
Vol. 25 - Num. 97
Originales
Variaciones y diferentes percepciones en la suplementación con vitamina D en la edad pediátrica en España
Diego de Sotto-Estebana, Guiomar Pérez de Nanclares Lealb, M.ª José Alcázar Villarc, Silvia Marín del Barriod, Lorena Miñones Suáreze, Eduard Mogas Viñalsf, Isolina Riaño Galáng, Luis Antonio Castaño Gonzálezh, José M.ª Martos Telloi, Grupo Metabolismo Fosfocálcico de la Sociedad Española de Endocrinología Pediátrica (SEEP)
aServicio de Pediatría. Clínica Rotger. Palma. Islas Baleares. España.
bLaboratorio de Genética Molecular. Hospital Universitario Araba-Txagorritxu. Vitoria. Álava. España.
cServicio de Pediatría. Hospital Universitario de Fuenlabrada. Fuenlabrada. Madrid. España.
dEndocrinología Pediátrica. Servicio de Pediatría. Hospital Sant Joan de Déu. Barcelona. España.
eEndocrinología Pediátrica. Servicio de Pediatría. Hospital Reina Sofia. Tudela. Navarra. España.
fEndocrinología Pediátrica. Servicio de Pediatría. Hospital Universitario Vall d´Hebron. Barcelona. España.
gServicio de Pediatría. Hospital Universitario Central de Asturias. Oviedo. Asturias. España.
hInstituto BioCruces. Endocrinología Pediátrica. Servicio de Pediatría. Hospital Universitario Cruces. Barakaldo. Vizcaya. España.
i Endocrinología Pediátrica. Servicio de Pediatría. Hospital Universitario Virgen de La Arrixaca. Murcia. España.
Correspondencia: D de Sotto-Esteban. Correo electrónico: sottomartin@gmail.com
Cómo citar este artículo: de Sotto-Esteban D, Pérez de Nanclares Leal G, Alcázar Villar MJ, Marín del Barrio S, Miñones Suárez L, Mogas Viñals E, et al. Variaciones y diferentes percepciones en la suplementación con vitamina D en la edad pediátrica en España . Rev Pediatr Aten Primaria. 2023;25:e1-e13.
Publicado en Internet: 21-03-2023 - Número de visitas: 19608
Resumen
Introducción: el raquitismo es un problema de salud a nivel global. La deficiencia de vitamina D se ha convertido en una pandemia, su interés ha aumentado por la implicación de la misma en múltiples acciones extraesqueléticas.
Material y métodos: se realizó una encuesta a través de correo electrónico entre pediatras españoles para estudiar su actitud en relación con la suplementación profiláctica de vitamina D.
Resultados: un 83% de los pediatras tienen políticas de profilaxis de vitamina D en su área. Un 61,6% inicia la profilaxis en las dos primeras semanas y un 81,5% la mantiene el primer año. Un 57,2% realiza una búsqueda de deficiencia de vitamina D, sobre todo si trabajan en medio hospitalario.
Conclusiones: las políticas de profilaxis con vitamina D son bastantes uniformes. Más de la mitad de los pediatras españoles realizan una búsqueda sistemática mediante analítica de deficiencia de vitamina D en sus pacientes con factores de riesgo durante la infancia y adolescencia.
Palabras clave
● Deficiencia de vitamina D ● Encuesta ● Pediatras españoles ● Profilaxis raquitismoINTRODUCCIÓN
La vitamina D es fundamental en el metabolismo fosfocálcico y la adquisición de masa ósea1. La principal fuente de vitamina D es su síntesis cutánea tras la exposición solar. La definición de deficiencia de vitamina D se basa en la medición de las concentraciones plasmáticas de 25-hidroxivitamina D (calcifediol). El metabolito activo, el calcitriol o 1-25(OH)D3, tiene una vida media muy corta, se afecta de forma tardía en el déficit y tiene una concentración muy baja, lo que dificulta su utilización como parámetro de referencia1-5.
En los últimos años es creciente el número de datos que avalan la importancia de la vitamina D en funciones extraesqueléticas. La vitamina /hormona D se encuentra comprometida en la regulación directa o indirecta de aproximadamente 2000 genes y está implicada en la patogenia de enfermedades infecciosas, alergias, enfermedades autoinmunes, enfermedades cardiovasculares, desórdenes mentales, diabetes y tumores1,3; estudios observacionales refieren asociación entre concentraciones más altas de vitamina D con un mejor curso de diversos procesos crónicos1. La deficiencia de vitamina D se ha descrito cada vez más frecuentemente en todas las etnias y todas las áreas, definiéndose por algunos autores como una importante pandemia a nivel de salud global3,4.
El raquitismo sigue constituyendo un problema de salud mundial en los países subdesarrollados2, resurgiendo en nuestro medio en relación con la migración6,7.
En cuanto a los puntos de corte para definir la deficiencia de vitamina D1-7, existe información suficiente para fundamentar el valor dintel en adultos, publicaciones para apoyar la decisión en la adolescencia y datos mucho más escasos en la infancia8,9. Así, en Pediatría no existen datos que apoyen la existencia de un umbral de absorción de calcio en relación con los niveles de vitamina D10; ni siquiera abundan los estudios cuando hablamos de salud ósea11,12.
En los últimos años diferentes asociaciones y sociedades profesionales han lanzado sus propuestas referentes a las situaciones en las que se debe medir la vitamina D y los niveles para definir su deficiencia, incluyendo más recientemente fundamentos relacionados con sus acciones extraesqueléticas. Saggese y cols. en su artículo de la posición italiana realiza una amplia revisión5, indicando como cifra más repetida para la definición de deficiencia de vitamina D niveles por debajo de 20 ng/ml (50 mmol/l), incluyendo algunos un grupo intermedio entre 20 y 30 ng/ml en el que se habla de insuficiencia; el Consenso Global para el Raquitismo2 propone un dintel inferior. El nivel de 20 ng/ml es el propuesto por la Asociación Española de Pediatría13.
España no escapa a la descripción general de un amplio porcentaje de población con deficiencia de vitamina D a nivel mundial; en población pediátrica se ha descrito en varias regiones, aunque no de forma uniforme en neonatos, lactantes, niños y adolescentes, incluso en áreas del mediterráneo y el sur con suficiente radiación solar14-20.
Existe bastante consenso en el tratamiento del raquitismo, aunque con sus diferentes pautas2; sin embargo, no es así en la suplementación profiláctica y el tratamiento ante presencia de niveles bajos en población sin clínica.
Dada la tasa de mayor crecimiento el primer año, se centran asimismo las recomendaciones de prevención de raquitismo en esta época de la vida y, junto con las recomendaciones generales en hábitos de vida, los principales organismos internacionales comenzaron a recomendar la administración profiláctica de vitamina D (IOM21, Endocrine Society3, Consenso Global2, AAP22); con pequeñas variaciones, la indicación más frecuente es la suplementación oral con 400 UI al día de vitamina D a todos los lactantes, independientemente del tipo de alimentación durante el primer año de vida.
Como la deficiencia de vitamina D siempre se traduce en el recién nacido2 y la vida media de la 25 OH vitamina D es de solo dos semanas, la prevención debe incluir también a las madres gestantes e iniciarse en los neonatos tras el nacimiento.
En España también existen recomendaciones de la AEP en el mismo sentido13, específicamente 400 UI de vitamina D al día en lactantes hasta el año. Asimismo, el grupo Previnfad de la AEPap23 realizó indicaciones en este sentido, aunque no de forma universal y no habiéndose revisado en los últimos años.
Existen pocos estudios que se centren en el grado de conocimiento de los profesionales de las medidas sanitarias, su cumplimiento y los factores relacionados que pueden influir en la implementación de estas. Una encuesta reciente en nuestro país sobre uso y conocimiento de pseudociencias por profesionales de Pediatría ponía en evidencia que un elevado número de pediatras españoles aconsejaba a los padres que administran a sus hijos tratamientos no avalados por la evidencia científica24.
En este sentido, nos propusimos realizar una encuesta por correo electrónico entre profesionales de Pediatría a nivel estatal para analizar aspectos relacionados con la vitamina D. Como objetivo principal nos propusimos analizar el grado de cumplimiento de las recomendaciones de profilaxis con vitamina D en nuestro medio. Entre los objetivos secundarios se encontraba analizar el conocimiento y las particularidades de la aplicación de esta medida entre los profesionales de Pediatría, así como la relación de las características profesionales de los sanitarios con el cumplimiento y los diferentes aspectos de las recomendaciones.
MATERIAL Y MÉTODOS
Estudio descriptivo realizado a través de una encuesta en línea de ámbito estatal en España mediante Google Docs sobre prácticas y percepciones en la suplementación con vitamina D en la edad pediátrica. La encuesta se difundió a través de la lista de correo de la Asociación Española de Pediatría (AEP) entre el 13/10/21 y 30/11/21, con un correo inicial y un recordatorio. Todas las preguntas menos una exigía contestación obligatoria.
La encuesta era anónima, voluntaria, asegurando la protección de datos, dirigida a pediatras existentes en la lista de correo de la AEP; en ella se solicitaba a los participantes su reenvío a médicos de familia y médicos generales que trabajaran en el campo del pediatra por no estar en dicha lista de correo. Para una población finita de profesionales adscritos a la AEP que estimamos de 12 219, se necesitan 983 profesionales para estimar los parámetros poblacionales, con una precisión de 3%, con una confianza de 95% y una situación de máxima indeterminación (p = 1-p).
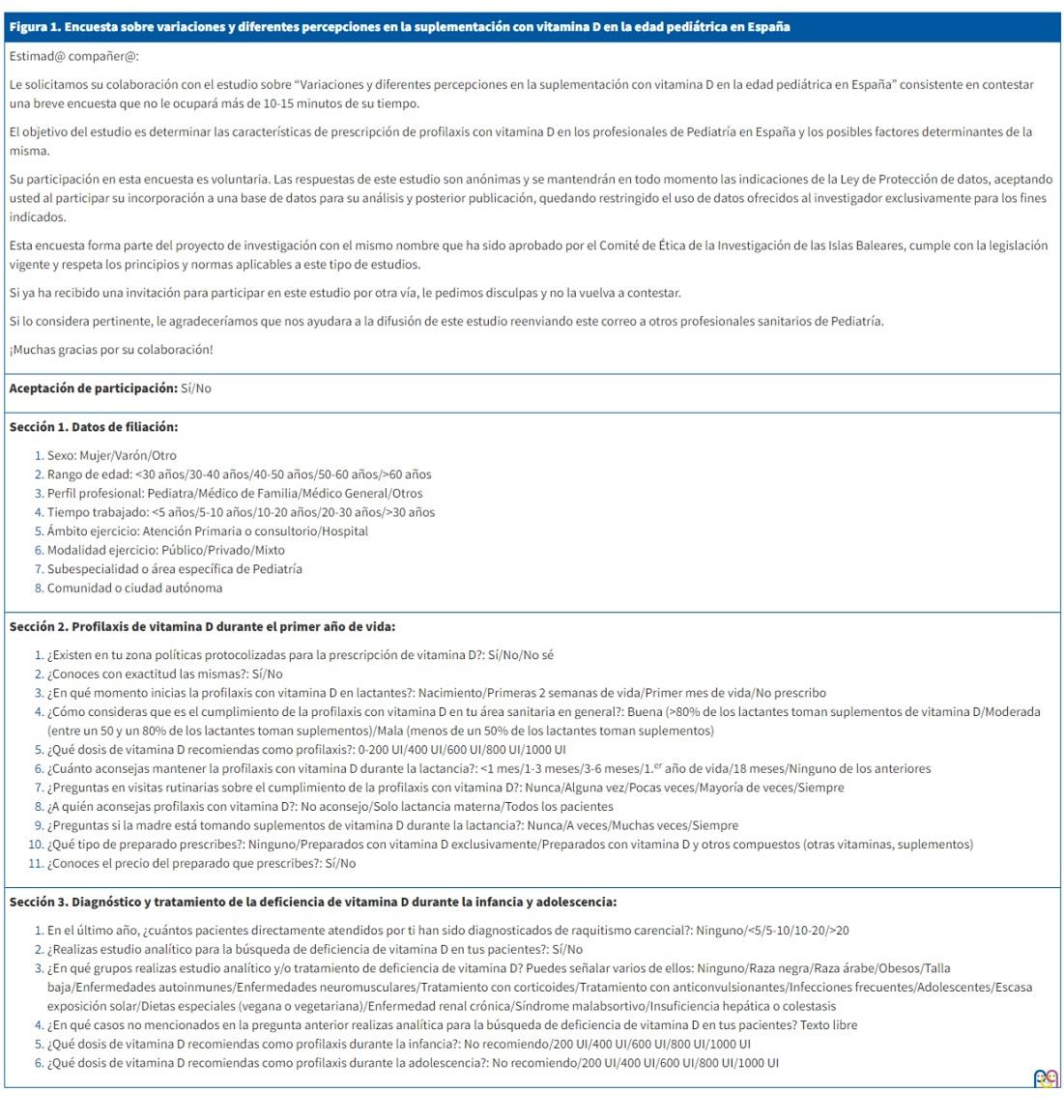
La encuesta estaba estructurada (Figura 1) en tres bloques, tras una pregunta de aceptación:
- Características de participantes (7 preguntas: sexo, edad, perfil profesional, tiempo de ejercicio profesional, ámbito de ejercicio profesional, modalidad de ejercicio profesional, subespecialidad o área de capacitación específica, comunidad o ciudad autónoma de residencia).
- Conocimiento y actitud sobre la profilaxis con vitamina D durante el periodo neonatal y lactancia (10 preguntas: existencia de política sanitaria de profilaxis con vitamina D y su conocimiento, opinión sobre el grado de cumplimiento, momento de inicio, duración y comprobación de la pauta de profilaxis, población objeto, tipo de preparado).
- Conocimiento y actitudes sobre el diagnóstico, la profilaxis y el tratamiento de la deficiencia de vitamina D durante la infancia y adolescencia (6 preguntas: diagnóstico de casos de raquitismo, búsqueda sistemática de deficiencia de vitamina D y en qué casos, dosis profilácticas de vitamina D en infancia y adolescencia).
| Figura 1. Encuesta sobre variaciones y diferentes percepciones en la suplementación con vitamina D en la edad pediátrica en España |
|---|
|
Estimad@ compañer@: Le solicitamos su colaboración con el estudio sobre “Variaciones y diferentes percepciones en la suplementación con vitamina D en la edad pediátrica en España” consistente en contestar una breve encuesta que no le ocupará más de 10-15 minutos de su tiempo. El objetivo del estudio es determinar las características de prescripción de profilaxis con vitamina D en los profesionales de Pediatría en España y los posibles factores determinantes de la misma. Su participación en esta encuesta es voluntaria. Las respuestas de este estudio son anónimas y se mantendrán en todo momento las indicaciones de la Ley de Protección de datos, aceptando usted al participar su incorporación a una base de datos para su análisis y posterior publicación, quedando restringido el uso de datos ofrecidos al investigador exclusivamente para los fines indicados. Esta encuesta forma parte del proyecto de investigación con el mismo nombre que ha sido aprobado por el Comité de Ética de la Investigación de las Islas Baleares, cumple con la legislación vigente y respeta los principios y normas aplicables a este tipo de estudios. Si ya ha recibido una invitación para participar en este estudio por otra vía, le pedimos disculpas y no la vuelva a contestar. Si lo considera pertinente, le agradeceríamos que nos ayudara a la difusión de este estudio reenviando este correo a otros profesionales sanitarios de Pediatría. ¡Muchas gracias por su colaboración! |
|
Aceptación de participación: Sí/No |
|
Sección 1. Datos de filiación:
|
|
Sección 2. Profilaxis de vitamina D durante el primer año de vida:
|
|
Sección 3. Diagnóstico y tratamiento de la deficiencia de vitamina D durante la infancia y adolescencia:
|
Se consideró de manera arbitraria como grado de cumplimiento de la profilaxis de vitamina D en lactantes en el área del profesional el estimado por el mismo: buen cumplimiento ≥80% de los casos, cumplimiento moderado entre 50 y 80% y mal cumplimiento <50%.
Se realizó análisis descriptivo univariante de los datos categóricos (recuento total y porcentajes) y un análisis bivariante utilizó la prueba de Chi cuadrado. Se consideró estadísticamente significativa una p <0,05. Se utilizó para el análisis estadístico SPSSv23.
RESULTADOS
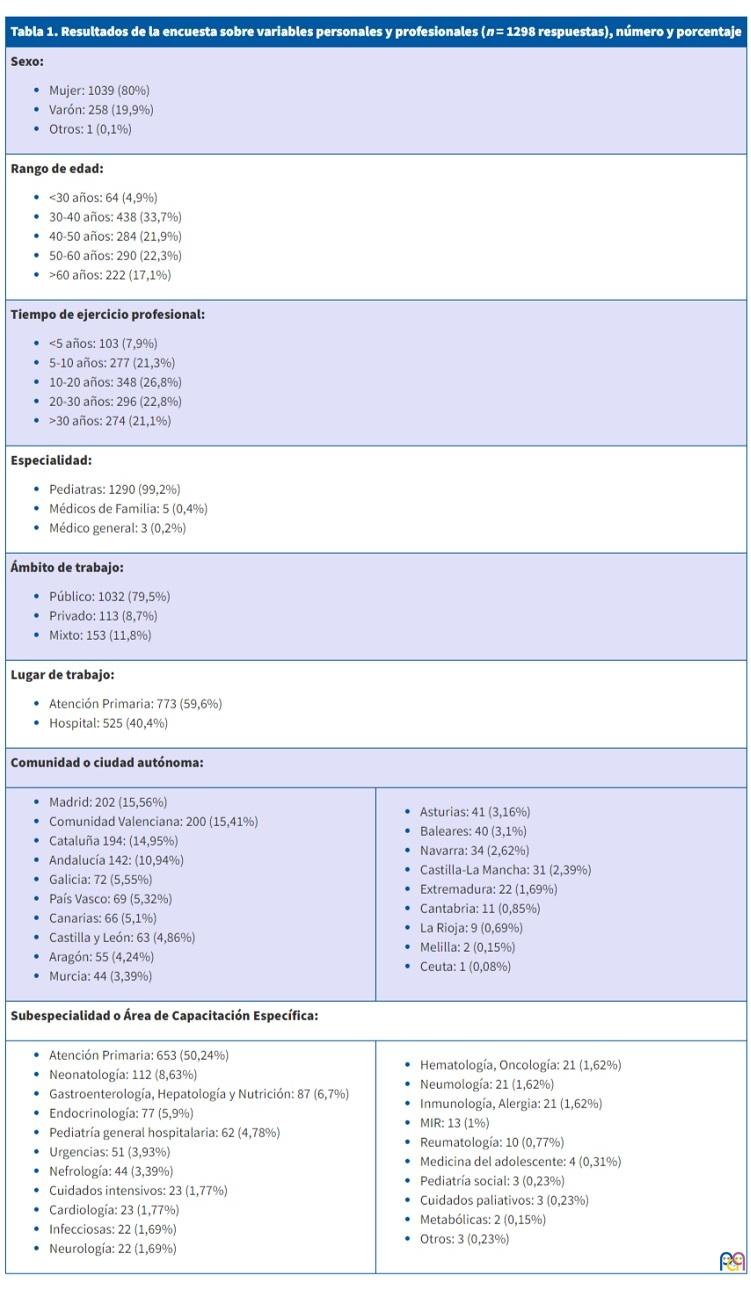
Un total de 1298 respuestas (un rechazo) fueron recibidas, lo que supone un 11% de la lista de correo y un 20,9% de los que abrieron el correo. En la Tabla 1 se reflejan los resultados de la encuesta sobre las diferentes características de los profesionales. Un 80% eran mujeres (1039), la distribución por rango de edad era uniforme salvo el grupo de menos de 30 años, que era el menos numeroso (4,9%). El tiempo de ejercicio profesional también se distribuía de manera relativamente uniforme. Un 99,2% eran pediatras, trabajando la mayoría en el ámbito público (79,5%), y más de la mitad de los encuestados ejercía en Atención Primaria-consultorio (59,6%); las comunidades autónomas más representadas fueron Madrid, Valencia, Cataluña y Andalucía.
| Tabla 1. Resultados de la encuesta sobre variables personales y profesionales (n = 1298 respuestas), número y porcentaje | |
|---|---|
|
Sexo:
|
|
|
Rango de edad:
|
|
|
Tiempo de ejercicio profesional:
|
|
|
Especialidad:
|
|
|
Ámbito de trabajo:
|
|
|
Lugar de trabajo:
|
|
|
Comunidad o ciudad autónoma: |
|
|
|
|
Subespecialidad o Área de Capacitación Específica: |
|
|
|
En relación con los conocimientos y opiniones sobre profilaxis con vitamina D durante el primer año de vida (Tabla 2), la gran mayoría tenía una política sanitaria establecida sobre la misma en su área de trabajo (83%) y un 76,3% la conocía con exactitud. Las mujeres la conocían con más frecuencia que los hombres (77,96% vs. 69,5%, p <0,01). Un 77,9% consideraba que el cumplimiento de esta era bueno en su zona.
| Tabla 2. Conocimientos y opiniones sobre profilaxis vitamina D en el primer año de vida |
|---|
|
Existencia de protocolos de profilaxis de raquitismo con vitamina D:
|
|
Conocimiento de las políticas sanitarias de profilaxis:
|
|
Grado de cumplimiento de la profilaxis estimado por los profesionales:
|
|
Inicio de profilaxis con vitamina D en lactantes:
|
|
Duración de profilaxis con vitamina D:
|
|
Dosis de vitamina D recomendada:
|
|
Comprobación del cumplimiento:
|
|
Población diana para profilaxis con vitamina D:
|
|
Cumplimiento de suplementos de vitamina D para la madre:
|
|
Tipo de preparado:
|
|
Conoce el precio del preparado:
|
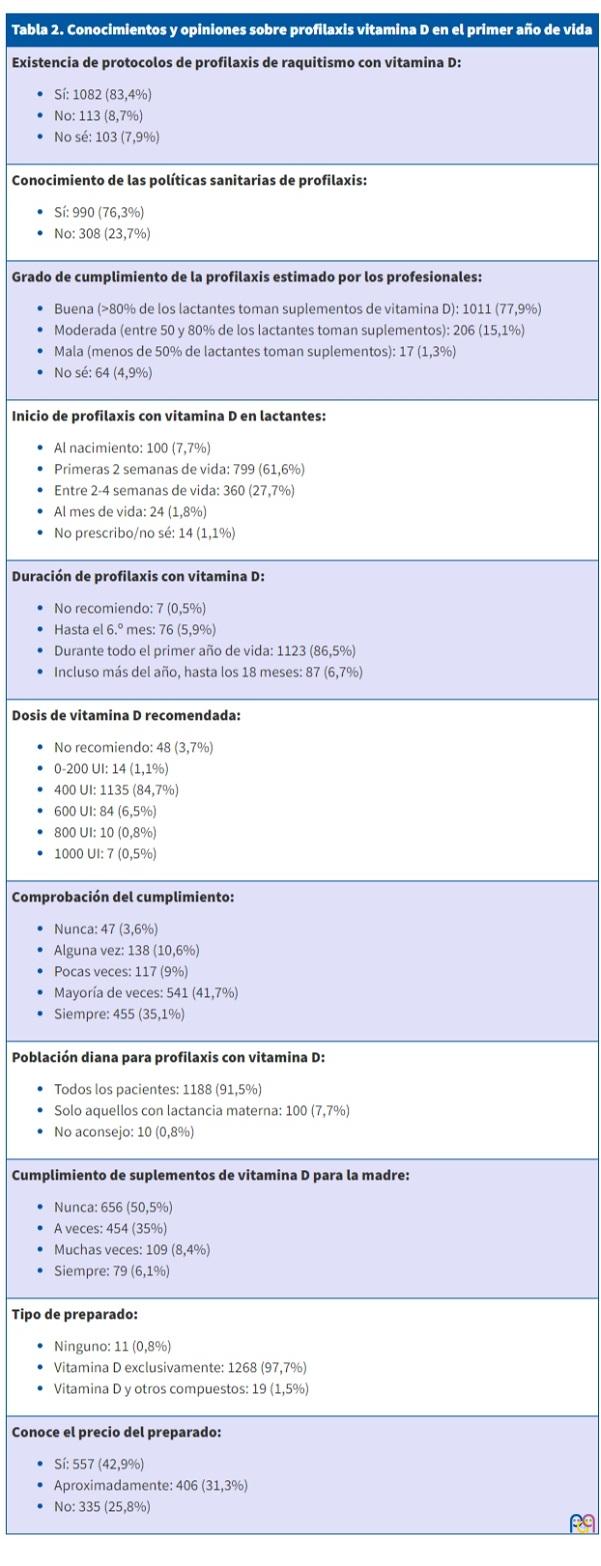
El 61,6% empieza la profilaxis en las dos primeras semanas de vida y solo un 1,8% en la maternidad. La gran mayoría (86,5%) la recomienda durante todo el primer año de vida (en Asturias hasta los 18 meses de vida en un 63,4% de los casos) y a todos los lactantes (91,5%), independientemente del tipo de alimentación (materna, artificial, mixta), con un tipo de preparado que contiene solo vitamina D en casi todos los casos (97,7%) y conociendo su precio exacto o aproximado (74,2%). La confirmación del cumplimiento de la profilaxis es la norma (35,1% y 41,7% preguntan siempre o casi siempre).
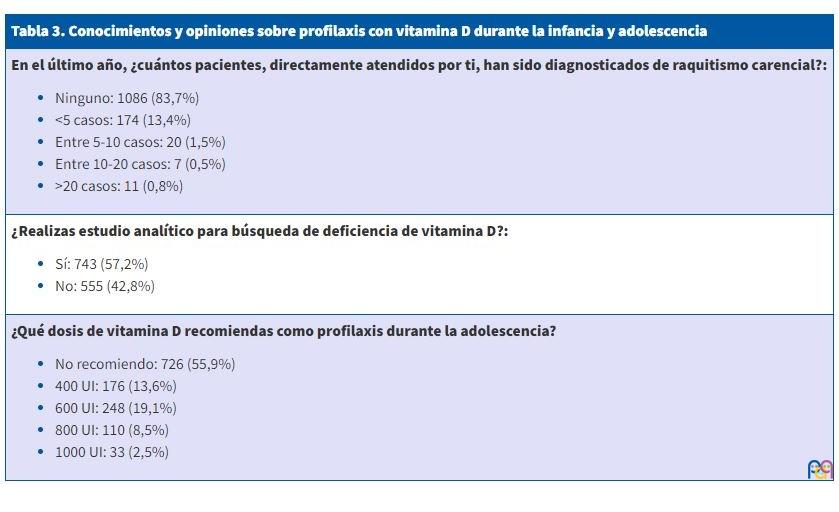
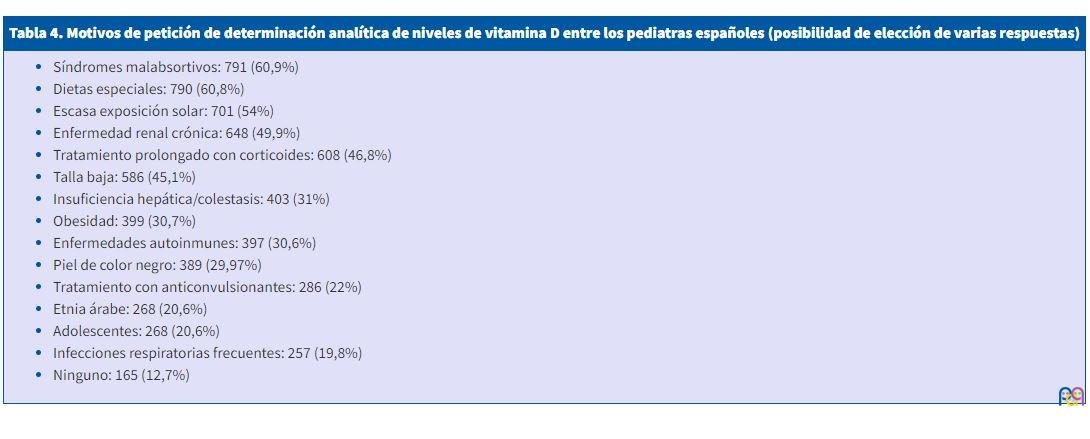
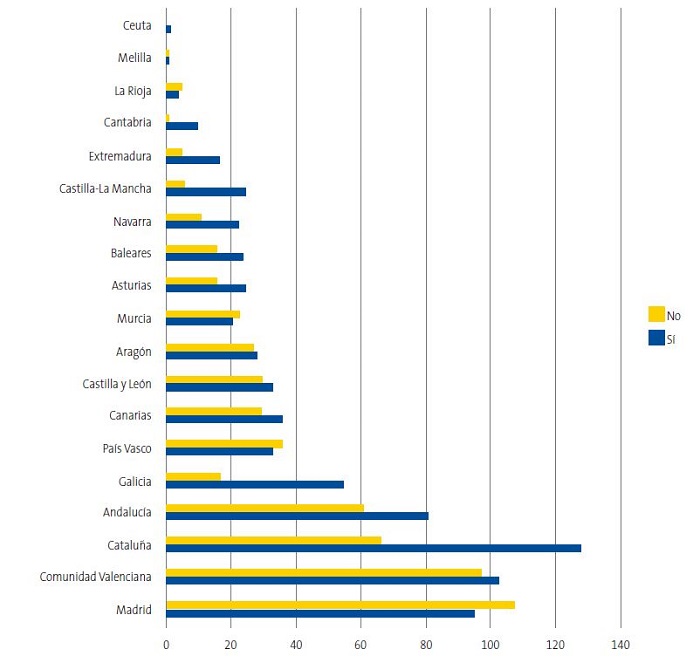
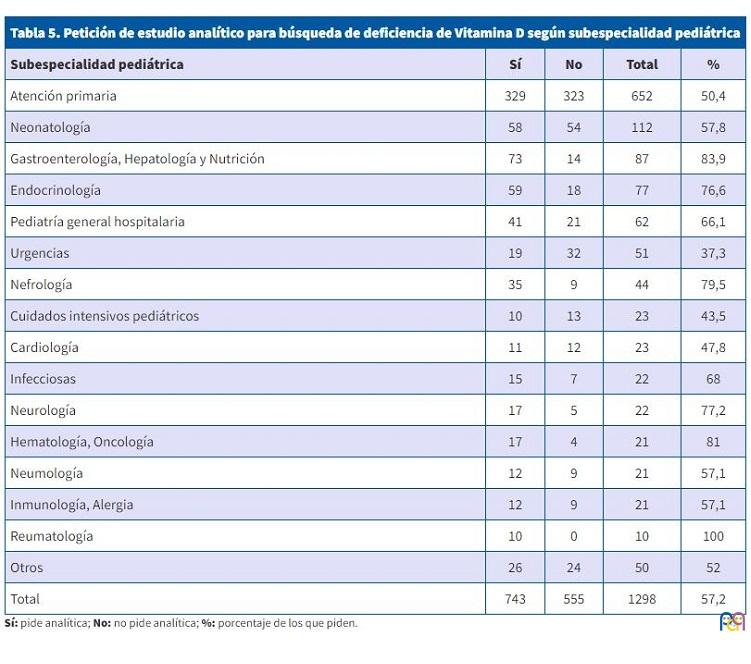
En cuanto a la actitud durante la infancia y adolescencia (Tabla 3), hay que señalar que no es frecuente en nuestro medio el diagnóstico de raquitismo (el 83,7% de los encuestados no tienen ningún caso). Un 57,2% de los pediatras realiza una búsqueda sistemática de deficiencia de vitamina D mediante petición de analítica en algún colectivo de sus pacientes. Entre estos grupos se encuentran principalmente aquellos que siguen dietas especiales, con escasa exposición solar o presencia de enfermedades, como fallo renal crónico, talla baja o síndrome malabsortivo (Tabla 4). Solicitaban en mayor medida una analítica para detectar la deficiencia de vitamina D los profesionales de medio hospitalario con respecto a los de Atención Primaria (67,6% vs. 50,2%, p <0,01), los que tenían entre 10-20 años de ejercicio profesional (un 67,2%, siendo aproximadamente mitad y mitad en los otros grupos) y entre 30 y 40 años de edad; variaba ampliamente entre las diferentes comunidades autónomas (Figura 2), aunque el porcentaje de respuestas en algunos casos era muy inferior. En cuanto a las subespecialidades pediátricas, fueron los reumatólogos, nefrólogos, endocrinólogos, gastroenterólogos, hematoncólogos y neurólogos los que más la demandaron (Tabla 5).
| Tabla 3. Conocimientos y opiniones sobre profilaxis con vitamina D durante la infancia y adolescencia |
|---|
|
En el último año, ¿cuántos pacientes, directamente atendidos por ti, han sido diagnosticados de raquitismo carencial?:
|
|
¿Realizas estudio analítico para búsqueda de deficiencia de vitamina D?:
|
|
¿Qué dosis de vitamina D recomiendas como profilaxis durante la adolescencia?
|
| Tabla 4. Motivos de petición de determinación analítica de niveles de vitamina D entre los pediatras españoles (posibilidad de elección de varias respuestas) |
|---|
|
| Figura 2. Petición de estudio analítico para búsqueda de deficiencia de vitamina D según comunidad o ciudad autónoma |
|---|
 |
| Tabla 5. Petición de estudio analítico para búsqueda de deficiencia de Vitamina D según subespecialidad pediátrica | ||||
|---|---|---|---|---|
| Subespecialidad pediátrica | Sí | No | Total | % |
| Atención primaria | 329 | 323 | 652 | 50,4 |
| Neonatología | 58 | 54 | 112 | 57,8 |
| Gastroenterología, Hepatología y Nutrición | 73 | 14 | 87 | 83,9 |
| Endocrinología | 59 | 18 | 77 | 76,6 |
| Pediatría general hospitalaria | 41 | 21 | 62 | 66,1 |
| Urgencias | 19 | 32 | 51 | 37,3 |
| Nefrología | 35 | 9 | 44 | 79,5 |
| Cuidados intensivos pediátricos | 10 | 13 | 23 | 43,5 |
| Cardiología | 11 | 12 | 23 | 47,8 |
| Infecciosas | 15 | 7 | 22 | 68 |
| Neurología | 17 | 5 | 22 | 77,2 |
| Hematología, Oncología | 17 | 4 | 21 | 81 |
| Neumología | 12 | 9 | 21 | 57,1 |
| Inmunología, Alergia | 12 | 9 | 21 | 57,1 |
| Reumatología | 10 | 0 | 10 | 100 |
| Otros | 26 | 24 | 50 | 52 |
| Total | 743 | 555 | 1298 | 57,2 |
La gran mayoría recomienda como dosis profiláctica de vitamina D durante la infancia 400 UI de colecalciferol (87,4%), mientras que no recomiendan la misma durante la adolescencia.
DISCUSIÓN
El perfil de los participantes es bastante parecido al existente en el directorio de socios de la AEP (12 219 socios, 8144 mujeres), salvo que respondieron proporcionalmente más mujeres (80% en encuesta vs. 66,7% en lista de correo) y que el grupo de menor edad participó en escasa cuantía (4,9% contestaron y representan un 15,9% de los encuestados). La mayoría de las profesionales trabajaban en Atención Primaria y las comunidades autónomas con más participación fueron las de más población.
En prácticamente todo el territorio estatal existe una política de salud pública de administración de colecalciferol como prevención del raquitismo y deficiencia de vitamina D, y en torno a tres cuartas partes de los profesionales dicen conocerla con exactitud.
Dada la falta de registros uniformes y fiables para medir el cumplimiento, decidimos, a semejanza de la encuesta realizada hace unos años a nivel europeo25 entre expertos del tema, utilizar la opinión de los propios profesionales como forma de estimar el grado de cumplimiento. Así, un 77,9% consideró que el cumplimiento era bueno (más del 80% de los padres seguían la indicación).
Un 61,6% de los profesionales indicaron su comienzo en las dos primeras semanas de vida. Los niveles de vitamina D en el recién nacido son equivalentes a los de la madre al final de la gestación y la vida media del 25 hidroxicalciferol es de dos semanas, luego debería ser norma general que el comienzo fuera en estas dos primeras semanas2,25. Solo un 1,8% refirió el comienzo ya desde la propia maternidad, que en el trabajo europeo se relacionó con una mayor tasa de seguimiento de la recomendación. La gran mayoría de profesionales recomienda la administración durante todo el primer año de vida, en consonancia con las recomendaciones más generalizadas (en Asturias está indicada durante el primer año y medio). Asimismo, la recomendación es universal, independientemente del tipo de alimentación, lo que también se ha visto que se relaciona con mejor adherencia a la medida25. Generalmente, se utilizan preparados que contienen solo vitamina D, aspecto positivo, pues son mucho más económicos.
En la adherencia a un tratamiento influyen tanto factores relacionados con los pacientes como con los profesionales sanitarios. En relación al cumplimiento de la profilaxis con vitamina D, los resultados de una encuesta patrocinada por el grupo de metabolismo óseo de la European Society for Paediatric Endocrinology (ESPE)25 pusieron de manifiesto que existía un mejor cumplimiento de las indicaciones cuando los padres eran informados al nacimiento antes del alta hospitalaria, la suplementación de los bebes era universal, existía alguna política de financiación a las familias para adquirir los suplementos y se incluía la monitorización del cumplimiento en las visitas de seguimiento de controles rutinarios.
En cuanto a la actitud durante la infancia y adolescencia, hay que señalar que no es frecuente en nuestro medio el diagnóstico de raquitismo (el 83,7% de los encuestados no tienen ningún caso). Un 57,2% de los pediatras realiza una búsqueda sistemática de deficiencia de vitamina D mediante petición de analítica en algún colectivo de sus pacientes. Entre estos grupos se encuentran principalmente aquellos que siguen dietas especiales, con escasa exposición solar o presencia de enfermedades, como fallo renal crónico, talla baja o síndromes malabsortivos (Tabla 5).
La gran mayoría recomienda como dosis profiláctica de vitamina D durante la infancia 400 UI de colecalciferol, mientras que no recomiendan la misma durante la adolescencia.
Entre los factores de riesgo para la deficiencia de vitamina D se encuentran: la piel oscura/negra, la escasa exposición al sol, la escasa ingesta dietética, los recién nacidos de madres con factores de riesgo para su deficiencia, la lactancia materna, la existencia de enfermedades crónicas como el fallo renal crónico, el fallo hepático y/o colestasis, los síndromes malabsortivos, el uso de medicaciones crónicas como anticonvulsionantes, glucocorticoides o antifúngicos y la obesidad1,5-9.
En nuestro país, siguiendo el ejemplo de la literatura internacional, se han realizado trabajos que reflejan la deficiencia de vitamina D en estos grupos de riesgo, como es el caso de la lactancia materna26, obesidad27-31, alergias32, infecciones33,34, atopia35, enfermedades hematológicas36 e ingesta de medicación anticomicial37, entre otras.
Debemos considerar que, aunque los expertos recomiendan suplementación con vitamina D en muchos de estos grupos de riesgo, no existen suficientes datos que avalen la búsqueda sistemática de deficiencia de vitamina D en ellos mediante analítica; por supuesto, ninguna prueba para hacerlo en población sana38,39. Es necesario conocer lo que se sabe con evidencia y aquellos apartados en los que necesitamos más datos, como queda reflejado en una reciente revisión del grupo francés40.
Los profesionales sanitarios a veces no ponemos en práctica recomendaciones que sabemos que tienen evidencia suficiente y, por el contrario, realizamos algunas que no la tienen.
Son varias e importantes las limitaciones de nuestro estudio, de las que destacamos dos: la respuesta a las encuestas suele ser baja y las personas más motivadas y con más interés en el tema son las que suelen responder. Además, hemos utilizado un parámetro subjetivo, como es la opinión de los profesionales para estimar el grado de cumplimiento de la administración de vitamina D preventiva a los niños por parte de los progenitores. Llama la atención la disparidad en el resultado de pediatras que no recomiendan profilaxis de vitamina D en las dos preguntas que abordan este punto, 7 frente a 48, sin poder explicar si ello se debe a factores relacionados con el diseño de la encuesta o con la fatiga/atención de los encuestados.
Como conclusiones, señalamos que las políticas sanitarias de administración profiláctica de vitamina D en el primer año de vida son bastante homogéneas en nuestro territorio, bien conocidas y el cumplimiento es considerado bueno. Por otro lado, hasta un 57,2% de los pediatras españoles buscan de manera activa la deficiencia de vitamina D en algunos de sus pacientes, aunque no exista evidencia en muchos casos para sustentarlo.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. El trabajo se ha presentado de forma parcial y muy resumida como comunicación oral en el Congreso de la Sociedad Española de Endocrinología Pediátrica realizado en mayo de 2022 en Oviedo.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: desarrollo del protocolo, investigación y redacción del texto (DSE), desarrollo del protocolo y del original para su publicación (el resto de los autores).
El estudio ha sido aprobado por el Comité de Ética e Investigación de las Islas Baleares (CEI IB 4510/21PI). Se han respetado las condiciones de la Ley de Protección de Datos, siendo los investigadores los únicos que han tenido acceso a los mismos con el único fin de este estudio.
AGRADECIMIENTOS
A Oana Bulilete, por su ayuda con el enfoque de la investigación y el trabajo estadístico.
BIBLIOGRAFÍA
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266-81.
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, Ozono K, et al. Global consensus recommendations on prevention and management of nutritional rickets. J Clin Endocrinol Metab. 2016;101:394-415.
- Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M. Drug and therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398-417.
- Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-30.
- Saggese G,Vierucci F, Prodam F, Cardinale F, Cetin I, Chiappini E, et al. Vitamin D in pediatric age: consensus of the Italian Pediatric Society ant the Italian Society of Preventive and Social Pediatrics,jointly with the Italian Federation of Pediatricians. Ital J Pediatr. 2018;44:51.
- Yeste D, Carrascosa A, Grupo Interhospitalario para el estudio del Raquitismo Carencial en Cataluña (GIERCC). Raquitismo carencial en la infancia: análisis de 62casos [Nutritional rickets in childhood: analysis of 62 cases]. Med Clin (Barc). 2003;121:23-7.
- Sánchez Muro JM, Yeste Fernández D, Marín Muñoz A, Fernández Cancio M, Audí Parera l, Carrascosa Lezcano A. Niveles plasmáticos de vitamina D en población autóctona y en poblaciones inmigrantes de diferentes etnias menores de 6 años de edad. An Pediatr (Barc). 2015:316-24.
- Atapattu N, Shaw N, Högler W. Relationship between serum 25-hydroxyvitamin D and parathyroid hormone in the search for a biochemical definition of vitamin D deficiency in children. Pediatr Res. 2013;74:552-6.
- Maguire JL, Birken C, Thorpe KE, Sochett EB, Parkin PC. Parathyroid hormone as a funtional indicator of vitamin D sufficiency in children. JAMA Pediatr. 2014;168:383-5.
- Abrams SA, Hicks PD, Hawthorne KM. Higher serum 25-hydroxivitamin D levels in school-age children are inconsistently associated with increased calcium absorption. J Clin Endocrinol Metab. 2009;94:2421-7.
- Golden NH, Abrams SA; Committee on Nutrition. Optimizing bone health in children and adolescents. Pediatrics. 2014;134:e1229-43.
- Fu Y, Hu Y, Quin Z, Zhao Y, Yang Z, Li Y, et al. Association of serum 25-hydroxivitamin D status with bone mineral density in 0-7 year-old children. Oncotarget. 2016;7:80811-9.
- Martínez Suárez V, Moreno Villares JM, Dalmau Serra J, Comité de Nutrición de la Asociación Española de Pediatría. Recomendaciones de ingesta de calcio y vitamina D: posicionamiento del Comité de Nutrición de la Asociación Española de Pediatría. An Pediatr (Barc). 2012;77:57.e1-8.
- De Sotto Esteban D, Ursina B, Ferrés l, Torbado P, Yáñez AM. Niveles de vitamina D y factores de riesgo asociados en recién nacidos sanos de Mallorca. Rev Esp Endocrinol Pediatr. 2015;6:51-60.
- Rodríguez-Rodríguez E, Aparicio A, López-Sobaler AM, Ortega RM. Vitamin D status in a group of Spanish schoolchildren. Minerva Pediatr. 2011;63:11-18.
- Togo A, Espadas Maciá D, Blanes Segura S, Sivó Díaz N, Villalba Martínez C ¿Existe déficit de vitamina D en los niños de una ciudad soleada en el Mediterráneo? An Pediatr (Barc). 2016;84:163-9.
- Fernández Bustillo JM, Fernández Pombo A, Gómez Bahamonde R, Sanmartín López E, Gualillo O. Vitamin D levels in a pediatric population of a primary care centre: a public health problem? Nutr Hosp. 2015;32:1061-6.
- Ruiz Ocaña P, Carrasco Fernández C, Zopeque García N, Sáez Benito A, Novalbos Ruiz JP, Lechuga Sancho AM. Niveles de vitamina D al final de la estación invernal en una población escolar sana. Rev Esp Endocrinol Pediatr. 2014;5:19-27.
- Martínez Redondo I, García Romero R, Calmarza P, De Arriba Muñoz A, Rodríguez,Martínez G, Labarta Aizpún JI. Deficiencia de vitamina D en niños aragoneses sanos. Nutr Hosp. 2018;35:782-8.
- Rodríguez-Dehli AC, Riaño-Galán I, Fernández-Somoano A, Navarrete-Muñoz EM, Espada M, Vioque J, et al. Hipovitaminosis D y factores asociados a los 4 años en el norte de España. An Pediatr (Barc). 2017;86:188-96.
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Ross AC, Taylor CL, Yaktine AL, Del Valle HB (Eds.). Dietary reference intakes for calcium and vitamin D. Committee to review dietary reference intakes for calcium and vitamin D. Washington: National Academ Press; 2011 [en línea] [consultado el 09/03/2023]. Disponible en www.ncbi.nlm.nih.gov/books/NBK56070/
- Golden NH, Abrams SA. Committee on Nutrition. Optimizing bone health in children and adolescents. Pediatrics. 2014;134:e1229-43.
- Pallás Alonso C, Ureta Velasco N, Alonso Díaz C; PAPPS Infancia y Adolescencia de semFYC. Suplementación de vitamina D en la infancia. Aten Primaria. 2012;44:682-3.
- Piñeiro Pérez R, Núñez Cuadros E, Cabrera García l, Díez López I, Escrig Fernández R, Gil Lemus MA, et al. (Comité de Medicamentos de la AEP). Resultados de una encuesta nacional sobre conocimiento y uso de pseudociencias por parte de los pediatras. An Pediatr (Barc). 2022;96:25-34.
- Uday S, Kongjonag A, Aguiar M, Tulchinsky T, Högler W. Variations in infant and childhood vitamin D supplementation programs across Europe and factors influencing adherence. Endocr Connect. 2017;6:667-75.
- Cabezuelo Huerta G, Vidal Micó S, Abeledo Gómez A, Frontera Izquierdo P. Niveles de vitamina D en lactantes. Relación con la lactancia materna. An Pediatr (Barc). 2007;66:491-5.
- Durá Travé T, Gallinas Victoriano F, Chueca Guindulain MJ, Berrade Zubiri S, Moreno Gónzalez P, Malumbres Chacón M. Prevalencia de hipovitaminosis D y factores asociados en la edad infantojuvenil. Aten Primaria. 2018;50:422-9.
- Gutiérrez Medina S, Gavela Pérez T, Domínguez Garrido MN, Blanco Rodríguez M, Gracés C, Rovira A, et al. Elevada prevalencia de déficit de vitamina D entre los niños y adolescentes obesos españoles. An Pediatr (Barc). 2014;80:229-35.
- Rodríguez Rodríguez E, Aparicio A, Andrés P, Ortega RM. Moderate vitamin D deficiency and inflammation related markers in overweight/obese schoolchildren. Int J Vitam Nutr Res. 2014;84:98-107.
- Barceló A, Morell García D, Ribot C, De la Peña M, Peña Zarza JA, Alonso Fernández A, et al. Vitamin D as a biomarker of health in snoring children: a familial aggregation study. Pediatr Res. 2022;91:1176-81.
- Barja Fernández S, Aguilera CM, Martínez Silva I, Vázquez R, Gil Campos M, Olza J, et al. 25-hydroxyvitamin D levels of children are inversely related to adiposity assessed by body mass index. J Physiol Biochem. 2018;74:111-8.
- Segovia Ortí R, Barceló A, De Sotto Esteban D, Sanchís P, Pons J. Association between vitamin D status and allergen sensitization in pediatric subjects in the Balearic Islands. Pediatr Allergy Immunol. 2021;32:1183-9.
- Rey C, Sánchez Arango D, López Herce J, Martínez Camblor P, García Hernández I, Prieto B, et al. Vitamin D deficiency at pediatric intensive care admission. J Pediatr (Rio J). 2014;90:135-42.
- Cebey López M, Pardo Seco J, Gómez Carballa A, Martinón Torres N, Rivero Calle I, Justicia A, et al. Role of vitamin D in hospitalized children with lower tract acute respiratory infections. J Pediatr Gastroenterol Nutr. 2016;62:479-85.
- Sanmartín R, Pardos C, Doste D, Aguilera J, Alijarde R, Agón Banzo PJ, et al. The association between atopic dermatitis and serum 25-hydroxyvitamin D in children: Influence of sun exposure, diet, and atopy features-A cross-sectional study. Pediatr Dermatol. 2020;37:294-300.
- Garrido C, Cela E, Beléndez C, Mata C, Huerta J. Status of vitamin D in children with sickle cell disease living in Madrid, Spain. Eur J Pediatr. 2012;171:1793-8.
- Durá Travé T, Gallinas Victoriano F, Malumbres Chacón M, Moreno Gónzalez P, Aguilera Albesa S, Yoldi Petri ME. Vitamin D deficiency in children with epilepsy taking valproate and levetiracetam as monotherapy. Epilepsy Res. 2018;139:80-4.
- Martínez Suarez V, Dalmau Serra J. Hipovitaminosis D ¿una epidemia real? Pediatr Integral. 2020;24:351-5.
- Mengual Gil JM. Vitamina D por encima del año de vida, ¿es necesaria o está de moda? En: AEPap (ed.). Curso de Actualización Pediatría 2018. Madrid: Lúa Ediciones 3.0; 2018. p. 17-30 [en línea] [consultado el 09/03/2023]. Disponible en www.aepap.org/sites/default/files/017-030_vitamina_d_por_encima_del_ano.pdf.
- Baccheta J, Edouard T, Laverny G, Bernardor J, Bertholet Thomas A, Castanet M, et al. Vitamin D and calcium intakes in general pediatric populations: A French expert consensus paper. Arch Pediatr. 2022;29:312-25.