
Vol. 25 - Num. 100
Originales
Problemas sociales: mucha frecuencia, poca formación
M.ª Llanos de la Torre Quiraltea, Rafael Jiménez Alésb, Raquel Páez Gonzálezc, Nisa Boukichou Abdelkaderd, Antonio Gancedo Barandae, M.ª Luisa Poch Olivéf
aPediatra. CS Labradores. Logroño. España
bPediatra. CS La Roda de Andalucía. Sevilla. España.
cPediatra. CS 5B. Albacete. España.
dEstadística. Unidad de Ciencia del Dato. Innovación Sanitaria de Fundación Rioja Salud. Centro de Investigación Biomédica de La Rioja (CIBIR). Logroño. La Rioja. España.
eServicio de Pediatría. Hospital Universitario Fundación Alcorcón. Madrid. España
fServicio de Neuropediatría. Hospital San Pedro. Logroño. España
Correspondencia: MLL de la Torre. Correo electrónico: mpmjlj@gmail.com
Cómo citar este artículo: de la Torre Quiralte MLL, Jiménez Alés R, Páez González R, Boukichou Abdelkader N, Gancedo Baranda A, Poch Olivé ML. Problemas sociales: mucha frecuencia, poca formación . Rev Pediatr Aten Primaria. 2023;25:389-98. https://doi.org/10.60147/a08fe31c
Publicado en Internet: 29-11-2023 - Número de visitas: 11541
Resumen
Introducción: la patología social pediátrica en relación con inequidades socioeconómicas, relaciones disfuncionales familiares, inmigración, adicciones, violencia hacia la infancia, etc. va en aumento. El objetivo de este trabajo es analizar su peso en la labor asistencial del pediatra, la descripción de la formación y los conocimientos en ese ámbito, y las razones que dificultan su implicación en estos temas.
Metodología: estudio multicéntrico a través de encuesta online cumplimentada por 407 profesionales médicos. Se analizaron 11 problemas en relación con el entorno familiar, escolar, pobreza, inmigración, adicciones y violencia.
Resultados: los problemas del entorno familiar o escolar fueron señalados como frecuentes o muy frecuentes por alrededor del 50% de los profesionales; los relacionados con inmigración, acoso y pobreza, por el 20-30%; y los referidos a violencia o adicciones, por menos del 10%. Sin embargo, los porcentajes de formación recibida (y de conocimientos) fueron muy bajos en todos los temas (la mayor formación se aprecia en violencia de género y abuso). Se desglosan los resultados según el ámbito profesional de trabajo (hospitalario o Atención Primaria), el entorno (urbano o rural) y la edad. La mayor dificultad que alegan los profesionales para el abordaje de estos problemas es precisamente la falta de formación.
Conclusiones: la patología social infantil está muy presente en la labor diaria del pediatra. Por ello, se precisa una adecuada formación y actualización en esta materia que permita detectar y atender esta patología como el resto de los problemas de la infancia. Se proponen acciones de mejora.
Palabras clave
● Determinantes sociales de la salud ● Formación pediátrica ● Pobreza ● Problemas familiares ● Problemas sociales ● ViolenciaINTRODUCCIÓN
En las últimas décadas, la patología social pediátrica ha aumentado enormemente en relación con inequidades socioeconómicas, relaciones disfuncionales familiares, inmigración, adicciones, violencia hacia la infancia, etc.1. Esta realidad implica la necesidad de cambiar la atención al niño, centrada en la enfermedad (y en los procesos agudos) y reorientarla hacia los condicionantes sociales de salud, con una perspectiva enfocada en la infancia y su entorno, lo que implica un abordaje coordinado multidisciplinar.
Los pediatras ocupan una posición privilegiada para detectar indicadores y condicionantes de riesgo. Las características propias de esos problemas implican un alto grado de sufrimiento en los menores y sus familias, lo que conlleva un aumento en la demanda de la atención sanitaria. La observación de las relaciones del niño con su entorno próximo durante los ingresos hospitalarios y el seguimiento del desarrollo (revisiones de los programas de salud infantil) y la atención de los procesos agudos de los niños en las consultas de Atención Primaria (AP) proporcionan una visión de cada niño en su conjunto. Se precisa, por tanto, una coordinación entre esos dos ámbitos, junto con los médicos de familia (y el personal de enfermería), y los referentes escolares, asociativos y de servicios sociales, para obtener una visión que permita detectar y ayudar a superar los eventos adversos que les puedan suceder.
Pero para ello se precisa saber, querer y poder preguntar (formación, implicación y medios para llevarlo a cabo).
La correcta detección de los problemas sociales considerados erróneamente como “menores” (provocados por la pobreza o la inmigración, por problemas familiares, por compañeros del colegio u otros menores, por la separación conflictiva de los progenitores, etc.) que tan frecuentemente vemos cada día en nuestro trabajo, redundaría en un mejor abordaje y disminuiría en gran medida las graves consecuencias que suelen provocar en la vida de esos futuros adultos. La mayoría de los problemas sociales más graves (abuso, maltrato, violencia, adicciones) están precedidos de los mencionados anteriormente.
La finalidad de este trabajo es analizar el peso de dichos problemas en la labor actual del pediatra, la descripción de la formación y los conocimientos en ese ámbito, y los obstáculos que subjetivamente aprecian para implicarse en su abordaje. Con los resultados obtenidos se podrán plantear estrategias que ayuden a mejorar la asistencia a nuestros pacientes.
MÉTODOS
Presentamos un estudio multicéntrico aprobado por el Comité Ético de Investigación Clínica de La Rioja (Ref. CEImLAR P.I. 532), para el que se construyó y validó un cuestionario elaborado por el propio equipo de investigación2.
Se diseñó un estudio descriptivo transversal mediante una encuesta online, utilizando Formularios de Google. Se distribuyó a nivel nacional entre profesionales médicos que trabajan con personas menores de edad (especialistas en Pediatría, en Medicina de Familia y Comunitaria y residentes [MIR] de ambas especialidades) a través de correo electrónico institucional (Asociación Española de Pediatría [AEP] y sociedades regionales integradas, AEP de Atención Primaria, Sociedad Española de Pediatría Social, Sociedad Española de Medicina de la Adolescencia, Asociación MIR España y Sociedad Española de Medicina de Familia y Comunitaria) y de la lista de distribución PEDIAP de RedIris que agrupa a los profesionales mencionados desde diferentes grupos de trabajo, mediante un enlace que garantizaba el anonimato y la voluntariedad. La población diana estimada es de unos 12 0003,4 (ajustando el nivel de confianza al 95%, serían necesarias 373 respuestas). Se obtuvieron 407 respuestas válidas. Se distribuyó el cuestionario durante los meses de junio y julio de 2021.
El estudio fue avalado por la Sociedad Española de Pediatría Social.
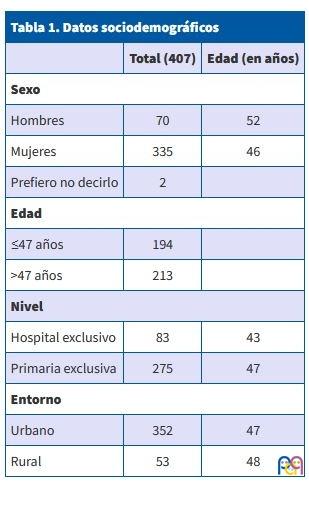
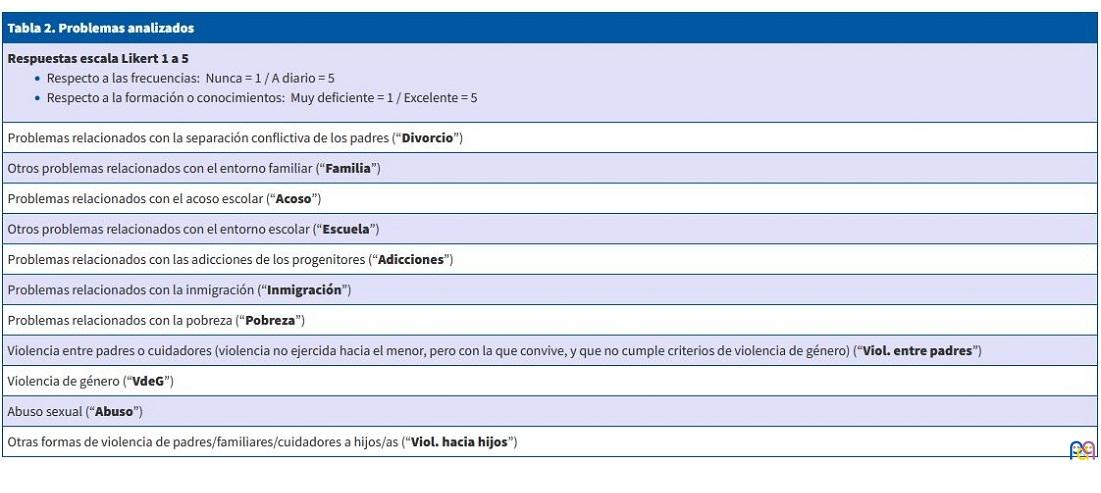
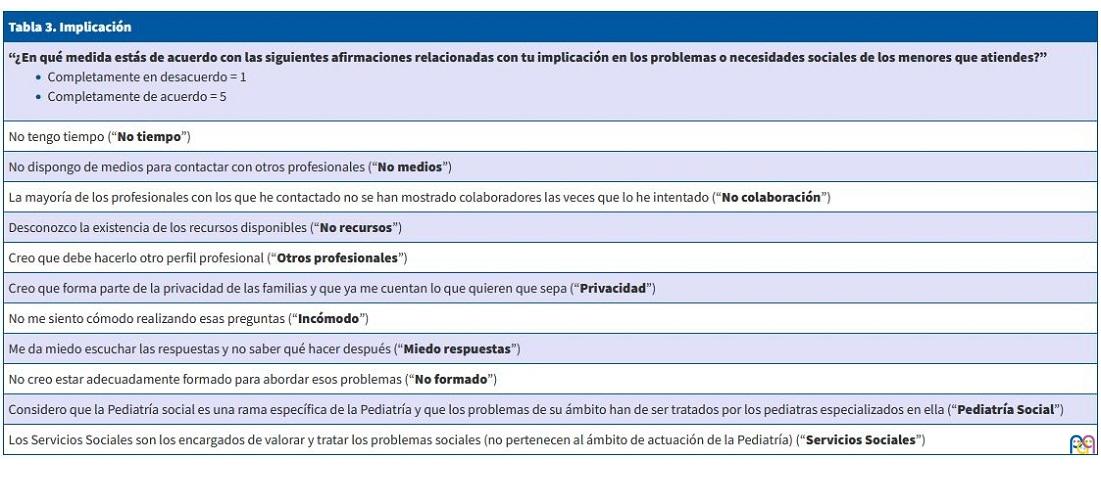
La encuesta recoge datos sociodemográficos de los profesionales (Tabla 1), y aspectos sobre frecuencia, formación ofertada y la apreciación personal de los propios conocimientos de cada encuestado sobre los problemas sociales que afectan a los menores, referido todo ello a los últimos 3 años (Tabla 2). Y los obstáculos que encuentran para su implicación al abordarlos (Tabla 3).
| Tabla 1. Datos sociodemográficos | ||
|---|---|---|
| Total (407) | Edad (en años) | |
| Sexo | ||
| Hombres | 70 | 52 |
| Mujeres | 335 | 46 |
| Prefiero no decirlo | 2 | |
| Edad | ||
| ≤47 años | 194 | |
| >47 años | 213 | |
| Nivel | ||
| Hospital exclusivo | 83 | 43 |
| Primaria exclusiva | 275 | 47 |
| Entorno | ||
| Urbano | 352 | 47 |
| Rural | 53 | 48 |
| Tabla 2. Problemas analizados |
|---|
Respuestas escala Likert 1 a 5
|
| Problemas relacionados con la separación conflictiva de los padres (“Divorcio”) |
| Otros problemas relacionados con el entorno familiar (“Familia”) |
| Problemas relacionados con el acoso escolar (“Acoso”) |
| Otros problemas relacionados con el entorno escolar (“Escuela”) |
| Problemas relacionados con las adicciones de los progenitores (“Adicciones”) |
| Problemas relacionados con la inmigración (“Inmigración”) |
| Problemas relacionados con la pobreza (“Pobreza”) |
| Violencia entre padres o cuidadores (violencia no ejercida hacia el menor, pero con la que convive, y que no cumple criterios de violencia de género) (“Viol. entre padres”) |
| Violencia de género (“VdeG”) |
| Abuso sexual (“Abuso”) |
| Otras formas de violencia de padres/familiares/cuidadores a hijos/as (“Viol. hacia hijos”) |
| Tabla 3. Implicación |
|---|
“¿En qué medida estás de acuerdo con las siguientes afirmaciones relacionadas con tu implicación en los problemas o necesidades sociales de los menores que atiendes?”
|
| No tengo tiempo (“No tiempo”) |
| No dispongo de medios para contactar con otros profesionales (“No medios”) |
| La mayoría de los profesionales con los que he contactado no se han mostrado colaboradores las veces que lo he intentado (“No colaboración”) |
| Desconozco la existencia de los recursos disponibles (“No recursos”) |
| Creo que debe hacerlo otro perfil profesional (“Otros profesionales”) |
| Creo que forma parte de la privacidad de las familias y que ya me cuentan lo que quieren que sepa (“Privacidad”) |
| No me siento cómodo realizando esas preguntas (“Incómodo”) |
| Me da miedo escuchar las respuestas y no saber qué hacer después (“Miedo respuestas”) |
| No creo estar adecuadamente formado para abordar esos problemas (“No formado”) |
| Considero que la Pediatría social es una rama específica de la Pediatría y que los problemas de su ámbito han de ser tratados por los pediatras especializados en ella (“Pediatría Social”) |
| Los Servicios Sociales son los encargados de valorar y tratar los problemas sociales (no pertenecen al ámbito de actuación de la Pediatría) (“Servicios Sociales”) |
Las respuestas (en escala Likert de 1 a 5) fueron cruzadas con las siguientes variables sociodemográficas:
- Edad del profesional: menores de 47 años y mayores de 47 años (media de edad en las respuestas).
- Nivel en el que se presta la atención: hospital o Atención Primaria (se excluyó para esta división las respuestas con labor asistencial en ambos niveles).
- Características de la población que se atiende: entorno urbano o rural (según los define el Instituto Nacional de Estadística5, usando el código postal del centro de trabajo).
Para el análisis presentado se utilizaron los programas estadísticos JASP y el software R v4.3.0. La comparación de las respuestas se obtuvo mediante el coeficiente de correlación de Pearson y el test U de Mann-Whitney. Las correlaciones entre las puntuaciones se calcularon mediante el coeficiente de correlación Tau-B de Kendall (Anexo 1).
RESULTADOS
Se obtuvieron 407 respuestas, el 90% (368) especialistas en Pediatría (resto: 26 MIR-Pediatría, 11 especialistas en Medicina de Familia y 2 MIR-Medicina de Familia). El 50% del total ejercían en las comunidades de Madrid, Andalucía o Cataluña, con menor representación del resto.
La principal limitación del estudio reside en que no se trata de una muestra aleatoria, sino que respondieron voluntariamente 407 profesionales, pese a que la gran difusión permitió que se distribuyera en prácticamente toda la población diana.
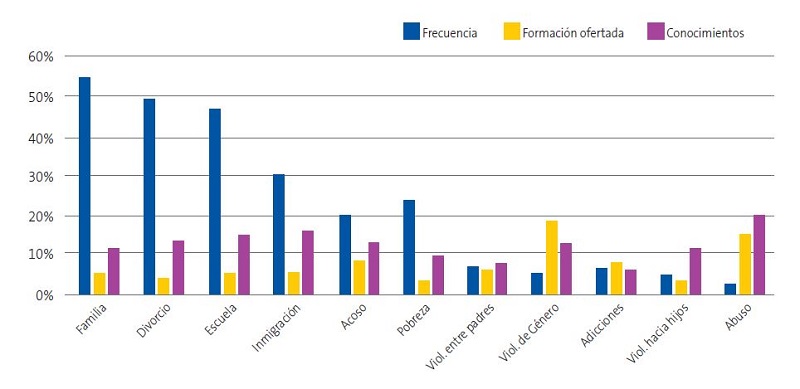
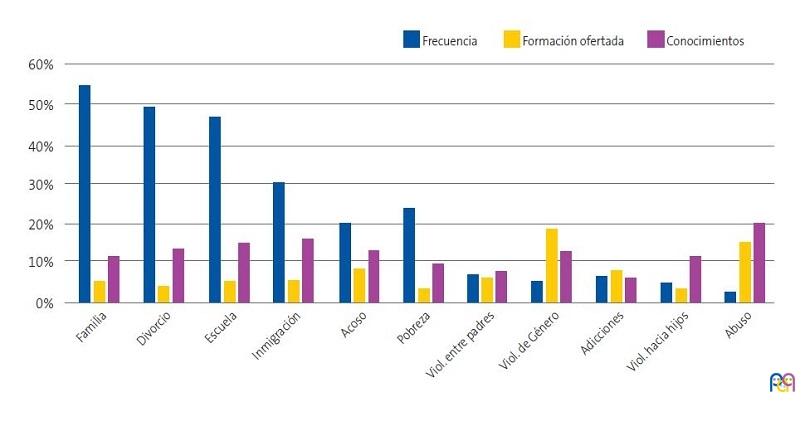
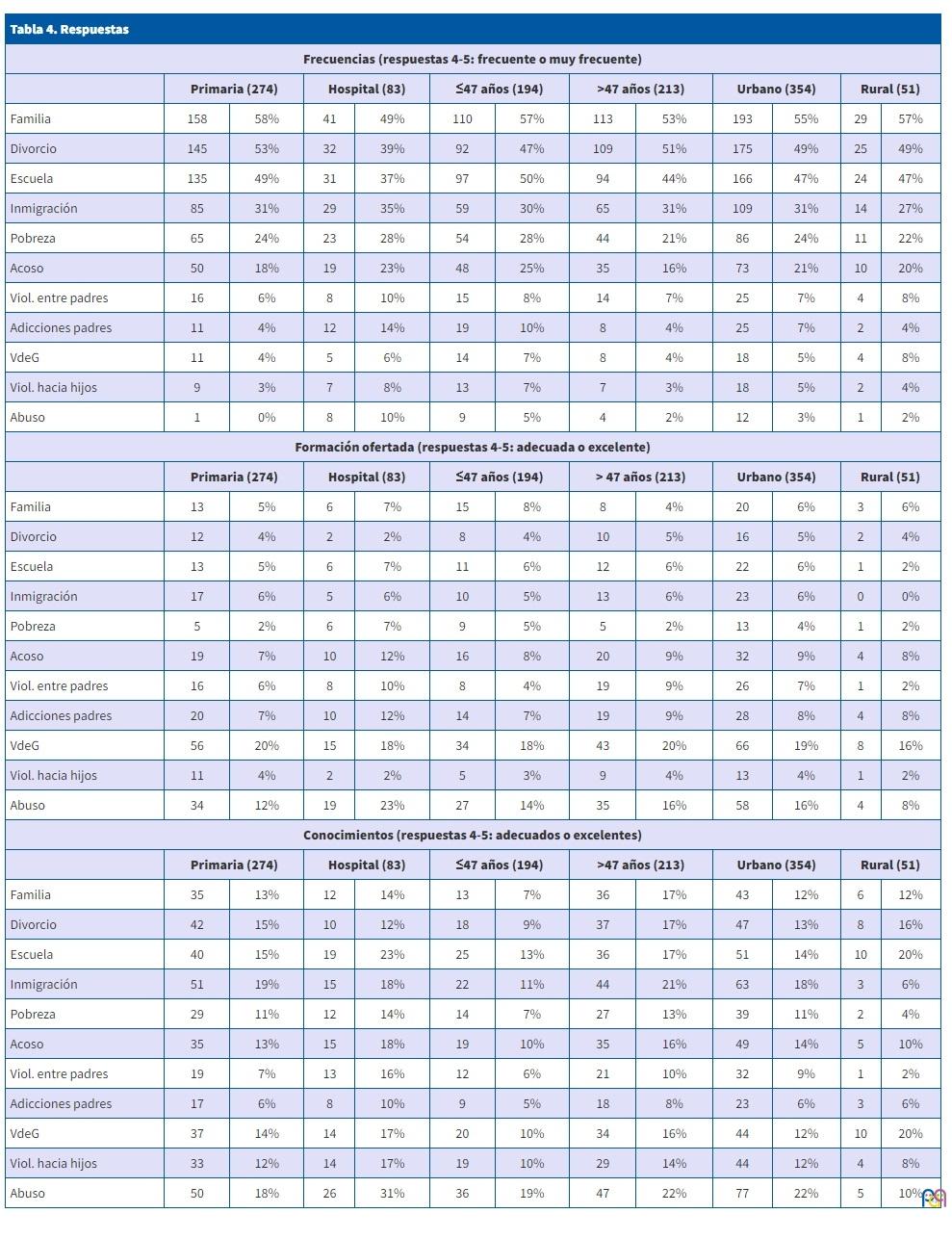
Respecto a la frecuencia de los problemas sociales, se señalan como frecuentes o muy frecuentes los problemas relacionados con el entorno familiar, separaciones conflictivas de los padres y con el entorno escolar (50-60%). Y lo contrario, los referidos a la violencia (contra los hijos o entre los padres, abuso, violencia de género) y adicciones de los progenitores: la gran mayoría los consideran poco o muy poco frecuentes (Figura 1 y Tabla 4).
| Figura 1. Problemas sociales (respuestas 4-5, en escala de 1 a 5) |
|---|
 |
| Tabla 4. Respuestas | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Frecuencias (respuestas 4-5: frecuente o muy frecuente) | ||||||||||||
| Primaria (274) | Hospital (83) | ≤47 años (194) | >47 años (213) | Urbano (354) | Rural (51) | |||||||
| Familia | 158 | 58% | 41 | 49% | 110 | 57% | 113 | 53% | 193 | 55% | 29 | 57% |
| Divorcio | 145 | 53% | 32 | 39% | 92 | 47% | 109 | 51% | 175 | 49% | 25 | 49% |
| Escuela | 135 | 49% | 31 | 37% | 97 | 50% | 94 | 44% | 166 | 47% | 24 | 47% |
| Inmigración | 85 | 31% | 29 | 35% | 59 | 30% | 65 | 31% | 109 | 31% | 14 | 27% |
| Pobreza | 65 | 24% | 23 | 28% | 54 | 28% | 44 | 21% | 86 | 24% | 11 | 22% |
| Acoso | 50 | 18% | 19 | 23% | 48 | 25% | 35 | 16% | 73 | 21% | 10 | 20% |
| Viol. entre padres | 16 | 6% | 8 | 10% | 15 | 8% | 14 | 7% | 25 | 7% | 4 | 8% |
| Adicciones padres | 11 | 4% | 12 | 14% | 19 | 10% | 8 | 4% | 25 | 7% | 2 | 4% |
| VdeG | 11 | 4% | 5 | 6% | 14 | 7% | 8 | 4% | 18 | 5% | 4 | 8% |
| Viol. hacia hijos | 9 | 3% | 7 | 8% | 13 | 7% | 7 | 3% | 18 | 5% | 2 | 4% |
| Abuso | 1 | 0% | 8 | 10% | 9 | 5% | 4 | 2% | 12 | 3% | 1 | 2% |
| Formación ofertada (respuestas 4-5: adecuada o excelente) | ||||||||||||
| Primaria (274) | Hospital (83) | ≤47 años (194) | > 47 años (213) | Urbano (354) | Rural (51) | |||||||
| Familia | 13 | 5% | 6 | 7% | 15 | 8% | 8 | 4% | 20 | 6% | 3 | 6% |
| Divorcio | 12 | 4% | 2 | 2% | 8 | 4% | 10 | 5% | 16 | 5% | 2 | 4% |
| Escuela | 13 | 5% | 6 | 7% | 11 | 6% | 12 | 6% | 22 | 6% | 1 | 2% |
| Inmigración | 17 | 6% | 5 | 6% | 10 | 5% | 13 | 6% | 23 | 6% | 0 | 0% |
| Pobreza | 5 | 2% | 6 | 7% | 9 | 5% | 5 | 2% | 13 | 4% | 1 | 2% |
| Acoso | 19 | 7% | 10 | 12% | 16 | 8% | 20 | 9% | 32 | 9% | 4 | 8% |
| Viol. entre padres | 16 | 6% | 8 | 10% | 8 | 4% | 19 | 9% | 26 | 7% | 1 | 2% |
| Adicciones padres | 20 | 7% | 10 | 12% | 14 | 7% | 19 | 9% | 28 | 8% | 4 | 8% |
| VdeG | 56 | 20% | 15 | 18% | 34 | 18% | 43 | 20% | 66 | 19% | 8 | 16% |
| Viol. hacia hijos | 11 | 4% | 2 | 2% | 5 | 3% | 9 | 4% | 13 | 4% | 1 | 2% |
| Abuso | 34 | 12% | 19 | 23% | 27 | 14% | 35 | 16% | 58 | 16% | 4 | 8% |
| Conocimientos (respuestas 4-5: adecuados o excelentes) | ||||||||||||
| Primaria (274) | Hospital (83) | ≤47 años (194) | >47 años (213) | Urbano (354) | Rural (51) | |||||||
| Familia | 35 | 13% | 12 | 14% | 13 | 7% | 36 | 17% | 43 | 12% | 6 | 12% |
| Divorcio | 42 | 15% | 10 | 12% | 18 | 9% | 37 | 17% | 47 | 13% | 8 | 16% |
| Escuela | 40 | 15% | 19 | 23% | 25 | 13% | 36 | 17% | 51 | 14% | 10 | 20% |
| Inmigración | 51 | 19% | 15 | 18% | 22 | 11% | 44 | 21% | 63 | 18% | 3 | 6% |
| Pobreza | 29 | 11% | 12 | 14% | 14 | 7% | 27 | 13% | 39 | 11% | 2 | 4% |
| Acoso | 35 | 13% | 15 | 18% | 19 | 10% | 35 | 16% | 49 | 14% | 5 | 10% |
| Viol. entre padres | 19 | 7% | 13 | 16% | 12 | 6% | 21 | 10% | 32 | 9% | 1 | 2% |
| Adicciones padres | 17 | 6% | 8 | 10% | 9 | 5% | 18 | 8% | 23 | 6% | 3 | 6% |
| VdeG | 37 | 14% | 14 | 17% | 20 | 10% | 34 | 16% | 44 | 12% | 10 | 20% |
| Viol. hacia hijos | 33 | 12% | 14 | 17% | 19 | 10% | 29 | 14% | 44 | 12% | 4 | 8% |
| Abuso | 50 | 18% | 26 | 31% | 36 | 19% | 47 | 22% | 77 | 22% | 5 | 10% |
Los problemas en relación con la inmigración y la pobreza se sitúan en frecuencias medias (la cuarta parte los señalan como frecuentes).
Esas diferencias se acentúan más según el ámbito de trabajo: los profesionales que ejercen en Atención Primaria perciben aún con mayor frecuencia los problemas familiares y escolares, y en muy pocas ocasiones atienden problemas en relación con la violencia, abuso y adicciones (5% o menos, frente al 10% en los de hospital). Ni la edad de los profesionales ni el entorno en el que trabajan (rural/urbano) implican diferencias en la detección.
El reducido tamaño muestral de cada grupo provoca que las diferencias obtenidas entre ellos resulten significativas en pocos casos. Pero analizando correlaciones entre las variables (Anexo 1), se aprecia que, en general, cuanto más frecuentes se detectan unos problemas, más frecuentemente se detectan también los demás. Lo que más fuertemente correlaciona es la inmigración y la pobreza. También las variables referidas a violencia tienen una correlación positiva entre ellas y con las adicciones de los progenitores. Y es positiva también la correlación entre los problemas del entorno familiar y separaciones conflictivas, con los del ámbito escolar. Así como los problemas de inmigración y pobreza, con los de adicciones de los padres y el entorno familiar.
Los resultados muestran la poca formación ofertada, especialmente en los problemas que más frecuentemente atendemos. En cualquiera de los grupos analizados. Únicamente en los problemas sobre violencia de género y sobre abuso, el 19% y el 15%, refieren que se les ha ofrecido una adecuada formación (prácticamente el doble que en los otros problemas). En el ámbito hospitalario se aprecian porcentajes mayores de formación sobre problemas sociales que en Primaria (exceptuando en violencia de género, que es mayor en Primaria).
La formación ofertada en cualquier tipo de violencia correlaciona con una mayor frecuencia de detección de las diferentes formas de violencia analizadas.
El entorno rural está escasamente representado (53 de 407), pero en todos los problemas estudiados los porcentajes de formación son menores que en el urbano, a pesar de que los porcentajes de frecuencia de presentación de los problemas sociales son prácticamente iguales en ambos entornos.
Solo el 10-20% de los encuestados refieren poseer los conocimientos adecuados en la mayoría de los problemas estudiados en todos los grupos (pese a la escasa formación ofertada y considerando la gran frecuencia de muchos de estos problemas). Esos porcentajes mayores en conocimientos que en formación ofertada implican que se están formando por vías distintas a la reglada en los programas formativos institucionales.
Existen diferencias significativas en conocimientos a favor de: el ámbito hospitalario (en las variables escuela, acoso, violencia entre padres, abuso), en los profesionales de más edad (familia, divorcio, pobreza), y en el entorno urbano (inmigración, violencia entre padres, abuso). Los profesionales de más edad consideran en general que tienen más conocimientos en todos los aspectos estudiados.
Se aprecia una correlación positiva entre la mayor formación ofertada en los problemas analizados y los conocimientos percibidos.
Aunque es preciso insistir en los pobres resultados en general de la formación y de los conocimientos en los problemas sociales, según las respuestas obtenidas.
Acorde a esos resultados, un 54% de los profesionales señalan como principal obstáculo, para su implicación (Figura 2) en estos problemas, la falta de formación en ellos, así como la falta de conocimientos de los recursos disponibles para su resolución o mejora (38%). En una cuarta parte de las respuestas recibidas, los profesionales refieren no sentirse cómodos indagando en estas cuestiones e incluso con miedo de no saber qué hacer con las respuestas que obtienen de los menores y sus familias. La falta de tiempo es también un obstáculo referido en el 28% de las respuestas.
| Figura 2. Implicación: motivos que impiden la implicación en problemas sociales (respuestas 4-5, en escala de 1 a 5) |
|---|
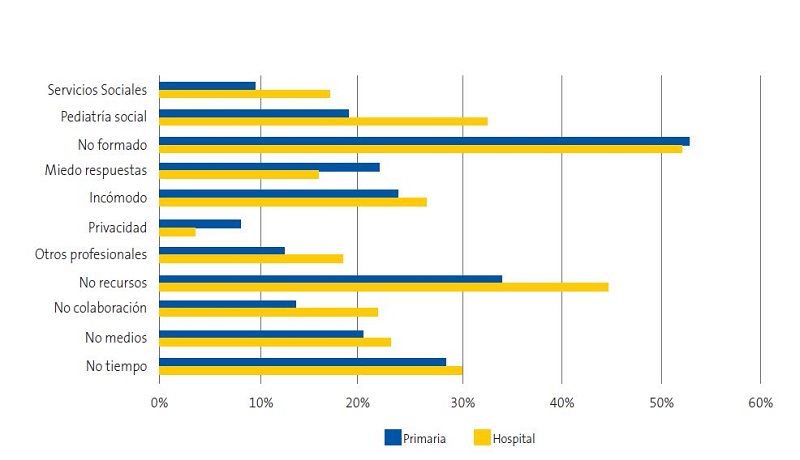 |
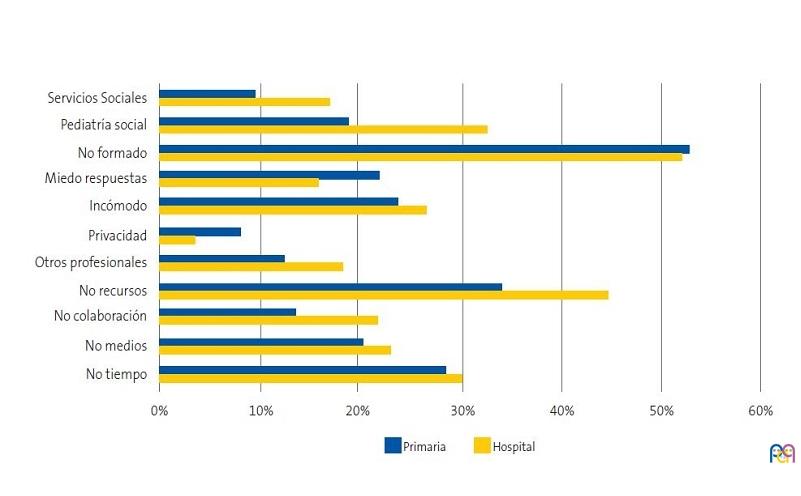
Solo el 11% del total consideran que estos problemas no pertenecen al ámbito de actuación de la Pediatría (frente al 71% que sí).
Se evidencia que, a mayor edad, mayor implicación (acorde también al aumento de conocimientos).
Respecto a la pregunta “Considero que la Pediatría social es una rama específica de la Pediatría y que los problemas de su ámbito han de ser tratados por los pediatras especializados en ella”, el 22% del total está de acuerdo con esa afirmación (52% en desacuerdo). Desglosando según el ámbito de trabajo, las diferencias se acentúan. Un 33% de los que trabajan en hospital responden que deben ser tratados por pediatras especializados en Pediatría social (otro 33% lo contrario). Sin embargo, solo el 19% de los que trabajan en Primaria están de acuerdo con ello (el 57% están en desacuerdo).
Los resultados globales del análisis correlacional muestran que, a mayor formación, mayores conocimientos. A mayor conocimiento, aumenta la frecuencia de detección y aumenta el grado de implicación (encontramos menos dificultades para abordar estos problemas).
DISCUSIÓN
La detección de los problemas sociales y su correcto abordaje se puede enseñar y se puede aprender.6-8 La definición de la Pediatría incluye a la Pediatría social como parte fundamental de la especialidad, así como el enfoque biopsicosocial de los problemas de la infancia y adolescencia9.
Tanto la Clasificación Internacional de Enfermedades de la OMS (CIE-11: https://icd.who.int/es) como la Clasificación Internacional de Atención Primaria de la WONCA (CEIP-2: www.who.int/standards/classifications/other-classifications/international-classification-of-primary-care) desarrollan los motivos de consulta con un enfoque biopsicosocial, ofreciendo la posibilidad de registrar de forma codificada los problemas sociales. Es preciso, por tanto, que se introduzcan como materias de estudio en la formación básica de los profesionales que atienden a los menores10-12.
Los resultados de este estudio muestran que hay algunos problemas sociales muy frecuentes, para los que se recibe poca formación y, por lo tanto, se abordan con escasos conocimientos y, en consecuencia, con temor a no hacerlo correctamente, pudiendo incluso hacer pensar que si no se está formado es que no son problema del pediatra.
Los más frecuentes no son los relacionados con la violencia hacia los menores (afortunadamente), sino con circunstancias del entorno, que les afectan a ellos junto a sus familias y su comunidad, haciendo que el problema del niño quede diluido en el contexto de problemas familiares o de la comunidad en la que vive (como puede ser el caso de inmigrantes o del pueblo gitano)13.
Son problemas que les provocan numerosos síntomas, malestar, sufrimiento y consecuencias en su desarrollo psicológico, emocional y relacional, así como menor rendimiento escolar y aumento de patologías a corto, medio y largo plazo. El pediatra, desde esa perspectiva global e integradora, debe conocer a fondo el entorno no solo familiar, sino social de sus niños, los factores locales que influyen en las inequidades o vulneran los derechos de los niños, la red de ayuda social y sus lagunas. Y conocer también la influencia positiva de la red de apoyo de que se disponga y que influirá en la evolución y en la calidad de vivencia de muchos problemas14, teniendo en cuenta que tanto los factores de riesgo como los factores protectores no tienen una relación directa causa-efecto, sino una asociación de probabilidad15.
De hecho, la intervención y la ayuda para superar esos problemas o minimizar sus consecuencias ayudaría muy probablemente también a detectar y disminuir los problemas en relación con la violencia y el abuso de los menores16,17.
En relación con las diferencias observadas entre la frecuencia de detección y la formación y conocimientos en el ámbito laboral (hospital/Atención Primaria), conviene recordar que, pese a que el 59% de las plazas de pediatría del Sistema Nacional de Salud corresponden a AP, la formación de los residentes es mayoritariamente hospitalaria, de manera que, cumpliendo el programa oficial de la especialidad, los residentes de Pediatría solo pasan el 6% de su periodo formativo en AP18,19.
Puede que el hecho de abordar problemas más graves (violencia) en el hospital influya en que la formación se centre más en ellos, cuando resultan mucho más frecuentes otro tipo de problemas. Es el caso del divorcio de los progenitores (uno de los más frecuentemente detectados según los datos presentados), que repercute intensamente en la vida de los hijos, con cambios en los cuidados habituales, descenso en el nivel económico, cambio de colegio, nuevas parejas de los progenitores que conllevan nuevos procesos de adaptación, etc., en nuestras consultas se pueden presentar como problemas de conducta, ansiedad, abdominalgia o cefalea, o bajo rendimiento escolar20.
Como en cualquier otra patología, el primer paso para abordar a estos pacientes pasa por elaborar una historia clínica completa21,22. La historia social debe formar parte de la historia clínica y ha de ser la herramienta fundamental para abordar los problemas de salud de forma integral y para activar los mecanismos de contención o mejora en caso de riesgo, o simplemente para entender e interpretar muchos signos o síntomas que pueden presentar los niños.
Se detecta así que los problemas sociales se mezclan y aumentan las consecuencias negativas. Un ejemplo evidente de ello es la pobreza que a menudo se añade a la inmigración, monoparentalidad, adicciones, violencia…23-25. La negligencia, entendida como una falta de acción que causa daño, es la forma de violencia más habitual y, sin embargo, es la menos percibida1. Es necesario visibilizarla más allá de lo material (con frecuencia es emocional y social), lo que requiere nuestra implicación en su búsqueda activa.
Los profesionales sanitarios tenemos la oportunidad y la obligación de tener en cuenta estos factores en la atención que prestamos, conociendo que con frecuencia “el acceso a la atención médica o social de calidad varía en proporción inversa a su necesidad en la población asistida” (Ley de Cuidados Inversos, Hart)26.
No admitiríamos que para ningún problema físico que ocurriese con tanta frecuencia en los menores que atendemos, tuviéramos tan poca formación y tan pocos conocimientos. Detectar la vulnerabilidad para proteger a las personas menores de edad debe ser una obligación imperiosa de la comunidad, pero especialmente de aquellas personas que trabajamos al servicio de los menores y sus familias27-29. Toda Pediatría es social, pues no puede (ni debe) haber otra forma de entender la Pediatría ni otra forma de mirar a la infancia. La falta de implicación (motivada en la mayoría por la falta de formación como expresan los resultados) nos hace formar parte del maltrato institucional a la infancia30.
Este estudio pone de manifiesto que la formación que reciben los profesionales médicos encargados de la atención a la infancia y los conocimientos que creen poseer respecto a los problemas sociales están lejos de corresponderse con lo necesario para una atención adecuada. Lo conveniente sería iniciar el aprendizaje desde el pregrado, pero lo que resulta imprescindible es que los pediatras reciban la formación adecuada durante la especialización para su correcto abordaje.
Y por ello creemos necesario:
- Considerar la violencia como un problema de salud (resultaría más fácil añadirlo en los programas de formación desde el inicio).
- Incrementar la formación sobre los Determinantes Sociales de Salud y las Experiencias Adversas en la Infancia.
- Formación en los profesionales que atienden a la infancia sobre el establecimiento de vínculos saludables con personas de referencia, adecuada interacción con el entorno y regulación de las emociones.
- Valorar la implantación de programas de visita domiciliaria para acercarnos a las realidades sociales de los menores que atendemos.
- Desarrollar programas de coordinación efectiva y eficaz entre Atención Primaria y hospitalaria, con Enfermería (incluyendo matronas), con médicos de familia (los niños no viven solos), y con otros servicios comunitarios especializados: Servicios Sociales, Salud Mental, Educación y, en caso necesario, con Fuerzas y Cuerpos de Seguridad del Estado y Sistema Judicial.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del manuscrito publicado.
INFORMACIÓN COMPLEMENTARIA
Anexo 1. Consultar en este enlace.
BIBLIOGRAFÍA
- Romeo Biedma FJ, Horno Goicoechea P. Ver para proteger. Claves para comprender la violencia contra niños, niñas y adolescentes y para desarrollar medidas de protección eficaces. UNICEF España; Dirección de sensibilización y políticas de infancia. Área de incidencia política y estudios. 2022 [en línea] [consultado el 09/08/2023]. Disponible en www.observatoriodelainfancia.es/oia/esp/descargar.aspx?id=7872&tipo=documento
- Jiménez Alés R, Páez González R, De la Torre Quiralte MLL, Poch Olivé ML, Boukichou Abdelkader N, Andrés Esteban EM. Creación y validación de un instrumento para cuantificar actitudes, conocimientos y dificultades en el abordaje de los problemas sociales. An Pediatr (Barc) 2023;98(6):418-26. https://doi.org/10.1016/j.anpedi.2022.12.010
- Ministerio de Sanidad. Portal Estadístico. Área de Inteligencia de Gestión. Sistema de Información de Atención Primaria (SIAP). Número de profesionales. Pediatría [en línea] [consultado el 09/08/2023]. Disponible en: https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/S/sistema-de-informacion-de-atencion-primaria-siap
- Ministerio de Sanidad. Portal Estadístico. Área de Inteligencia de Gestión. Sistema de Información de Atención Especializada (SIAE). Número de profesionales. Pediatría [en línea] [consultado el 09/08/2023]. Disponible en https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/S/siae
- Ministerio de Transportes, Movilidad y Agenda Urbana, 2021. Áreas Urbanas en España 2021. Madrid: Ministerio de Transportes, Movilidad y Agenda Urbana, 21-39 [en línea] [consultado el 09/08/2023]. Disponible en https://cvp.mitma.gob.es/downloadcustom/sample/3152
- Hardcastle K, Bellis MA. Asking about adverse childhood experiences (ACEs) in general practice: evaluation findings from a pilot study in Anglesey. North Wales, Cardiff: Public Health Wales, 2019 [en línea] [consultado el 09/08/2023]. Disponible en www.researchgate.net/publication/332222562_Asking_about_adverse_childhood_experiences_ACEs_in_General_Practice_Evaluation_findings_from_a_pilot_study_in_Anglesey_North_Wales
- Szilagyi M, Kerker BD, Storfer-Isser A, Stein RE, Garner A, O'Connor KG, et al. Factors Associated With Whether Pediatricians Inquire About Parents' Adverse Childhood Experiences. Acad Pediatr. 2016;16:668-75. https://doi.org/10.1016/j.acap.2016.04.013
- Thang C, Kucaj S, Forkey H, Lopez N, Ocampo A, Inkelas M, et al. Training Pediatric Interns to be Trauma-Responsive Providers by Adapting a National Evidence-Informed Curriculum for Pediatricians. Acad Pediatr. 2023;23:219-21. https://doi.org/10.1016/j.acap.2022.02.020
- Programa oficial de la especialidad de Pediatría y sus Áreas específicas [en línea] [consultado el 09/08/2023]. Disponible en: www.boe.es/eli/es/o/2006/09/20/sco3148
- Martínez González C. Ser pediatra en tiempos de pandemia. Form Act Pediatr Aten Prim. 2022;15(1):1-3.
- Kerker BD, Storfer-Isser A, Szilagyi M, Stein RE, Garner AS, O'Connor KG, et al. Do Pediatricians Ask About Adverse Childhood Experiences in Pediatric Primary Care? Acad Pediatr. 2016;16:154-60. https://doi.org/10.1016/j.acap.2015.08.002
- Hardcastle K, Bellis MA, Sharp CA, Hughes K. Exploring the health and service utilisation of general practice patients with a history of adverse childhood experiences (ACEs): an observational study using electronic health records. BMJ Open. 2020;25:10. https://doi.org/10.1136/bmjopen-2019-036239
- Estrategia Nacional para la Igualdad, Inclusión y Participación del Pueblo Gitano 2021-2030. Ministerio de Derechos Sociales y Agenda 2030. Gobierno de España [en línea] [consultado el 09/08/2023]. Disponible en www.mdsocialesa2030.gob.es/derechos-sociales/poblacion-gitana/estrategia-nacional/futura-estrategia.htm
- Sánchez Vázquez AR. Apego y experiencias adversas en la infancia. En: Problemas psicosociales en Pediatría. Continuum 2021 [en línea] [consultado el 09/08/2023]. Disponible en https://continuum.aeped.es/modules/listado/1027
- Martínez Bernat l, Villar Villar G. Recién nacido con riesgo social. Pediatr Integral 2019;XXIII(3):154-160.
- Pinto Rubio M, Zabaleta Rueda A, Gorrotxategi Gorrotxategi P. Las experiencias adversas en la infancia. Detección precoz y prevención de sus consecuencias. Form Act Pediatr Aten Prim. 2023;16:49-53.
- Conn AM, Szilagyi MA, Jee SH, Manly JT, Briggs R, Szilagyi PG. Parental perspectives of screening for adverse childhood experiences in pediatric primary care. Fam Syst Health. 2018;36:62-72. https://doi.org/10.1037/fsh0000311
- Fernández-Cuesta Valcarce M.A., Villaizán Pérez C. Incremento de la rotación del residente de pediatría por el centro de salud, ¿una opción para mitigar la crisis de la pediatría de atención primaria? An Pediatr (Barc) 2022;97:77-8. https://doi.org/10.1016/j.anpedi.2022.06.018
- Green C, Stein REK, Storfer-Isser A, Garner AS, Kerker BD, Szilagyi M, et al. Do Subspecialists Ask About and Refer Families with Psychosocial Concerns? A Comparison with General Pediatricians. Matern Child Health J. 2019;23:61-71. https://doi.org/10.1007/s10995-018-2594-y
- Mardomingo MJ, Seijo. Psicopatología de los hijos en los procesos de ruptura de pareja. En: Fariña Rivera F, Ortuño Muñoz P (eds.). La gestión positiva de la ruptura de pareja con hijos. Valencia: Tirant lo Blanch; 2020.
- Pérez Candás JI, Grupo de Pediatría Social y Comunitaria AEPap. Programa de identificación del riesgo psicosocial en la infancia y la adolescencia (II). Form Act Pediatr Aten Prim. 2022;15:153-60.
- Gancedo Baranda A (ed.). Manual para la atención a situaciones de Maltrato Infantil. Madrid: Editorial Grupo 2 Comunicación Médica; 2021 [en línea] [consultado el 09/08/2023]. Disponible en https://seup.org/pdf_public/gt/Maltrato_infantil.pdf
- UNICEF. Diagnóstico de la situación de la infancia en España antes de la aplicación de la Garantía Infantil Europea, Oficina Regional de UNICEF para Europa y Asia Central, Ginebra, 2021. [consultado el 09/08/2023]. Disponible en www.unicef.org/eca/sites/unicef.org.eca/files/2021-11/Spanish Deep Dive Literature review ES.pdf
- Llano JC. El estado de la pobreza. 12.º Informe AROPE. Seguimiento de los indicadores de la Agenda UE 2030 (2015-2022). Madrid, Red Europea de Lucha contra la Pobreza y la Exclusión Social, 2022, 257 [en línea] [consultado el 09/08/2023]. Disponible en www.eapn.es/estadodepobreza/
- Singh G, Zhu H, Cheung CR. Public health for paediatricians: Fifteen-minute consultation on addressing child poverty in clinical practice Arch Dis Child Educ Pract Ed 2021;106:326-32. https://doi.org/10.1136/archdischild-2020-319636
- Hart JT. The inverse care law. Lancet. 1971; 27:405-12. https://doi.org/10.1016/S0140-6736(71)92410-X
- Páez González R, Martínez González C. Frikípatas. Rev Pediatr Aten Primaria. 2023;25:e47-e48.
- Beck AF, Klein MD. Moving From Social Risk Assessment and Identification to Intervention and Treatment. Acad Pediatr. 2016;16(2):97-8. https://doi.org/10.1016/j.acap.2016.01.001
- Pérez Candás, JI. Programa de identificación del riesgo psicosocial en la infancia y la adolescencia (I). Form Act Pediatr Aten Prim. 2022;15(3):111-8.
- Salamanca García l. El maltrato institucional a los-as niños-as. Una aproximación desde la praxis socioeducativa con niños-as en desventaja. Revista de Educación Social 2018;27:176-202.