

Vol. 25 - Num. 100
Originales
La promoción de la lectura y su relación con las vocaciones y entornos profesionales
Ana Garach Gómeza, Iván Gutiérrez Garcíab, Antonio Molina Carballoc, Jesús L. Megíasd
aPediatra. CS Zaidín Sur. Granada. España.
bPediatra. Hospital Universitario Nuestra Señora de la Candelaria. Santa Cruz de Tenerife. España
cPediatra. Departamento de Pediatría. Facultad de Medicina. Universidad de Granada. Granada. España.
dPsicólogo. Departamento de Psicología Experimental. Facultad de Psicología. Universidad de Granada. Granada. España.
Correspondencia: A Garach. Correo electrónico: anagarach@hotmail.com
Cómo citar este artículo: Garach Gómez A, Gutiérrez García I, Molina Carballo A, Megías JL. La promoción de la lectura y su relación con las vocaciones y entornos profesionales . Rev Pediatr Aten Primaria. 2023;25:377-87. https://doi.org/10.60147/76a271c6
Publicado en Internet: 21-11-2023 - Número de visitas: 2876
Resumen
Introducción: la promoción de hábitos de vida saludables es una práctica habitual entre los pediatras. Dentro de estos se encuentra la promoción de la lectura, que entraña numerosos beneficios para la infancia: estimula la actividad cerebral y su reserva cognitiva, aumenta la concentración y el desarrollo del lenguaje y permite trabajar las emociones.
El objetivo de este estudio es conocer la realidad de la práctica de la promoción de la lectura desde las consultas de Pediatría, así como su relación con la vocación pediátrica (clínica, preventiva y social) y los entornos profesionales (residencia, hospital y Atención Primaria).
Material y métodos: estudio transversal, descriptivo de ámbito nacional, mediante encuesta en línea a residentes de Pediatría, pediatras hospitalarios/as y de Atención Primaria llevado a cabo en marzo de 2022.
Resultados: participaron 326 pediatras, un 16,8% hospitalarios/as, un 69,8% de Atención Primaria y 13,4% residentes de Pediatría. El 18,8% seleccionaron la vocación preventiva, el 60,8%, la clínica y el 20,5%, la social. Junto con una descripción detallada del tipo de actividades de promoción de la lectura que se realizan en nuestro país, los resultados mostraron, en primer lugar, que la vocación médica se relacionó con su mayor o menor realización (χ2(2) = 13,11, p <0,001), siendo los pediatras con vocación social los que informaron llevarlas a cabo en un mayor porcentaje. En segundo lugar, también el ámbito de trabajo apareció como un condicionante para la realización de estas actividades (χ2(2) = 19,0, p <0,001), que se llevan a cabo más frecuentemente en las consultas de Atención Primaria.
Conclusiones: las actividades de promoción de la lectura son realizadas mayormente por los profesionales de Atención Primaria, en el marco de otras actividades de promoción de la salud, vinculadas principalmente con su mayor vocación por la Pediatría social.
Palabras clave
● Desarrollo infantil ● Promoción de la lectura ● Promoción de la salud ● Vocación médicaINTRODUCCIÓN
Aunque existen diferentes definiciones de la especialidad de Pediatría, la orden ministerial que aprobó en España su programa formativo (BOE-A-2006-17999) la conceptualizó como la “medicina integral del periodo evolutivo de la existencia humana desde la concepción hasta el final de la adolescencia”.
Las funciones de la Pediatría son muy amplias y diversas, ya que incluyen todo aquello que concierne a:
- Los cuidados de la infancia y adolescencia sanas (Pediatría preventiva).
- Los modos de asistencia médica integral, total y continuada en niños, niñas y adolescentes en estado de enfermedad (Pediatría clínica).
- Las interrelaciones individuales y con la comunidad de la infancia y adolescencia sanas y enfermas en el medio físico y humano en el que de manera ininterrumpida y con características propias se desarrolla (Pediatría social)1.
El ejercicio de la Pediatría puede llevarse a cabo en medio hospitalario o extrahospitalario, dependiendo de la subespecialidad pediátrica. De las 17 subespecialidades reconocidas en el Libro Blanco de las Especialidades Pediátricas promovido por la Asociación Española de Pediatría2, la mayoría de ellas se desarrollan en medio hospitalario, siendo la Pediatría de Atención Primaria la que realiza su ejercicio asistencial en los centros de salud. Según los datos del Ministerio de Sanidad de 2021, España cuenta con algo más de 4750 pediatras trabajando en hospitales, más de 1800 desarrollando su formación como médicos internos residentes3 y unos 6600 desempeñando su profesión en medio extrahospitalario4.
La elección de la subespecialidad y el área de trabajo en el que desempeña su ejercicio el profesional de la Pediatría depende en gran medida de sus intereses vocacionales. La vocación médica puede definirse de varias formas, pero tal vez alcance un amplio consenso la que propone que es una motivación profunda de servicio al paciente y a la sociedad que está determinada por las vivencias y el entorno5. Según las distintas funciones de la Pediatría, podemos distinguir entre pediatras que sienten más su vocación como preventivos, otros como clínicos y otros como sociales. Aunque todas las subespecialidades pediátricas comparten lo concerniente al estado de enfermedad de la infancia, desde la Pediatría realizada en la Atención Primaria de salud se destaca la importancia de las medidas preventivas y un abordaje de la infancia desde un punto de vista biopsicosocial. Sus principales objetivos son: por un lado, proporcionar una atención médica y cuidados continuos, integrales, centrados en el niño/a y la familia, que han se ser coordinados y llevados a cabo en el medio en el que el niño/a crece y se desarrolla, desde el nacimiento hasta la finalización del crecimiento somático y el desarrollo psicosocial; y por otro, prestar una atención individualizada, considerando el contexto social y comunitario con un enfoque poblacional, no solo de grupos de riesgo6.
Por tanto, la Pediatría de Atención Primaria tiene como una de sus señas de identidad llevar a cabo la promoción de hábitos saludables. Los consejos proporcionados en esta dirección deben ser adaptados a la edad del niño/a, comunicados desde la primera visita, realizándose en gran medida en los programas de salud infantil. En ese sentido, la posición del pediatra de Atención Primaria con respecto al niño/a y su familia es privilegiada, ya que nos permite hacer un seguimiento longitudinal del crecimiento y desarrollo de este, desde que nace hasta que alcanza los 14 años. La Pediatría abarca todo el neurodesarrollo, por lo que incluso sería aconsejable no finalizar la edad pediátrica a los 14, sino a los 18 años, o incluso posteriormente, como ocurre en otros países. Los hábitos que promueven la salud pueden proporcionar un impacto muy favorable sobre el correcto desarrollo del niño/a, sobre su salud global, entendida esta desde un punto de vista biopsicosocial7.
Dentro de los consejos ofrecidos en las visitas de salud infantil, hay uno, la promoción de la lectura, que cada vez cobra más importancia, al haberse demostrado el impacto positivo que ocasiona8. Los beneficios de la lectura en voz alta durante los primeros años de vida son numerosos. Por ello, se incluye dentro de las actividades que los/as pediatras podemos promover desde los primeros controles de salud infantil. Entre estos beneficios podemos destacar los siguientes9:
- La lectura en voz alta estimula la actividad de las áreas cerebrales que tienen que ver con la comprensión narrativa y la creación de imágenes mentales, lo que repercute en el aprendizaje de la lengua oral y escrita.
- Influye en el desarrollo cognitivo del niño/a, al poder escuchar, pensar, sentir, preguntar, responder, asociar…
- Posee un impacto significativo en el desarrollo del lenguaje, aumentando su capacidad lingüística al escuchar palabras nuevas y expresiones más complejas que las que oye a diario.
- Facilita la relación con el lenguaje de los libros, más complejo que el lenguaje hablado.
- Permite trabajar el mundo de las emociones: establece momentos de intimidad entre quienes leen y escuchan, crea y refuerza vínculos afectivos y ayuda a expresar y compartir emociones.
Siendo tan relevantes y comprobados los beneficios de la promoción de la lectura desde las consultas de Pediatría, se torna necesario conocer cuál es la realidad de esta práctica en nuestro contexto, así como algunos de los factores que podrían estar influyendo en su mayor o menor implantación. Para ello, los objetivos del presente estudio son conocer, en primer lugar, los ámbitos de trabajo de los/as pediatras en nuestro país y su vinculación con sus vocaciones de origen en el ejercicio de la profesión; y, en segundo lugar, identificar cuántas de las actividades que realizan se encuadran dentro de un marco preventivo, en el que se insertan las de promoción de la lectura, sus modalidades y dificultades para implantarlas.
MATERIAL Y MÉTODOS
Participantes: participaron un total de 326 pediatras (273 mujeres y 53 hombres), con una edad media ± desviación estándar (DS), de 47 ± 12,77 años (mujeres: 46,8 ± 12,1; hombres: 51 ± 15,1). De ellos, 54 (16,8%) ejercían la Pediatría en medio hospitalario, 224 (69,8%) en Atención Primaria y 43 (13,4%) se encontraban en su periodo de residencia. Todos los participantes firmaron un consentimiento informado para participar en la encuesta y se accedió a ellos mediante envíos masivos por listas de distribución de grupos de pediatras. El proyecto fue aprobado por el Comité de Ética de la Universidad de Granada.
Diseño del estudio: estudio transversal, descriptivo y de ámbito nacional, llevado a cabo mediante encuesta en línea durante el mes de marzo de 2022. Como criterio de inclusión se determinó que los participantes se encontraran trabajando en activo en el momento de realizarla. La encuesta fue implementada mediante la plataforma Qualtrics Version XM (2020).
Variables: las variables recogidas se detallan a continuación.
- Referidas a los propios participantes: edad, sexo, número de hijos/as, ámbito donde desarrollan la mayor parte de la actividad profesional (Atención Primaria, hospitalaria o residencia), presión asistencial percibida en su trabajo (valorada en una escala del 1 al 5, siendo 1 muy poca presión asistencial y 5 mucha presión asistencial) y años de ejercicio profesional como pediatras.
- Respecto a la población atendida, se pidió a los participantes que estimaran el nivel socioeconómico y educativo (NSE) de la población a la que atendían, mediante la escala de Clase Social Subjetiva de MacArthur desarrollada por Adler et al. (2000) en su versión para adultos10. Esta escala es el instrumento estándar para realizar una valoración del estatus social subjetivo. En esta medida se le presenta al participante una figura de una escalera que contiene 10 peldaños que se corresponden con diferentes posiciones en clase social, yendo desde 1 (escalón más bajo, posición más baja en la clase social) a 10 (escalón más alto, posición más alta en la clase social). Se les pedía que escogiesen el peldaño que mejor representase a su población atendida, haciendo una estimación subjetiva que considerase ingresos, educación y estatus laboral.
- El Programa Oficial de la Especialidad de Pediatría y sus Áreas Específicas describe como ámbitos de actuación de la Pediatría la función de cuidados del niño/a y adolescente sano (Pediatría preventiva), la asistencia médica integral total y continuada del niño/a y adolescente en estado de enfermedad (Pediatría clínica) y las relaciones del niño/a y adolescente sano y enfermo con su entorno (Pediatría social)1. En relación con ello, preguntamos a los encuestados cuál de estas funciones era la que representaba mejor su vocación principal en el ejercicio de la profesión.
- Por último, se pidió que estimasen el tiempo que invierten en actuaciones de promoción de la salud. Además, se les preguntó acerca de la realización de actividades de promoción de la lectura, su frecuencia y tipo llevadas a cabo, en el caso de realizarse.
Análisis estadísticos: el análisis descriptivo de las variables cualitativas se concreta mediante el cálculo de las distintas medidas de tendencia central y frecuencias relativas. Para las comparaciones de datos referidos a los propios participantes se realizaron ANOVA unifactoriales, para las comparaciones pareadas post hoc (pruebas de Tukey) y el test χ2 para los contrastes de porcentajes. Se consideran significativos los resultados con valor p inferior a 0,05. El análisis de los datos se realiza mediante el programa estadístico Jamovi, versión 2.3.21.
RESULTADOS
En la Tabla 1 se presentan algunos datos básicos de los participantes (edad, número de hijos/as, presión asistencial percibida y estimación del NSE de la población atendida), en función del ámbito donde llevan a cabo su ejercicio profesional (hospital o Atención Primaria), dejando un grupo propio para quienes se encuentran en su periodo de residencia. Como puede verse, tal como era esperable, la edad de los pediatras residentes fue significativamente menor que la de quienes ejercían la Pediatría en hospital y Atención Primaria, y la de estos últimos, mayor que la de los pediatras de hospital. En relación con el número de hijos/as, no hubo diferencias entre los pediatras de hospital y Atención Primaria. Respecto a la presión asistencial percibida, el grupo de pediatras residentes es el que señala sufrirla en mayor medida. En relación con el NSE estimado para los pacientes atendidos, no se observan diferencias significativas en función del ámbito laboral.
| Tabla 1. Características de la muestra según ámbito de trabajo (media ± DS) | |||||
|---|---|---|---|---|---|
| Hospital (n = 54) | Atención Primaria (n = 224) | Residentes (n = 43) | Estadístico Fs (gl = 2) | p valor | |
| Edad | 43,3a ± 9,7 | 51,6b ± 9,9 | 28,1c ± 2,6 | 481 | p <0,001 |
| N.º de hijos | 1,9a ± 1,1 | 1,9a ± 1,1 | 0,1b ± 0,4 | 212 | p <0,001 |
| Presión asistencial | 3,7a ± 0,9 | 3,6a ± 0,9 | 4b ± 0,6 | 5,5 | p <0,05 |
| NSE población atendida | 5,1 ± 1,50 | 5,3 ± 1,79 | 5,1 ± 1,38 | 0,62 | p = 0,54 |
| Nota: letras diferentes indican diferencias estadísticamente significativas en cada fila en las comparaciones post hoc (prueba de Tukey) dos a dos. Ausencia de letras indica que un valor no es estadísticamente diferente de ninguno de los demás de su fila.
DS: desviación estándar; NSE: nivel socioeconómico y educativo. |
|||||
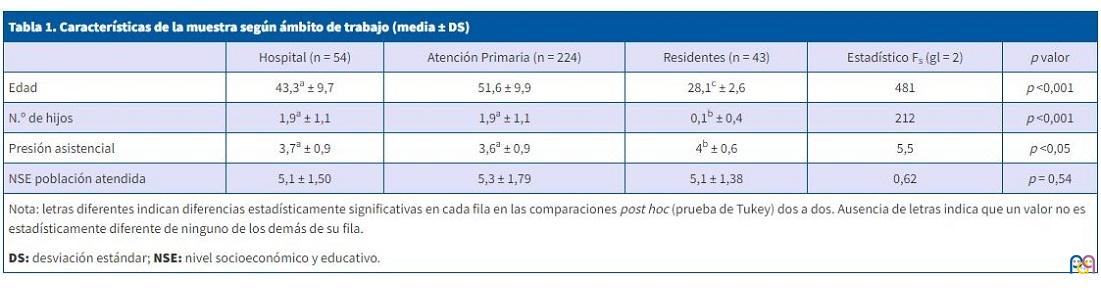
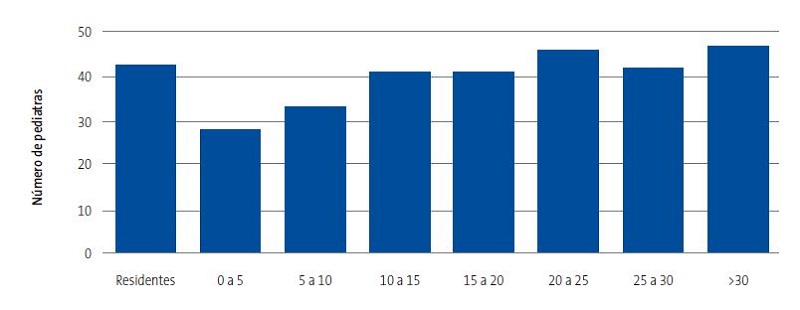
La Figura 1 muestra la distribución de los participantes según los años de ejercicio profesional. La primera barra corresponde a los residentes y en el resto de barras se representan agrupados los pediatras tanto de Atención Primaria como de hospital.
| Figura 1. Años de ejercicio profesional como pediatras |
|---|
 |
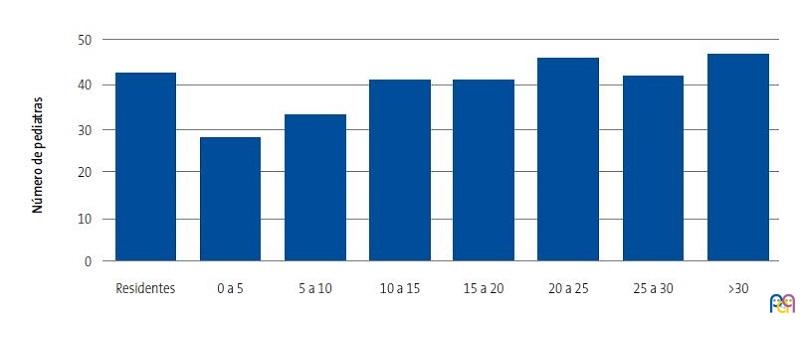
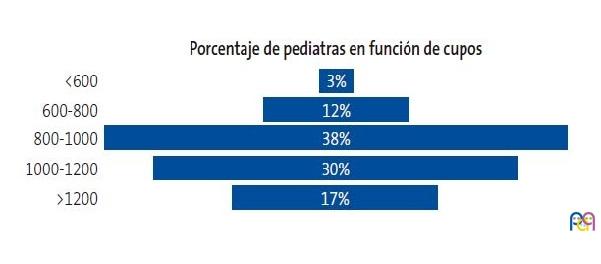
Respecto a los cupos de los pediatras de Atención Primaria, estos fueron muy variables entre los participantes en el estudio. Observamos en la Figura 2 que el cupo de 800-1000 niños/as es el más frecuente entre ellos (un 38%), seguido de los cupos de 1000 a 1200 niños/as (30%) y de los que tienen más de 1200 niños/as a su cargo (17%).
| Figura 2. Cupos de los pediatras de Atención Primaria |
|---|
 |
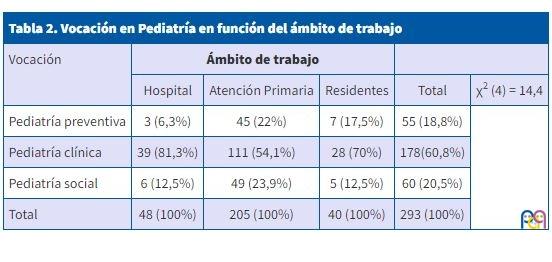
Respecto a las vocaciones informadas por los participantes (preventiva, clínica y social), la Tabla 2 recoge la distribución de las mismas, según el ámbito de trabajo. Como puede observarse, la vocación clínica es la mayoritaria en todos los ámbitos, aunque destaca sobre todo entre los pediatras hospitalarios y los residentes. Por otra parte, las vocaciones de Pediatría social y preventiva son escogidas significativamente más por los pediatras de Atención Primaria que por los demás.
| Tabla 2. Vocación en Pediatría en función del ámbito de trabajo | |||||
|---|---|---|---|---|---|
| Vocación | Ámbito de trabajo | ||||
| Hospital | Atención Primaria | Residentes | Total | χ2 (4) = 14,4 | |
| Pediatría preventiva | 3 (6,3%) | 45 (22%) | 7 (17,5%) | 55 (18,8%) | |
| Pediatría clínica | 39 (81,3%) | 111 (54,1%) | 28 (70%) | 178(60,8%) | |
| Pediatría social | 6 (12,5%) | 49 (23,9%) | 5 (12,5%) | 60 (20,5%) | |
| Total | 48 (100%) | 205 (100%) | 40 (100%) | 293 (100%) | |
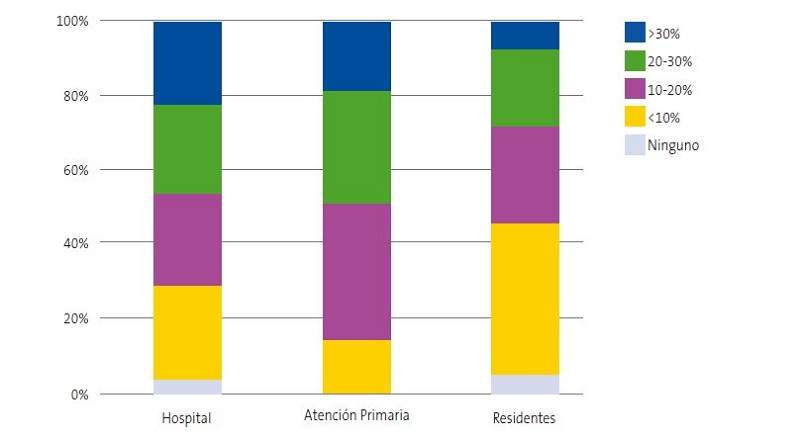
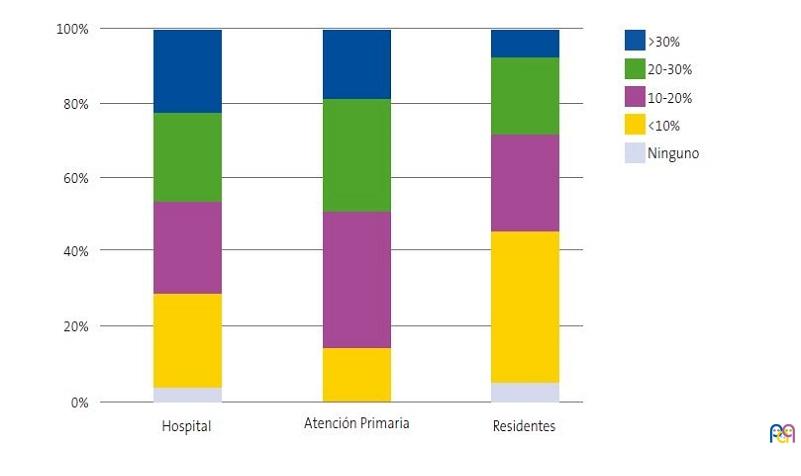
En la Figura 3 se muestra el tiempo dedicado por los distintos profesionales a actividades de promoción de la salud, encontrándose diferencias entre los distintos ámbitos de trabajo, χ2(8) = 26,1, p <0,001. La mayoría de los pediatras responden que realizan actividades de promoción de la salud, pero son los que trabajan en Atención Primaria los que más tiempo dedican a las mismas, especialmente en comparación con lo dedicado por los residentes.
| Figura 3. Tiempo dedicado a actividades de promoción de la salud |
|---|
 |
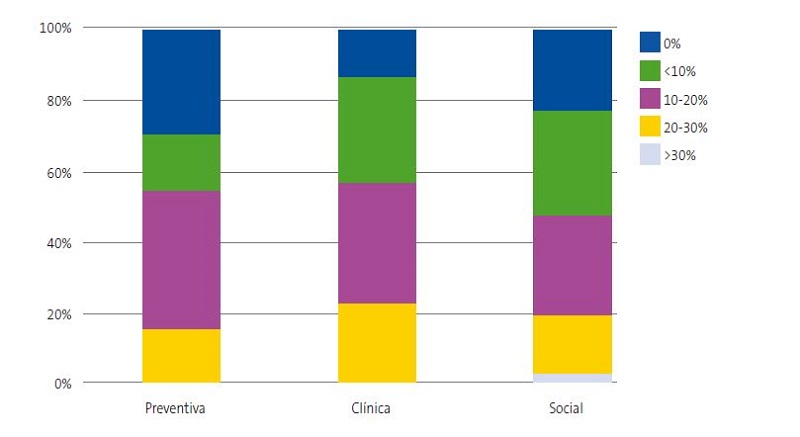
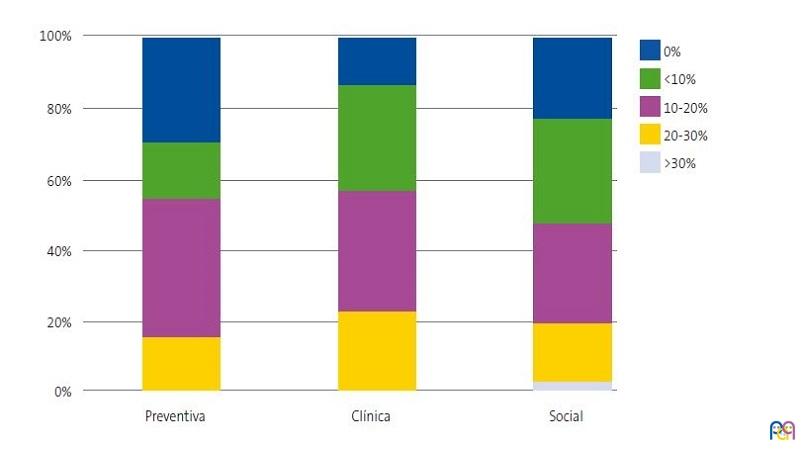
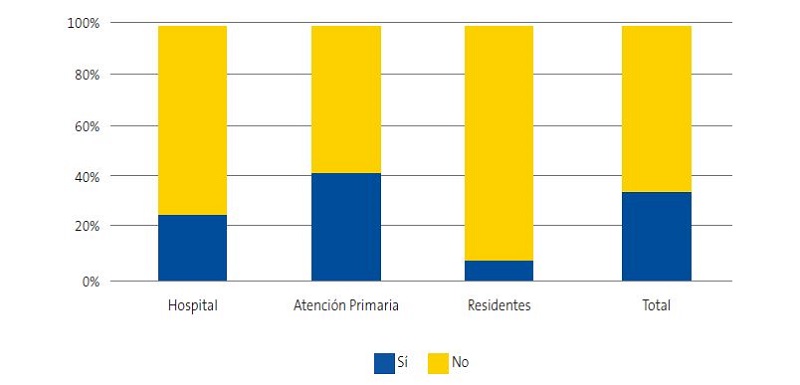
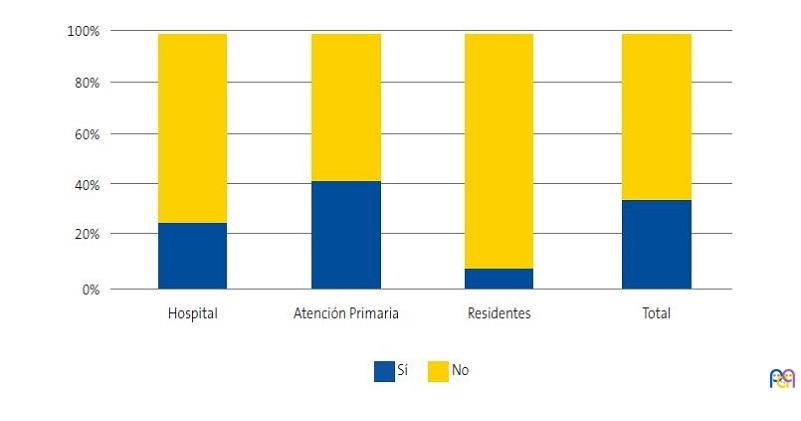
La vocación médica también influye en la mayor o menor realización de actividades de promoción de la salud, tal como se muestra en la Figura 4, siendo los pediatras que tienen vocación preventiva los que más tiempo dedican a la misma; sin embargo, esta diferencia no alcanzó la significación estadística (χ2(8) = 13,8, p <0,09). Con respecto a las actividades de promoción de la lectura, una forma concreta de promoción de la salud, también se encontraron diferencias significativas en función del lugar de trabajo, χ2(2) = 19,0, p <0,001, siendo los pediatras de Atención Primaria quienes más informaron realizarlas (41,7% frente al 25% de los hospitalarios y 7,7% de los residentes) (Figura 5).
| Figura 4. Realización de actividades de promoción de la salud según vocación |
|---|
 |
| Figura 5. Realización de actividades de promoción de la lectura según lugar de trabajo y en el total de la muestra |
|---|
 |
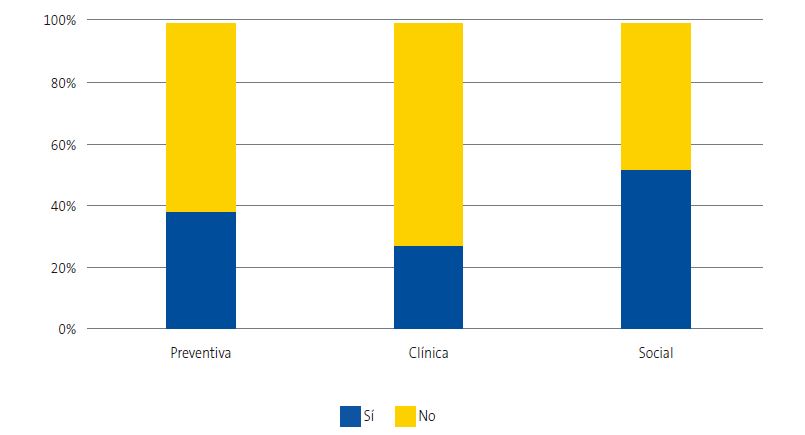
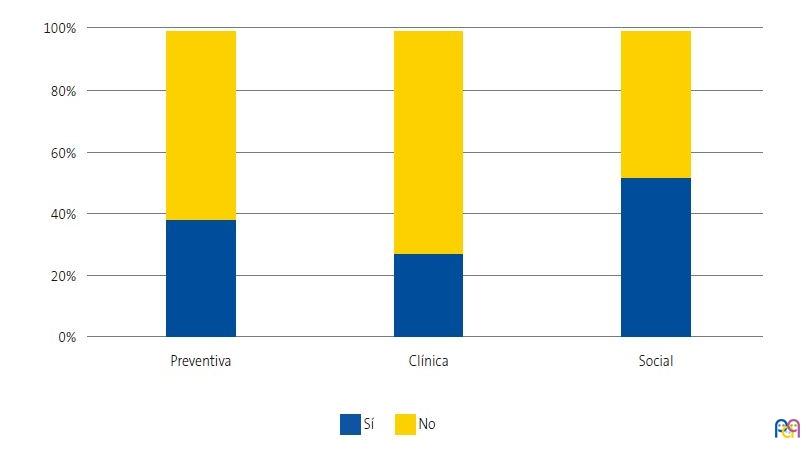
Para comprobar si existe algún tipo de relación entre la vocación informada y la realización de actividades de promoción de la lectura, realizamos un nuevo análisis que puso de manifiesto que entre quienes presentan vocación social se encuentra el porcentaje mayor de profesionales que lleva a cabo este tipo de actividades (52,7% frente a 38,2% entre los que informan vocación preventiva y 27,3% entre los que muestran vocación clínica), (χ2(2) = 13,11, p <0,001) (Figura 6).
| Figura 6. Realización de actividades de promoción de la lectura según vocación |
|---|
 |
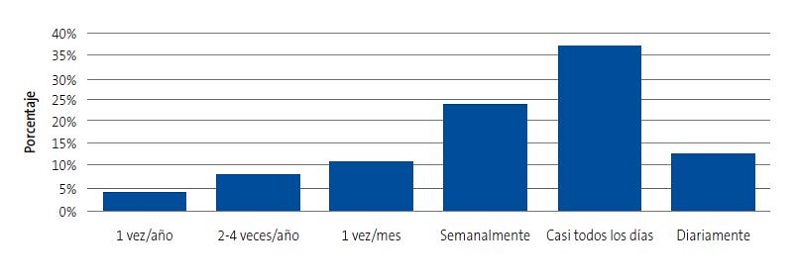
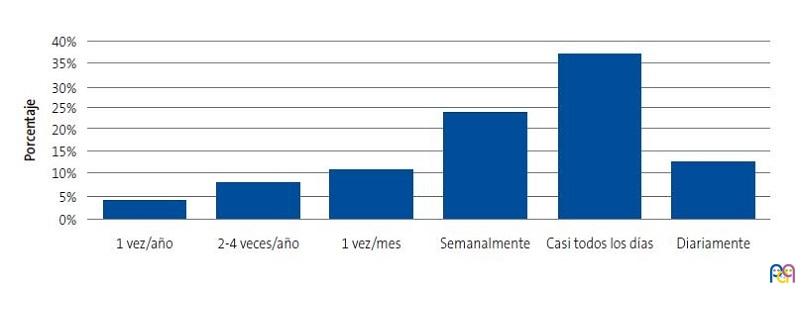
Entre los pediatras que realizan actividades de promoción de la lectura hay diferencias notables en cuanto a su frecuencia de realización, tal y como muestra la Figura 7, siendo la mitad quienes las realizan diaria o casi diariamente.
| Figura 7. Frecuencia de realización de actividades de promoción de la lectura (porcentaje de profesionales) |
|---|
 |
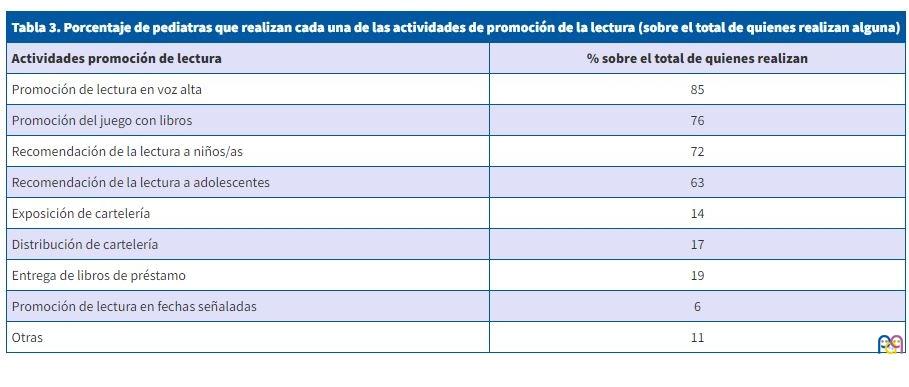
Respecto al tipo de actividades de promoción de la lectura, también son muy variadas y pueden observarse en la Tabla 3. La mayoría de los pediatras que realizan este tipo de actividades llevan a cabo más de una modalidad. La más frecuente es la recomendación de la lectura en voz alta (85%). Les sigue la recomendación a los niños/as de que dediquen tiempo a la lectura (76%) y también a los adolescentes (63%). El 72% promueve el uso de los libros como herramienta de juego e interacción de padres/madres con sus hijos/as, aprendiendo a pasar páginas, identificando imágenes de libros, etc., según la edad de estos. Un 14% tienen en su consulta o en sala de espera cartelería que promueve la práctica de la lectura y el 17% difunde la misma (octavillas, trípticos…). El 19% realiza entrega de libros de préstamo y un 6% apoya las actividades de promoción de la lectura en fechas señaladas (feria del libro, mes de la lectura…).
| Tabla 3. Porcentaje de pediatras que realizan cada una de las actividades de promoción de la lectura (sobre el total de quienes realizan alguna) | |
|---|---|
| Actividades promoción de lectura | Porcentaje sobre el total de quienes realizan |
| Promoción de lectura en voz alta | 85 |
| Promoción del juego con libros | 76 |
| Recomendación de la lectura a niños/as | 72 |
| Recomendación de la lectura a adolescentes | 63 |
| Exposición de cartelería | 14 |
| Distribución de cartelería | 17 |
| Entrega de libros de préstamo | 19 |
| Promoción de lectura en fechas señaladas | 6 |
| Otras | 11 |
Por otra parte, a quienes dijeron no llevar a cabo actividades de promoción de la lectura (65,6% de los encuestados), se les preguntó por los motivos de ello. Sus respuestas fueron también diversas, siendo la más frecuente la falta de tiempo (66 pediatras, 43,2%), seguida por la falta de espacio (27 pediatras, 16,4%) y falta de apoyo (13 pediatras, 8,5%).
DISCUSIÓN
En el trabajo que presentamos han participado un número importante de pediatras, con representación importante no solo de los dos ámbitos de trabajo de la Pediatría (hospitalario y Atención Primaria), sino también de quienes se encuentran haciendo la residencia. Sus edades cubren todo el espectro del colectivo y pertenecen a diferentes generaciones, con dedicaciones que van desde el inicio de la residencia hasta la jubilación. En la muestra hubo, como era de esperar, una mayor representación de mujeres que de hombres, con mayor presencia en Atención Primaria, donde los cupos informados se ajustan a valores habituales. Es decir, aunque no hayamos seguido en la selección de los participantes un muestreo aleatorio, la composición final de la muestra es suficientemente amplia y variada como para considerar que sus opiniones representan adecuadamente las del conjunto de la profesión.
En relación con las vocaciones profesionales, nuestro estudio revela que la vocación clínica es la mayoritaria en general entre los pediatras entrevistados, siendo más elegida por residentes y quienes ejercen la profesión en el ámbito hospitalario que por los pediatras de Atención Primaria. Sin embargo, la vocación preventiva es la menos señalada en general, si bien el subgrupo de pediatras de Atención Primaria se adhiere a ella en mayor medida que el resto. Por último, la vocación por la Pediatría social también fue minoritaria entre los encuestados, aunque presente especialmente también entre los pediatras que trabajan en Atención Primaria.
Respecto a las actividades de promoción de la salud, la mayoría de los profesionales informa dedicarle más del 10% de su tiempo de ejercicio profesional, siguiendo las recomendaciones de la Organización Mundial de la Salud, que señala constantemente la importancia de este tipo de actividades. La 9.ª Conferencia Mundial de Promoción de la Salud11 reafirmó que la salud es un derecho universal, un recurso esencial para la vida diaria y un objetivo social compartido, y señaló que los sistemas sanitarios se deben orientar hacia la prevención y promoción de la salud12. Esta es una tarea compartida entre profesionales que trabajan tanto en el ámbito hospitalario como en Atención Primaria, aunque es mayor el porcentaje de estos últimos que dedican un mayor tiempo a este tipo de actividades. Cada vez cobra más importancia un abordaje de la salud integral de la infancia, en la que se centre la atención en la familia, y se responda y apoye a las mismas durante todo el proceso madurativo de la infancia13.
Nuestra encuesta revela también que los residentes de Pediatría son los que menos tiempo dedican a la realización de actividades de promoción de la salud. Estos resultados están en línea con los de otros estudios que muestran que solo uno de cada cuatro residentes de Pediatría manifiesta su deseo de trabajar en Atención Primaria una vez finalizada la residencia14. Actualmente nos encontramos con un problema de déficit de pediatras de Atención Primaria y una previsión de que este déficit aumente. Ante esta circunstancia, las autoridades sanitarias deberían hacer un esfuerzo en la formación MIR y conseguir que las plazas de Pediatría de Atención Primaria sean más atractivas para los nuevos especialistas15.
Centrándonos en el objetivo prioritario de nuestro estudio, las actividades de promoción de la lectura son llevadas a cabo aproximadamente por un tercio de los pediatras encuestados, aunque su prevalencia es mayor entre quienes trabajan en Atención Primaria. Son muchas las asociaciones a nivel internacional que promueven la realización de estas actividades. La Asociación Americana de Pediatría (AAP) considera que la promoción de la lectura es un componente esencial de la Atención Primaria16 y la Asociación Española de Pediatras de Atención Primaria (AEPap), junto con otras asociaciones a nivel nacional, también señala la importancia de la promoción de la lectura, al defender que la lectura en voz alta debería de ser una actividad habitual en los hogares, ya que, aunque por sí sola no soluciona las desventajas sociales y las carencias culturales, favorece que el aprendizaje de la lectura y la escritura sea un logro más fácil para todos los niños y niñas, sin distinción, a la par que propicia una mejor relación emocional entre las personas adultas y la infancia17.
Intentando caracterizar cómo son las prácticas de promoción de la lectura en la Pediatría en España, nuestro estudio ha puesto de manifiesto una gran diversidad de actividades, siendo la promoción de la lectura en voz alta la más practicada, seguida por la recomendación de la lectura a niños/as y por la promoción del juego con libros. Es de resaltar que el grupo de adolescentes es animado a leer en un porcentaje algo inferior que el de niños/as de menos edad. Entre las prácticas menos realizadas se encuentran la entrega de libros de préstamo en la consulta, valerse de cartelería en consulta o sala de espera o infografía entregada en consulta para realizar esta práctica, así como la recomendación ocasional de la práctica de la lectura por parte de los pediatras en fechas señaladas, como el día del libro o el mes de la lectura. Los hallazgos en nuestro estudio sobre las prácticas concretas coinciden con las recomendaciones habituales sobre la amplia variedad de actividades que se pueden realizar desde la consulta de Pediatría. Por ejemplo, la AAP propone las siguientes: (1) informar a padres y madres de que leer en voz alta con sus hijos e hijas puede mejorar las relaciones entre ellos/as y preparar a la infancia para el aprendizaje; (2) asesorar a padres y madres sobre actividades de lectura compartida apropiadas para el desarrollo que sean agradables para todos/as y que ayuden a tener contacto con el lenguaje de los libros, imágenes y la palabra escrita; (3) proporcionar libros apropiados para el desarrollo que se puedan entregar en las visitas de salud infantil, sobre todo a aquellos de condiciones socioeconómicas y familiares más desfavorables; (4) asociarse con otros defensores de la infancia para influir en los mensajes y políticas nacionales que apoyen y promuevan estas experiencias clave de lectura temprana compartida18. Salvo la cuarta, todas las demás son llevadas a cabo en diferente medida por un número considerable de pediatras españoles/as, tal como hemos encontrado en nuestro estudio.
Limitaciones: la extrapolación de los resultados de nuestro estudio puede verse limitada por haber accedido a la muestra mediante listas de distribución, lo que no garantiza un muestreo representativo de la población objeto de estudio. Sin embargo, la configuración final de participantes con presencia de un alto número de profesionales, entornos de trabajo, edades y años de dedicación se asemeja notablemente a la realidad de la profesión en nuestro país.
CONCLUSIONES
De los datos recogidos podemos concluir que las actividades de promoción de la lectura son realizadas mayormente por los profesionales de Atención Primaria, en el marco de otras actividades de promoción de la salud, a su vez vinculadas principalmente con la vocación por la Pediatría social.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: diseño, preparación de instrumentos, análisis de resultados (AGG, IGG, JLM), captación de participantes, recogida de datos (AGG, IGG), redacción primer borrador (AGG), revisión y elaboración del manuscrito final (todos).
ABREVIATURAS
AAP: Asociación Americana de Pediatría · AEPap: Asociación Española de Pediatría de Atención Primaria · DS: desviación estándar · MIR: médico interno residente · NSE: nivel socioeconómico y educativo.
BIBLIOGRAFÍA
- Orden SCO/3148/2006, de 20 de septiembre, por la que se aprueba y publica el programa formativo de la especialidad de Pediatría y sus Áreas Específicas. En: BOE núm. 246. Año 2006 [en línea] [consultado el 10/10/2023]. Disponible en www.boe.es/buscar/doc.php?id=BOE-A-2006-17999
- Asociación Española de Pediatría. Libro blanco de las ACES Pediátricas. Año 2021 [en línea] [consultado el 10/10/2023]. Disponible en https://luaediciones.com/aep/aces2021/
- Portal Estadístico Ministerio de Sanidad, Área de Inteligencia y Gestión, Sistema de Información de Atención Especializada, Área de profesionales y Especialidades. En: Portal Estadístico, Área de Inteligencia de Gestión. Año 2021 [en línea] [consultado el 10/10/2023]. Disponible en https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/C/siae/siae/hospitales/personal-y-formacion/areas-profesionales-y-especialidades
- Portal Estadístico Ministerio de Sanidad, Área de Inteligencia y Gestión, Sistema de Información de Atención Primaria, Área de profesionales y Modalidades Asistenciales. En: Portal Estadístico, Área de Inteligencia de Gestión. Año 2021 [en línea] [consultado el 10/10/2023]. Disponible en https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/C/sistema-de-informacion-de-atencion-primaria-siap/profesionales/modalidades-asistenciales
- Hidalgo Cantabrana C, González García M, González Rodríguez S, Hidalgo A, Hidalgo Cantabrana C, González García M, et al. Sobre la vocación médica a través de opiniones tomadas de la literatura médica y de ficción. Rev Med Cine. 2020;16(4):319-30. https://dx.doi.org/10.14201/rmc2020164319330
- Asociación Española de Pediatría de Atención Primaria. Competencias específicas pediatría de atención primaria. En: AEPap [en línea] [consultado el 10/10/2023]. Disponible en www.aepap.org/sites/default/files/documento/archivos-adjuntos/competencias_especificas_pediatria_de_ap_aepap.pdf
- Council on Early Childhood, Council on School Health. The Pediatrician’s Role in Optimizing School Readiness. 2016;138:e20162293. https://doi.org/10.1542/peds.2016-2293
- Duursma E, Augustyn M, Zuckerman B. Reading aloud to children: the evidence. Arch Dis Child. 2008;93:554-7. https://doi.org/10.1136/adc.2006.106336
- Garach Gómez A, Alperi García S, Gutiérrez García I. La lectura como herramienta de promoción de la salud. Form Act Pediatr Aten Prim. 2021;14:133-6.
- Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol Off J Div Health Psychol Am Psychol Assoc. 2000;19:586-92. https://doi.org/1037//0278-6133.19.6.586
- 9.a Conferencia Mundial de Promoción de la Salud. Acuerdo de dirigentes mundiales para promover la salud en pro de los Objetivos de Desarrollo Sostenible. En: Organización Mundial de la Salud. Año 2016 [en línea] [consultado el 10/10/2023]. Disponible en www.who.int/es/news/item/21-11-2016-9th-global-conference-on-health-promotion-global-leaders-agree-to-promote-health-in-order-to-achieve-sustainable-development-goals
- Camarelles Guillem F. Los retos de la prevención y promoción de la salud, y los del PAPPS. Aten Primaria. 2018;50(1):1-2. https://doi.org/10.1016/S0212-6567(18)30358-5
- Inkelas M, Oberklaid F. Improving preventive and health promotion care for children. Isr J Health Policy Res. 2018;7:62. https://doi.org/10.1186/s13584-018-0259-3
- Álvarez Casaño M, Gorrotxategi Gorrotxategi PJ, Castillo Campos l, Cámara Otegui A, Martín Moya R, Fuentes Redondo T, et al. Salidas laborales de los residentes de Pediatría. Datos del periodo 2014-2017. Rev Pediatr Aten Primaria. 2019;21:247-53.
- Gorrotxategi Gorrotxategi P, García Vera C, Graffigna Lojendio A, Sánchez Pina C, Palomino Urda N, Rodríguez Fernández-Oliva CR, et al. Situación de la Pediatría de Atención Primaria en España en 2018. Rev Pediatr Aten Primaria. 2018;20:e89-e104.
- Zuckerman B, Needlman R. 30 Years of Reach Out and Read: Need for a Developmental Perspective. 2020;145:e20191958. https://doi.org/10.1542/peds.2019-1958
- Manifiesto de la voz a las letras. En: Asociación Entrelibros [en línea] [consultado el 10/10/2023]. Disponible en www.asociacionentrelibros.es/wp-content/uploads/2016/12/de-la-voz-a-las-letras.pdf
- Council on Early Childhood, High PC, Klass P. Literacy promotion: an essential component of primary care pediatric practice. 2014;134:404-9. https://doi.org/10.1542/peds.2014-1384
Comentarios
Este artículo aún no tiene comentarios.