

Vol. 24 - Num. 96
Original Papers
Factors associated with night sleep in adolescents
Raúl Jiménez Boraitaa, Daniel Arriscado Alsinab, Josep M.ª Dalmau Torresc, Esther Gargallo Ibortc
aProfesor. Universidad Isabel I. Burgos. Universidad Internacional de La Rioja. Logroño. España.
bProfesor. Universidad Isabel I. Burgos. España.
cProfesor. Universidad de La Rioja. Logroño. España.
Correspondence: R Jiménez. E-mail: raul.jimenez@unir.net
Reference of this article: Jiménez Boraita R, Arriscado Alsina D, Dalmau Torres JM, Gargallo Ibort E. Factors associated with night sleep in adolescents . Rev Pediatr Aten Primaria. 2022;24:375-84.
Published in Internet: 10-11-2022 - Visits: 3976
Abstract
Introduction: during adolescence there are many changes in lifestyle that also affect sleep patterns, patterns that are key in the development of young people and their health status. Therefore, the objective of the study was to analyze the relationship and influence of various lifestyle habits, physical and psychosocial health indicators, and sociodemographic variables on the duration of night sleep.
Method: a cross-sectional study was applied to a sample of 761 students (14.51±1.63 years) from 25 educational centers in a region of northern Spain. The hours of nightly sleep was assessed, as well as adherence to the Mediterranean diet, physical activity engagement, health-related quality of life, self-esteem, maximum oxygen uptake, body mass index, academic performance, and various sociodemographic factors.
Results: being older and having a higher body mass index, as well as less adherence to the Mediterranean diet and studying in urban centers were predictors of a lower number of hours of nightly sleep, explaining 26.2% of its variance. Likewise, adolescents who did not meet the nightly sleep recommendations had lower rates of health-related quality of life and self-esteem, as well as lower levels of physical activity and maximal oxygen uptake.
Conclusions: interventions aimed at preventing sleep disorders should take into account the aforementioned predictive factors, directing efforts towards promoting healthy habits and environments conducive to rest, especially in urban areas.
Keywords
● Adolescent ● Health ● Life habits ● Sleep ● Well-beingINTRODUCTION
Sleep is defined as a physiological state characterised by being reversible, transient and periodical, a function necessary for life and one of the habits with the greatest impact on health.1 Current recommendations for the population aged 13 to 18 years focus on adherence to a duration of night-time sleep of 8 to 10 hours.2 However, this is a stage in which sleep regulation becomes complicated.3
Poor quality and duration of night-time sleep in the young population is a growing concern in the field of public health.4 There is an increasing trend in the frequency of problems falling asleep in adolescents. According to the international study Health Behaviour in School-aged Children, approximately 24% of adolescents have sleep problems.5 In Spain, based on the Pasos Report6, 51.3% of adolescents sleep fewer hours than recommended on weekdays and 44.6% on weekends. Still, sleep patterns appear to vary substantially based on the country and other sociodemographic factors, such as household income or age.4
Previous studies have found that sleep has an important impact on the general health of the population, especially in children and adolescents, in whom non-adherence to recommendations can have serious immediate and future consequences.7 In this regard, the literature has demonstrated its interaction with other lifestyle habits, such as physical activity (PA) or dietary habits.8,9 In addition, sleep patterns are associated with different aspects of physical and psychological health, including emotional, cognitive and social health,10 cardiovascular and metabolic health11 and various mental health disorders, such as anxiety or depression.12
Effective interventions aimed at improving sleep habits in the adolescent population seems to have positive effects on general health.13 Educational settings play a key role in their promotion due to their accessibility and potential for transmitting positive values associated with sleep behaviours, knowledge and hygiene.14 In addition, the promotion of healthy sleep habits before adulthood is essential, as sleep disturbances during adolescence have a direct impact on sleep disorders in later stages.15
An overall understanding of the factors associated with night-time sleep could be particularly relevant for health prevention and promotion in the adolescent population. Therefore, the aim of our study was to assess night-time sleep in a representative sample of adolescents, analysing the influence of various indicators of physical and psychosocial health, lifestyle habits and sociodemographic factors. To do so, we assessed the duration of night-time sleep, the level of PA, the adherence to the Mediterranean diet (MD), health-related quality of life (HRQoL), self-esteem, the body mass index (BMI), maximal oxygen consumption (VO2max) and academic performance, in addition to the aforementioned sociodemographic factors.
MATERIAL AND METHODS
Study design and participants
We conducted a cross-sectional study in a representative sample of adolescents enrolled in years 1 and 4 of compulsory secondary education (ESO: Educación Secundaria Obligatoria) in schools of La Rioja, a region in Northern Spain. We selected the participants by single-stage cluster sampling, in which the sampling units were the ESO year 1 and year 4 classes in the region. To achieve a representative sample in both education years, given the size of the population (3470 students in year 1 of the ESO and 2548 in year 4 of the ESO), for a level of confidence of 95%, a precision of 5% and an expected proportion of 50%, we estimated that we needed 346 year 1 students and 334 year 4 students to achieve a representative sample. Given that the average number of students per class was 25 in both cases, and assuming a participation of 60%, we increased those figures correspondingly, randomly selecting 23 year 1 classes and 22 year 4 classes. We invited all students in the selected classes to participate and, since 82% accepted, the final sample included 761 adolescents belonging to 45 classes in 25 schools, of who 383 were year 1 students and 378 year 4 students. Their ages ranged from 12 to 17 years (14.51 ± 1.63 years), and 50.3% were male and 49.7% female.
Before participation, we obtained the written informed consent of the parents or legal guardians of each student. Furthermore, the participation of the students in the research was voluntary, and students provided verbal assent. The study adhered to the principles of the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of La Rioja. The field work for data collection was carried out between January and June 2018.
Variables
We estimated the hours of night-time sleep based on two questions that asked about the time participants usually went to bed and got up on weekdays. The duration of night-time sleep was calculated as the difference in hours between the times reported by the participants in these two questions. Once we had obtained the duration of sleep, we categorised students based on the recommendations of the American Academy of Sleep Medicine2 for the adolescent population as “in adherence” if the slept 8 or more hours or “not in adherence” if they slept fewer hours.
We assessed adherence to the MD through the KIDMED questionnaire.16 This instrument consists of 16 items with dichotomous answers (yes/no) concerning the consumption of foods associated with the Mediterranean dietary pattern. The overall score can range from −4 to 12, and higher scores indicate greater adherence to the MD.
We assessed the level of PA by means of the Physical Activity Questionnaire for Adolescents, which has been validated for the Spanish adolescent population.17 This instrument comprises 9 items that assess the PA performed in the past 7 days. The possible final score ranges from 1 to 5 points, and higher scores correspond to higher levels of PA. In addition, the questionnaire includes a tenth item that allows the exclusion of respondents who were unable to engage in PA as usual in the 7-day period of interest due to illness, injury or any other reason. However, this was not the case in any of the participants.
We assessed HRQoL with the KIDSCREEN-27 questionnaire, validated for use in Spanish adolescents.18 It has 27 items rated on a Likert scale and grouped into 5 dimensions: physical wellbeing, psychological wellbeing, autonomy and parent relations, school environment and social support and peers. We calculated the final scores according to the instructions of the authors of the questionnaire, and higher scores are associated with a more positive perception of quality of life.
For the assessment of self-esteem, we used the Rosenberg scale validated in Spanish adolescents.19 This instrument comprises 10 items rated on a scale from 1 to 4 to assess positive and negative feelings about the self. The final score can range from 10 to 40 and higher scores are associated with greater self-esteem.
When it came to sociodemographic data, participants reported their own sex, date of birth and nationality (born in Spain or in another country). We established the type of setting of the schools (urban or rural) based on the number of inhabitants in the location, considering a population of at least 5000 an urban town. Socioeconomic status (SES) was established by means of the Family Affluence Scale (FAS II), a questionnaire comprised of 4 questions about material wealth.20 The final score ranges from 0 to 9, and is categorised as follows: low (≤2), medium (3-5) or high (≥6). In the analysis of the data, we combined participants with a low (1.8%) and medium (28%) SES into a single category due to the small percentage of the former.
In addition, with the aim of identifying and excluding from the analysis self-reports filled out randomly, dishonestly or pseudo-randomly, we used the Oviedo Infrequency Scale, which consists of a series of questions with basic dichotomous yes/no responses.21 We inserted 6 of these questions throughout the questionnaire (for instance, “have you ever watched a movie on television?”). Participants who responded illogically to more than one of these questions were excluded from the analysis. Specifically, this was the case in 2 participants
We assessed cardiorespiratory fitness with a 20-metre shuttle run test.22 In this test, 2 line markers are set up at a distance of 20 m to demarcate the starting point and end of each shuttle. Participants have to run at the pace marked by an audio signal, which establishes the time available to run the distance between the two lines in succession. The initial speed is 8.5 km/h, and it increases by 0.5 km/h each minute. The test ended when the participant stopped or did not complete the distance at the established pace in 2 consecutive shuttles. Afterward, with the obtained results, we calculated the VO2max using the formula provided by the author of the test.
The height and weight were measured with a Holtain® stadiometer (Holtain Ltd., Dyfed, United Kingdom) accurate to 1 mm and a SECA® scale (713, Hamburg, Germany) accurate to 0.1 kg, respectively. Once these measurements were taken, we calculated the body mass index (BMI).
We assessed academic performance by reviewing the grades of the students, obtained through the Department of Education of the Government of La Rioja, and specifically basing it on the average grade obtained in the year that the study was conducted. Before doing so, we requested explicit consent from the families of the participants, which was granted by 90% of them.
Statistical analysis
We have expressed quantitative variables as mean and standard deviation, and qualitative variables in terms of frequencies. We assessed the normality and homogeneity of variance of the data with the Kolmogorov-Smirnov and Levene tests, respectively. We compared means with the Student t test in the case of a normal distribution and otherwise with the Mann-Whitney U test. We used the χ2 test to analyse the association between qualitative variables.
To identify potential predictors of the hours of night-time sleep, we fitted a multiple linear regression model with the backward elimination method. The variables included in the model were: sex, nationality, socioeconomic status, school setting, HRQoL, self-esteem, adherence to the MD, level of PA, VO2max and BMI. The statistical analysis was performed with the software IBM-SPSS® version 25 for Windows, and we defined statistical significance as p <0.05.
RESULTS
Of the total sample, 28.2% of adolescents did not adhere to night-time sleep recommendations. The age, adherence to MD, level of PA, VO2max, BMI and academic performance of adolescents in relation to their adherence to night-time sleep recommendations are shown in Table 1. We found that adolescents who adhered to recommendations exhibited greater adherence to the MD and had higher levels of PA and VO2max values, while their age and BMI were lower.
| Table 1. Characteristics of the sample in relation to adherence to night-time sleep recommendations | |||
|---|---|---|---|
| Hours of night-time sleep | P value | ||
| Did not adhere (n = 215) |
Adhered (n = 546) |
||
| Age | 15.54 ± 1.32 | 14.1 ± 1.57 | <0.001 |
| Adherence to Mediterranean diet | 6.86 ± 2.14 | 7.48 ± 2.08 | <0.001 |
| Physical activity | 2.51 ± 0.6 | 2.65 ± 0.62 | 0.005 |
| Maximal oxygen consumption | 43.29 ± 7.94 | 44.55 ± 6.39 | 0.028 |
| Body mass index | 21.76 ± 3.21 | 20.72 ± 3.23 | <0.001 |
| Academic performance | 6.51 ± 1.35 | 6.62 ± 1.51 | 0.294 |
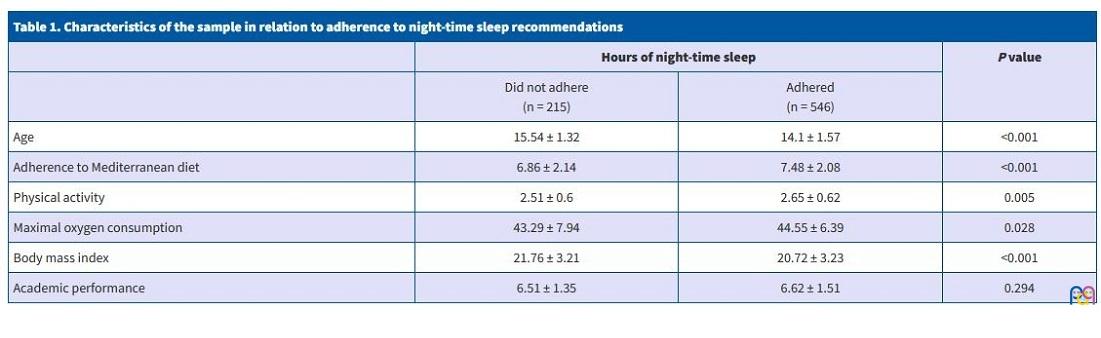
Table 2 presents the results of the assessments of self-esteem and HRQoL, overall and for its 5 dimensions, in relation to the adherence to night-time sleep recommendations. Adolescents that met sleep recommendations had significantly higher scores for self-esteem and HRQoL, overall and in every dimension save for “social support and peers”, in which we found no differences.
| Table 2. Psychosocial wellbeing in relation to adherence to night-time sleep recommendations | |||
|---|---|---|---|
| Hours of night-time sleep | P value | ||
| Did not adhere (n = 215) |
Adhered (n = 546) |
||
| Health-related quality of life | 241.16 ± 30.19 | 253.64 ± 33.67 | <0.001 |
| Physical wellbeing | 43.79 ± 8.62 | 45.2 ± 8.68 | <0.001 |
| Psychological wellbeing | 47.67 ± 8.24 | 51.15 ± 9.59 | <0.001 |
| School environment | 47.08 ± 8.36 | 50.71 ± 9.53 | <0.001 |
| Autonomy and parents | 49.84 ± 8.57 | 51.62 ± 8.72 | 0.048 |
| Social support and peers | 52.78 ± 9.88 | 53.87 ± 9.08 | 0.184 |
| Self-esteem | 31.77 ± 4.7 | 33.05 ± 4.98 | <0.001 |
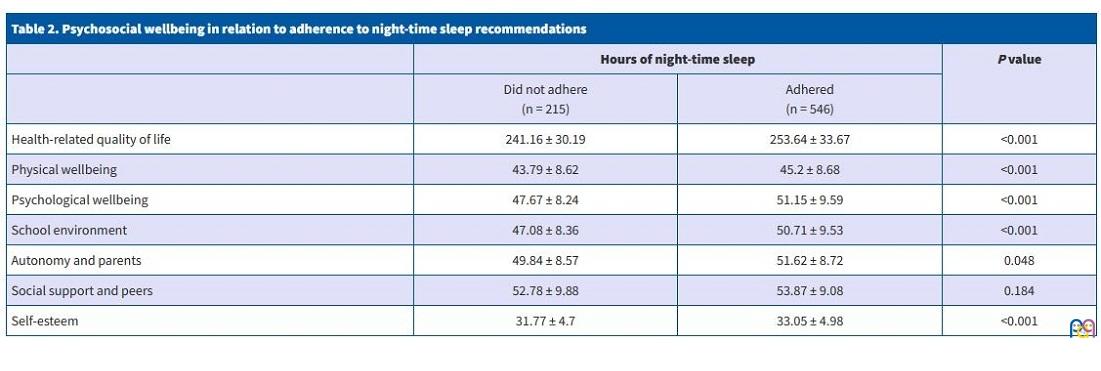
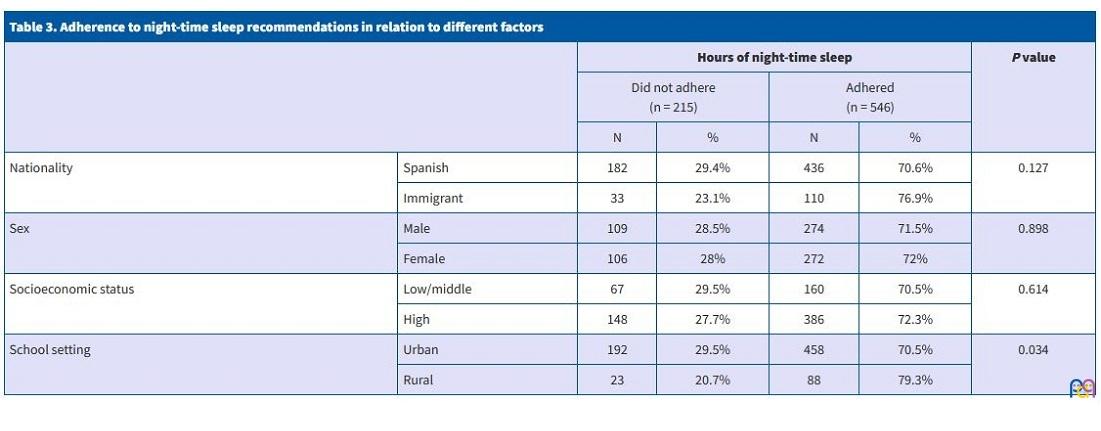
Table 3 reflects the impact of specific sociodemographic factors on the adherence to night-time sleep recommendations. We only found significant differences based on the setting of the school, with a higher frequency of non-adherence in students in urban areas.
| Table 3. Adherence to night-time sleep recommendations in relation to different factors | ||||||
|---|---|---|---|---|---|---|
| Hours of night-time sleep | P value | |||||
| Did not adhere (n = 215) |
Adhered (n = 546) |
|||||
| N | % | N | % | |||
| Nationality | Spanish | 182 | 29.4% | 436 | 70.6% | 0.127 |
| Immigrant | 33 | 23.1% | 110 | 76.9% | ||
| Sex | Male | 109 | 28.5% | 274 | 71.5% | 0.898 |
| Female | 106 | 28% | 272 | 72% | ||
| Socioeconomic status | Low/middle | 67 | 29.5% | 160 | 70.5% | 0.614 |
| High | 148 | 27.7% | 386 | 72.3% | ||
| School setting | Urban | 192 | 29.5% | 458 | 70.5% | 0.034 |
| Rural | 23 | 20.7% | 88 | 79.3% | ||
Lastly, Table 4 presents the results of the multiple linear regression analysis of the hours of night-time sleep. Older age, a higher BMI, lower adherence to the MD and attendance to school in an urban setting were predictors of decreased night-time sleep duration, and explained up to 26.2% of the variance in the number of hours of night-time sleep.
| Table 4. Predictors of duration of night-time sleep | ||||
|---|---|---|---|---|
| Hours of night-time sleep | ||||
| B | T | P value | R2 | |
| Age | -0.435 | -12.472 | <0.001 | 0.262 |
| Location of school (urban setting) | -0.159 | -4.734 | <0.001 | |
| Adherence to Mediterranean diet | 0.71 | 2.097 | 0.036 | |
| Body mass index | -0.074 | -2.144 | 0.032 | |

DISCUSIÓN
The results of the study show that 28.2% of participants did not adhere with sleep recommendations for the adolescent population, a percentage that was lower compared to the results of a previous nationwide study.6
Night-time sleep was associated with several indicators of physical and psychosocial health, lifestyle habits and sociodemographic variables, which allowed the identification of predictors.
Age was one of them, as older adolescents slept the fewest hours per night. A study by Mazzer (2019)23 corroborates this decreasing trend with increasing age in adolescents, and also showed an increase in the prevalence of cases of poor sleep associated with psychological distress. In this sense, there is a relevant frequency of problems in other areas associated with sleep disturbances in adolescents, an issue that persists in adulthood15 and that may be related to the use and impact of social networks and screens, in addition to increasing deficiencies in a weekly structure or schedule with increasing age in youth.24,25
The setting also served as a predictor of the hours of sleep, with a lower proportion of adherence to recommendations in the group of adolescents who attended schools in urban areas. Residence in more urbanised areas has been found to be associated with poorer quality, duration and regularity of sleep in adolescents.26 Factors related to various physical and social aspects (population density or availability of green spaces), aspects related to the neighbourhood (safety, order and social relations) or environmental factors (air pollution, noise or exposure to artificial light) seem to have a key impact on sleep habits.27
Adolescents with higher BMIs slept fewer hours, confirming BMI as a predictor of sleep duration. The association between sleep and obesity is widely documented in the previous literature, evincing the important effect of sleep habits on body composition.28 Evidence to date has identified an increased BMI as a risk factor for disorders such as sleep apnoea,29 which may result in respiratory difficulties leading in turn to intermittent hypoxaemia, increased daytime somnolence and/or poorer sleep quality.30 Increases in fat mass also appear to be associated with different biological mechanisms that have a direct impact on sleep.31
Last of all, among the lifestyle habits, the MD diet was also a predictor, with adolescents who adhered less to it reporting fewer hours of sleep at night. The MD has been found to be positively associated with sleep, both directly and through the improvement of de body composition.32 The consumption of vegetables and fruits seemed to have a positive impact on sleep due to their polyphenol content, as these substances have a direct impact on biological mechanisms such as the circadian rhythm.33 Furthermore, decreased sleep duration was associated with a greater intake of sandwiches, fast food and sugary drinks and a lesser intake of fruits and nuts.34
In addition to the predictors described above, night-time sleep was associated with other variables, including sociodemographic characteristics and indicators related to physical health and lifestyle habits.
As regards psychosocial health, the scores for both self-esteem and perceived quality of life (overall and in its 5 dimensions) were lower in adolescents who did not adhere to sleep recommendations. Sleep deprivation seems to affect physical wellbeing, as it increases the prevalence of symptoms such as headache, fatigue and dizziness.35 Some studies have corroborated the association between sleep duration and psychological wellbeing in adolescents,36 finding that decreased sleep duration increases the probability of experiencing mental health disorders37 and perceiving the family climate negatively.38
Inadequate sleep patterns are a determinant in school burnout in adolescents,39 which could partly explain our findings in relation to wellbeing in the school environment.
The PA level was lower in adolescents who did not meet night-time sleep recommendations, and in this regard the literature shows that increasing levels of physical activity is likely to improve sleep quality.40 Furthermore, moderate intensity to vigorous PA is associated with greater sleep duration and efficiency,41 although different factors modulate this effect, such as mental health disorders42 or the improvement of electrophysiological and biochemical elements of sleep associated with aerobic exercise.43
The maximal oxygen consumption values were also lower in adolescents who did not meet night-time sleep recommendations, which could result from the decreased levels of physical activity noted above.44 In this regard, the association between lifestyle habits and cardiorespiratory fitness is well established, and previous studies have found an association between poor sleep habits and a lower cardiorespiratory fitness 45 as well as an increased cardiovascular and metabolic disease risk.46
One of the strengths of the study was that we obtained a representative sample of adolescents, which allowed us to assess the association of the hours of night-time sleep with other lifestyle habits, different sociodemographic variables and indicators of physical and psychosocial wellbeing. For the purpose of future research, it may be worth considering the assessment of sleep through polysomnography or accelerometers. In any case, the instruments used in this study have been found reliable and valid in previous studies in samples of similar characteristics. On the other hand, the cross-sectional study design did not allow an assessment of causality, and in the future, studies with a longitudinal design could complement our current findings.
CONCLUSION
An older age, higher BMI, lower adherence to the MD attendance to schools in urban areas were predictors of fewer hours of night-time sleep de horas, explaining 26.2% of the variance in sleep duration. Adolescents who did not adhere to night-time sleep recommendations had lower scores for self-esteem and HRQoL (overall score and most of the dimensions), a lower level of PA and lower VO2max values. The observed associations underscore the need to develop interventions for the prevention of sleep disorders from a multidisciplinary approach. In this regard, the development of spaces more suitable for rest in urban areas as well as the promotion of PA and adherence to healthy dietary patterns could have a positive impact on both sleep duration and quality and, in turn, on the general health of adolescents, especially those who are older or reside in urban areas.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
FUNDING
This study was partially funded by the Instituto de Estudios Riojanos (IER) of the regional government of La Rioja through Resolution no. 55/2018, of July 9 of the Administration of the IER for the awarding of grants to scientific studies on subjects pertaining to La Rioja for the 2018-2019 period.
ABREVIATURAS
BMI: body mass index · ESO: Educación Secundaria Obligatoria (Compulsory Secondary Education) · FAS II: Family Affluence Scale II · HRQoL: health-related quality of life · MD: Mediterranean diet · PA: physical activity · SES: socioeconomic status · VO2max: maximal oxygen consumption.
REFERENCES
- Kryger M, Roth T, Dement W. Principles and practice of sleep medicine. 5th ed. St. Louis, MI: Elsevier Saunders; 2011.
- Paruthi S, Brooks LJ, D'Ambrosio C, Hall WA, Kotagal S, Lloyd RM, et al. Recommended amount of sleep for pediatric populations: a consensus statement of the American Academy of Sleep Medicine. J Clin Sleep Med. 2016;12:785-6.
- Crowley SJ, Wolfson AR, Tarokh l, Carskadon MA. An update on adolescent sleep: New evidence informing the perfect storm model. J Adolesc. 2018;67:55-65.
- Gariepy G, Danna S, Gobiņa I, Rasmussen M, De Matos MG, Tynjälä J, et al. How are adolescents sleeping? Adolescent sleep patterns and sociodemographic differences in 24 European and North American countries. J Adolesc Health. 2020;66:81-8.
- Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A, et al. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Copenhagen; 2020. In: World Health Organization [online] [accessed 10/10/2022]. Available at https://apps.who.int/iris/handle/10665/332104
- Gasol Foundation. Resultados principales del estudio PASOS 2019 sobre la actividad física, los estilos de vida y la obesidad de la población española de 8 a 16 years. Sant Boi de Llobregat, España: Gasol Foundation; 2019 [online] [accessed 10/10/2022]. Available at www.gasolfoundation.org/wp-content/uploads/2020/08/Estudio-PASOS-2019.pdf
- Owens JA, Weiss MR. Insufficient sleep in adolescents: causes and consequences. Minerva Pediat. 2017;69:326-36.
- Fenton S, Burrows TL, Skinner JA, Duncan MJ. The influence of sleep health on dietary intake: a systematic review and meta-analysis of intervention studies. J Hum Nutr Diet. 2020;34:273-85.
- Atoui S, Chevance G, Romain AJ, Kingsbury C, Lachance JP, Bernard P. Daily associations between sleep and physical activity: A systematic review and meta-analysis. Sleep Med Rev. 2021;57:101426.
- Dong l, Martinez AJ, Buysse DJ, Harvey AG. A composite measure of sleep health predicts concurrent mental and physical health outcomes in adolescents prone to eveningness. Sleep Health. 2019;5:166-74.
- Cespedes EM, Quante M, Rifas-Shiman SL, Redline S, Oken E, Taveras EM. Objective sleep characteristics and cardiometabolic health in young adolescents. Pediatrics. 2018;142:e20174085
- Berger AT, Wahlstrom KL, Widome R. Relationships between sleep duration and adolescent depression: a conceptual replication. Sleep Health. 2019;5:175-9.
- Blake MJ, Blake LM, Schwartz O, Raniti M, Waloszek JM, Murray G, et al. Who benefits from adolescent sleep interventions? Moderators of treatment efficacy in a randomized controlled trial of a cognitive‐behavioral and mindfulness‐based group sleep intervention for at‐risk adolescents. J Child Psychol Psychiatry. 2018;59:637-49.
- Chung KF, Chan MS, Lam YY, Lai CSY, Yeung WF. School‐Based Sleep Education Programs for Short Sleep Duration in Adolescents: A Systematic Review and Meta-Analysis. J Sch Health. 2017;87:401-8.
- Fatima Y, Doi SA, Najman JM, Al Mamun A. Continuity of sleep problems from adolescence to young adulthood: results from a longitudinal study. Sleep Health. 2017;3:290-5.
- Serra l, Ribas l, Ngo J, Ortega RM, García A, Pérez C, et al. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004;7:931-5.
- Martínez D, Martínez de Haro V, Pozo T, Welk GJ, Villagra A, Calle ME, et al. Fiabilidad y validez del cuestionario de actividad física PAQ-A en adolescentes españoles. Rev Esp Salud Publica. 2009;83:427-39.
- Aymerich M, Berra S, Guillamón I, Herdman M, Alonso J, Ravens U, et al. Desarrollo de la versión en español del KIDSCREEN: un cuestionario de calidad de vida para la población infantil y adolescente. Gac Sanit. 2005;19:93-102.
- Atienza FL, Moreno Y, Balaguer I. Análisis de la dimensionalidad de la escala de autoestima de Rosenberg en una muestra de adolescentes valencianos. Rev Psicol. 2000;22:29-42.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med. 2008;66:1429-36.
- Fonseca E, Paíno M, Lemos S, Villazón Ú, Muñiz J. Validation of the Schizotypal Personality Questionnaire Brief form in adolescents. Schizophr Res. 2009;111:53-60.
- Leger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. 1988;6:93-101.
- Mazzer K, Boersma K, Linton SJ. A longitudinal view of rumination, poor sleep and psychological distress in adolescents. J Affect Disord. 2019;245:686-96.
- Twenge JM, Martin GN, Spitzberg BH. Trends in US Adolescents’ media use, 1976–2016: The rise of digital media, the decline of TV, and the (near) demise of print. Psychology of Popular Media Culture. 2019;8:329.
- Belmon LS, van Stralen MM, Busch V, Harmsen IA, Chinapaw MJM. What are the determinants of children's sleep behavior? A systematic review of longitudinal studies. Sleep Med Rev. 2019;43:60-70.
- Galina SD, Souza JC, Valdez P, Azevedo CVM. Daily light exposure, sleep-wake cycle and attention in adolescents from different urban contexts. Sleep Med. 2021;81:410-7.
- Billings ME, Hale l, Johnson DA. Physical and Social Environment Relationship With Sleep Health and Disorders. Chest. 2020;157:1304-12.
- Duraccio KM, Krietsch KN, Chardon ML, Van Dyk TR, Beebe DW. Poor sleep and adolescent obesity risk: a narrative review of potential mechanisms. Adolesc Health Med Ther. 2019;10:117-30.
- Quintas-Neves M, Preto J, Drummond M. Assessment of bariatric surgery efficacy on Obstructive Sleep Apnea (OSA). Rev Port Pneumol. 2016;22:331-6.
- Naismith S, Winter V, Gotsopoulos H, Hickie I, Cistulli P. Neurobehavioral functioning in obstructive sleep apnea: differential effects of sleep quality, hypoxemia and subjective sleepiness. J Clin Exp Neuropsychol. 2004;26:43-54.
- Muscogiuri G, Barrea l, Annunziata G, Di Somma C, Laudisio D, Colao A, et al. Obesity and sleep disturbance: the chicken or the egg? Crit Rev Food Sci Nutr. 2019;59:2158-65.
- Muscogiuri G, Barrea l, Aprano S, Framondi l, Di Matteo R, Laudisio D, et al. Sleep Quality in Obesity: Does Adherence to the Mediterranean Diet Matter? Nutrients. 2020;12:1364
- Noorwali E, Hardie l, Cade J. Bridging the Reciprocal Gap between Sleep and Fruit and Vegetable Consumption: A Review of the Evidence, Potential Mechanisms, Implications, and Directions for Future Work. Nutrients. 2019;11:1382.
- Mozaffarian N, Heshmat R, Ataie-Jafari A, Motlagh ME, Ziaodini H, Shafiee G, et al. Association of sleep duration and snack consumption in children and adolescents: The CASPIAN-V study. Food Sci Nutr. 2020;8:1888-97.
- Paiva T, Gaspar T, Matos MG. Sleep deprivation in adolescents: correlations with health complaints and health-related quality of life. Sleep Med. 2015;16:521-7.
- Kalak N, Lemola S, Brand S, Holsboer-Trachsler E, Grob A. Sleep duration and subjective psychological well-being in adolescence: a longitudinal study in Switzerland and Norway. Neuropsychiatr Dis Treat. 2014;10:1199-207.
- Zhang J, Paksarian D, Lamers F, Hickie IB, He J, Merikangas KR. Sleep Patterns and Mental Health Correlates in US Adolescents. J Pediatr. 2017;182:137-43.
- Kalak N, Gerber M, Kirov R, Mikoteit T, Pühse U, Holsboer-Trachsler E, et al. The relation of objective sleep patterns, depressive symptoms, and sleep disturbances in adolescent children and their parents: a sleep-EEG study with 47 families. J Psychiatr Res. 2012;46:1374-82.
- Evers K, Chen S, Rothmann S, Dhir A, Pallesen S. Investigating the relation among disturbed sleep due to social media use, school burnout, and academic performance. J Adolesc. 2020;84:156-64.
- Lang C, Kalak N, Brand S, Holsboer-Trachsler E, Pühse U, Gerber M. The relationship between physical activity and sleep from mid adolescence to early adulthood. A systematic review of methodological approaches and meta-analysis. Sleep Med Rev. 2016;28:32-45.
- Master l, Nye RT, Lee S, Nahmod NG, Mariani S, Hale l, et al. Bidirectional, Daily Temporal Associations between Sleep and Physical Activity in Adolescents. Sci Rep. 2019;9:7732.
- Su Y, Wang SB, Zheng H, Tan WY, Li X, Huang ZH, et al. The role of anxiety and depression in the relationship between physical activity and sleep quality: A serial multiple mediation model. J Affect Disord. 2021;290:219-26.
- Aseem A, Chaudhry N, Hussain ME. Effect of moderate intensity aerobic exercise training on electrophysiological and biochemical correlates of sleep. Sport Sciences for Health. 2021;17:1-9.
- Nevill AM, Duncan MJ, Sandercock G. Modeling the dose-response rate/associations between VO2max and self-reported Physical Activity Questionnaire in children and adolescents. J Sport Health Sci. 2020;9:90-5.
- Mota J, Vale S. Associations between sleep quality with cardiorespiratory fitness and BMI among adolescent girls. Am J Hum Biol. 2010;22:473-5.
- Sehn AP, Gaya AR, Dias AF, Brand C, Mota J, Pfeiffer KA, et al. Relationship between sleep duration and TV time with cardiometabolic risk in adolescents. Environ Health Prev Med. 2020;25:42.
Comments
This article has no comments yet.