mobile phone, the mean age in our sample was 10.35 years, with a standard deviation (SD) of 2.08. Twenty-eight percent of children had a mobile phone of their own. More than half had received a brand new phone, while others had “passed down” phones. There were no significant differences in the mean age between these two groups.
Most children that had a mobile phone of their own had access to the Internet. Only 5% did not. When we compared the mean age of children without internet access in their mobile phone or who only had access through WiFi compared to the group that had limited or unlimited data plans, we also found significant differences: 9.58 years (no access/only WiFi), 12.95 years (limited data) and 11.88 years (unlimited data). Table 2 presents the distribution of these categories in adolescent participants.
In terms of supervising mobile phone use, 78% of adults reported controlling the applications the minor installed on the phone: 70% by establishing usage rules or the signing of a contract with the child prior to their receipt of the phone and 32% by the use of a parental control service. Most used Google’s Family Link®, and 32.2% acknowledged that their children were not adhering to the agreed rules. Also, 28.8% of adults did not check the phone of the child or adolescent to see what they posted, texted or searched. Another 50.8% reported checking every once in a while, and 28.8% checking nearly daily. In addition, 50.8% had set a schedule in which mobile phone use was allowed. Of all participants, 47.5% had their phones in their bedroom through the night. Also, 57.6% had limits in what they could spend.
Forty percent of the adults expressed concern about their children’s mobile phone usage. The mean age of children whose mobile phone usage concerned the accompanying adult (8.73 years) was significantly greater compared to children whose usage did not concern the adult (5.63). Of all adults, 33.3% stated that they did not believe they were setting a good example for children in their own usage of these devices.
We found significant differences in the educational attainment of the responsible adult in association with the type of internet access and the control of mobile phone usage. Thus, children of parents with an elementary education were more likely to have no internet access or only have access through WiFi, and these parents were also most likely to install parental control applications and monitor the download of applications. In contrast, most children of parents who completed secondary education, vocational training or university degrees had internet access, in most cases with limited data, and were less likely to be subject to parental controls. On the other hand, parental age was not significantly associated with the amount of time the children used their phones, children having a mobile phone of their own nor the characteristics of mobile phone usage or internet access.
Other aspects we analysed in relation to mobile phone usage was the family structure, the use of prescription glasses, sleep disturbances and the practice of extracurricular sports.
In the sample, 11% of the parents were separated, and we found significant differences in association with this variable in the ownership of mobile phones and the type of phone. Of the children whose parents lived together, 74.5% did not have a mobile phone, compared to 53.8% whose parents were separated. Children of parents who lived together were more likely to get brand new phone (68.6%). Children of separated parents were more likely to get a used mobile phone (66.7%). However, there were no significant differences between children whose parents lived together versus apart in the hours of mobile phone use, internet access or parental controls or supervision. We also found no association between the national origin of the family or the number of siblings and the possession (or lack thereof) of a mobile phone or what children used the mobile phone for.
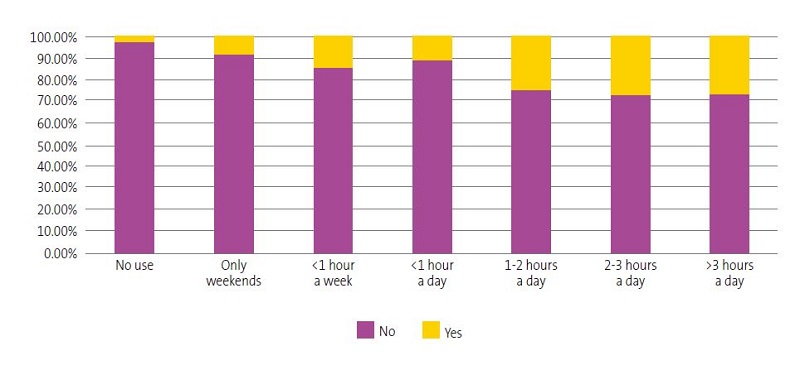
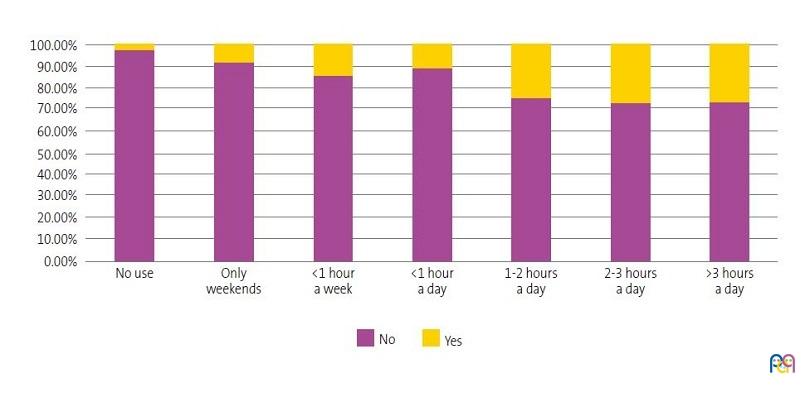
Of the children who did not own a mobile phone, only 8.6% used glasses, compared to 28.6% of children who owned one of these devices, a significantly larger proportion. We also found that the proportion of children who used glasses increased in proportion to the number of hours they used the mobile phone (Fig. 5).
| Figure 5. Use of prescription glasses in relation to the hours of mobile phone use |
|---|
 |
When it came to sleep disturbances, while the proportion of paediatric participants that had sleep problems was slightly greater among those that had a phone of their own, the difference was not statistically significant. We also found no association between the weekly hours of extracurricular sports and ownership of a phone. Lastly, we found no association between the body mass index (BMI) and the hours of usage.
Most parents thought that their children were not getting lower marks at school since getting their own mobile phone, while 16.9% did think their marks had decreased for this reason. On their part, 70.3% of adolescents reported that having their own mobile phone had not had an impact on their marks. We did not find a significant association between academic performance, the times that the phone was off or having a contract or rules in place regarding the use of the phone, whether these were upheld or not.
Last of all, we studied mobile phone dependence through the TMD questionnaire, which comprises 12 items grouped into 4 sections: withdrawal, abuse, tolerance and lack of control (Table 2). The item that the greatest number of adolescents answered in the affirmative (56%) was “When I feel lonely, I use the mobile phone (calls, SMSs, WhatsApp...)”, which is in the lack of control section. In the withdrawal section, 52% of adolescents stated “I spend more time than I would like [using] the mobile phone […]” and 42% “I have gone to bed later or slept less because I was using my mobile phone”. In the tolerance section, 44% stated “As soon as I get up in the morning, the first thing I do is see who has called me on my mobile phone or if someone has sent me an SMS”. The section with the fewest affirmative answers was the abuse section.
We found a significant association between lack of control and an increased number of hours of mobile phone use in survey participants. There was also an association between withdrawal, abuse, tolerance and lack of control and the group by adolescents that reported thinking that they used the mobile phone too much.
We did not find an association with the group that stated that their academic performance had worsened since they had a mobile phone of their own.
DISCUSSION
The use of mobile phones in the paediatric population is widespread, as reflected in our study and the previous literature on the subject.10
In the developed world, internet access is part of our everyday lives. A European study found that nearly half the children aged 9 to 16 years have a smartphone of their own that they use daily to access the internet.11 It was only to be expected that mobile phones would be the device used most frequently by children to access the internet, as most parents and many adolescents always carry their phones with them.1
There is no widespread consensus on the minimum age recommended for owning a mobile phone, although a growing number of experts recommend postponing it as much as possible.12 Yet, the mean age at acquiring the first mobile phone is lower than recommended, as observed in our sample (10.35 years), similar to the one reported in previous studies, like the one conducted by Unicef.13
Minors are exposed to numerous dangers when they go online. Thanks to campaigns implemented from the educational and health care systems, these risks are increasingly known by children and their guardians, who set up parental controls and supervise their children’s online activity. An unexpected finding of our study was that was parents with lower educational attainment were more likely to set up parental controls. We were unable to find an explanation for this. In other studies, like the one conducted by Jiménez Morales,14 this trend was reversed.
Other authors have documented the association between mobile phone abuse and the development of behavioural and sleep problems, obesity and myopia.16 A significant volume of research is currently devoted to studying the impact of mobile phone usage on health17 and academic performance.18 In our study, we only found a statistically significant association with vision problems. A potential limitation of this result is that the prevalence of refraction errors increases proportionally with increasing age, at the same time as, as observed in our study, the hours of mobile phone use increase proportionally as well.
The minimum age recommended by WhatsApp to start using the application is 16 years. For other social media applications, like Instagram or TikTok, it is 13 years. In spite of this, their use is widespread among children, as demonstrated by our survey.
An increasing number of authors argue that problematic mobile phone use has the characteristics of addictive behaviour.3
According to the definition of dependence given by Chóliz,4 PMPU is a condition characterised by:
- Excessive use, both in terms of high economic costs and the number of calls and messages.
- Interpersonal problems associated with excessive use.
- Interference with academic or daily life activities.
- Tolerance, understood as a gradual increase in the amount of use needed to obtain the same level of satisfaction and the need to replace operative devices with newer models that appear in the market.
- Withdrawal symptoms, understood as an urgent need to use a mobile phone after some time has elapsed since it was last used, as well as mood changes when mobile use is restricted or not allowed.
- Loss of control, understood as the inability to stop the addictive behaviour.
In this study, we used the brief version of the TMD developed by Chóliz in children aged 11 or older, an age group for which the test has been validated,19 and found many affirmative answers to the items in the four domains of the test, especially in relation to lack of control. The participants were aware of their own usage as problematic, as these affirmative answers were correlated to increased mobile phone use and to the statement that they believed they used the mobile phone more than they should.
CONCLUSION
Mobile phone use habits have an important impact on children’s lives. We have found that mobile phones are the devices children use most frequency to surf the web.
The mean age at which children get their first mobile phone is lower than recommended, and in our study in particular was 10.35 years. Social media applications are used before the age recommended by the corresponding platforms.
Mobile phone abuse can generate behaviours with features consistent with addiction, as demonstrated in our study. Children can recognise mobile phone dependence from an early age.
As paediatricians, we need to be adequately educated on the use of new technologies to be able to guide families in making rational use of these devices. Our routine health check-ups should include aspects related to digital health, providing tools to facilitate adequate use of the internet and social media.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. The project was funded through the AEPap–FPS 2022 grant for research in primary care paediatrics, for which we want to express our deep appreciation.
AUTHOR CONTRIBUTIONS
All authors contributed equally to the writing of the manuscript.
ABBREVIATIONS
BMI: body mass index · FoMO: fear of missing out · PMPU: problematic mobile phone use · SD: standard deviation · SM: social media · TMD: Test of Mobile phone Dependence.
REFERENCES
- Fischer Grote L, Kothgassner OD, Felnhofer A. The impact of problematic smartphone use on children's and adolescents' quality of life: A systematic review. Acta Paediatr. 2021;110:1417-24.
- De Sola J, Talledo H, Rodríguez de Fonseca F, Rubio G. Prevalence of problematic cell phone use in an adult population in Spain as assessed by the Mobile Phone Problem Use Scale (MPPUS). PLoS One. 2017; 12(8): e0181184.
- Billieux J, Maurage P, López Fernández O, Kuss,DJ, Griffiths MD. Can Disordered Mobile Phone Use Be Considered a Behavioral Addiction? An Update on Current Evidence and a Comprehensive Model for Future Research. Addict. Rep. 2015;2:156-62.
- Chóliz M. Mobile phone addiction in adolescence: evaluation and prevention of mobile addiction in teenagers. LAP, Lambert Academic Publishing. 2010.
- Thapa K, Lama S, Pokharel R, Sigdel R, Rimal SP. Mobile phone dependence among undergraduate students of a medical college of Eastern Nepal: A Descriptive Cross-sectional Study. JNMA J Nepal Med Assoc. 2020;58:234-9.
- Alavi SS, Ghanizadeh M, Mohammadi MR, Jannatifard F, Salehi M, Farahani M, et al. Psychometric Properties of Mobile Phone Abuse (MPA): Exploratory and Confirmatory Factor Analysis in Student Mobile Users. Iran J Psychiatry. 2021 (2):187-97.
- Zhang J, Zhang X, Zhang K, Lu X, Yuan G, Yang H, et al. An updated of meta-analysis on the relationship between mobile phone addiction and sleep disorder. J Affect Disord. 2022;305:94-101.
- Dibben GO, Martin A, Shore CB, Johnstone A, McMellon C, Palmer V, et al. Adolescents' interactive electronic device use, sleep and mental health: a systematic review of prospective studies. J Sleep Res. 2023:e13899.
- Sohn S, Rees P, Wildridge B, Kalk NJ, Carter B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: A systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019;19:1-10.
- Mascheroni G, Ólafsson K. The mobile Internet: Access, use, opportunities and divides among European children. New Media & Society 2016;18:1657-79.
- Smahel D, Machackova H, Mascheroni G, Dedkova l, Staksrud E, Ólafsson K, et al. EU Kids Online 2020: Survey results from 19 countries. EU Kids Online. (2020) [online] [accessed 05/09/2023]. Available at www.lse.ac.uk/media-and-communications/research/research-projects/eu-kids-online/eu-kids-online-2020
- Dienlin T, Johannes N. The impact of digital technology use on adolescent well-being. Dialogues Clin Neurosci. 2020;22:135-42.
- Andrade B, Guadix I, Rial A, Suárez F. Impacto de la tecnología en la adolescencia. Relaciones, riesgos y oportunidades. (2021). Madrid: UNICEF España [online] [accessed 05/09/2023]. Available at www.unicef.es/publicacion/impacto-de-la-tecnologia-en-la-adolescencia
- Jiménez Morales M, Montaña M, Medina Bravo P. Childhood use of mobile devices: Influence of mothers’ socio-educational level. Rev Comunicar 2020 64 XXVIII.
- Álvarez Peregrina C, Sánchez Tena MÁ, Martínez Pérez C, Villa Collar C. The Relationship Between Screen and Outdoor Time With Rates of Myopia in Spanish Children. Front Public Health. 2020;8:560378.
- Wang J, Li M, Zhu D, Cao Y. Smartphone Overuse and Visual Impairment in Children and Young Adults: Systematic Review and Meta-Analysis. J Med Internet Res. 2020;22:e21923.
- Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9:e023191.
- Yadav MS, Kodi SM, Deol R. Impact of mobile phone dependence on behavior and academic performance of adolescents in selected schools of Uttarakhand, India. J Educ Health Promot. 2021;10:327.
- Cerutti R, Presaghi F, Spensieri V, Fontana A, Amendola S. Adaptation and Psychometric Analysis of the Test of Mobile Phone Dependence-Brief Version in Italian Adolescents. Int J Environ Res Public Health. 2021;18:2612.