
Vol. 24 - Num. 96
Originales
Factores asociados al sueño nocturno de los adolescentes
Raúl Jiménez Boraitaa, Daniel Arriscado Alsinab, Josep M.ª Dalmau Torresc, Esther Gargallo Ibortc
aProfesor. Universidad Isabel I. Burgos. Universidad Internacional de La Rioja. Logroño. España.
bProfesor. Universidad Isabel I. Burgos. España.
cProfesor. Universidad de La Rioja. Logroño. España.
Correspondencia: R Jiménez. Correo electrónico: raul.jimenez@unir.net
Cómo citar este artículo: Jiménez Boraita R, Arriscado Alsina D, Dalmau Torres JM, Gargallo Ibort E. Factores asociados al sueño nocturno de los adolescentes . Rev Pediatr Aten Primaria. 2022;24:375-84.
Publicado en Internet: 10-11-2022 - Número de visitas: 12938
Resumen
Introducción: durante la adolescencia se producen numerosos cambios en los hábitos de vida que afectan también a los patrones de sueño; patrones que son clave en el desarrollo de los jóvenes y en su estado de salud. Por ello, el objetivo del estudio fue analizar la relación e influencia de diversos hábitos de vida, indicadores de salud física y psicosocial, y variables sociodemográficas sobre la duración del sueño nocturno.
Material y métodos: el estudio se llevó a cabo sobre una muestra de 761 estudiantes (14,51 ± 1,63 años) de 25 centros educativos de una región del norte de España. Se valoró el número de horas de sueño nocturno, así como la adherencia a la dieta mediterránea, nivel de actividad física, calidad de vida relacionada con la salud, autoestima, consumo máximo de oxígeno, índice de masa corporal, rendimiento académico y diversos factores sociodemográficos.
Resultados: tener mayor edad e índice de masa corporal, así como una menor adherencia a la dieta mediterránea y estudiar en centros de zonas urbanas fueron predictores de un menor número de horas de sueño nocturno, llegando a explicar el 26,2% de su varianza. Asimismo, los adolescentes que no cumplían con las recomendaciones de sueño nocturno presentaron menores índices de calidad de vida relacionada con la salud y autoestima, así como niveles más bajos de actividad física y consumo máximo de oxígeno.
Conclusiones: las intervenciones dirigidas a la prevención de los trastornos del sueño deberían tener en cuenta los factores predictores citados, orientando los esfuerzos hacia el fomento de hábitos saludables y entornos propicios para el descanso, especialmente, en zonas urbanas.
Palabras clave
● Adolescente ● Bienestar ● Hábitos de vida ● Salud ● SueñoINTRODUCCIÓN
El sueño es definido como un estado fisiológico que se caracteriza por ser reversible, transitorio y periódico, siendo una función necesaria para la vida y uno de los hábitos de mayor influencia en la salud1. Las recomendaciones establecidas para la población de entre 13 y 18 años se centran en el cumplimento de un sueño nocturno de entre 8 y 10 horas2. No obstante, es en esta etapa donde su regulación resulta más complicada3.
La insuficiencia en la calidad y duración del sueño nocturno en la población juvenil se ha consolidado como una preocupación incipiente en Salud Pública4. La dificultad para su conciliación en adolescentes muestra una tendencia ascendente. Según el estudio internacional Health Behaviour in School-aged Children, alrededor del 24% de los mismos sufren problemas vinculados con el sueño5. En el caso de España, el 51,3% de los adolescentes duermen menos horas de las recomendadas durante los días lectivos y el 44,6%, durante los fines de semana, según los resultados ofrecidos por el Informe Pasos6. No obstante, los patrones de sueño parecen variar notablemente en función del país y de otros aspectos sociodemográficos, como el nivel económico familiar o la edad4.
Estudios previos han demostrado que el sueño tiene una implicación clave en la salud general de la población, especialmente durante la etapa infanto-juvenil, donde el incumplimiento de las recomendaciones puede desencadenar graves consecuencias en el presente y futuro7. En este sentido, la literatura ha demostrado su interacción con otros hábitos de vida, como la actividad física (AF) o la conducta alimentaria8,9. Además, los patrones de sueño también se han vinculado a diversos aspectos de la salud física y psicológica, relacionándose con la salud emocional, cognitiva y social10, así como con la salud cardiometabólica11 y diferentes trastornos mentales como la ansiedad o la depresión12.
La eficacia de las intervenciones dirigidas a la mejora de los hábitos de sueño en la población adolescente parece tener efectos positivos en su salud general13. En este sentido, el entorno educativo tiene un papel clave en su promoción debido a las posibilidades de accesibilidad y transmisión de valores positivos relacionados con su comportamiento, conocimiento e higiene14. Asimismo, la promoción de unos hábitos de sueño saludables en etapas previas a la adultez resulta primordial, ya que las alteraciones de este hábito padecidas durante la adolescencia influyen de manera directa sobre los trastornos del sueño en etapas posteriores15.
El conocimiento desde una perspectiva global de los factores asociados al sueño nocturno podría ser de especial relevancia para la prevención y promoción de la salud adolescente. Por ello, el presente estudio examina el sueño nocturno en una muestra representativa de adolescentes, analizando la influencia de diversos indicadores de salud física y psicosocial, de sus hábitos de vida y de diversos factores sociodemográficos. Para ello, se valoró la duración del sueño nocturno, el nivel de AF, la adherencia a la dieta mediterránea (DM), la calidad de vida relacionada con la salud (CVRS), la autoestima, el índice de masa corporal (IMC), el consumo máximo de oxígeno (VO2max) y el rendimiento académico, además de los citados factores sociodemográficos.
MATERIAL Y MÉTODOS
Diseño de estudio y participantes
Se llevó a cabo un estudio transversal con una muestra representativa de adolescentes de primero y cuarto curso de Educación Secundaria Obligatoria (ESO) de los centros educativos de La Rioja, una región al norte de España. Para su selección, se realizó un muestreo por conglomerados monoetápico, considerando como unidades de muestreo las aulas correspondientes a los citados cursos. Con el fin de lograr la representatividad en ambos cursos y teniendo en cuenta la población (3470 escolares en 1.º de ESO y 2548 en 4.º de ESO), se estableció un intervalo de confianza del 95%, un nivel de precisión del 5% y una proporción de la población del 50%. Con estos parámetros, la representatividad se alcanzaba con 346 y 334 estudiantes de primero y cuarto curso, respectivamente. Considerando que la media de alumnos por aula era de 25 en ambos casos y estimando una participación del 60%, se aumentaron en correspondencia las cifras expuestas, seleccionando de forma aleatoria 23 aulas de primer curso y 22 de cuarto. Se invitó a participar en el estudio a todos los alumnos de las aulas seleccionadas y, dado que la tasa de aceptación fue del 82%, la muestra final estuvo formada por 761 adolescentes de 45 aulas de 25 centros educativos, perteneciendo 383 al primer curso y 378 al cuarto. Sus edades se comprendieron entre los 12 y los 17 años (14,51 ± 1,63 años), siendo un 50,3% chicos y 49,7% chicas.
Previamente a dicha participación, se solicitó el consentimiento informado por escrito de los padres o tutores legales de los estudiantes. Del mismo modo, la colaboración de estos en la investigación fue voluntaria y consentida de forma verbal. Se respetaron los fundamentos éticos de la Declaración de Helsinki y el proyecto fue aprobado por el Comité Ético de Investigación Clínica de La Rioja, llevándose a cabo el trabajo de campo para la recolección de datos entre enero y junio de 2018.
Variables
El número de horas de sueño nocturno se estimó a través de dos preguntas vinculadas a la hora en la que se acostaban y se despertaban normalmente durante los días laborales de la semana. La duración del sueño nocturno se calculó en función de la diferencia de horas entre las respuestas definidas por los participantes en ambas preguntas. Una vez computado el cálculo, se agrupó al alumnado en función de las recomendaciones de la American Academy of Sleep Medicine2 para la población adolescente: “cumple”, si dormían 8 o más horas, y “no cumple” para valores inferiores.
La adherencia a la DM se analizó a través del cuestionario KIDMED16. El mismo consta de dieciséis ítems de carácter dicotómico (sí o no) relacionados con el consumo de alimentos asociados a un patrón dietético mediterráneo. La puntuación general se sitúa entre menos cuatro y doce, y los valores más altos indican una mayor adherencia a la DM.
El nivel de AF se estimó con el cuestionario Physical Activity Questionnaire for Adolescents, validado en adolescentes españoles17. El instrumento consta de nueve ítems que valoran la AF realizada durante los últimos siete días. La puntuación final se comprende entre uno y cinco, siendo las puntuaciones más altas las que representan un mayor nivel de AF. Además, el cuestionario añade una décima pregunta que permite descartar a los participantes que no han podido realizar su AF habitual en los citados siete días debido a una enfermedad, lesión o cualquier otro motivo. No obstante, ningún participante se vio afectado por esta circunstancia.
La valoración de la CVRS se realizó con el cuestionario KIDSCREEN-27, validado en adolescentes españoles18. Se compone de 27 ítems de tipo Likert agrupados en cinco dimensiones: bienestar físico, bienestar psicológico, autonomía y relación con los padres, entorno escolar, y apoyo social y pares. Para el cálculo de la puntuación final se siguieron las instrucciones indicadas por los autores del cuestionario, siendo los valores más altos los vinculados a una percepción de calidad de vida más positiva.
La autoestima se evaluó con la escala de Rosenberg validada en adolescentes españoles19. Este instrumento consta de diez ítems con respuestas calificadas de uno a cuatro que valoran el grado de satisfacción de una persona hacía ella misma. La puntuación final contiene valores comprendidos entre diez y cuarenta, donde los más altos son los asociados a una mayor autoestima.
En cuanto a los datos sociodemográficos, los participantes informaron de su sexo, fecha de nacimiento y nacionalidad (nacido en España o en otro país). El tipo de localidad de los centros educativos (urbana o rural) se determinó en función del número de habitantes, considerando a aquellas con más de 5000 como municipios urbanos. Por su parte, el nivel socioeconómico (NSE) se valoró con el cuestionario Family Affluence Scale (FAS II), compuesto por cuatro preguntas relacionadas con la posesión familiar de bienes materiales20. La puntuación final se comprende entre cero y nueve, categorizando los resultados del siguiente modo: bajo (≤2), medio (3-5) o alto (≥6). Para el tratamiento de los datos se agrupó a aquellos que informaron un NSE bajo (1,8%) y medio (28%), debido al bajo porcentaje de los primeros.
Además, con el fin de detectar y excluir del análisis los cuestionarios realizados de modo aleatorio, deshonesto o pseudoaleatorio, se utilizó la Escala Oviedo de Infrecuencia de Respuesta, formada por preguntas de respuesta elemental y dicotómico (sí o no)21. Se introdujeron intercaladamente seis de estas preguntas a lo largo del cuestionario (por ejemplo, “¿Has visto alguna vez una película en la televisión?”). Los participantes que respondieron en más de una ocasión de forma contraria a la lógica fueron excluidos del análisis. Concretamente, dos sujetos se vieron afectados por esta circunstancia.
La evaluación de la capacidad cardiorrespiratoria (CCR) se realizó con el test de ida y vuelta de 20 metros22. En el mismo se delimitan dos líneas trasversales a una distancia de 20 metros que indican el inicio y final del recorrido. Los participantes deben mantener el ritmo de carrera de acuerdo con el ritmo establecido por una señal acústica, que marca el tiempo disponible para recorrer la distancia entre ambas líneas de forma sucesiva. La velocidad inicial de carrera es de 8,5 km/h, aumentando en 0,5 km/h cada minuto. La prueba finaliza cuando los participantes se detienen o no completan el recorrido en el ritmo establecido en dos ocasiones consecutivas. Posteriormente, con los resultados obtenidos, se calculó el VO2max mediante la fórmula estipulada por el autor de la prueba.
La determinación de la altura y el peso se realizó a través de un tallímetro Holtain® (Holtain Ltd., Dyfed, Reino Unido) con una precisión de un milímetro y una balanza SECA® (713, Hamburg, Alemania) con una precisión de 0,1 kg, respectivamente. Una vez tomadas las medidas, se calculó el índice de masa corporal (IMC).
El rendimiento académico se valoró a través de las calificaciones de los escolares proporcionadas por la Consejería de Educación del Gobierno de La Rioja, siendo determinado por la nota media obtenida en el curso en que se llevó a cabo el estudio. Previamente, se solicitó el consentimiento expreso de las familias participantes, obteniendo la autorización del 90% de las mismas.
Análisis estadístico
Las variables cuantitativas se presentan en función de sus medias y desviaciones típicas, mientras que las variables cualitativas se presentan según sus frecuencias. La normalidad y la homocedasticidad de los datos fueron analizadas con la prueba de Kolmogorov-Smirnov y Levene, respectivamente. El contraste de medias se realizó con la prueba T de Student para variables con distribución normal y U de Mann-Whitney para aquellas con distribución no normal. Por su parte, se utilizó el test Chi-cuadrado de Pearson para el análisis de asociación entre las variables cualitativas.
Para identificar posibles predictores de las horas de sueño nocturno, se realizó una regresión lineal múltiple utilizando el método de eliminación hacia atrás. Las variables incluidas en el modelo fueron: sexo, nacionalidad, nivel socioeconómico, localización del centro escolar, CVRS, autoestima, adherencia a la DM, nivel de AF, VO2max e IMC. El análisis estadístico se realizó mediante el programa IBM-SPSS® en su versión 25 para Windows, estableciendo la significación estadística en p <0,05.
RESULTADOS
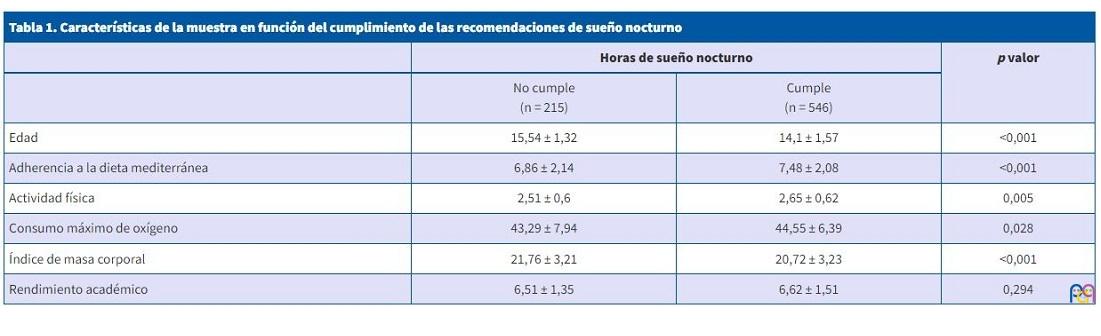
El 28,2% de los adolescentes no cumplían con las recomendaciones de sueño nocturno. La edad, adherencia a la DM, nivel de AF, VO2max, IMC y rendimiento académico de los adolescentes en función del cumplimento de las recomendaciones del sueño nocturno se muestran en la Tabla 1. El análisis reveló que los adolescentes que cumplían las recomendaciones presentaron valores significativamente superiores de adherencia a la DM, el nivel de AF y el VO2max, mientras que la edad y el IMC fueron menores.
| Tabla 1. Características de la muestra en función del cumplimiento de las recomendaciones de sueño nocturno | |||
|---|---|---|---|
| Horas de sueño nocturno | p valor | ||
| No cumple (n = 215) |
Cumple (n = 546) |
||
| Edad | 15,54 ± 1,32 | 14,1 ± 1,57 | <0,001 |
| Adherencia a la dieta mediterránea | 6,86 ± 2,14 | 7,48 ± 2,08 | <0,001 |
| Actividad física | 2,51 ± 0,6 | 2,65 ± 0,62 | 0,005 |
| Consumo máximo de oxígeno | 43,29 ± 7,94 | 44,55 ± 6,39 | 0,028 |
| Índice de masa corporal | 21,76 ± 3,21 | 20,72 ± 3,23 | <0,001 |
| Rendimiento académico | 6,51 ± 1,35 | 6,62 ± 1,51 | 0,294 |
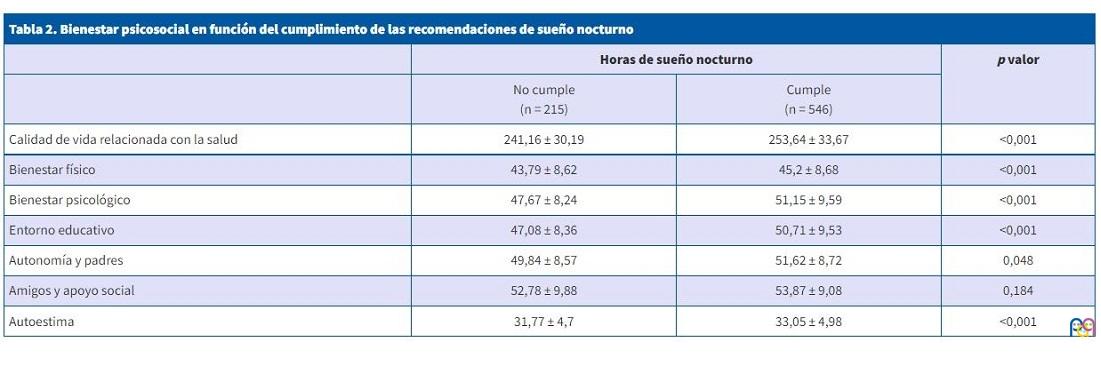
La Tabla 2 recoge los resultados de la autoestima y la CVRS, así como de sus cinco dimensiones en función del cumplimiento de las recomendaciones de sueño nocturno. Los adolescentes que cumplían con las mismas presentaron valores significativamente superiores tanto en la autoestima y el cómputo global de la CVRS como en todas sus dimensiones, excepto en “amigos y apoyo social”, donde no existieron diferencias.
| Tabla 2. Bienestar psicosocial en función del cumplimiento de las recomendaciones de sueño nocturno | |||
|---|---|---|---|
| Horas de sueño nocturno | p valor | ||
| No cumple (n = 215) |
Cumple (n = 546) |
||
| Calidad de vida relacionada con la salud | 241,16 ± 30,19 | 253,64 ± 33,67 | <0,001 |
| Bienestar físico | 43,79 ± 8,62 | 45,2 ± 8,68 | <0,001 |
| Bienestar psicológico | 47,67 ± 8,24 | 51,15 ± 9,59 | <0,001 |
| Entorno educativo | 47,08 ± 8,36 | 50,71 ± 9,53 | <0,001 |
| Autonomía y padres | 49,84 ± 8,57 | 51,62 ± 8,72 | 0,048 |
| Amigos y apoyo social | 52,78 ± 9,88 | 53,87 ± 9,08 | 0,184 |
| Autoestima | 31,77 ± 4,7 | 33,05 ± 4,98 | <0,001 |
La Tabla 3 recoge la influencia de algunos factores sociodemográficos sobre el cumplimiento de dichas recomendaciones. Únicamente se hallaron diferencias significativas en función de la localización del centro escolar, donde las tasas de incumplimiento eran mayores por parte de los adolescentes que estudiaban en centros de zonas urbanas.
| Tabla 3. Cumplimiento de las recomendaciones de sueño nocturno en función de diferentes factores | ||||||
|---|---|---|---|---|---|---|
| Horas de sueño nocturno | p valor | |||||
| No cumple (n = 215) |
Cumple (n = 546) |
|||||
| N | % | N | % | |||
| Nacionalidad | Españoles | 182 | 29,4% | 436 | 70,6% | 0,127 |
| Migrantes | 33 | 23,1% | 110 | 76,9% | ||
| Sexo | Chicos | 109 | 28,5% | 274 | 71,5% | 0,898 |
| Chicas | 106 | 28% | 272 | 72% | ||
| Nivel socioeconómico | Bajo/Medio | 67 | 29,5% | 160 | 70,5% | 0,614 |
| Alto | 148 | 27,7% | 386 | 72,3% | ||
| Localización del centro escolar | Urbano | 192 | 29,5% | 458 | 70,5% | 0,034 |
| Rural | 23 | 20,7% | 88 | 79,3% | ||

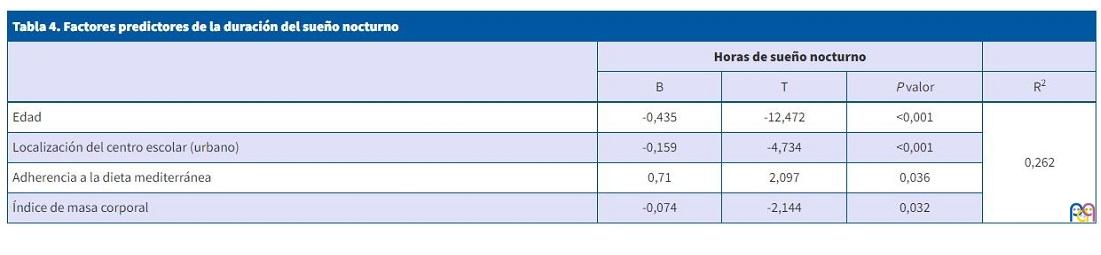
Finalmente, en la Tabla 4 se presenta el modelo de regresión lineal múltiple para el número de horas de sueño nocturno. Tener mayor edad e IMC, así como una menor adherencia a la DM y estudiar en centros de zonas urbanas fueron factores predictores de un menor número de horas de sueño nocturno, llegando a explicar hasta un 26,2% de la varianza del mismo.
| Tabla 4. Factores predictores de la duración del sueño nocturno | ||||
|---|---|---|---|---|
| Horas de sueño nocturno | ||||
| B | T | P valor | R2 | |
| Edad | -0,435 | -12,472 | <0,001 | 0,262 |
| Localización del centro escolar (urbano) | -0,159 | -4,734 | <0,001 | |
| Adherencia a la dieta mediterránea | 0,71 | 2,097 | 0,036 | |
| Índice de masa corporal | -0,074 | -2,144 | 0,032 | |
DISCUSIÓN
Los resultados obtenidos en el estudio mostraron que el 28,2% de los participantes no cumplían con las recomendaciones de sueño establecidas para la población adolescente, tasas inferiores a las halladas en un estudio previo de corte nacional6.
El sueño nocturno se asoció con diversos indicadores de salud física y psicosocial, hábitos de vida y variables sociodemográficas, pudiendo establecerse factores predictores.
La edad fue uno de ellos, siendo los adolescentes mayores los que presentaron menos horas de sueño nocturno. El estudio de Mazzer (2019)23 confirma esta tendencia descendente en la duración del sueño a medida que aumenta la edad de los adolescentes, reflejándose asimismo en un aumento en la prevalencia de casos asociados a la angustia psicológica. En esta línea, resulta significativa la frecuencia de problemas vinculados con el sueño entre los adolescentes, cuestión que manifiesta una persistencia durante la edad adulta15 y que puede estar relacionada con un mayor uso e influencia de las redes sociales y pantallas, así como con carencias en la estructura de un horario semanal a medida que aumenta la edad de los jóvenes24,25.
La localización también mostró su valor predictor en las horas de sueño nocturno, siendo los adolescentes que acudían a centros de zonas urbanas los que mostraron menores tasas de cumplimento de las recomendaciones. La residencia en entornos con mayores niveles de urbanización ha demostrado asociarse con una menor calidad, duración y regularidad del sueño en adolescentes26. Componentes relacionados a diversas cuestiones físicas y sociales (densidad de población o disponibilidad de zonas verdes), a aspectos vinculados al vecindario (seguridad, orden y relaciones sociales) o a factores de índole ambiental (contaminación del aire, ruido o exposición a la luz artificial), parecen tener un efecto clave en los hábitos del sueño27.
Los adolescentes con mayor IMC presentaron menor número de horas de sueño nocturno, confirmándose como otro factor predictor. La asociación entre el sueño y la obesidad ha sido corroborada ampliamente en la literatura previa, demostrando la determinante influencia que tienen los hábitos de sueño sobre la composición corporal28. La evidencia científica señala el aumento del IMC como un factor de riesgo en trastornos como la apnea obstructiva del sueño29, lo que podría conllevar dificultades respiratorias que den lugar a una hipoxemia intermitente, mayor somnolencia diurna o/y calidad del sueño30. El aumento de tejido adiposo también parece vincularse a diferentes mecanismos biológicos que parecen influir de forma directa en el sueño31.
Por último, en relación con los hábitos de vida, la DM también fue un factor predictor, de modo que aquellos adolescentes con menor adherencia a la misma reportaron un menor número de horas de sueño nocturno. La DM ha demostrado asociarse positivamente con el sueño tanto de forma directa como a través de la mejora de la composición corporal32. El consumo de verduras y frutas parece ejercer un efecto positivo en el sueño debido al contenido de polifenoles, los cuales tienen una influencia directa en mecanismos biológicos como el ritmo circadiano33. Asimismo, una corta duración del sueño se vincula con un mayor consumo de bocadillos, comida rápida, refrescos, así como con una menor ingesta de frutas y frutos secos34.
Además de los factores predictores descritos anteriormente, el sueño nocturno presentó asociaciones con otras variables sociodemográficas, indicadores relacionados con la salud física y hábitos de vida.
En relación con la salud psicosocial, tanto la autoestima como la calidad de vida percibida (en su puntuación global y en cuatro de las cinco dimensiones que la conforman), presentaron índices más bajos los adolescentes que no cumplían con las recomendaciones. La falta del sueño parece afectar al bienestar físico, puesto que genera una mayor prevalencia de síntomas como dolores de cabeza, fatiga y mareos35. Hay estudios que confirman la asociación entre la duración del sueño y el bienestar mental de los adolescentes36, de modo que cuanto menor es la duración, mayor es la probabilidad de sufrir trastornos mentales37, así como una peor percepción del clima familiar38.
Los patrones de sueño inadecuados constituyen un factor determinante en el agotamiento escolar de los adolescentes39, que podría justificar en parte los resultados obtenidos en relación con el bienestar escolar.
El nivel de AF fue menor en los adolescentes que no cumplían las recomendaciones de sueño nocturno y, en este sentido, la literatura advierte de que una mayor realización de ejercicio físico genera mayores probabilidades de tener una mejor calidad de sueño40. Además, la AF realizada a intensidad moderada o vigorosa se vincula con una mayor eficiencia y duración de dicho sueño41, aunque existen diferentes aspectos mediadores, como los trastornos mentales42 o la mejora de elementos electrofisiológicos y bioquímicos del sueño asociados al ejercicio aeróbico43.
Los valores de consumo máximo de oxígeno también fueron menores en los adolescentes que no cumplían las recomendaciones de sueño nocturno, lo que podría ser consecuencia de los menores niveles de actividad física anteriormente mencionados44. En este sentido, la asociación entre los estilos de vida y la capacidad cardiorrespiratoria es manifiesta, existiendo estudios que asocian peores hábitos del sueño con una capacidad cardiorrespiratoria más baja45 y un mayor riesgo cardiometabólico46.
La obtención de una muestra representativa de adolescentes es una de las fortalezas del presente estudio, posibilitando valorar la vinculación de las horas de sueño nocturno con otros hábitos de vida, diferentes variables sociodemográficas e indicadores de salud física y psicosocial. En este sentido, la valoración del sueño a través de un polisomnograma o el uso de acelerómetros serían cuestiones a considerar como prospectiva. En cualquier caso, los instrumentos utilizados han mostrado su fiabilidad y validez en estudios previos con muestras de similares características. Asimismo, el diseño trasversal del estudio no permitió valorar la causalidad de los resultados, por lo que la realización de futuros estudios de corte longitudinal podría complementar las conclusiones obtenidas.
CONCLUSIÓN
Tener mayor edad e IMC, así como una menor adherencia a la DM y estudiar en centros de zonas urbanas fueron predictores de un menor número de horas de sueño nocturno, llegando a explicar el 26,2% de su varianza. Los adolescentes que no cumplían con las recomendaciones de sueño nocturno presentaron menores índices de autoestima y CVRS (en su puntuación global y en la de la mayoría de sus dimensiones), así como niveles más bajos de AF y VO2max. Las asociaciones encontradas ponen de manifiesto la necesidad de abordar las intervenciones dirigidas a la prevención de los trastornos del sueño desde una perspectiva interdisciplinar. En este sentido, la promoción de espacios urbanos más propicios para el descanso, así como el impulso de la práctica de AF y la adherencia a patrones dietéticos saludables podrían redundar de forma positiva tanto en la cantidad como en la calidad del sueño y, por ende, en la salud en general de los adolescentes, especialmente en la de los mayores y los residentes en zonas urbanas.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
FINANCIACIÓN
El estudio fue parcialmente financiado por el Instituto de Estudios Riojanos (IER) del Gobierno de La Rioja a través de la “Resolución n.º 55/2018, de 9 de julio, de la gerencia del instituto de estudios riojanos para la concesión de ayudas para estudios científicos de temática riojana convocadas para el año 2018-2019'.
ABREVIATURAS
AF: actividad física · CCR: capacidad cardiorrespiratoria · CVRS: calidad de vida relacionada con la salud · DM: dieta mediterránea · ESO: Educación Secundaria Obligatoria · FAS II: cuestionario Family Affluence Scale · IMC: índice de masa corporal · NSE: nivel socioeconómico · VO2max: consumo m2áximo de oxígeno.
BIBLIOGRAFÍA
- Kryger M, Roth T, Dement W. Principles and practice of sleep medicine. 5th ed. St. Louis, MI: Elsevier Saunders; 2011.
- Paruthi S, Brooks LJ, D'Ambrosio C, Hall WA, Kotagal S, Lloyd RM, et al. Recommended amount of sleep for pediatric populations: a consensus statement of the American Academy of Sleep Medicine. J Clin Sleep Med. 2016;12:785-6.
- Crowley SJ, Wolfson AR, Tarokh l, Carskadon MA. An update on adolescent sleep: New evidence informing the perfect storm model. J Adolesc. 2018;67:55-65.
- Gariepy G, Danna S, Gobiņa I, Rasmussen M, De Matos MG, Tynjälä J, et al. How are adolescents sleeping? Adolescent sleep patterns and sociodemographic differences in 24 European and North American countries. J Adolesc Health. 2020;66:81-8.
- Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A, et al. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Copenhagen; 2020. En: Organización Mundial de la Salud [en línea] [consultado el 10/10/2022]. Disponible en https://apps.who.int/iris/handle/10665/332104
- Resultados principales del estudio PASOS 2019 sobre la actividad física, los estilos de vida y la obesidad de la población española de 8 a 16 años. Sant Boi de Llobregat, España. En: Gasol Foundation; 2019 [en línea] [consultado el 10/10/2022]. Disponible en https://www.gasolfoundation.org/es/estudio-pasos/
- Owens JA, Weiss MR. Insufficient sleep in adolescents: causes and consequences. Minerva Pediat. 2017;69:326-36.
- Fenton S, Burrows TL, Skinner JA, Duncan MJ. The influence of sleep health on dietary intake: a systematic review and meta-analysis of intervention studies. J Hum Nutr Diet. 2020;34:273-85.
- Atoui S, Chevance G, Romain AJ, Kingsbury C, Lachance JP, Bernard P. Daily associations between sleep and physical activity: A systematic review and meta-analysis. Sleep Med Rev. 2021;57:101426.
- Dong l, Martinez AJ, Buysse DJ, Harvey AG. A composite measure of sleep health predicts concurrent mental and physical health outcomes in adolescents prone to eveningness. Sleep Health. 2019;5:166-74.
- Cespedes EM, Quante M, Rifas-Shiman SL, Redline S, Oken E, Taveras EM. Objective sleep characteristics and cardiometabolic health in young adolescents. Pediatrics. 2018;142:e20174085.
- Berger AT, Wahlstrom KL, Widome R. Relationships between sleep duration and adolescent depression: a conceptual replication. Sleep Health. 2019;5:175-9.
- Blake MJ, Blake LM, Schwartz O, Raniti M, Waloszek JM, Murray G, et al. Who benefits from adolescent sleep interventions? Moderators of treatment efficacy in a randomized controlled trial of a cognitive-behavioral and mindfulness-based group sleep intervention for at risk adolescents. J Child Psychol Psychiatry. 2018;59:637-49.
- Chung KF, Chan MS, Lam YY, Lai CSY, Yeung WF. School-Based Sleep Education Programs for Short Sleep Duration in Adolescents: A Systematic Review and Meta-Analysis. J Sch Health. 2017;87:401-8.
- Fatima Y, Doi SA, Najman JM, Al Mamun A. Continuity of sleep problems from adolescence to young adulthood: results from a longitudinal study. Sleep Health. 2017;3:290-5.
- Serra l, Ribas l, Ngo J, Ortega RM, García A, Pérez C, et al. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004;7:931-5.
- Martínez D, Martínez de Haro V, Pozo T, Welk GJ, Villagra A, Calle ME, et al. Fiabilidad y validez del cuestionario de actividad física PAQ-A en adolescentes españoles. Rev Esp Salud Publica. 2009;83:427-39.
- Aymerich M, Berra S, Guillamón I, Herdman M, Alonso J, Ravens U, et al. Desarrollo de la versión en español del KIDSCREEN: un cuestionario de calidad de vida para la población infantil y adolescente. Gac Sanit. 2005;19:93-102.
- Atienza FL, Moreno Y, Balaguer I. Análisis de la dimensionalidad de la escala de autoestima de Rosenberg en una muestra de adolescentes valencianos. Rev Psicol. 2000;22:29-42.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med. 2008;66:1429-36.
- Fonseca E, Paíno M, Lemos S, Villazón Ú, Muñiz J. Validation of the Schizotypal Personality Questionnaire Brief form in adolescents. Schizophr Res. 2009;111:53-60.
- Leger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. 1988;6:93-101.
- Mazzer K, Boersma K, Linton SJ. A longitudinal view of rumination, poor sleep and psychological distress in adolescents. J Affect Disord. 2019;245:686-96.
- Twenge JM, Martin GN, Spitzberg BH. Trends in US Adolescents’ media use, 1976–2016: The rise of digital media, the decline of TV, and the (near) demise of print. Psychology of Popular Media Culture. 2019;8:329.
- Belmon LS, van Stralen MM, Busch V, Harmsen IA, Chinapaw MJM. What are the determinants of children's sleep behavior? A systematic review of longitudinal studies. Sleep Med Rev. 2019;43:60-70.
- Galina SD, Souza JC, Valdez P, Azevedo CVM. Daily light exposure, sleep-wake cycle and attention in adolescents from different urban contexts. Sleep Med. 2021;81:410-7.
- Billings ME, Hale l, Johnson DA. Physical and Social Environment Relationship With Sleep Health and Disorders. Chest. 2020;157:1304-12.
- Duraccio KM, Krietsch KN, Chardon ML, Van Dyk TR, Beebe DW. Poor sleep and adolescent obesity risk: a narrative review of potential mechanisms. Adolesc Health Med Ther. 2019;10:117-30.
- Quintas-Neves M, Preto J, Drummond M. Assessment of bariatric surgery efficacy on Obstructive Sleep Apnea (OSA). Rev Port Pneumol. 2016;22:331-6.
- Naismith S, Winter V, Gotsopoulos H, Hickie I, Cistulli P. Neurobehavioral functioning in obstructive sleep apnea: differential effects of sleep quality, hypoxemia and subjective sleepiness. J Clin Exp Neuropsychol. 2004;26:43-54.
- Muscogiuri G, Barrea l, Annunziata G, Di Somma C, Laudisio D, Colao A, et al. Obesity and sleep disturbance: the chicken or the egg? Crit Rev Food Sci Nutr. 2019;59:2158-65.
- Muscogiuri G, Barrea l, Aprano S, Framondi l, Di Matteo R, Laudisio D, et al. Sleep Quality in Obesity: Does Adherence to the Mediterranean Diet Matter? Nutrients. 2020;12:1364.
- Noorwali E, Hardie l, Cade J. Bridging the Reciprocal Gap between Sleep and Fruit and Vegetable Consumption: A Review of the Evidence, Potential Mechanisms, Implications, and Directions for Future Work. Nutrients. 2019;11:1382.
- Mozaffarian N, Heshmat R, Ataie-Jafari A, Motlagh ME, Ziaodini H, Shafiee G, et al. Association of sleep duration and snack consumption in children and adolescents: The CASPIAN-V study. Food Sci Nutr. 2020;8:1888-97.
- Paiva T, Gaspar T, Matos MG. Sleep deprivation in adolescents: correlations with health complaints and health-related quality of life. Sleep Med. 2015;16:521-7.
- Kalak N, Lemola S, Brand S, Holsboer-Trachsler E, Grob A. Sleep duration and subjective psychological well-being in adolescence: a longitudinal study in Switzerland and Norway. Neuropsychiatr Dis Treat. 2014;10:1199-207.
- Zhang J, Paksarian D, Lamers F, Hickie IB, He J, Merikangas KR. Sleep Patterns and Mental Health Correlates in US Adolescents. J Pediatr. 2017;182:137-43.
- Kalak N, Gerber M, Kirov R, Mikoteit T, Pühse U, Holsboer-Trachsler E, et al. The relation of objective sleep patterns, depressive symptoms, and sleep disturbances in adolescent children and their parents: a sleep-EEG study with 47 families. J Psychiatr Res. 2012;46:1374-82.
- Evers K, Chen S, Rothmann S, Dhir A, Pallesen S. Investigating the relation among disturbed sleep due to social media use, school burnout, and academic performance. J Adolesc. 2020;84:156-64.
- Lang C, Kalak N, Brand S, Holsboer-Trachsler E, Pühse U, Gerber M. The relationship between physical activity and sleep from mid adolescence to early adulthood. A systematic review of methodological approaches and meta-analysis. Sleep Med Rev. 2016;28:32-45.
- Master l, Nye RT, Lee S, Nahmod NG, Mariani S, Hale l, et al. Bidirectional, Daily Temporal Associations between Sleep and Physical Activity in Adolescents. Sci Rep. 2019;9:7732.
- Su Y, Wang SB, Zheng H, Tan WY, Li X, Huang ZH, et al. The role of anxiety and depression in the relationship between physical activity and sleep quality: A serial multiple mediation model. J Affect Disord. 2021;290:219-26.
- Aseem A, Chaudhry N, Hussain ME. Effect of moderate intensity aerobic exercise training on electrophysiological and biochemical correlates of sleep. Sport Sciences for Health. 2021;17:1-9.
- Nevill AM, Duncan MJ, Sandercock G. Modeling the dose-response rate/associations between VO2max and self-reported Physical Activity Questionnaire in children and adolescents. J Sport Health Sci. 2020;9:90-5.
- Mota J, Vale S. Associations between sleep quality with cardiorespiratory fitness and BMI among adolescent girls. Am J Hum Biol. 2010;22:473-5.
- Sehn AP, Gaya AR, Dias AF, Brand C, Mota J, Pfeiffer KA, et al. Relationship between sleep duration and TV time with cardiometabolic risk in adolescents. Environ Health Prev Med. 2020;25:42.