
Vol. 26 - Num. 101
Originales
Melatonina en trastornos del sueño: comparación de distintos productos y revisión bibliográfica
Victoria Domínguez Leóna, Beatriz Flores Méndezb, Cristóbal Coronel Rodríguezb
aMIR-Pediatría. CS Amante Laffón. Sevilla. España .
bPediatra. CS Amante Laffón. Sevilla. España.
Correspondencia: V Domínguez. Correo electrónico: victoriadominguezleon@gmail.com
Cómo citar este artículo: Domínguez León V, Flores Méndez B, Coronel Rodríguez C. Melatonina en trastornos del sueño: comparación de distintos productos y revisión bibliográfica . Rev Pediatr Aten Primaria. 2024;26:23-34. https://doi.org/10.60147/45efa623
Publicado en Internet: 07-02-2024 - Número de visitas: 89651
Resumen
Introducción: los trastornos del sueño en Pediatría son un problema creciente. La melatonina es el producto de elección y es común recibir publicidad de múltiples productos que la contienen. En este texto se lleva a cabo un análisis comparativo de los mismos, examinando la evidencia científica más reciente, con el fin de determinar si está justificado o no su uso.
Métodos: se ha realizado un estudio descriptivo de los productos que contenían melatonina comercializados en España, de venta en farmacias y dirigidos a la población pediátrica. Posteriormente, se ha llevado a cabo una revisión de documentos sobre el uso de melatonina en niños y sobre cada componente extra presente en los productos recogidos.
Resultados: se analizaron 53 productos. La forma de administración mayoritaria fue en gotas o mililitros. La dosis recomendada habitual de melatonina fue de 1 mg al día. El componente añadido más frecuente registrado fue la vitamina B6, y melisa y pasiflora fueron las plantas más utilizadas. Ninguno de los productos estaba catalogado como fármaco por la Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) y tampoco se encontró en la publicidad de ninguno referencias bibliográficas.
Conclusiones: aunque es conocida la eficacia de la melatonina en trastornos del sueño, actualmente no hay un consenso sobre su dosis eficaz en edad pediátrica. Las sustancias que más frecuentemente se asocian a melatonina cuentan con poca bibliografía que respalde sus resultados sobre el sueño, además de que para ellas tampoco existen, de momento, dosis estandarizadas para la población infantil.
Palabras clave
● Melatonina ● Trastornos del sueñoINTRODUCCIÓN
Los trastornos del sueño en Pediatría son una preocupación creciente: se observan hasta en un 25% de los niños y adolescentes sanos1. Pueden tener importantes consecuencias en su desarrollo físico, cognitivo y emocional1,2. Es fundamental abordarlos de manera adecuada para prevenirlas o mitigarlas.
En búsqueda de soluciones terapéuticas, la melatonina ha surgido como producto de elección. Es una hormona producida por la glándula pineal y desempeña un papel fundamental en la regulación de los ritmos circadianos y el sueño, disminuyendo la latencia de este. En Pediatría, la melatonina se ha utilizado para tratar diversos trastornos, como el insomnio, el trastorno del ritmo circadiano y el trastorno del sueño relacionado con el autismo3. Hay evidencia de un efecto positivo en la latencia y el tiempo total de sueño con su consumo, sin que las revisiones proporcionen información sobre si hay mejoría en la calidad de este o del funcionamiento diurno4. Los efectos adversos derivados de su uso suelen no ser graves, pero faltan estudios que lo confirmen. Se baraja, por ejemplo, su relación con la pubertad precoz. Es por esto que, en algunos países, como en los nórdicos, la melatonina se considera un fármaco que necesita receta médica para su consumo2.
En este contexto, es común recibir publicidad de múltiples productos que contienen melatonina en Atención Primaria, los cuales se distinguen por la concentración de la misma, el modo de administración y los ingredientes adicionales añadidos, a menudo atribuyéndoles propiedades específicas. Aunque la utilidad de la melatonina cuenta con respaldo en la bibliografía científica, existe menos evidencia sobre las propiedades de los ingredientes añadidos.
Este texto se propone llevar a cabo un análisis comparativo de los productos principales de melatonina en Pediatría, los ingredientes que incorporan y las dosis que se recomiendan en su ficha técnica, examinando la evidencia científica más reciente, con el fin de determinar si es justificado o no el uso de estos en el tratamiento de los trastornos del sueño en niños.
MÉTODOS
Realizamos un estudio descriptivo de los productos que contienen melatonina comercializados en España y de venta libre en farmacias y comercio electrónico. Se incluyeron formulaciones en gotas, mililitros, espray, sobres o gominolas, aptas según el fabricante para menores de 15 años. De todos ellos se recogió nombre, laboratorio, concentración de melatonina, componentes añadidos, aditivos, alérgenos, dosis recomendada y edad de uso según fabricante. También se analizó si estaban catalogados por la Agencia Española de Medicamentos y Productos Sanitarios (AEMPS).
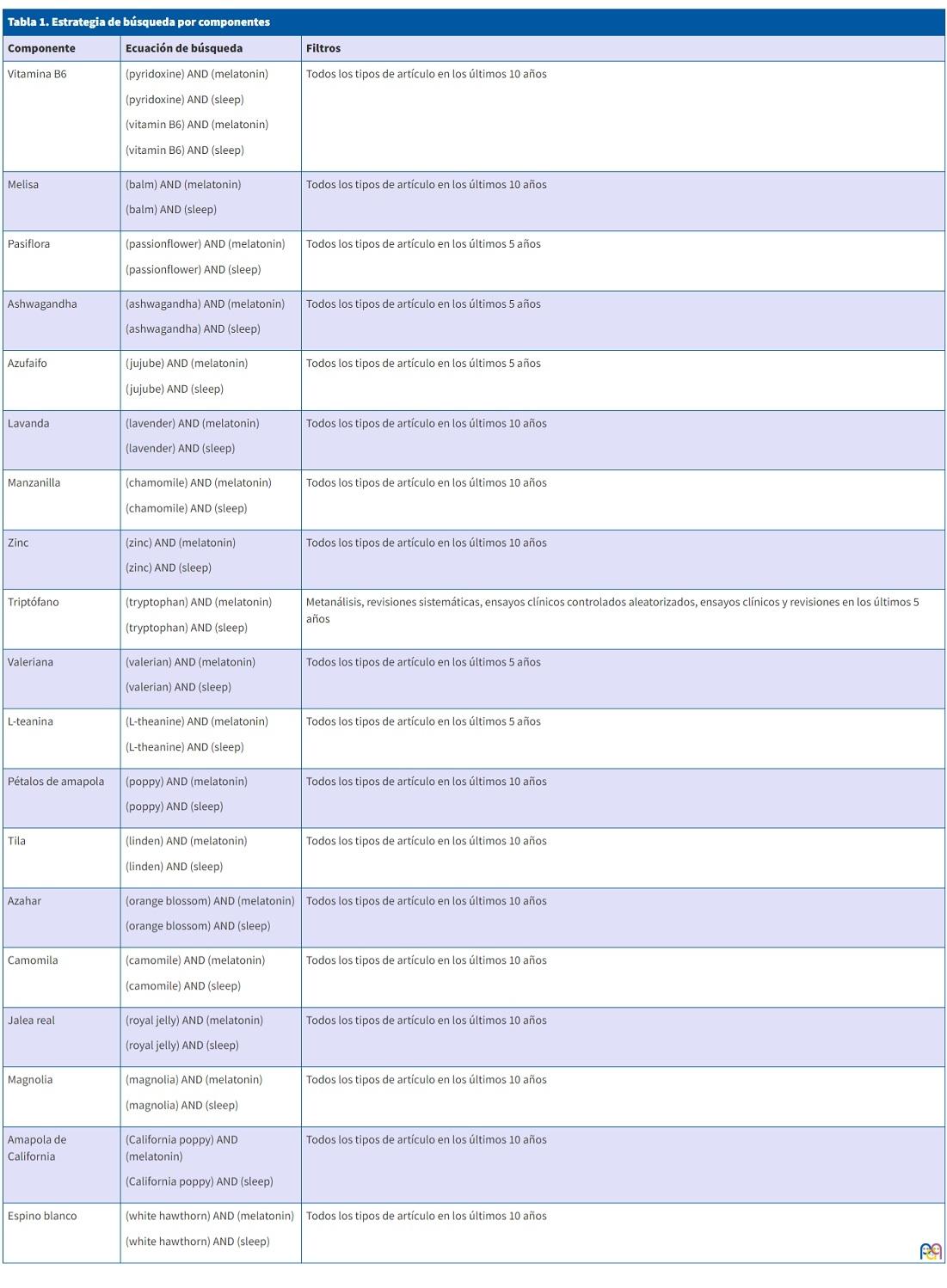
Posteriormente, se llevó a cabo una revisión de las publicaciones en PubMed en el último año, relacionados con la melatonina y su uso en niños sanos. Esta búsqueda se realizó en inglés, con la ecuación: “(melatonin) AND (children)”. Se recogieron metanálisis, revisiones sistemáticas, ensayos clínicos controlados aleatorizados, ensayos clínicos y revisiones. También utilizamos la misma estrategia, pero acotando la investigación a artículos españoles, con la siguiente ecuación: “(melatonina) AND (niños)”. Tuvimos que ampliar la búsqueda a 10 años para conseguir resultados. Además, se consideró la bibliografía aportada por los fabricantes. En segundo lugar, se investigó la bibliografía existente sobre cada componente que fuera diferente a melatonina en los productos recogidos, siendo la estrategia de búsqueda la indicada en la Tabla 1.
| Tabla 1. Estrategia de búsqueda por componentes | ||
|---|---|---|
| Componente | Ecuación de búsqueda | Filtros |
| Vitamina B6 |
(pyridoxine) AND (melatonin) (pyridoxine) AND (sleep) (vitamin B6) AND (melatonin) (vitamin B6) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Melisa |
(balm) AND (melatonin) (balm) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Pasiflora |
(passionflower) AND (melatonin) (passionflower) AND (sleep) |
Todos los tipos de artículo en los últimos 5 años |
| Ashwagandha |
(ashwagandha) AND (melatonin) (ashwagandha) AND (sleep) |
Todos los tipos de artículo en los últimos 5 años |
| Azufaifo |
(jujube) AND (melatonin) (jujube) AND (sleep) |
Todos los tipos de artículo en los últimos 5 años |
| Lavanda |
(lavender) AND (melatonin) (lavender) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Manzanilla |
(chamomile) AND (melatonin) (chamomile) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Zinc |
(zinc) AND (melatonin) (zinc) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Triptófano |
(tryptophan) AND (melatonin) (tryptophan) AND (sleep) |
Metanálisis, revisiones sistemáticas, ensayos clínicos controlados aleatorizados, ensayos clínicos y revisiones en los últimos 5 años |
| Valeriana |
(valerian) AND (melatonin) (valerian) AND (sleep) |
Todos los tipos de artículo en los últimos 5 años |
| L-teanina |
(L-theanine) AND (melatonin) (L-theanine) AND (sleep) |
Todos los tipos de artículo en los últimos 5 años |
| Pétalos de amapola |
(poppy) AND (melatonin) (poppy) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Tila |
(linden) AND (melatonin) (linden) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Azahar |
(orange blossom) AND (melatonin) (orange blossom) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Camomila |
(camomile) AND (melatonin) (camomile) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Jalea real |
(royal jelly) AND (melatonin) (royal jelly) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Magnolia |
(magnolia) AND (melatonin) (magnolia) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Amapola de California |
(California poppy) AND (melatonin) (California poppy) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
| Espino blanco |
(white hawthorn) AND (melatonin) (white hawthorn) AND (sleep) |
Todos los tipos de artículo en los últimos 10 años |
RESULTADOS
Revisión de los productos con melatonina
Se analizaron 37 marcas farmacéuticas diferentes, sumando un total de 53 productos. La forma de administración mayoritaria fue en gotas o mililitros (38,5%) (Tabla 2).
| Tabla 2. Productos con melatonina de venta libre en farmacias | ||||||
|---|---|---|---|---|---|---|
| Producto (farmacéutica)® | Melatonina | Otros componentes | Formato | Modo de administración | Edad de uso | Alérgenos |
| Aquilea sueño Express (Aquilea) | 1 mg/1 puff | No | 12 mL | 1 puff | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Aquilea sueño gotas (Aquilea) | 1 mg/4 gotas | 3,2 mg manzanilla y 2 mg melisa/4 gotas | 20 mL | 4 gotas | No especificado | Sin gluten, sin lactosa |
| Aquilea sueño gummies (Aquilea) | 0,95 mg melatonina + 1 mg melotime/1 gominola | 100 mg melisa, 25 mg pasiflora, 25 mg amapola de California y 1,4 mg de vitamina B6/1 gominola | 30 gominolas | 1 gominola | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Aquilea sueño Instant (Aquilea) | 1,95 mg/1 sobre | 100 mg melisa, 100 mg pasiflora, 50 mg amapola de California/1 sobre | 25 sobres | 1 sobre | No especificado | Sin gluten, sin lactosa |
| Arkosueño melatonin gotas (Arkopharma) | 1 mg/4 gotas | No | 30 mL | 4 gotas | >6 meses | No especificado |
| Buonadiem (Buona) | 1 mg/0,2 mL | No | 20 mL | 4 gotas | No especificado | Sin gluten, sin lactosa |
| Buonadiem 5 tripto (Buona) | 1 mg/0,5 mL | 1,5 mg zinc y 10 mg triptófano/0,5 mL | 30 mL | 0,5 mL | No especificado | Sin gluten, sin lactosa |
| Buonadiem plus (Buona) | 1 mg/1 sobre | 1,4 mg vitamina B6 y 100 mg L-teanina/1 sobre | 20 sobres | 1 sobre | No especificado | Sin gluten, sin lactosa |
| Dormipol (Plantapol) | 1 mg/1 mL | No | 30 mL | 1 mL | No especificado | No especificado |
| Holoextract melatonina sueño (Equisalud) | 1 mg/4 gotas | 2,5 mg pasiflora y 2,5 mg amapola de California/4 gotas | 50 mL | 4 gotas | No especificado | No especificado |
| Jellykids dulces sueños (Eladiet) | 1 mg/10 mL | 150 mg jalea real, 200 mg lavada, 125 mg manzanilla, 500 mg melisa y 125 mg tila/10 mL | 250 mL | 10 mL | >3 años | Sin gluten, sin lactosa |
| Just sleep melatonina gotas (Ceutics) | 0,5 mg/5 gotas | No | 30 mL | 5 gotas | >12 años | No especificado |
| Kurasueño de inicio (Kurasana) | 1 mg/2 puff | No | 60 mL | 2 puff | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Kurasueño de mantenimiento (Kurasana) | 1 mg/3 puff | 1,7 mg vitamina B6 y 25,5 mg triptófano/3 puff | 60 mL | 3 puff | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Lipolife liposomal melatonina (Equisalud) | 1 mg/1 puff | No | 30 ml | 1 puff | No especificado | No especificado |
| Melamil (Humana) | 1 mg/4 gotas | No | 30 mL | 4 gotas | No especificado | Sin gluten |
| Melamil tripto (Humana) | 1 mg/0,5 mL | 1,4 mg vitamina B6 y 29 mg triptófano/0,5 mL | 30 mL | 0,5 mL | >3 años | Sin gluten |
| Melanoctina gotas sublinguales (Plameca) | 1,95 mg/0,5 mL | No | 50 mL | de 0,1 mL a 0,25 mL | >3 años | Sin gluten, sin lactosa |
| Melanoctina spray (Plameca) | 0,95 mg/3 puff | No | 30 mL | de 1 a 3 puff | >3 años | Sin gluten, sin lactosa, sin PLV |
| Melatonin Pura Gotas (ESI) | 1 mg/1 mL | No | 50 mL | 10 gotas o 1 mL | >3 años | Sin gluten, sin lactosa, sin azúcares |
| Melatonin Pura Gotas Hierbas de la noche (ESI) | 1 mg/1 mL | 10,08 mg valeriana, 30 mg manzanilla, 100,2 mg pasiflora, 100,2 mg amapola de California, 16,12 mg tila, 31,4 mg espino blanco/1 mL | 50 mL | 1 mL | No especificado | Sin gluten, sin lactosa |
| Melatonin Pura Gotas Junior (ESI) | 1 mg/1 mL | No | 40 mL | 1 mL | >3 años | Sin gluten, sin lactosa, sin azúcares |
| Melatonin Pura Spray (ESI) | 1 mg/2 puff | No | 20 mL | 1 o 2 pulverizaciones | No especificado | Sin gluten, sin azúcares |
| Melatonin Sleep support gummies (Weider) | 1 mg/1 gominola | 0,7 mg vitamina B6/1 gominola | 60 gominolas | 1 gominola | No especificado | Sin gluten, sin azúcares |
| Melatonina & GO (Pharma & Go) | 1 mg/22 gotas | No | 30 mL | 11 o 22 gotas | No especificado | No especificado |
| Melatonina + Ashwagandha pasiflora y camomila (Sanon) | 1,8 mg/1 stick | 150 mg ashwagandha, 150 mg camomila, 180 mg pasiflora/1 stick | 30 sticks | 1 stick | >12 años | No especificado |
| Melatonina family gotas (Epaplus Sleepcare) | 1 mg/4 gotas | 0,21 mg vitamina B6/4 gotas | 30 mL | 4 gotas | No especificado | No especificado |
| Melatonina spray (Longlife) | 1 mg/1 puff | No | 30 mL | 1 o 2 puff | No especificado | Sin gluten |
| Melatonina flash (Natysal) | 0,98 mg/1 puff | No | 30 mL | 1 puff | >6 años | No especificado |
| Melatonina gotas (Soria Natural) | 1,8 mg/10 gotas | No | 50 mL | 10 gotas o 0,5 mL | >3 años | Sin gluten |
| Melatonina gotas (Soñodina) | 1 mg/3 gotas | 0,21 mg vitamina B6/3 gotas | 20 mL | 3 gotas | >3 años | Sin gluten, sin lactosa |
| Melatonina gotas (Farline) | 1 mg/4 gotas | No | 30 mL | 4 gotas | >3 años | No especificado |
| Melatonina gotas (Zenement) | 1 mg/4 gotas | No | 50 mL | de 4 a 7 gotas | No especificado | Sin gluten, sin lactosa |
| Melatonina líquida Kids (Drasanvi) | 1 mg/10 gotas | 0,67 mg vitamina B6/10 gotas | 50 mL | 10 gotas | No especificado | Sin gluten |
| Melatonova líquida (Nova Diet) | 1 mg/1 mL | No | 30 mL | 1 mL | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Mellatoplus gotas (Lavigor) | 1 mg/3 gotas | No | 30 mL | 3 gotas | No especificado | No especificado |
| Natusleep sueño gominolas (Natusure) | 1 mg/1 gominola | 0,7 mg vitamina B6/1 gominola | 60 gominolas | 1 gominola | >8 años | Sin gluten, sin lactosa |
| Ninamil (FARDI) | 1 mg/1 mL | No | 50 mL | 1 mL | No especificado | Sin gluten, sin lactosa, sin azúcares |
| NS melatonina gotas (CINFA) | 1 mg/4 gotas | No | 30 mL | 4 gotas | >6 meses | Sin gluten, sin lactosa, sin PLV, sin frutos secos |
| Oniria gotas (Italfarmaco) | 1 mg/4 gotas | No | 25 mL | 4 gotas | No especificado | Sin gluten, sin lactosa, sin azúcares |
| Serenesi notte (ESI) | 1 mg/2 mL | 250 mg ashwagandha y 200 mg lavanda/2 mL | 50 mL | 1 o 2 mL | >3 años | Sin gluten, sin azúcares |
| Serenotte gotas (Specchiasol) | 1,9 mg/12 gotas | 55,1 mg amapola de California, 18,2 mg pétalos de amapola y 15,2 mg L-teanina/12 gotas | 50 mL | 12 gotas | >3 años | Sin gluten |
| Seripnol gotas (Neuraxpharm) | 1 mg/10 gotas | 5 mg magnolia, 2 mg azufaifo y 30 mg L-teanina/10 gotas | 30 mL | 10 gotas | No especificado | Sin gluten |
| Sleep vitamins (Chic & love) | 1 mg/1 gominola | 0,7 mg vitamina B6/1 gominola | 60 gominolas | 1 gominola | No especificado | Sin gluten, sin azúcares |
| Sleep well liquid (Zentrity by naturitas) | 1 mg/4 gotas | 3,2 mg manzanilla, 2 mg melisa y 2 mg pasiflora/4 gotas | 50 mL | 4 gotas | No especificado | Sin gluten, sin lactosa |
| Sleepeel gotas (Heel) | 1 mg/0,5 mL | 40 mg melisa, 100 mg pasiflora, 1,2 mg vitamina B6 y 1,5 mg triptófano/0,5 mL | 30 mL | 0,5 mL | >3 años | Sin gluten, sin lactosa |
| Sleepeel noche (Heel) | 1 mg/1 gominola | 40 mg melisa, 100 mg pasiflora y 1,4 mg vitamina B6/1 gominola | 60 gominolas | 1 gominola | >3 años | Sin gluten, sin lactosa |
| Sleepeel spray (Heel) | 1 mg/3 puff | 40 mg melisa, 100 mg pasiflora y 1,2 mg vitamina B6/2 puff | 20 mL | 3 puff | >3 años | Sin gluten, sin lactosa, sin azúcares |
| Somnolem melatonina spray (Waydiet) | 1 mg/3 puff | 289,8 mg azahar, 6 mg melisa, 0,73 mg vitamina B1, 0, 93 mg vitamina B6 y 3 mcg vitamina B8/3 puff | 20 mL | 3 puff | >12 años | Sin gluten |
| Soñadores gotas (Ordesa) | 1 mg/0,5 mL | 1,4 mg vitamina B6 y 20 mg triptófano/0,5 mL | 30 mL | 0,5 mL | >3 años | Sin gluten, sin lactosa, sin PLV |
| Soñadores spray (Ordesa) | 1 mg/1 puff | No | 15 mL | 1 puff | >3 años | No especificado |
| Sweet sleep gummies (Jelly Pills) | 1 mg/2 gominolas | 25 mg manzanilla y 0,7 mg vitamina B6/2 gominolas | 60 gominolas | 2 gominolas | No especificado | Sin gluten, sin lactosa |
| ZzzQuil NATURA (Vicks) | 1 mg/1 gominola | 30 mg valeriana, 10 mg camomila, 10 mg lavanda y 1,4 mg vitamina B6/1 gominola | 30 o 60 gominolas | 1 gominola | No especificado | No especificado |
|
PLV: proteínas de leche de vaca. |
||||||
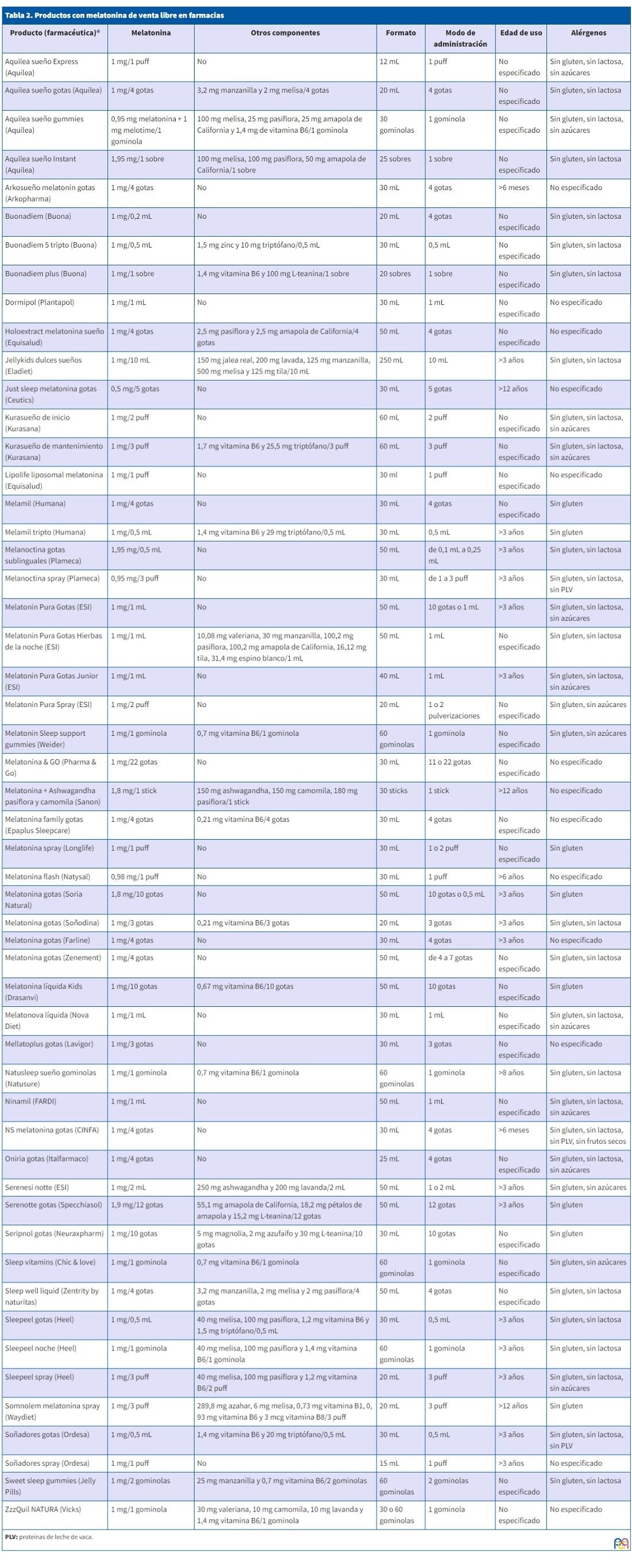
En cuanto a la dosis recomendada habitual de melatonina, fue de 1 mg al día, excepto en un 9,4% de los productos que recomendaban dosis de hasta 1,95 mg de melatonina diaria. Un 47% de los artículos solo contenían melatonina en su composición. El componente adicional más frecuente registrado, hasta en un 32% de los productos, fue la vitamina B6, con un rango de dosis de 0,21 a 1,7 mg al día (dosis mayoritaria de 1,4 mg diarios). Melisa y pasiflora fueron las plantas más utilizadas, en un 16,9% de los productos, con dosis entre 2 y 500 mg diarios (40 mg la más frecuente) y entre 2,5 y 180 mg diarios (100 mg lo más frecuente), respectivamente. El azahar, la jalea real, la magnolia, el azufaifo, el espino blanco y los pétalos de amapola solo se recogieron en un único producto cada uno. La combinación más frecuente fue de melisa con pasiflora, seguida de pasiflora con amapola de California, de vitamina B6 con triptófano y de manzanilla con melisa.
Sobre los aditivos, encontramos el ácido cítrico como acidulante, el benzoato de sodio y el sorbato de potasio como conservantes, el monooleato de sorbitán polioxietilenado y la lecitina de soja como emulsionantes, la goma xantana como espesante, el glicerol como estabilizante y el sorbitol o manitol o la sucralosa como edulcorantes. Solo en un producto se recogió la presencia de aceite de palma y en otro de ellos, dióxido de silicio.
Revisión de la bibliografía
Tras la búsqueda inicial, se localizaron 5 artículos que hablan de melatonina en la infancia; 2 de ellos se excluyeron por ocuparse del uso de melatonina en niños no sanos (trastorno del espectro autista y trastorno por déficit de atención con hiperactividad). Nos quedamos, por tanto, con 3 artículos. Tras la búsqueda de artículos en español se obtuvieron 3; uno de ellos fue excluido por tratar del sueño en niños con patología y el otro por tratarse de una versión más antigua del consenso de sueño con el que finalmente trabajamos.
En la búsqueda específica por componentes se encontraron 3 artículos para vitamina B6, 2 para melisa, 2 para pasiflora, 7 para ashwagandha, 5 para azufaifo, 2 para lavanda, 1 para manzanilla, 2 para zinc, 4 para triptófano, 4 para valeriana, y 4 para l-teanina. Para pétalos de amapola, tila, azahar, camomila, jalea real, magnolia, amapola de California y espino blanco no se encontraron estudios sobre su mecanismo de acción o su relación con el sueño.
Ninguno de los productos estaba recogido específicamente en la AEMPS. Solo un fabricante recogía bibliografía sobre su producto, 2 ensayos clínicos de su uso como inductor del sueño en niños para procesos diagnósticos no invasivos y 1 ensayo clínico en niños con cefalea crónica. Estos artículos no se incluyeron en el análisis de la discusión, ya que no cumplían el objetivo de esta revisión.
DISCUSIÓN
Dosis de melatonina recomendada
Actualmente no hay un consenso establecido sobre la dosis de melatonina eficaz en edad pediátrica. En las principales revisiones se recomienda su inicio en lactantes y preescolares con 1-3 mg diarios y en niños mayores, con 2,5-5 mg diarios, aumentando gradualmente según respuesta3,4. Se especifica que el tratamiento no debe superar de manera continuada las 4 semanas. Cabe destacar que se estima una recaída al retirar la melatonina en el 90% de casos de insomnio de inicio tratado únicamente con esta sustancia3. Todos coinciden en que debe ser administrado siempre a la misma hora, entre 20-60 minutos antes de irse a dormir3,4.
En comparación, en los productos revisados, la dosis recomendada inicial fue de 1 mg al día, salvo en 5 de ellos, que recomendaban iniciar con 1,95 mg diarios. Dosis que, según la evidencia descrita previamente, podría no ser suficiente según las características del paciente. Ninguno hace distinciones de dosis según rango de edad ni recomienda aumentarla si el efecto no es el deseado.
Componentes adicionales
Vitamina B6
16 de los 53 productos revisados (30,2%) contenían, entre otros componentes, vitamina B6, siendo el más frecuentemente usado diferente a la melatonina. Aunque se le atribuye un impacto positivo en el sueño en algunos casos5-7, la investigación es limitada y suele estudiarse su efecto junto con el de otros componentes. Además, su relación con el insomnio no es tan clara como ocurre con el magnesio, que tiene un papel más establecido en la regulación del sueño. No hay consenso en la dosis eficaz, pero sí está claro que la dosis máxima segura es de 100 mg/día para evitar efectos secundarios como neuropatía sensorial, fotosensibilidad, problemas gastrointestinales…5. La mayoría de ellos recomendaban 1,4 mg diarios.
Melisa y Pasiflora
Un 16,9% de los productos revisados contenían Melissa officinalis y Pasiflora incarnata, 40 mg y 100 mg diarios de cada planta fue lo más recomendado. Son las plantas más utilizadas en los productos revisados. Hay evidencia de que sus propiedades pueden influir positivamente en el sueño y el insomnio8-11. Algunos datos disponibles atribuyen a la melisa propiedades antibacterianas, neuroprotectoras y antiinflamatorias, además de propiedades sedantes o relajantes, que apoyan su utilidad en el insomnio y situaciones de estrés9,10. No hay datos sobre la dosis eficaz que se debe administrar para cada efecto. La pasiflora a su vez tiene efecto ansiolítico, sedante y ayuda a la regulación del sueño, aumentando la actividad de las neuronas GABAérgicas y la melatonina en sangre10,11. Sin embargo, tampoco hay evidencias de la dosis eficaz que debemos administrar para obtener estos beneficios.
Ashwagandha
La Withania somnifera es una planta medicinal tradicional de India que se ha usado durante siglos para tratar el insomnio. Se ha estudiado por presentar una variedad de actividades biológicas como neuroprotector, propiedades antimicrobianas, antidiabéticas, antiinflamatorias, adaptogénicas, para reducir la ansiedad y como un compuesto natural con potencial para inducir, mejorar la calidad y la latencia de inicio del sueño en pacientes con insomnio12-18. Se cree que actúa a través de los receptores GABA16,17. Es un compuesto bien tolerado. No está clara la dosis eficaz; hay estudios en los que se utilizan 300 mg de extracto dos veces al día y otros en los que la dosis depende del peso (10-50 mg/kg diarios)13-15.
Dos de los 53 productos analizados contenían esta sustancia. La dosis que recomiendan es de 150 mg y 250 mg diarios. Esta dosis, teniendo en cuenta que hablamos de pacientes pediátricos y pesan menos que los adultos, podrían ser acordes a la evidencia descrita.
Azufaifo
El Ziziphus jujuba es una fruta que se cultiva en diversas partes del mundo y se ha utilizado en la medicina tradicional por sus posibles beneficios para el sueño y la relajación. Aunque no es un inductor del sueño como tal, se le atribuyen propiedades que pueden contribuir a mejorar la calidad de este en personas con trastornos del sueño, influyendo sobre todo en su latencia19-23. Hay datos que sugieren que su mecanismo de acción principal es la estimulación de los receptores GABA22,23, aunque en la actualidad se necesitan más estudios para poder confirmarlo. La mayoría de las veces se utiliza en combinación con otras hierbas. No se encontró evidencia en ninguno de los artículos revisados sobre la dosis recomendada.
Solo uno de los productos revisados en este estudio contenía azufaifo, con 2 mg diarios como dosis recomendada.
Lavanda
Es una planta principalmente conocida por su aroma, pero también se ha demostrado su impacto positivo en el sueño por sus propiedades sedantes e hipnóticas. Sus ingredientes activos y mecanismos para mejorar el sueño aún no están claros, aunque hay estudios que la relacionan con los sistemas GABAérgico, colinérgico, histaminérgico, las monoaminas en el sistema límbico24 y el serotoninérgico25. Ninguno de los artículos revisados especifica dosis recomendadas de esta sustancia.
Dos de los productos revisados en este estudio contenían lavanda entre sus componentes. La dosis recomendada fue de 10 mg y 200 mg en cada uno de ellos.
Manzanilla
La Matricaria chamomilla es una hierba que se ha utilizado tradicionalmente por sus propiedades relajantes y su potencial para promover un sueño tranquilo. Aunque las investigaciones sobre su efecto son limitadas, algunos estudios sugieren que puede tener efectos positivos sobre el sueño y menos efectos secundarios que los fármacos convencionales26.
Cinco de los productos revisados contenían manzanilla entre sus componentes. La dosis recomendada es muy variable: desde 3,2 a 125 mg diarios. No se han encontrado estudios que especifiquen la dosis efectiva recomendada.
Zinc
La relación entre las concentraciones de este mineral esencial en sangre y la calidad del sueño es un tema de creciente interés. Hay datos que sugieren un papel potencial en la optimización de la calidad del sueño27,28, en especial en los adolescentes27. Sin embargo, la evidencia es aún muy escasa y se necesitan más estudios para comprender adecuadamente las funciones del mismo en la transmisión glutamatérgica y otros tipos de neurotransmisores relacionadas con este proceso28. No hemos encontrado en la bibliografía revisada dosis efectiva recomendada.
En nuestro estudio solo uno de los productos analizados contiene zinc, con una dosis recomendada de 1,5 mg diarios.
Triptófano
Es un aminoácido esencial que desempeña un papel importante en la síntesis de proteínas y la producción de neurotransmisores en el cerebro, como es la serotonina, a partir de la cual se sintetiza la melatonina29-32. Se han identificado mejoras en los parámetros del sueño después del consumo de triptófano; entre ellas destaca un mayor tiempo y eficiencia del mismo, una disminución de su latencia, una mejoría en los despertares nocturnos y también disminución de las parasomnias29,31,32. Se necesitan más estudios a largo plazo sobre dietas específicas enriquecidas en triptófano y el sueño29. Cabe destacar que las fuentes de alimentos ricos en glucosa también pueden tener una influencia positiva en el sueño, ya que la glucosa favorece el paso del triptófano a través de la barrera hematoencefálica30. El rango de dosis utilizado en estudios sobre este aminoácido en edad pediátrica con trastornos de parasomnia fue de 500 a 4500 mg diaria (dosis media de 2400 mg diarios)32.
Únicamente el 9,4% de los productos de este estudio incluían triptófano entre sus componentes. La dosis diaria recomendada en tres de ellos es algo más homogénea en un rango entre 20-30 mg diarios; en los otros dos la dosis es de 10 mg y 1,5 mg, todas ellas mucho menores que las descritas en los artículos revisados.
Valeriana
Es una planta medicinal que se ha utilizado tradicionalmente para tratar trastornos del sueño, como el insomnio, y estados de ansiedad33-36.
Algunos estudios sugieren que la valeriana puede ser útil, por sus propiedades sedantes y ansiolíticas, para mejorar la calidad subjetiva del sueño y reducir la dificultad para conciliarlo33,35,36, aunque requiere una administración repetida para obtener efectos significativos33. Las dosis en los principales estudios oscilan entre 160 y 600 mg al día, aunque no se especifica dosis mínima eficaz36. Se desconoce el mecanismo de acción preciso de esta hierba, aunque se cree que ocurre a través de la acción sobre el neurotransmisor GABA por la inhibición de la actividad simpática35. En determinados estudios, no se encuentran beneficios significativos en comparación con placebo35,36. La falta de consistencia en los resultados puede deberse a diferencias en la calidad de los estudios, las dosis utilizadas y las formas de administración de la valeriana. A pesar de las diferencias comentadas, la mayoría de la bibliografía revisada coincide en la seguridad de esta sustancia y la escasez de efectos secundarios33,35.
Dentro de la composición de los productos revisados solo dos la incluían. La dosis diaria recomendada fue 10,08 mg en uno de ellos y 30 mg en el otro, muy inferior a la utilizada en los principales estudios.
l-teanina
Es un aminoácido no proteico que se encuentra principalmente en las hojas del té verde. Se ha estudiado por sus posibles efectos en la relajación y la reducción del estrés, y algunos estudios sugieren que puede tener un impacto positivo en la calidad del sueño37-40. Se cree que estimula la producción de ondas alfa en el cerebro, que están asociadas con un estado de relajación, sin somnolencia posterior ni alteración de las funciones motoras39,40. Además, puede aumentar la producción de dopamina y serotonina, al mejorar los niveles de GABA, que están involucrados en el control del estado de ánimo y el sueño40. Se cree que puede mejorar de manera segura y efectiva la calidad del sueño en niños con trastorno por déficit de atención e hiperactividad (TDAH)35,40. La dosis utilizada en la bibliografía revisada fue en niños de 8 y 12 años con TDAH de 400 mg diarios40 y en adultos sanos de 200 mg al día39; dosis altas son generalmente bien toleradas (hasta 4000 mg/kg/día)39 y con pocos efectos adversos asociados38.
Solo tres productos dentro del total contenían l-teanina. Las dosis recomendadas diarias fueron de 100 mg, 30 mg y 15,2 mg en cada uno de ellos, dosis muy dispar si los comparamos entre sí y menor a la utilizada en los principales estudios.
Para finalizar, destacamos que la recogida de estos datos ha sido dificultosa por no encontrarse muchas veces bien especificada o iconografiada la composición de los productos. Pensamos que esto puede deberse a que se consideran complementos alimenticios y no están sometidos a los controles que se les exige a los fármacos como sucede en otros países2.
CONCLUSIÓN
Aunque es de sobra conocida la eficacia de la melatonina en trastornos del sueño y ha sido ampliamente estudiado este efecto, actualmente no hay un consenso establecido sobre su dosis eficaz en edad pediátrica.
Además, en los últimos años han surgido combinaciones de melatonina con otros tipos de sustancias, como la melisa y la pasiflora, las más usadas según nuestra revisión. Sin embargo, hay más bibliografía que respalde el uso de otras sustancias mucho menos utilizadas como la ashwagandha, la valeriana, la l-teanina y el azufaifo. Además, muy pocas dosis están estandarizadas, ya que faltan estudios, no solo en población pediátrica, sino también en adultos; y cuando hay alguna dosis establecida como eficaz, esta, al estar generalmente estudiada en adultos, suele ser utilizada en menor cuantía para la edad infantil (salvo en el caso de la ashwagandha, en la que sí se corresponden las dosis revisadas con las usadas).
Con los resultados obtenidos en este trabajo podemos afirmar que la melatonina es un producto eficaz con amplio respaldo para su uso en trastornos del sueño; sin embargo, tampoco está exenta de efetos secundarios y por esto creemos que debe ser considerada un fármaco, siendo prescrito por los profesionales pertinentes cumpliendo una pauta y condiciones de uso. Sobre los excipientes que acompañan a la melatonina en estos productos, dada la escasez de revisiones sobre ellos en Pediatría y la gran heterogeneidad en los estudios sobre tipo de compuesto y dosis, podemos concluir que falta evidencia para respaldar su uso.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del manuscrito publicado.
ABREVIATURAS
AEMPS: Agencia Española de Medicamentos y Productos Sanitarios · TDAH: trastorno por déficit de atención e hiperactividad.
BIBLIOGRAFÍA
- Edemann-Callesen H, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. Use of melatonin in children and adolescents with idiopathic chronic insomnia: a systematic review, meta-analysis, and clinical recommendation. EClinicalMedicine. 2023;61:102048. http://dx.doi.org/10.1016/j.eclinm.2023.102048
- Händel MN, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. The short-term and long-term adverse effects of melatonin treatment in children and adolescents: a systematic review and GRADE assessment. EClinicalMedicine. 2023;61:102083. http://dx.doi.org/10.1016/j.eclinm.2023.102083
- Pin Arboledas G, Soto Insuga V, Jurado Luque MJ, Fernandez Gomariz C, Hidalgo Vicario I, Lluch Rosello A, et al. Insomnio en niños y adolescentes. Documento de consenso. An Pediatr (Barc). 2017;86(3):165.e1-165.e11.
- Edemann-Callesen H, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. Use of melatonin for children and adolescents with chronic insomnia attributable to disorders beyond indication: a systematic review, meta-analysis and clinical recommendation. EClinicalMedicine. 2023;61:102049. http://dx.doi.org/10.1016/j.eclinm.2023.102049
- García-García C, Baik I. Effects of poly-gamma-glutamic acid and vitamin B6 supplements on sleep status: a randomized intervention study. Nutr Res Pract. 2021;15(3):309. http://dx.doi.org/10.4162/nrp.2021.15.3.309
- Lemoine P, Bablon J-C, Da Silva C. A combination of melatonin, vitamin B6 and medicinal plants in the treatment of mild-to-moderate insomnia: A prospective pilot study. Complement Ther Med. 2019;45:104–8. http://dx.doi.org/10.1016/j.ctim.2019.05.024
- Djokic G, Vojvodic P, Korcok D, Agic A, Rankovic A, Djordjevic V, et al. The effects of magnesium – melatonin - Vit B complex supplementation in treatment of insomnia. Open Access Maced J Med Sci. 2019;7(18):3101-5. http://dx.doi.org/10.3889/oamjms.2019.771
- Zam W, Quispe C, Sharifi-Rad J, López MD, Schoebitz M, Martorell M, et al. An updated review on the properties of Melissa officinalis l.: Not exclusively anti-anxiety. Front Biosci (Schol Ed). 2022;14(2):16. http://dx.doi.org/10.31083/j.fbs1402016
- Roe AL, Venkataraman A. The safety and efficacy of botanicals with nootropic effects. Curr Neuropharmacol. 2021;19(9):1442-67.
- Kim G-H, Yi SS. Chronic oral administration of Passiflora incarnata extract has no abnormal effects on metabolic and behavioral parameters in mice, except to induce sleep. Lab Anim Res. 2019;35(1). http://dx.doi.org/10.1186/s42826-019-0034-9
- Kim G-H, Kim Y, Yoon S, Kim S-J, Yi SS. Sleep-inducing effect of Passiflora incarnata l. extract by single and repeated oral administration in rodent animals. Food Sci Nutr. 2020;8(1):557-66. http://dx.doi.org/10.1002/fsn3.1341
- Langade D, Kanchi S, Salve J, Debnath K, Ambegaokar D. Efficacy and safety of ashwagandha (Withania somnifera) root extract in insomnia and anxiety: A double-blind, randomized, placebo-controlled study. Cureus. 2019;11(9).
- Murthy SV, Fathima SN, Mote R. Hydroalcoholic extract of ashwagandha improves sleep by modulating GABA/histamine receptors and EEG slow-wave pattern in in vitro - in vivo experimental models. Prev Nutr Food Sci. 2022;27(1):108-20. http://dx.doi.org/10.3746/pnf.2022.27.1.108
- Park CW, Hong K-B, Suh HJ, Ahn Y. Sleep-promoting activity of amylase-treated Ashwagandha (Withania somnifera l. Dunal) root extract via GABA receptors. J Food Drug Anal. 2023;31(2):27-28. http://dx.doi.org/10.38212/2224-6614.3456
- Cheah KL, Norhayati MN, Husniati Yaacob l, Abdul Rahman R. Effect of Ashwagandha (Withania somnifera) extract on sleep: A systematic review and meta-analysis. PLoS One. 2021;16(9):e0257843. http://dx.doi.org/10.1371/journal.pone.0257843
- Mikulska P, Malinowska M, Ignacyk M, Szustowski P, Nowak J, Pesta K, et al. Ashwagandha (Withania somnifera) - current research on the health-promoting activities: A narrative review. Pharmaceutics. 2023;15(4):1057.
- Charu B, Atul U, Umesh S. Efficacy of Brimhana Nasya and Ashwagandha (Withania somnifera (l.) Dunal) root powder in primary insomnia in elderly male: A randomized open-label clinical study. Ayu. 2020;41(3):159. https://doi.org/10.4103/ayu.AYU_177_19
- Kelgane SB, Salve J, Sampara P, Debnath K. Efficacy and tolerability of ashwagandha root extract in the elderly for improvement of general well-being and sleep: A prospective, randomized, double-blind, placebo-controlled study. Cureus. 2020; http://dx.doi.org/10.7759/cureus.7083
- Deng Q, Huang l, Yu F, Lin J, Hu l, Zhao J, et al. Biomedical analytics of four Chinese medicinals in treatment of insomnia based on network pharmacology. Biomed Res Int. 2022;2022:1-11.
- Shergis JL, Hyde A, Meaklim H, Varma P, Da Costa C, Jackson ML. Medicinal seeds Ziziphus spinosa for insomnia: A randomized, placebo-controlled, cross-over, feasibility clinical trial. Complement Ther Med. 2021;57:102657. http://dx.doi.org/10.1016/j.ctim.2020.102657
- Luo H, Sun S-J, Wang Y, Wang Y-l. Revealing the sedative-hypnotic effect of the extracts of herb pair Semen Ziziphi spinosae and Radix Polygalae and related mechanisms through experiments and metabolomics approach. BMC Complement Med Ther. 2020;20(1). http://dx.doi.org/10.1186/s12906-020-03000-8
- Bae GY, Ahn Y, Hong K-B, Jung E-J, Suh HJ, Jo K. Sleep-Enhancing Effect of Water Extract from Jujube (Zizyphus jujuba Mill.) Seeds Fermented by Lactobacillus brevis L32. Foods. 2023;12(15):2864.
- Eom S, Lee S, Lee J, Sohn S-O, Lee JH, Park J. A combination of Rosa multiflora and Zizyphus jujuba enhance sleep quality in anesthesia-induced mice. Int J Mol Sci. 2022;23(22):14177.
- Xu Y, Ma l, Liu F, Yao l, Wang W, Yang S, et al. Lavender essential oil fractions alleviate sleep disorders induced by the combination of anxiety and caffeine in mice. J Ethnopharmacol. 2023;302:115868.
- Bruni O, Ferini-Strambi l, Giacomoni E, Pellegrino P. Herbal remedies and their possible effect on the GABAergic system and sleep. Nutrients. 2021;13(2):530.
- Abdullahzadeh M, Matourypour P, Naji SA. Investigation effect of oral chamomilla on sleep quality in elderly people in Isfahan: A randomized control trial. J Educ Health Promot. 2017.
- Ji X, Liu J. Associations between blood zinc concentrations and sleep quality in childhood: A cohort study. Nutrients. 2015;7(7):5684–96.
- Cherasse Y, Urade Y. Dietary zinc acts as a sleep modulator. Int J Mol Sci. 2017;18(11):2334.
- Binks H, E. Vincent G, Gupta C, Irwin C, Khalesi S. Effects of diet on sleep: A narrative review. 2020;12(4):936. http://dx.doi.org/10.3390/nu12040936
- Pereira N, Naufel MF, Ribeiro EB, Tufik S, Hachul H. Influence of dietary sources of melatonin on sleep quality: A review. J Food Sci. 2020;85(1):5–13. http://dx.doi.org/10.1111/1750-3841.14952
- Saidi O, Rochette E, Doré É, Maso F, Raoux J, Andrieux F, et al. Randomized double-blind controlled trial on the effect of proteins with different tryptophan/large neutral amino acid ratios on sleep in adolescents: The PROTMORPHEUS study. Nutrients. 2020;12(6):1885. http://dx.doi.org/10.3390/nu12061885
- Innocenti A, Lentini G, Rapacchietta S, Cinnirella P, Elia M, Ferri R, et al. The role of supplements and over-the-counter products to improve sleep in children: A systematic review. Int J Mol Sci. 2023;24(9):7821. http://dx.doi.org/10.3390/ijms24097821
- Shinjyo N, Waddell G, Green J. Valerian root in treating sleep problems and associated disorders - A systematic review and meta-analysis. J Evid Based Integr Med. 2020;25:2515690X2096732. http://dx.doi.org/10.1177/2515690x20967323
- Zhao F-Y, Xu P, Kennedy GA, Conduit R, Zhang W-J, Wang Y-M, et al. Identifying complementary and alternative medicine recommendations for insomnia treatment and care: a systematic review and critical assessment of comprehensive clinical practice guidelines. Front Public HealtH. 2023;11. http://dx.doi.org/10.3389/fpubh.2023.1157419
- Borrás S, Martínez-Solís I, Ríos JL. Medicinal plants for insomnia related to anxiety: An updated review. Planta Med. 2021;87(10/11):738-53. http://dx.doi.org/10.1055/a-1510-9826
- Guadagna S, Barattini DF, Rosu S, Ferini-Strambi l. Plant extracts for sleep disturbances: A systematic review. Evid Based Complement Alternat Med. 2020;2020:1-9. http://dx.doi.org/10.1155/2020/3792390
- Deshpande SN, Simkin DR. Complementary and integrative approaches to sleep disorders in children. Child Adolesc Psychiatr Clin N Am. 2023;32(2):243-72.
- Zhang Y, Jia X, Chen X, Liu Y, Zhao Z, Hao J, et al. l-theanine and Neumentix mixture improves sleep quality and modulates brain neurotransmitter levels in mice. Ann Palliat Med. 2021;10(4):4572–81. http://dx.doi.org/10.21037/apm-21-663
- Thiagarajah K, Chee HP, Sit NW. Effect of alpha-S1-casein tryptic hydrolysate and l-theanine on poor sleep quality: A double blind, randomized placebo-controlled crossover trial. Nutrients. 2022;14(3):652. http://dx.doi.org/10.3390/nu14030652
- Dasdelen MF, Er S, Kaplan B, Celik S, Beker MC, Orhan C, et al. A novel Theanine complex, Mg-l-Theanine improves sleep quality via regulating brain electrochemical activity. Front Nutr. 2022;9. http://dx.doi.org/10.3389/fnut.2022.874254