

Test for the early detection of reading and writing learning disabilities
Fernando Cuetosa, P Suárez-Coallab, M. I Molinac, M. C Llenderrozasd
aDepartamento de Psicología. Universidad de Oviedo. España.
bDepartamento de Psicología, Universidad de Oviedo. España.
cPediatra. CS de Durango. Vizcaya. España.
dEnfermera Pediátrica. CS de Durango. Vizcaya. España.
Correspondence: F Cuetos. E-mail: fcuetos@uniovi.es
Reference of this article: Cuetos F, Suárez-Coalla P, Molina MI, Llenderrozas MC. Test for the early detection of reading and writing learning disabilities. Rev Pediatr Aten Primaria. 2015;17:e99-e107.
Published in Internet: 18-06-2015 - Visits: 201698
Abstract
Introduction: the diagnosis of dyslexia usually occurs several years after the literacy learning begins. By then, many dyslexic children have faced academic failure and loss of self-esteem. An early diagnosis could avoid many of these problems. Furthermore, intervention programs are more effective when applied early.
Objectives: the aim of this study was to develop a test for the early diagnosis of dyslexia, based on phonological processing deficits presented by these children, and applicable to four years old children, before they face reading.
Material and methods: the test consists of six subtasks with five items each, which can be passed between six and ten minutes. The six subtasks evaluate the main components of phonological processing: discrimination of phonemes, syllable segmentation, phoneme identification, repetition of pseudowords, verbal short-term memory and verbal fluency.
Results: the data, obtained from a sample of 298 four years old children, show a good reliability and high construct validity of the test. Normative values are given in percentiles and cutoffs, below of which children are considered at risk of suffering dyslexia.
Conclusions: the application of this simple test to children in pediatric clinics and early childhood education schools, will allow the detection of children at risk for dyslexia, in order to intervene as early as possible, before they face the literacy learning.
Keywords
● Dyslexia ● Phonological processing ● Prevention testINTRODUCTION
Learning to read and write is one of the main challenges that children must face in the early years of schooling. Most of them can meet this challenge without excessive difficulty, but there is a significant percentage that experience serious learning disabilities, which probably lead to school failure, as most educational contents are delivered through reading materials.1 Some of these cases only involve a delay in reading caused by family problems, low motivation, etc, while others are due to a dyslexic disorder of neurobiological aetiology. Although there are widely variable estimations of the proportion of dyslexic children in the literature, some authors mention figures of 17%.2 In Spanish-language populations, in which spelling is pretty straightforward, the percentage is estimated at 3% to 4%.3,4
Dyslexia is detected several years after children start to learn to read and write, when certain children fail to properly acquire these skills despite making an effort to learn and having normal cognitive skills and favourable family and school environments. This leads to delays in academic performance compared to their peers, and what is more worrisome, to a considerable decrease in self-esteem. The longer it takes to address the issue, the harder it is to remedy it, as children gradually become unmotivated and lose interest in reading, while their brain plasticity decreases. In fact, when dyslexic disorders are detected early, intervention outcomes are significantly better.5,6
The point is how to predict the potential presence of reading disabilities as early as possible, since, as we know, it is not until the child has started learning and several years have passed without success that we can speak of dyslexia. But by then, precious time has been lost during which interventions would have been highly effective. Ideally, treatment would start at an early age, even before children start being taught reading and writing in school. To do so, it would be necessary to know the predictive factors for reading, that is, to know whether there are any abnormalities in dyslexic children that lead to their problems in learning to read and write.
Numerous studies conducted in recent decades clearly point at phonological processing.7-9 Adequate phonological processing is essential to learn how to read and write, as reading consists in turning graphemes or letters into phonemes, and writing in turning phonemes into letters. Thus, if a child has trouble discriminating phonemes, cannot segment speech into smaller units like syllables or phonemes, or is unable to hold several phonemes in short-term memory while reading or writing a word, the child will definitely have difficulty learning to read and write. In fact, all dyslexic children have difficulties in phonological processing. In agreement with this, the definition given by the International Dyslexia Association (2002) literally states that "dyslexia is a specific learning disability that is neurobiological in origin. It is characterised by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language."10
In this regard, there are several types of empirical studies that support a causal relationship between phonological awareness and reading and writing. The most important ones are:
- Longitudinal studies that demonstrate that children with better phonological skills learn to read and write earlier. Numerous studies have been conducted in the English language that prove this relationship.11-13 One study conducted in Spanish14 had 50 preschoolers undergo several phonological processing tests before starting to learn to read and write, specifically in the second year of Spanish preschool, with a mean age of 4 years and 3 months. The tasks involved discriminating phonemes, repeating made-up words (pseudowords), short-term memory tasks and quickly naming objects. Two and a half years later, when children finished the third year of preschool, at a mean age of 5 years and 10 months, the children performed several tasks from the PROLEC-R reading test15 and the PROESC16 writing test. The authors found a strong correlation between the results in the phonological processing tasks and the results in the reading tasks, with children that had scored high in phonological tasks also scoring high in reading and writing tasks, and children that had scored low in phonological tasks showing greater difficulties in reading and writing two and a half years later.
- Intervention studies that show that training in phonological skills leads to improved reading and writing. Numerous studies17-22 have demonstrated that just by practising phonological awareness exercises, children in the early years of school automatically improve on their reading and writing skills.
- Studies that show that children with phonological deficits go on to experience difficulties reading and writing.23-25 Lyytinen;et al26 followed up a group of Finnish-speaking at-risk children over several years, evaluating them every six months. They were considered to be at risk because they had a family history of dyslexia. When the children developed language, the authors started evaluating their performance in phonological tasks such as differentiating between “ata” with a short consonant and “atta” with a long consonant. At-risk children were observed to have greater difficulty performing this kind of tasks, and when reading started to be taught, many of these children displayed significant reading disabilities.
Therefore, in light of the intimate relationship between phonological processing and reading and writing, phonological processing is unquestionably the best predictor of how well children will learn to read and write. Furthermore, training on phonological skills considerably improves the learning of reading and writing. In fact, it is the most appropriate and successful type of intervention in dyslexic children, especially when it is done at a very early age.6,21,27 Simos et al6; obtained images of the brain by means of magnetoencephalography of a group of at-risk children at 4 years of age, and observed a lesser activation of the superior temporal region of the left hemisphere, an area involved in phonological processing, compared to a control group of children of the same age. Subsequently, at-risk children participated in an intervention programme twice a week. Four months later, the authors observed that the children’s phonological processing had improved considerably, but the most interesting finding was that neuroimaging now showed an activation of the superior temporal region in the left hemisphere that was similar to that of control children. This seems to suggest that speech therapy interventions at age 4 years are much more successful, due to brain plasticity at that age.
In light of these results, it seems that early detection of children at risk of reading learning disabilities is of the essence, even before formal reading training starts. If a quick- and easy-to-administer test were available to paediatricians that perform the 4-year checkup and to teachers of second year of early childhood education, they could identify many of the at-risk children and bring up the need for speech therapy in these children. This would undoubtedly prevent many cases of reading and writing disorders.
The aim of this study was to develop such a test, that is, one of quick implementation, but sensitive to phonological abnormalities. To achieve this, we used tasks that were short and that measured different aspects of phonological processing, such as phoneme discrimination, phonological awareness, repetition of unknown words, short-term memory and verbal fluency. These activities are related, but require different processes and involve different areas of the brain.28 Thus, its purpose would be to identify children at risk of suffering reading and writing learning disorders to be able to intervene and prevent the development of those very disorders.
MATERIALS AND METHODS
Participants
A total of 298 children 4 years of age participated in the study; 122 were evaluated in paediatric offices in various health care centres in the basic health zones of Bilbao and the Comarca Interior de Vizcaya when they came for their 4-year checkup. The other 176 children were evaluated in early childhood education centres in Amorebieta, Donostia and Oviedo. All tests were performed individually.
Materials
As seen in Appendix 1, the test consisted of six phonological processing subtasks. The first one involved phoneme discrimination, the second syllable segmentation, the third phoneme identification, the fourth pseudoword repetition, the fifth memory span using digits, and the sixth verbal fluency. Each subtask was scored on a scale of 0 to 5, so the overall score ranged between 0 and 30.
Task
Each child was given the subtasks that compose the test in the order that they appear and following the directions included in the appendix. Before children were given the items that get scored, they were given several trial items to ensure that they had understood the directions.
RESULTS
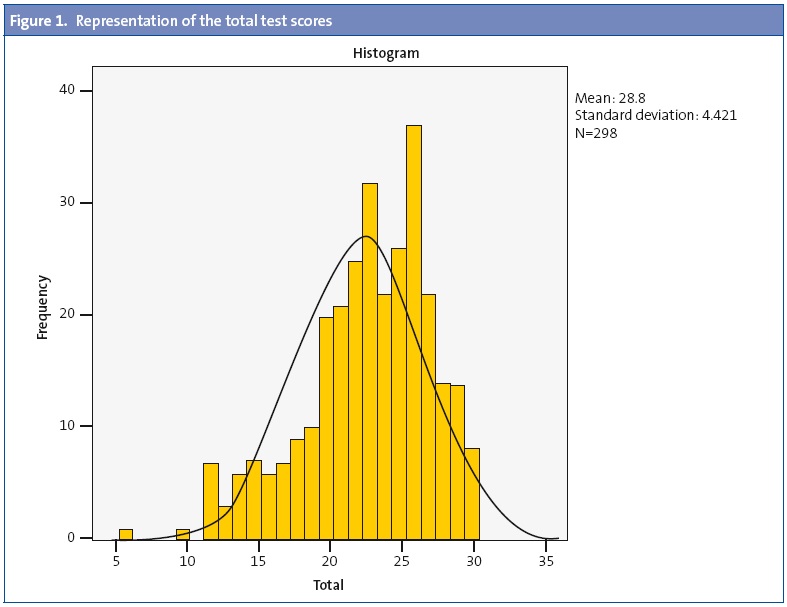
As Table 1 shows, the mean score was 22.80 over 30. The mean score for each subtask ranged from 3.26 in the verbal fluidity task to 4.27 in the phoneme discrimination task.

Figure 1 shows the distribution of the scores, which fit a normal distribution with a slight increase in the left tail that results from the children that have phonological processing difficulties.
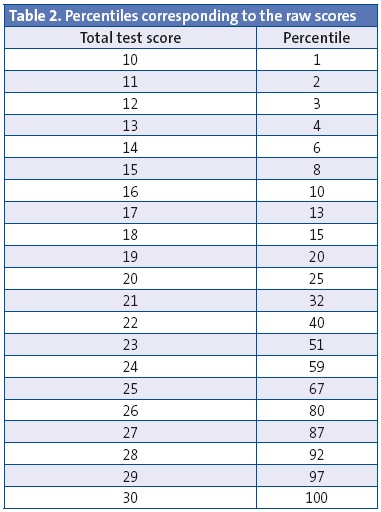
We calculated the percentiles based on the scores of all participants (Table 2).
Furthermore, with the purpose of establishing qualitative categories based on quantitative data, we considered that scores between one standard deviation (SD) below the mean and one SD above the mean were normal, as is usually done. That is, scores between 18.38 (22.80 -4.42) and 27.22 (22.80 +4.42) were considered normal scores. Scores above 27 would correspond to children that performed well, and scores under 18 to children at risk. If we were to apply a standard deviation and a half rather than a single SD, the cut-off point would be at 16.17. This value suggests that we could consider any children with scores below 16 as severe cases. There were 31 children in all that scored 16 or less, which amounted to 10.4% of the total.
In the end, based on the data obtained from this sample, we can establish the following four categories: a) between 27 and 30 points: good performance; b) between 18 and 27 points: normal; c) between 16 and 18 points: mild difficulties, and d) less than 16 points: severe difficulties.
Reliability
We calculated the reliability by means of Cronbach’s α using the number of correct answers in all of the tests. The Cronbach’s α was 0.73, a very high value that indicated that the test is very reliable.
Validity
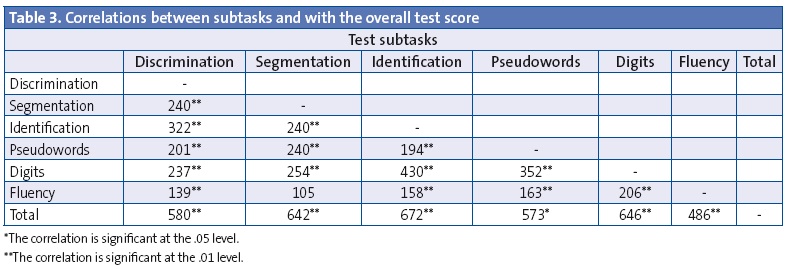
We assessed construct validity by means of the correlations between the six subtasks that compose the test and between the subtasks and the overall test score. As can be seen in Table 3, there are strong correlations between the subtasks, and these correlations are statistically significant except for the one between verbal fluidity and syllable segmentation. As for the correlations between the subtasks and the overall test score, they were all very strong, with the highest correlation corresponding to phoneme identification and the lowest to verbal fluidity.
DISCUSSION
The purpose of this study was to develop a brief test for the early detection of reading and writing learning difficulties. The early detection of these difficulties, even before formal learning of reading and writing starts, may prevent school failure and suffering in many children and families. The results of research studies in recent years clearly show that assessment of phonological processing can be used to identify children at risk of having these learning difficulties.11,14,29
Therefore, in developing this test we took into account different aspects of phonological processing, all of which were related to reading and writing, such as phoneme discrimination, phonological awareness, short-term memory and vocabulary. Phoneme discrimination allows writing from dictation; phonological awareness is necessary to break down speech into its smaller units (syllables and phonemes) to later connect them to the corresponding graphemes; short-term memory is necessary to hold verbal information while words or sentences are being read or written, and an adequate vocabulary allows learning how to read fluidly.
All of these components are deeply interconnected, and it shows in that whenever there is a deficit in any, there is usually a deficit in all, as seen in dyslexic children.30,31 These components are also correlated in the assessment of normal children.28
The data of our study, with a sample of nearly 300 children, has shown strong correlations between all the components and of the components with the overall test, which means that the test has a good construct validity. The test has also shown a high reliability based on Cronbach’s alpha, which means that it can be used to detect difficulties in phonological processing, and consequently to predict difficulties in learning reading and writing. Children that score low in this test are likely to have difficulty learning to read or write if nothing is done to prevent it. The purpose of this test is precisely to keep these difficulties from happening, as early interventions in at-risk children are much more effective.
The administration of the test in children 4 years of age is easy and quick. Completing it takes an average of six to ten minutes, and the score obtained indicates whether the child needs the support of a speech therapist to prevent problems in reading and writing. In fact, the test itself shows the cut-off values under which children are considered to be at risk. The test was designed bearing in mind the paediatricians that conduct the 4-year checkup and the early childhood education teachers who work with this age group. We are convinced that its implementation and the subsequent speech therapy interventions will prevent school failure and the loss of self-esteem in many children.
CONFLICTS OF INTEREST
This study was conducted as part of the project PSI2012-31913 of the Ministerio de Economía y Competitividad (Ministry of Economics and Competitiveness).
REFERENCES
- Cuetos F. Psicología de la lectura. Madrid: Wolters-Kluwer; 2008.
- Shaywitz SE, Shaywitz BA, Fletcher JM, Escobar MD. Prevalence of reading disability in boys and girls. Results of the Connecticut Longitudinal Study. JAMA. 1990;264:998-1002.
- Cuetos F. Dislexias evolutivas: un puzzle por resolver. Revista de Logopedia, Foniatría y Audiología. 2009;29:78-84.
- Jiménez JE, Rodríguez C, Ramírez G. Spanish developmental dyslexia: prevalence, cognitive profile, and home literacy experiences. J Exp Child Psychol. 2009;103:167-85.
- Papanicolaou AC, Simos PG, Breier JI, Fletcher JM, Foorman BR, Francis D, et al. Brain mechanisms for reading in children with and without dyslexia: a review of studies of normal development and plasticity. Dev Neuropsychol. 2003;24:593-612.
- Simos PG, Fletcher JM, Bergman E, Breier JI, Foorman BR, Castillo EM, et al. Dyslexia-specific brain activation profile becomes normal following successful remedial training. Neurology. 2002;58:1203-13.
- Snowling MJ. From language to reading and dyslexia. Dyslexia. 2001;7:37-46.
- Ramus F. Outstanding questions about phonological processing in dyslexia. Dyslexia. 2001;7:197-216.
- Ramus F. Dyslexia. Talk of two theories. Nature. 2001;412:393-5.
- Lyon GR, Shaywitz SE, Shaywitz BA. Defining dyslexia, comorbidity, teachers’ knowledge of language and reading: a definition of dyslexia. Ann Dyslexia. 2003;53:1-14.
- Caravolas M, Volin J, Hulme C. Phoneme awareness is a key component of alphabetic literacy skills in consistent and inconsistent orthographies: evidence from Czech and English children. J Exp Child Psychol. 2005;92:107-39.
- Parrila RK, Kirby JR, McQuarrie L. Articulation rate, naming speed, verbal short-term memory, and phonological awareness: Longitudinal predictors of early reading development? Scientific Studies Reading. 2004;8:3-26.
- Wagner R, Torgesen J, Rashotte C, Hecht S, Barker T, Burgess S, et al. Changing relations between phonological processing abilities and word-level reading as children develop from beginning to skilled readers: a 5 year longitudinal study. Dev Psychol. 1997;33:468-79.
- Suárez-Coalla P, García de Castro M, Cuetos F. Variables predictoras de la lectura y la escritura en castellano. Infancia y Aprendizaje. 2013;36:77-89.
- Cuetos F, Rodríguez B, Ruano E. Evaluación de los procesos lectores. PROLEC-R. Madrid: Ediciones TEA; 2007.
- Cuetos F, Ramos JL, Ruano E. Evaluación de los procesos de escritura. PROESC. Madrid: Ediciones TEA; 2002.
- Brady S, Fowler A, Stone B, Winbury N. Training phonological awareness: a study with inner-city kindergarten children. Ann Dyslexia. 1994;44:26-59.
- Ehri L, Nunes S, Willows D, Schuster B. Phonemic awareness instruction helps children learn to read: Evidence from the National Reading Panel’s metaanalysis. Reading Research Quarterly. 2001;36:250-87.
- Foorman BR, Breier JI, Fletcher JM. Interventions aimed at improving reading success: an evidence-based approach. Dev Neuropsychol. 2003;24:613-39.
- Hatcher PJ, Hulme C, Snowling MJ. Explicit phoneme training combined with phonic reading instruction helps young children at risk of reading failure. J Child Psychol Psychiatry. 2004;45:338-58.
- Temple E, Deutsch GK, Poldrack RA, Miller SL, Tallal P, Merzenich MM, et al. Neural deficits in children with dyslexia ameliorated by behavioral remediation: evidence from functional MRI. Proc Natl Acad Sci USA. 2003;100:2860-5.
- Torgesen JK, Alexander AW, Wagner RK, Rashotte CA, Voeller KK, Conway T. Intensive remedial instruction for children with severe reading disabilities: immediate and long-term outcomes from two instructional approaches. J Learn Disabil. 2001;34:33-58.
- Bruck M. Persistence of dyslexics’ phonological awareness deficits. Dev Psychol. 1992;26:874-88.
- Swan D, Goswami U. Phonological awareness deficits in developmental dyslexia and the phonological representations hypothesis. J Exp Child Psychol. 1997;66:18-41.
- Vellutino FR, Fletcher JM, Snowling MJ, Scanlon DM. Specific reading disability (dyslexia): what have we learned in the past four decades? J Child Psychol Psychiatry. 2004;45:2-40.
- Lyytinen H, Ahonen T, Eklund K, Guttorm T, Laakso M, Leinonen S, et al. Developmental pathways of children with and without familial risk for dyslexia during the first years of life. Dev Neuropsychol. 2001;20:535-54.
- Suárez-Coalla P. Intervención en dislexia evolutiva. Revista Logopedia, Foniatría y Audiología. 2009;29:131-7.
- Turkeltaub PE, Gareau L, Flowers DL, Zeffiro TA, Eden GF. Development of neural mechanisms for reading. Nat Neurosci. 2003;6:767-73.
- Défior S. ¿Cómo facilitar el aprendizaje inicial de la lectoescritura? Papel de las habilidades fonológicas. Infancia y Aprendizaje. 2008;31:333-45.
- De Jong PF, van der Leij A. Specific contributions of phonological abilities to early reading acquisition: results from a Dutch latent variable longitudinal study. J Educ Psychol. 1999;91:450-76.
- Wagner RK, Torgesen JK. The nature of phonological processing and its causal role in the acquisition of reading skills. Psychological Bull. 1987;101:192-212.
APPENDIX 1
Test for predicting reading and writing difficulties
First and Last Names / Date of Birth / Date of test administration
Phoneme discrimination (minimal pairs). “Let’s play a game. I will tell you two words and you have to tell me whether they are the same or they are different, if the words are the same or not. Pay attention: Gol-gol (they are the same), dar-bar (they sound very similar but they are not the same, they are different). Now it’s your turn: coz-coz..., mil-mis... Very well, let’s carry on!”.
pan-paz • luz-luz • pez-tez • cal-col • fin-fin
Total:
Syllable segmentation. “Now you have to clap your hands. Watch how I do it: casa ca-sa; now a longer one: ventana: ven-ta-na. Now it’s your turn, dedo: ....... vaso:..... Very good!”.
pera • lazo • cometa • oveja • mariposa
Total:
Phoneme identification. “I’m going to make a sound for you /r/, repeat it with me. Now tell me whether you hear it in these words. Is /r/ in zorro? (yes); Do you hear /r/ in the word pelo? (no). Let’s do it with other words...”.
carro • sillón • ratón • rojo • piña
Total:
Pseudoword repetition. “Now we’re going to play a repetition game. You have to repeat some words that don’t exist, because I made them up. OK? Repeat what I say: jepo, socata... Very good! Are you ready to continue?".
nigo • muspe • diplo • tingano • pelagro
Total:
Digit repetition. “I am going to tell you a few numbers and you have to repeat them. Pay good attention so you don’t miss”.
8 5
1-6 7-2
5-2-1 6-4-8
5-3-1-8 3-7-4-1
4-1-8-3-9 6-3-2-5-8
Total:
Verbal fluidity. Animal names. “What is your favourite animal? ... Great. Now tell me all the animals you can think of”.
Number of animals
Total:
Total score (over 30):
Instructions for the administration and scoring of the reading-predicting tasks
This test evaluates a series of skills related to reading acquisition: syllable awareness, phoneme discrimination, phonological memory, and verbal fluidity. The test comprises six tasks, each of which has a maximum score of 5 points, so that the maximum overall score is 30 points. The test takes approximately five minutes.
There are suggested instructions for each task, but sometimes further explanation is required for the child to understand what is expected.
- Phoneme discrimination. The child has to say whether two words are the same or different, and to that end the child is given examples of two words that are the same (mano-mano) and of two words that are different (mano-león). This task is not hard to understand. Scoring: one point given for each correctly identified pair.
- Syllable segmentation. This task measures syllable awareness, and the child is asked to segment the word into syllables by clapping hands or knocking on the table. The child will be given several examples: those included in the directions, the child’s name, the mother’s name… and then the test items will be presented. Scoring: one point given for each correctly segmented word.
- Phoneme identification. Assesses the capacity of isolating phonemes within a word. The child is asked to tell us whether he or she can hear a sound (the phoneme /r/) within a word. The child is told the isolated phoneme and asked to reproduce it (in some cases the child will not be able to perfectly pronounce the phoneme), then some examples will be given of words that contain the phoneme: arrrrroz, Rrrramón, rrrrío,... After which the task is performed. Scoring: one point is given per word.
- Repetition of pseudowords. This task is very simple. The child simply has to repeat the words. Scoring: one point is given per word repeated correctly.
- Digit repetition. It is a measure of phonological memory. The child has to repeat series of numbers, starting with one number, and if the child repeats it correctly, then two, then three… If the child fails he or she is given another opportunity with the series in the second column. If the child fails in both attempts, the task is halted and the largest number of digits correctly repeated written down. Numbers are presented at a rate of one per second. Scoring: the score will correspond to the largest number of digits repeated correctly.
- Verbal fluidity. The child has to name all the animals he or she can think of in one minute. The number of animals named will be documented. Scoring: points will be given depending on the number of animals named. 0–1: 0 points; 2–3: 1 point; 4–5: 2 points; 6–7: 3 points; 8–9: 4 points; 10 or more: 5 points.
The total score is obtained by adding the partial scores of the six tasks:
- 27 to 30 points: good performance.
- 18 to 27 points: normal.
- 16 to 18 points: mild difficulties.
- Less than 16 points: severe difficulties.