

Vol. 26 - Num. 101
Original Papers
Melatonin in sleep disorders. Comparison of different products and literature review
Victoria Domínguez Leóna, Beatriz Flores Méndezb, Cristóbal Coronel Rodríguezb
aMIR-Pediatría. CS Amante Laffón. Sevilla. España .
bPediatra. CS Amante Laffón. Sevilla. España.
Correspondence: V Domínguez. E-mail: victoriadominguezleon@gmail.com
Reference of this article: Domínguez León V, Flores Méndez B, Coronel Rodríguez C. Melatonin in sleep disorders. Comparison of different products and literature review . Rev Pediatr Aten Primaria. 2024;26:23-34. https://doi.org/10.60147/45efa623
Published in Internet: 07-02-2024 - Visits: 4822
Abstract
Introduction: sleep disorders are a growing problem in paediatrics. Melatonin is the drug of choice and it is common to receive advertising for multiple products containing melatonin in primary care. In this paper, a comparative analysis of these products is carried out, examining the most recent scientific evidence, in order to determine whether their use is justified or not.
Methods: we conducted a descriptive study on melatonin-containing products sold in pharmacies in Spain and aimed at the paediatric population. Subsequently, we performed a systematic review of documents on the use of melatonin in children and on each extra component present in the collected products.
Results: the analysis included 53 products. The most common dosage was in drops or millilitres. The usual recommended dose of melatonin was 1 mg per day. The most frequently reported added component was vitamin B6, and lemon balm and passionflower were the most frequently used herbs. None of the products were specifically listed in the Spanish Agency for Medicines and Health Products, and no bibliographical references were provided in the advertising of any of the products.
Conclusions: although the efficacy of melatonin in sleep disorders is well known, there is currently no consensus on its effective dose in children. There is little evidence on the substances most frequently combined with melatonin to support their results in sleep, and there are no standardised doses for them or lower doses are used due to a lack of studies in the paediatric population.
Keywords
● Melatonin ● Sleep disordersINTRODUCTION
Sleep disorders in the paediatric population are a growing concern: they are detected in up to 25% of healthy children and adolescents.1 These disorders may have an important impact on their physical, cognitive and emotional development. 1,2 They must be managed adequately to prevent or mitigate this impact.
In the search for possible treatments, melatonin has emerged as the drug of choice. It is a hormone produced by the pineal gland and plays an essential role in the regulation of circadian rhythms and sleep, reducing sleep onset latency. In paediatric care, melatonin has been used to treat various disorders, such as insomnia, circadian rhythm disorders and sleep problems associated with autism.3 There is evidence of a positive effect on onset latency and total sleep duration with its use, but reviews offer no data on whether it can improve sleep quality or daytime functioning.4 The adverse events of melatonin tend to be mild, but there are no studies confirming it. For instance, there are concerns regarding a potential association with early puberty. For this reason, some countries, for instance the Nordic countries, melatonin is a drug that requires prescription for its use.2
In this context, it is not unusual to receive advertisements for multiple melatonin-containing products in primary care, which differ from each other in the concentration of melatonin, the route of administration and the additional ingredients in the formulation, to which specific properties are often attributed. Although the usefulness of melatonin is supported by scientific evidence, there are fewer data on the properties of the added ingredients.
The purpose of this article is to present a comparative analysis of the main melatonin products for the paediatric population, their ingredients and the doses recommended in their label/product data sheets, in addition to a review of the most recent scientific evidence to determine whether the use of these products is justified in the management of sleep disorders in children.
METHODS
We conducted a descriptive study of the products containing the largest amounts of melatonin commercially available in Spain and sold over the counter in pharmacies and online. The review included dosage forms administered in drops, millilitres, sprays, powder packets or gummies that were appropriate for use in children aged less than 15 years per the manufacturer. For each of these products, we recorded the name, manufacturing laboratory, concentration of melatonin, additional components, additives, allergens and the recommended dose and age range for use according to the manufacturer. We also checked whether the product was catalogued by the Agencia Española de Medicamentos y Productos Sanitarios (AEMPS, Spanish Agency of Medicines and Medical Devices).
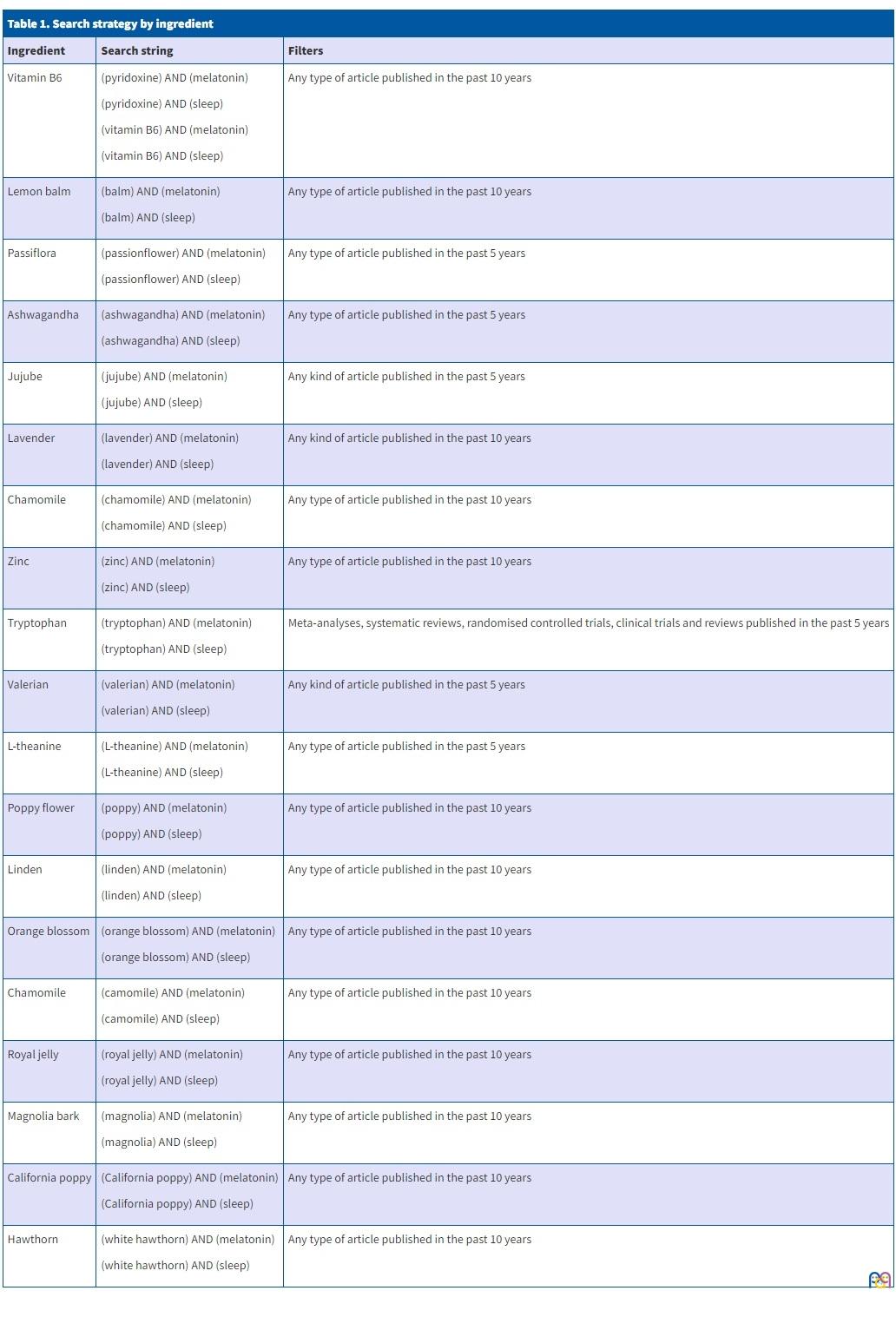
Subsequently, we performed a review of publications in PubMed in the past year regarding melatonin and its use in healthy children. We performed the search using English terms, with the search string “(melatonin) AND (children)”. We selected articles corresponding to meta-analyses, systematic reviews, randomised controlled trials, clinical trains and reviews. We also applied the same search strategy, this time limiting the search to Spanish articles, with the search string “(melatonina) AND (niños)”. In this search, we had to expand the time range to the last 10 years to obtain results. We also analysed the documentation provided by manufacturers. In addition, we searched the literature on any active ingredients other than melatonin contained in these products, using the search strategies outlined in Table 1.
| Table 1. Search strategy by ingredient | ||
|---|---|---|
| Ingredient | Search string | Filters |
| Vitamin B6 |
(pyridoxine) AND (melatonin) (pyridoxine) AND (sleep) (vitamin B6) AND (melatonin) (vitamin B6) AND (sleep) |
Any type of article published in the past 10 years |
| Lemon balm |
(balm) AND (melatonin) (balm) AND (sleep) |
Any type of article published in the past 10 years |
| Passiflora |
(passionflower) AND (melatonin) (passionflower) AND (sleep) |
Any type of article published in the past 5 years |
| Ashwagandha |
(ashwagandha) AND (melatonin) (ashwagandha) AND (sleep) |
Any type of article published in the past 5 years |
| Jujube |
(jujube) AND (melatonin) (jujube) AND (sleep) |
Any kind of article published in the past 5 years |
| Lavender |
(lavender) AND (melatonin) (lavender) AND (sleep) |
Any kind of article published in the past 10 years |
| Chamomile |
(chamomile) AND (melatonin) (chamomile) AND (sleep) |
Any type of article published in the past 10 years |
| Zinc |
(zinc) AND (melatonin) (zinc) AND (sleep) |
Any type of article published in the past 10 years |
| Tryptophan |
(tryptophan) AND (melatonin) (tryptophan) AND (sleep) |
Meta-analyses, systematic reviews, randomised controlled trials, clinical trials and reviews published in the past 5 years |
| Valerian |
(valerian) AND (melatonin) (valerian) AND (sleep) |
Any kind of article published in the past 5 years |
| L-theanine |
(L-theanine) AND (melatonin) (L-theanine) AND (sleep) |
Any type of article published in the past 5 years |
| Poppy flower |
(poppy) AND (melatonin) (poppy) AND (sleep) |
Any type of article published in the past 10 years |
| Linden |
(linden) AND (melatonin) (linden) AND (sleep) |
Any type of article published in the past 10 years |
| Orange blossom |
(orange blossom) AND (melatonin) (orange blossom) AND (sleep) |
Any type of article published in the past 10 years |
| Chamomile |
(camomile) AND (melatonin) (camomile) AND (sleep) |
Any type of article published in the past 10 years |
| Royal jelly |
(royal jelly) AND (melatonin) (royal jelly) AND (sleep) |
Any type of article published in the past 10 years |
| Magnolia bark |
(magnolia) AND (melatonin) (magnolia) AND (sleep) |
Any type of article published in the past 10 years |
| California poppy |
(California poppy) AND (melatonin) (California poppy) AND (sleep) |
Any type of article published in the past 10 years |
| Hawthorn |
(white hawthorn) AND (melatonin) (white hawthorn) AND (sleep) |
Any type of article published in the past 10 years |
RESULTS
Review of melatonin products
We analysed 37 different manufacturing brands, adding up to a total of 53 products. Most doses were given as drops or millilitres (38.5%) (Table 2).
| Table 2. Products with melatonin sold over the counter in pharmacies | ||||||
|---|---|---|---|---|---|---|
| Product (manufacturer)® | Melatonin | Other ingredients | Dosage form | Administration | Age range | Allergens |
| Aquilea sueño Express (Aquilea) | 1 mg/1 puff | No | 12 mL | 1 puff | Not specified | Gluten-free, lactose-free, sugar-free |
| Aquilea sueño gotas (Aquilea) | 1 mg/4 drops | 3.2 mg chamomile and 2 mg lemon balm/4 drops | 20 mL | 4 drops | Not specified | Gluten-free, lactose-free |
| Aquilea sueño gummies (Aquilea) | 0.95 mg melatonin + 1 mg melotime/1 gummy | 100 mg lemon balm, 25 mg Passiflora, 25 mg California poppy and 1.4 mg vitamin B6/1 gummy | 30 gummies | 1 gummy | Not specified | Gluten-free, lactose-free, sugar-free |
| Aquilea sueño Instant (Aquilea) | 1.95 mg/1 packet | 100 mg lemon balm, 100 mg Passiflora, 50 mg California poppy/1 packet | 25 packets | 1 packet | Not specified | Gluten-free, lactose-free |
| Arkosueño melatonin gotas (Arkopharma) | 1 mg/4 drops | No | 30 mL | 4 drops | >6 months | Not specified |
| Buonadiem (Buona) | 1 mg/0.2 mL | No | 20 mL | 4 drops | Not specified | Gluten-free, lactose-free |
| Buonadiem 5 tripto (Buona) | 1 mg/0.5 mL | 1.5 mg zinc and 10 mg tryptophan/0.5 mL | 30 mL | 0.5 mL | Not specified | Gluten-free, lactose-free |
| Buonadiem plus (Buona) | 1 mg/1 packet | 1.4 mg vitamin B6 and 100 mg L-theanine/1 packet | 20 packets | 1 packet | Not specified | Gluten-free, lactose-free |
| Dormipol (Plantapol) | 1 mg/1 mL | No | 30 mL | 1 mL | Not specified | Not specified |
| Holoextract melatonina sueño (Equisalud) | 1 mg/4 drops | 2.5 mg Passiflora and 2.5 mg California poppy/4 drops | 50 mL | 4 drops | Not specified | Not specified |
| Jellykids dulces sueños (Eladiet) | 1 mg/10 mL | 150 mg royal jelly, 200 mg lavender, 125 mg chamomile, 500 mg lemon balm and 125 mg linden/10 mL | 250 mL | 10 mL | >3 years | Gluten-free, lactose-free |
| Just sleep melatonina gotas (Ceutics) | 0.5 mg/5 drops | No | 30 mL | 5 drops | >12 years | Not specified |
| Kurasueño de inicio (Kurasana) | 1 mg/2 puffs | No | 60 mL | 2 puffs | Not specified | Gluten-free, lactose-free, sugar-free |
| Kurasueño de mantenimiento (Kurasana) | 1 mg/3 puffs | 1.7 mg vitamin B6 and 25.5 mg tryptophan/3 puffs | 60 mL | 3 puffs | Not specified | Gluten-free, lactose-free, sugar-free |
| Lipolife liposomal melatonina (Equisalud) | 1 mg/1 puff | No | 30 ml | 1 puff | Not specified | Not specified |
| Melamil (Humana) | 1 mg/4 drops | No | 30 mL | 4 drops | Not specified | Gluten-free |
| Melamil tripto (Humana) | 1 mg/0.5 mL | 1.4 mg vitamin B6 and 29 mg tryptophan/0.5 mL | 30 mL | 0.5 mL | >3 years | Gluten-free |
| Melanoctina gotas sublinguales (Plameca) | 1.95 mg/0.5 mL | No | 50 mL | 0.1 mL to 0.25 mL | >3 years | Gluten-free, lactose-free |
| Melanoctina spray (Plameca) | 0.95 mg/3 puffs | No | 30 mL | 1 to 3 puffs | >3 years | Gluten-free, lactose-free, CMP-free |
| Melatonin Pura Gotas (ESI) | 1 mg/1 mL | No | 50 mL | 10 drops or 1 mL | >3 years | Gluten-free, lactose-free, sugar-free |
| Melatonin Pura Gotas Hierbas de la noche (ESI) | 1 mg/1 mL | 10.08 mg valerian, 30 mg chamomile, 100.2 mg Passiflora, 100.2 mg California poppy, 16.12 mg linden, 31.4 mg hawthorn/1 mL | 50 mL | 1 mL | Not specified | Gluten-free, lactose-free |
| Melatonin Pura Gotas Junior (ESI) | 1 mg/1 mL | No | 40 mL | 1 mL | >3 years | Gluten-free, lactose-free, sugar-free |
| Melatonin Pura Spray (ESI) | 1 mg/2 puffs | No | 20 mL | 1 or 2 sprays | Not specified | Gluten-free, sugar-free |
| Melatonin Sleep support gummies (Weider) | 1 mg/1 gummy | 0.7 mg vitamin B6/1 gummy | 60 gummies | 1 gummy | Not specified | Gluten-free, sugar-free |
| Melatonina & GO (Pharma & Go) | 1 mg/22 drops | No | 30 mL | 11 or 22 drops | Not specified | Not specified |
| Melatonina + Ashwagandha pasiflora y camomila (Sanon) | 1.8 mg/1 stick | 150 mg ashwagandha, 150 mg chamomile, 180 mg Passiflora/1 stick | 30 sticks | 1 stick | >12 years | Not specified |
| Melatonina family gotas (Epaplus Sleepcare) | 1 mg/4 drops | 0.21 mg vitamin B6/4 drops | 30 mL | 4 drops | Not specified | Not specified |
| Melatonina spray (Longlife) | 1 mg/1 puff | No | 30 mL | 1 o 2 puffs | Not specified | Gluten-free |
| Melatonina flash (Natysal) | 0.98 mg/1 puff | No | 30 mL | 1 puff | >6 years | Not specified |
| Melatonina gotas (Soria Natural) | 1.8 mg/10 drops | No | 50 mL | 10 drops or 0.5 mL | >3 years | Gluten-free |
| Melatonina gotas (Soñodina) | 1 mg/3 drops | 0.21 mg vitamin B6/3 drops | 20 mL | 3 drops | >3 years | Gluten-free, lactose-free |
| Melatonina gotas (Farline) | 1 mg/4 drops | No | 30 mL | 4 drops | >3 years | Not specified |
| Melatonina gotas (Zenement) | 1 mg/4 drops | No | 50 mL | 4 to 7 drops | Not specified | Gluten-free, lactose-free |
| Melatonina líquida Kids (Drasanvi) | 1 mg/10 drops | 0.67 mg vitamin B6/10 drops | 50 mL | 10 drops | Not specified | Gluten-free |
| Melatonova líquida (Nova Diet) | 1 mg/1 mL | No | 30 mL | 1 mL | Not specified | Gluten-free, lactose-free, sugar-free |
| Mellatoplus gotas (Lavigor) | 1 mg/3 drops | No | 30 mL | 3 drops | Not specified | Not specified |
| Natusleep sueño gominolas (Natusure) | 1 mg/1 gummy | 0.7 mg vitamin B6/1 gummy | 60 gummies | 1 gummy | >8 years | Gluten-free, lactose-free |
| Ninamil (FARDI) | 1 mg/1 mL | No | 50 mL | 1 mL | Not specified | Gluten-free, lactose-free, sugar-free |
| NS melatonina gotas (CINFA) | 1 mg/4 drops | No | 30 mL | 4 drops | >6 months | Gluten-free, lactose-free, CMP-free, nut-free |
| Oniria gotas (Italfarmaco) | 1 mg/4 drops | No | 25 mL | 4 drops | Not specified | Gluten-free, lactose-free, sugar-free |
| Serenesi notte (ESI) | 1 mg/2 mL | 250 mg ashwagandha and 200 mg lavender/2 mL | 50 mL | 1 or 2 mL | >3 years | Gluten-free, sugar-free |
| Serenotte gotas (Specchiasol) | 1.9 mg/12 drops | 55.1 mg California poppy, 18.2 mg poppy petals and 15.2 mg L-theanine/12 drops | 50 mL | 12 drops | >3 years | Gluten-free |
| Seripnol gotas (Neuraxpharm) | 1 mg/10 drops | 5 mg magnolia, 2 mg jujube and 30 mg L-theanine/10 drops | 30 mL | 10 drops | Not specified | Gluten-free |
| Sleep vitamins (Chic & love) | 1 mg/1 gummy | 0.7 mg vitamin B6/1 gummy | 60 gummies | 1 gummy | Not specified | Gluten-free, sugar-free |
| Sleep well liquid (Zentrity by naturitas) | 1 mg/4 drops | 3.2 mg chamomile, 2 mg lemon balm and 2 mg Passiflora/4 drops | 50 mL | 4 drops | Not specified | Gluten-free, lactose-free |
| Sleepeel gotas (Heel) | 1 mg/0.5 mL | 40 mg lemon balm, 100 mg Passiflora, 1.2 mg vitamin B6 and 1.5 mg tryptophan/0.5 mL | 30 mL | 0.5 mL | >3 years | Gluten-free, lactose-free |
| Sleepeel noche (Heel) | 1 mg/1 gummy | 40 mg lemon balm, 100 mg Passiflora and 1.4 mg vitamin B6/1 gummy | 60 gummies | 1 gummy | >3 years | Gluten-free, lactose-free |
| Sleepeel spray (Heel) | 1 mg/3 puffs | 40 mg lemon balm, 100 mg Passiflora and 1.2 mg vitamin B6/2 puff | 20 mL | 3 puffs | >3 years | Gluten-free, lactose-free, sugar-free |
| Somnolem melatonina spray (Waydiet) | 1 mg/3 puffs | 289.8 mg orange blossom, 6 mg lemon balm, 0.73 mg vitamin B1, 0, 93 mg vitamin B6 and 3 mcg vitamin B8/3 puff | 20 mL | 3 puffs | >12 years | Gluten-free |
| Soñadores gotas (Ordesa) | 1 mg/0.5 mL | 1.4 mg vitamin B6 and 20 mg tryptophan/0.5 mL | 30 mL | 0.5 mL | >3 years | Gluten-free, lactose-free, CMP-free |
| Soñadores spray (Ordesa) | 1 mg/1 puff | No | 15 mL | 1 puff | >3 years | Not specified |
| Sweet sleep gummies (Jelly Pills) | 1 mg/2 gummies | 25 mg chamomile and 0.7 mg vitamin B6/2 gummies | 60 gummies | 2 gummies | Not specified | Gluten-free, lactose-free |
| ZzzQuil NATURA (Vicks) | 1 mg/1 gummy | 30 mg valerian, 10 mg chamomile, 10 mg lavender and 1.4 mg vitamin B6/1 gummy | 30 or 60 gummies | 1 gummy | Not specified | Not specified |
|
CMP: cow’s milk protein. |
||||||
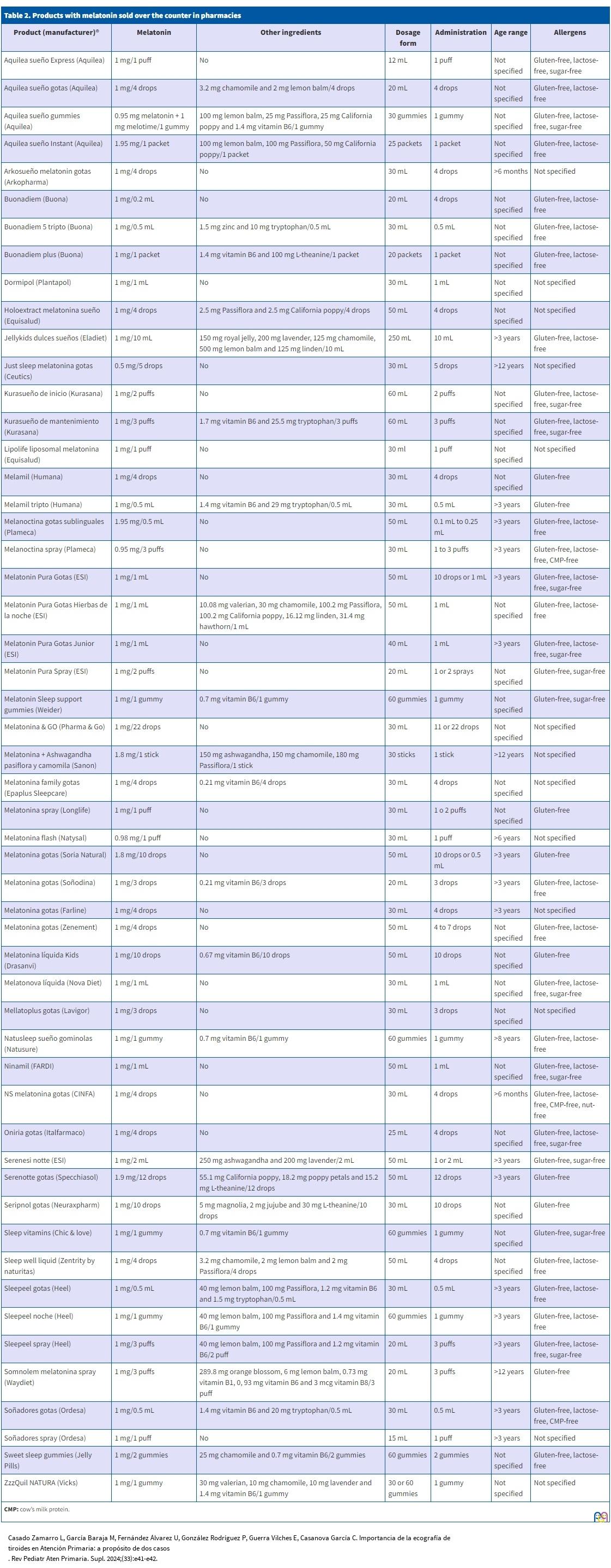
The dose of melatonin typically recommended by the manufacturer was 1 mg a day, although 9.4% of products had greater recommended doses of up to 1.95 mg of melatonin a day. Forty-seven percent of the products had melatonin as the sole active ingredient. The most frequently added active ingredient, found in as many as 32% of the products, was vitamin B6, with a dose range of 0.21 to 1.7 mg a day (most frequent dose, 1.4 mg/day). Lemon balm and Passiflora were the most frequently added herbal ingredients, present in 16.9% of the products at doses of 2 to 500 mg a day (most frequently 40 mg) and 2.5 to 180 mg a day (most frequently 100 mg), respectively. Orange blossom, royal jelly, magnolia bark, jujube, hawthorn and poppy were each only found in one product. The most frequent combination was lemon balm with Passiflora, followed by Passiflora with California poppy, vitamin B6 with tryptophan and manzanilla with lemon balm.
When it came to the excipients, we found citric acid used as an acidulant, sodium benzoate and potassium sorbate as preservatives, sorbitan monooleate polyoxyethylene and soy lecithin as emulsifiers, xanthan gum as a thickener, glycerol as a stabiliser and sorbitol or mannitol or sucralose as sweeteners. Only one product contained palm oil and one other product contained silicon dioxide.
Review of the literature
After the initial search, we identified 5 articles discussing the use of melatonin in children; we excluded 2 because they focused on the use of melatonin in children with health conditions (autism spectrum disorder, attention-deficit hyperactivity disorder). Thus, we selected 3 articles from this search. The Spanish language search yielded 3 articles, one of which was excluded due to focusing on children with disease and the other for being an older version of the sleep consensus document that we ended up including in the review.
In the specific search for active ingredients, we found 3 articles for vitamin B6, 2 for lemon balm, 2 for Passiflora, 7 for ashwagandha, 5 for jujube, 2 for lavender, 1 for manzanilla, 2 for zinc, 4 for tryptophan, 4 for valerian and 4 for l-theanine. We did not find any studies regarding the mechanism of action or the association with sleep of common poppy, Tilia, jujube, other chamomile species, royal jelly, magnolia bark, California poppy and hawthorn.
None of these products was registered specifically in the AEMPS. Only one manufacturer presented literature references regarding the product, 2 clinical trials of its use to induce sleep in children for non-invasive diagnostic procedures and 1 clinical trial in children with chronic headache. We did not include these articles in the analysis presented in the discussion, as they did not fit the scope of our review.
DISCUSSION
Recommended melatonin dose
At present, there is no established consensus on the dose of melatonin that is effective in the paediatric population. The main reviews recommend its use starting with doses of 1 to 3 mg a day in infancy and early childhood, with doses of 2.5 to 5 mg a day in older children, increasing the dose gradually based on the response.3,4 They also specify that continuous treatment should not exceed 4 weeks in duration. We ought to highlight that recurrence is expected upon discontinuation of melatonin in 90% of cases of sleep-onset insomnia treated exclusively with this substance.3 All reviews agree that melatonin should always be given at the same time, 20 to 60 minutes before bedtime.3,4
In comparison, in the reviewed products, the recommended initial dose was 1 mg a day, except in 5 products, which recommended starting with 1.95 mg a day. Doses that, based on the evidence described above, may not be sufficient depending on the characteristics of the patient. None of the manufacturers recommended different doses based on age or increasing the dose if the desired effect is not achieved.
Additional components
Vitamin B6
Sixteen of the 53 reviewed products (30.2%) contained, among other components, vitamin B6, which was the most frequently used component other than melatonin. Although it is attributed a positive impact on sleep in some cases, 5-7 there is limited evidence and its administration is usually studied in combination with other components. Furthermore, its association with insomnia is not as clear as it is with magnesium, whose role in sleep regulation is more clearly established. There is no consensus regarding the effective dose, but it is clear that the maximum safe dose is 100 mg/day to avoid adverse events such as sensory neuropathy, photosensitivity, gastrointestinal problems…5 The most frequently recommended dose is 1.4 mg a day.
Lemon balm and Passiflora
Among the reviewed products, 16.9% contained Melissa officinalis and Pasiflora incarnata, and the most recommended doses of each of these plants were 40 mg and 100 mg daily. They were the plants used most frequently in the reviewed products. There is evidence that their properties may have a beneficial effect on sleep and insomnia.8-11 Some studies attribute antibacterial, neuroprotective and anti-inflammatory properties to lemon balm in addition to its sedative or relaxing properties, which supports its use to alleviate insomnia or stress.9,10 There is no evidence on the dose that is effective to achieve each of these effects. Passiflora, in turn, has anxiolytic and sedative effects and helps regulate sleep, increasing the activity of γ-aminobutyric acid-producing neurons and melatonin in blood.10,11 However, there is also no evidence on the dose that would be effective to achieve these benefits.
Ashwagandha
Withania somnifera is a medicinal plant that has been used in India for centuries to treat insomnia. It has been studied on account of biological activity that may have neuroprotector, antimicrobial, antidiabetic, anti-inflammatory and adaptogenic effects to reduce anxiety and as a natural compound with potential for inducing sleep, reducing sleep latency onset and improving sleep quality in patients with insomnia.12-18 It is believed to work through interaction with GABA receptors.16,17. This compound is well tolerated. The effective dose has yet to be clearly established, some studies have used 300 mg of extract twice daily and others a dose based on weight (10-50 mg/kg a day).13-15
Two of the 53 analysed products contained ashwagandha. The recommended doses were 150 mg and 250 mg daily. This doses, given that we are discussing the paediatric population, in which the body weight is smaller compared to adults, may be consistent with the existing evidence.
Jujube
Ziziphus jujuba is a fruit grown in different parts of the world and used in traditional medicine as having positive effects on sleep and relaxation. Although it does not induce sleep directly, it is attributed properties that could contribute to improve its quality in individuals with sleep disorders, particularly in relation to sleep latency.19-23 There are data that suggest that its main mechanism of action is the stimulation of GABA receptors,22,23 although additional studies are required to confirm this. It is most frequently used in combination with other herbal remedies. We did not find any data in any of the reviewed articles regarding the recommended dosage.
Only one of the products reviewed in our study contained jujube, and the recommended dose is 2 mg a day.
Lavender
This plant is chiefly known for its aroma, but there is also evidence of its positive impact on sleep due to its sedative and hypnotic properties. The active ingredients and mechanisms of lavender that aid sleep have not been clearly establish, although there are studies that associate it with GABAergic, cholinergic and histaminergic systems, monoamines in the limbic system24 and the serotoninergic system.25 None of the reviewed articles specified recommended doses of this substance.
Two of the products reviewed in the study included lavender. The recommended dose was 10 mg in one and 200 mg in the other.
Manzanilla
Matricaria chamomilla, known as manzanilla in Spain, is one of the chamomile plants traditionally used for its relaxing properties and the potential to promote calm sleep. Although the evidence on its effects are limited, some studies suggest that it may have positive effects on sleep and fewer adverse effects than conventional drugs.26
Five of the reviewed products had manzanilla among their components. The recommended dose varies widely: from 3.2 to 125 mg a day. We did not find studies specifying the recommended effective dose.
Zinc
The association between the concentration of this essential mineral in blood and sleep quality is attracting growing interest. There are data suggesting that zinc may play a role in sleep optimisation and quality,27,28 especially in adolescents.27 However, the evidence is still scarce and more studies are required to gain an adequate understanding of the role of zinc in glutamatergic transmission and its interaction with other neurotransmitters associated with sleep.28 We did not find a recommended effective dose in the reviewed literature.
In our study, only one of the reviewed products contained zinc, with a recommended dose of 1.5 mg a day.
Tryptophan
It is an essential amino acid that plays an important role in protein synthesis and the production of neurotransmitters in the brain, for instance, serotonin, from which melatonin is synthesised.29-32 Studies have found improvement in different sleep parameters following consumption of tryptophan, chief among them an increased duration and efficiency of sleep, a decreased latency, improvement in night wakings and a decrease in parasomnias.29,31,32 More studies with longer followups are required to assess specific diets enriched with tryptophan in relation to sleep.29 We ought to highlight that glucose-rich foods can also have a positive impact on sleep, as glucose facilitates the passage of tryptophan through the blood-brain barrier.30 The dose range used in studies on this amino acid in paediatric patients with parasomnias was 500 to 4500 mg daily (mean dose of 2400 mg/day).32
Only 9.4% of the products in our study included tryptophan among their ingredients. The recommended daily dose in 3 of these products was relatively homogeneous, in the range of 20 to 30 mg a day, for the other 2, the recommended doses were 10 mg and 1.5 mg, respectively, and all recommended doses were much lower than the doses reported in the reviewed literature.
Valerian
It is a medicinal plant traditionally used to treat sleep disorders, such as insomnia, and anxiety.33-36
Some studies suggest that valerian may be useful, due to its sedative and anxiety-reducing properties, to improve perceived sleep quality and reduce difficulty falling asleep,33,35,36 although it requires multiple doses to achieve significant effects.33 The doses used in the main studies ranged between 160 and 600 mg a day, although a minimum effective dose has not been established.36 The mechanism of action of valerian has not been clearly elucidated, although it is believed that it involves acting on the GABA neurotransmitter through inhibition of sympathetic activity.35 Some studies did not find significant benefits compared to placebo.35,36 The inconsistency of the results may be due to differences in the quality of the studies, the doses used and the routes of administration of valerian. Despite these differences, most of the sources reviewed agreed that this substance is safe and causes few adverse effects.33,35
Only 2 of the reviewed products included this component. The recommended daily dose was 10.08 mg in one of them and 30 mg in the other, far below the dose use in the main studies.
l-theanine
It is a non-protein amino acid chiefly found in green tea leaves. It has been studied for its possible relaxation and stress-reducing properties, and some studies suggest that it may have a positive impact on sleep quality.37-40 It is believed to stimulate the production of alpha waves in the brain, which are associated with a relaxed state, without causing subsequent somnolence or changes in motor function.39,40 It may also increase the production of dopamine and serotonin by improving GABA levels, which are involved in mood and sleep regulation.40 It is believed that it may safely and effectively improve sleep quality in children with attention-deficit hyperactivity disorder (ADHD).35,40 The doses used in the reviewed literature were 400 mg daily in children with ADHD aged 8 to 12 years40 and 200 mg a day in healthy adults39; high doses are generally well tolerated (up to 4000 mg/kg/day)39 with few associated adverse effects.38
Only 3 reviewed products contained l-theanine. The daily doses recommended in the label were 100 mg, 30 mg and 15.2 mg, respectively, doses that varied widely and that were all lower than the dose used in the most important studies.
To conclude, we ought to highlight that the collection of this information was challenging because in many instances the composition of the products was not clearly specified or represented graphically. The reason may be that these products are considered dietary supplements and are therefore not subject to the strict control imposed on pharmaceuticals, as is the case in other countries.2
CONCLUSION
Although the efficacy of melatonin for management of sleep disorders is well known and has been widely studied, a consensus has yet to be established regarding the effective dose of melatonin in the paediatric population.
Furthermore, in recent years, products combining melatonin with other substances(such as lemon balm and Passiflora, the most frequently additions according to our product review) have been introduced in the market. However, there is a larger volume of evidence supporting the use of substances used much less frequently, such as ashwagandha, valerian, l-theanine and jujube. In addition, few doses are standardised, as there is a dearth of studies not only in the paediatric population but also in adults, and when an effective dose has been established, since the studies have been conducted in adults, the substance is usually administered at lower doses in children (except in the case of ashwagandha, for which the doses recommended by the manufacturer match the doses reported in the literature).
Based on our findings, it is reasonable to assert that melatonin is an effective product with ample evidence in support of its use in the management of sleep disorders; however, it is not free of adverse effects and therefore we believe that it should be treated as a pharmaceutical, so that its use requires prescription by a competent professional and adheres to established indications and posology recommendations. As regards the additional ingredients combined with melatonin in these products, given the scarcity of the data on their use in paediatrics and the substantial heterogeneity of the studies on the types of added supplements and their dosage, we conclude that there is insufficient evidence to recommend their use.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
AUTHORSHIP
All authors contributed equally to the published manuscript.
ABBREVIATIONS
ADHD: attention-deficit hyperactivity disorder · AEMPS: Agencia Española de Medicamentos y Productos Sanitarios.
REFERENCES
- Edemann-Callesen H, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. Use of melatonin in children and adolescents with idiopathic chronic insomnia: a systematic review, meta-analysis, and clinical recommendation. EClinicalMedicine. 2023;61(102048):102048. http://dx.doi.org/10.1016/j.eclinm.2023.102048
- Händel MN, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. The short-term and long-term adverse effects of melatonin treatment in children and adolescents: a systematic review and GRADE assessment. EClinicalMedicine. 2023;61(102083):102083. http://dx.doi.org/10.1016/j.eclinm.2023.102083
- Pin Arboledas G, Soto Insuga V, Jurado Luque MJ, Fernandez Gomariz C, Hidalgo Vicario I, Lluch Rosello A, et al. Insomnio en niños y adolescentes. Documento de consenso. An Pediatr (Barc). 2017;86(3):165.e1-165.e11. https://aepap.org/sites/default/files/consenso_espanol_insomnio_2017.pdf
- Edemann-Callesen H, Andersen HK, Ussing A, Virring A, Jennum P, Debes NM, et al. Use of melatonin for children and adolescents with chronic insomnia attributable to disorders beyond indication: a systematic review, meta-analysis and clinical recommendation. EClinicalMedicine. 2023;61:102049. http://dx.doi.org/10.1016/j.eclinm.2023.102049
- García-García C, Baik I. Effects of poly-gamma-glutamic acid and vitamin B6 supplements on sleep status: a randomized intervention study. Nutr Res Pract. 2021;15(3):309. http://dx.doi.org/10.4162/nrp.2021.15.3.309
- Lemoine P, Bablon J-C, Da Silva C. A combination of melatonin, vitamin B6 and medicinal plants in the treatment of mild-to-moderate insomnia: A prospective pilot study. Complement Ther Med. 2019;45:104–8. http://dx.doi.org/10.1016/j.ctim.2019.05.024
- Djokic G, Vojvodic P, Korcok D, Agic A, Rankovic A, Djordjevic V, et al. The effects of magnesium – melatonin - Vit B complex supplementation in treatment of insomnia. Open Access Maced J Med Sci. 2019;7(18):3101-5. http://dx.doi.org/10.3889/oamjms.2019.771
- Zam W, Quispe C, Sharifi-Rad J, López MD, Schoebitz M, Martorell M, et al. An updated review on the properties of Melissa officinalis l.: Not exclusively anti-anxiety. Front Biosci (Schol Ed). 2022;14(2):16. http://dx.doi.org/10.31083/j.fbs1402016
- Roe AL, Venkataraman A. The safety and efficacy of botanicals with nootropic effects. Curr Neuropharmacol. 2021;19(9):1442-67. https://pubmed.ncbi.nlm.nih.gov/34315377/
- Kim G-H, Yi SS. Chronic oral administration of Passiflora incarnata extract has no abnormal effects on metabolic and behavioral parameters in mice, except to induce sleep. Lab Anim Res. 2019;35(1). http://dx.doi.org/10.1186/s42826-019-0034-9
- Kim G-H, Kim Y, Yoon S, Kim S-J, Yi SS. Sleep‐inducing effect of Passiflora incarnata l. extract by single and repeated oral administration in rodent animals. Food Sci Nutr. 2020;8(1):557-66. http://dx.doi.org/10.1002/fsn3.1341
- Langade D, Kanchi S, Salve J, Debnath K, Ambegaokar D. Efficacy and safety of ashwagandha (Withania somnifera) root extract in insomnia and anxiety: A double-blind, randomized, placebo-controlled study. Cureus. 2019;11(9). https://pubmed.ncbi.nlm.nih.gov/31728244/
- Murthy SV, Fathima SN, Mote R. Hydroalcoholic extract of ashwagandha improves sleep by modulating GABA/histamine receptors and EEG slow-wave pattern in in vitro - in vivo experimental models. Prev Nutr Food Sci. 2022;27(1):108-20. http://dx.doi.org/10.3746/pnf.2022.27.1.108
- Park CW, Hong K-B, Suh HJ, Ahn Y. Sleep-promoting activity of amylase-treated Ashwagandha (Withania somnifera l. Dunal) root extract via GABA receptors. J Food Drug Anal. 2023;31(2):27-28. http://dx.doi.org/10.38212/2224-6614.3456
- Cheah KL, Norhayati MN, Husniati Yaacob l, Abdul Rahman R. Effect of Ashwagandha (Withania somnifera) extract on sleep: A systematic review and meta-analysis. PLoS One. 2021;16(9):e0257843. http://dx.doi.org/10.1371/journal.pone.0257843
- Mikulska P, Malinowska M, Ignacyk M, Szustowski P, Nowak J, Pesta K, et al. Ashwagandha (Withania somnifera) - current research on the health-promoting activities: A narrative review. Pharmaceutics. 2023;15(4):1057. https://www.mdpi.com/1999-4923/15/4/1057
- Charu B, Atul U, Umesh S. Efficacy of Brimhana Nasya and Ashwagandha (Withania somnifera (l.) Dunal) root powder in primary insomnia in elderly male: A randomized open-label clinical study. Ayu. 2020;41(3):159. http://dx.doi.org/10.4103/ayu.ayu_177_1
- Kelgane SB, Salve J, Sampara P, Debnath K. Efficacy and tolerability of ashwagandha root extract in the elderly for improvement of general well-being and sleep: A prospective, randomized, double-blind, placebo-controlled study. Cureus. 2020; http://dx.doi.org/10.7759/cureus.7083
- Deng Q, Huang l, Yu F, Lin J, Hu l, Zhao J, et al. Biomedical analytics of four Chinese medicinals in treatment of insomnia based on network pharmacology. Biomed Res Int. 2022;2022:1-11. https://www.hindawi.com/journals/bmri/2022/9414262/
- Shergis JL, Hyde A, Meaklim H, Varma P, Da Costa C, Jackson ML. Medicinal seeds Ziziphus spinosa for insomnia: A randomized, placebo-controlled, cross-over, feasibility clinical trial. Complement Ther Med. 2021;57(102657):102657. http://dx.doi.org/10.1016/j.ctim.2020.102657
- Luo H, Sun S-J, Wang Y, Wang Y-l. Revealing the sedative-hypnotic effect of the extracts of herb pair Semen Ziziphi spinosae and Radix Polygalae and related mechanisms through experiments and metabolomics approach. BMC Complement Med Ther. 2020;20(1). http://dx.doi.org/10.1186/s12906-020-03000-8
- Bae GY, Ahn Y, Hong K-B, Jung E-J, Suh HJ, Jo K. Sleep-Enhancing Effect of Water Extract from Jujube (Zizyphus jujuba Mill.) Seeds Fermented by Lactobacillus brevis L32. Foods. 2023;12(15):2864. https://www.mdpi.com/2304-8158/12/15/2864
- Eom S, Lee S, Lee J, Sohn S-O, Lee JH, Park J. A combination of Rosa multiflora and Zizyphus jujuba enhance sleep quality in anesthesia-induced mice. Int J Mol Sci. 2022;23(22):14177. https://www.mdpi.com/1422-0067/23/22/14177
- Xu Y, Ma l, Liu F, Yao l, Wang W, Yang S, et al. Lavender essential oil fractions alleviate sleep disorders induced by the combination of anxiety and caffeine in mice. J Ethnopharmacol. 2023;302(115868):115868. https://www.sciencedirect.com/science/article/pii/S0378874122009072
- Bruni O, Ferini-Strambi l, Giacomoni E, Pellegrino P. Herbal remedies and their possible effect on the GABAergic system and sleep. Nutrients. 2021;13(2):530. https://www.mdpi.com/2072-6643/13/2/530
- Abdullahzadeh M, Matourypour P, Naji SA. Investigation effect of oral chamomilla on sleep quality in elderly people in Isfahan: A randomized control trial. J Educ Health Promot. 2017. https://pubmed.ncbi.nlm.nih.gov/28616420/
- Ji X, Liu J. Associations between blood zinc concentrations and sleep quality in childhood: A cohort study. Nutrients. 2015;7(7):5684–96. https://pubmed.ncbi.nlm.nih.gov/26184300/
- Cherasse Y, Urade Y. Dietary zinc acts as a sleep modulator. Int J Mol Sci. 2017;18(11):2334. https://www.mdpi.com/1422-0067/18/11/2334
- Binks H, E. Vincent G, Gupta C, Irwin C, Khalesi S. Effects of diet on sleep: A narrative review. Nutrients. 2020;12(4):936. http://dx.doi.org/10.3390/nu12040936
- Pereira N, Naufel MF, Ribeiro EB, Tufik S, Hachul H. Influence of dietary sources of melatonin on sleep quality: A review. J Food Sci. 2020;85(1):5–13. http://dx.doi.org/10.1111/1750-3841.14952
- Saidi O, Rochette E, Doré É, Maso F, Raoux J, Andrieux F, et al. Randomized double-blind controlled trial on the effect of proteins with different tryptophan/large neutral amino acid ratios on sleep in adolescents: The PROTMORPHEUS study. Nutrients. 2020;12(6):1885. http://dx.doi.org/10.3390/nu12061885
- Innocenti A, Lentini G, Rapacchietta S, Cinnirella P, Elia M, Ferri R, et al. The role of supplements and over-the-counter products to improve sleep in children: A systematic review. Int J Mol Sci. 2023;24(9):7821. http://dx.doi.org/10.3390/ijms24097821
- Shinjyo N, Waddell G, Green J. Valerian root in treating sleep problems and associated disorders - A systematic review and meta-analysis. J Evid Based Integr Med. 2020;25:2515690X2096732. http://dx.doi.org/10.1177/2515690x20967323
- Zhao F-Y, Xu P, Kennedy GA, Conduit R, Zhang W-J, Wang Y-M, et al. Identifying complementary and alternative medicine recommendations for insomnia treatment and care: a systematic review and critical assessment of comprehensive clinical practice guidelines. Front Public HealtH. 2023;11. http://dx.doi.org/10.3389/fpubh.2023.1157419
- Borrás S, Martínez-Solís I, Ríos JL. Medicinal plants for insomnia related to anxiety: An updated review. Planta Med. 2021;87(10/11):738-53. http://dx.doi.org/10.1055/a-1510-9826
- Guadagna S, Barattini DF, Rosu S, Ferini-Strambi l. Plant extracts for sleep disturbances: A systematic review. Evid Based Complement Alternat Med. 2020;2020:1-9. http://dx.doi.org/10.1155/2020/3792390
- Deshpande SN, Simkin DR. Complementary and integrative approaches to sleep disorders in children. Child Adolesc Psychiatr Clin N Am. 2023;32(2):243-72. https://pubmed.ncbi.nlm.nih.gov/37147039/
- Zhang Y, Jia X, Chen X, Liu Y, Zhao Z, Hao J, et al. l-theanine and Neumentix mixture improves sleep quality and modulates brain neurotransmitter levels in mice. Ann Palliat Med. 2021;10(4):4572–81. http://dx.doi.org/10.21037/apm-21-663
- Thiagarajah K, Chee HP, Sit NW. Effect of alpha-S1-casein tryptic hydrolysate and l-theanine on poor sleep quality: A double blind, randomized placebo-controlled crossover trial. Nutrients. 2022;14(3):652. http://dx.doi.org/10.3390/nu14030652
- Dasdelen MF, Er S, Kaplan B, Celik S, Beker MC, Orhan C, et al. A novel Theanine complex, Mg-l-Theanine improves sleep quality via regulating brain electrochemical activity. Front Nutr. 2022;9. http://dx.doi.org/10.3389/fnut.2022.874254
Comments
This article has no comments yet.