

Epidemia COVID. Tras el desconfinamiento ¿qué ocurrió en nuestras consultas de Atención Primaria?
Yolanda Martín Peinadora, Mar Braza Claverb, Raquel Girón del Ríoa, Clara Torres Delafuea, Soledad Gallego Campilloa
aPediatra. CS Goya.
bMIR-Pediatría. Hospital Infantil Universitario Niño Jesús .
Correspondencia: Y Martín. Correo electrónico: yolmarpei@gmail.com
Cómo citar este artículo: Martín Peinador Y, Braza Claver M, Girón del Río R, Torres Delafue C, Gallego Campillo S. Epidemia COVID. Tras el desconfinamiento ¿qué ocurrió en nuestras consultas de Atención Primaria? Rev Pediatr Aten Primaria. 2022;24:e53-e60.
Publicado en Internet: 12-04-2022 - Número de visitas: 11654
Resumen
Introducción: el 11 de marzo de 2020 la Organización Mundial de la Salud (OMS) declaró una pandemia, provocada por un nuevo coronavirus SARS-CoV-2. El rápido aumento de transmisiones obligó a gobiernos y autoridades sanitarias a tomar medidas para frenar el avance de la pandemia. Tras la primera ola epidémica y con un descenso documentado en el número de casos, comenzó la desescalada de las medidas implantadas y el desconfinamiento de la población. En este momento epidemiológico quisimos analizar la actividad asistencial pediátrica llevada a cabo, con objeto de conocer el modelo de consulta realizado (presencial/no presencial), los motivos de consulta atendida y el grado de resolución.
Material y métodos: estudio descriptivo, observacional y retrospectivo sobre los pacientes atendidos en las consultas de Pediatría de Atención Primaria en un centro de salud de la ciudad de Madrid, durante el mes de junio de 2020.
Resultados: se atendieron un total de 1321 pacientes, 34% menos que el mismo período del año anterior. La modalidad de consulta realizada fue presencial en un 49% y no presencial en el 51%. La consulta telefónica fue la opción mayoritaria como alternativa a la presencial. Un 20,7% del total de motivos de consulta fueron atendidos vía telemática.
Conclusiones: tras la crisis sanitaria ocasionada por la COVID-19 la modalidad de atención no presencial ha adquirido protagonismo y mayor grado de resolución en nuestras consultas pediátricas. Pensamos que debe potenciarse mediante la incorporación de herramientas telemáticas, y así coexistir y complementar al modelo habitual de atención presencial.
Palabras clave
● Atención Primaria ● Consulta no presencial ● COVID-19 ● PandemiaINTRODUCCIÓN
En diciembre de 2019 las autoridades sanitarias de la República Popular China comunicaron la aparición de una serie de casos de neumonía de causa desconocida. Las primeras investigaciones determinaron que se trataba de un nuevo tipo de coronavirus que denominaron SARS-CoV-2, con alta tasa de contagiosidad. La enfermedad que producía, denominada COVID-19, se iniciaba como una infección respiratoria similar a la causada por otros patógenos habituales. La mayoría de los casos cursaban de forma leve (80%), pero un pequeño porcentaje (hasta un 5%), podía evolucionar de forma grave: síndrome de dificultad respiratoria, hipoxemia, shock séptico y posible fallo multiorgánico, acabando incluso con la vida del paciente (1-3,5%). La mayoría de los pacientes tenían entre 30 y 79 años con una mínima afectación de la población infantil, el 1% de los casos reportados1. Tres meses después se habían producido más de 150 000 casos y cerca de 6000 muertos en todo el mundo según datos del Centro Europeo para el Control de Enfermedades (ECDC)2.
El 11 de marzo de 2020 la Organización Mundial de la Salud (OMS) eleva la situación de emergencia pública a pandemia3. La rapidez en la evolución de los casos, a escala nacional e internacional, obligó a la adopción de medidas inmediatas y contundentes para hacer frente a esta situación. El 14 de marzo el gobierno de España declara el estado de alarma. Pretendía con ello establecer una seria de medidas con el fin de proteger la salud y la seguridad de los ciudadanos, contener la propagación de la enfermedad, así como reforzar el Sistema Nacional de Salud4. Se restringió la libre circulación de las personas y se interrumpieron las actividades de ocio, con gran limitación de la actividad económica. Se cerraron colegios y centros educativos y gran parte de la actividad laboral trató de desarrollarse de forma telemática, salvo servicios esenciales.
En los primeros meses la población más afectada, según la Red Nacional de Vigilancia Epidemiológica (RENAVE)5, fue la franja de edad comprendida entre 50 y 59 años y el 55% de los casos eran mujeres. Entre los pacientes hospitalizados el perfil eran varones (55%) y un 21% tenía 70-79 años de edad6. Los niños se afectaban menos que los adultos, pero podrían infectarse igual, lo que se explicaría porque la mayor parte de las infecciones pediátricas son casos leves o asintomáticos, no demandando atención médica en muchas de las ocasiones1,7,8. No obstante se han publicado casos de enfermedad grave en niños asociada a infección por SARS-CoV-29-11.
El estudio de seroprevalencia de SARS-CoV-2 realizado en España entre abril y mayo de 2020 (ENE-COVID)12 aportó una seroprevalencia media de un 5%. La ciudad de Madrid, ubicación de este estudio, tenía una de las cifras más altas, superior al 10%. En los niños menores de 10 años era inferior al 3,1%.
En este contexto epidemiológico nuestro sistema público de salud debía de adaptarse y dar respuesta a esta emergencia sanitaria. Las autoridades sanitarias españolas, con el apoyo de sociedades científicas y grupos de expertos, publicaron diversos documentos desplegando la estrategia para la atención y seguimiento de los pacientes COVID13-15.
A partir de mayo de 2020, comenzaron a disminuir el número de casos y la saturación hospitalaria, observándose un aplanamiento de la curva epidémica. El gobierno decidió iniciar un desconfinamiento por fases para recuperar lentamente la llamada “nueva normalidad”16 (Fig. 1).
| Figura 1. Cronograma orientativo para la transición hacia la nueva normalidad |
|---|
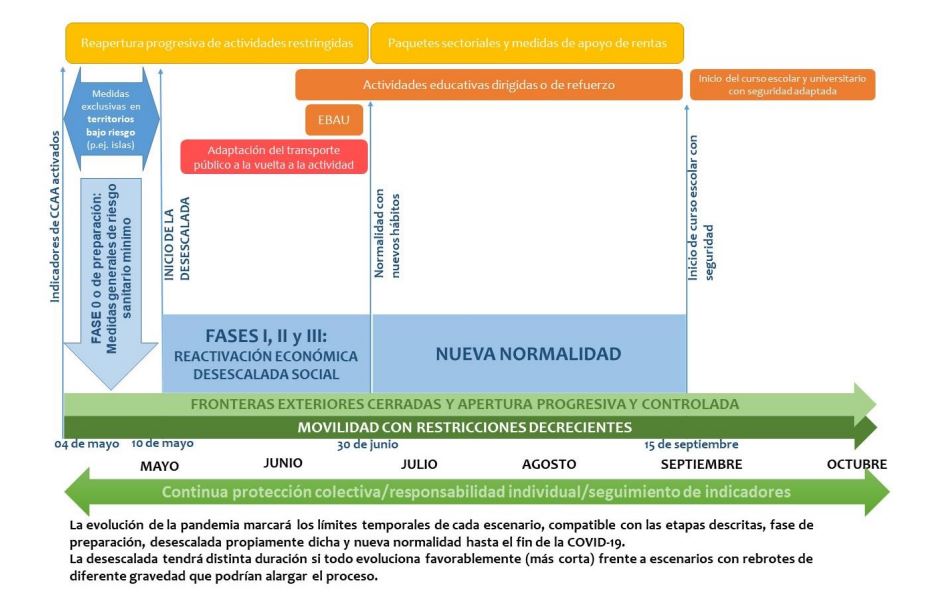 |

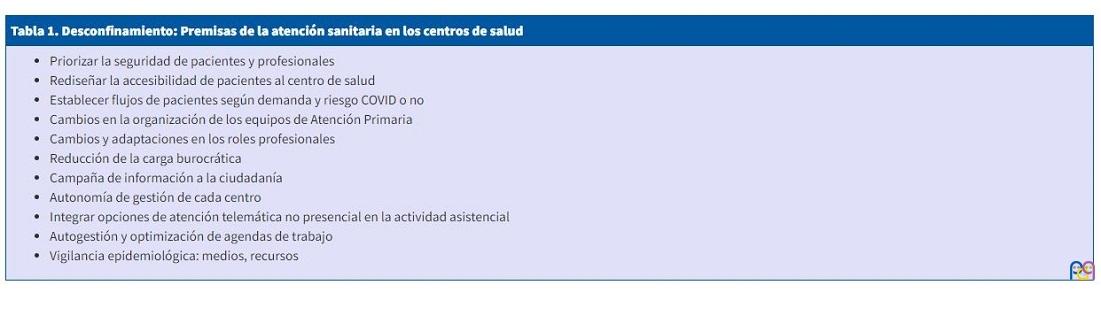
A lo largo del mes de junio se fue avanzando en esa desescalada, donde era preciso seguir adoptando medidas para hacer frente a la pandemia y evitar un nuevo incremento de casos. Medidas que afectaban a todas las esferas sociales y no solo al ámbito sanitario, produciendo un cambio en nuestra forma de vivir y relacionarnos. En nuestras consultas debíamos ir retomando la actividad habitual, pero manteniendo circuitos de atención seguros, con una serie de premisas establecidas en base a una realidad vivida y lecciones aprendidas (Tabla 1).
| Tabla 1. Desconfinamiento: Premisas de la atención sanitaria en los centros de salud |
|---|
|
OBJETIVOS
Nos planteamos describir y analizar la actividad asistencial pediátrica llevada a cabo en este centro de salud al iniciar la fase de desconfinamiento, con el objetivo principal de conocer cómo estábamos desarrollando la consulta, modalidades de atención, presencial versus no presencial, perfil de la demanda atendida y grado de resolución.
MATERIAL Y MÉTODOS
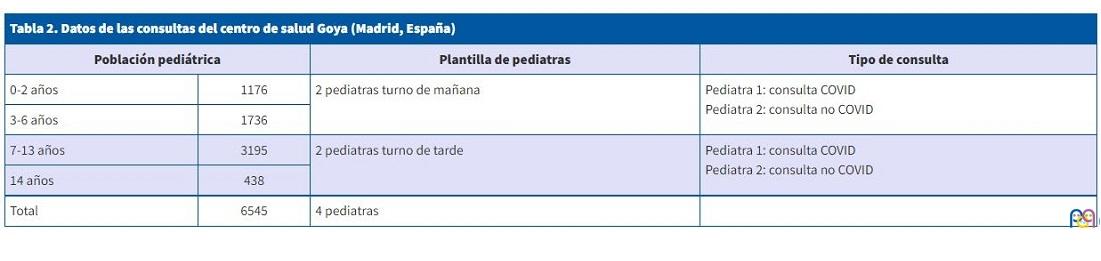
Estudio descriptivo, observacional y retrospectivo, basado en las historias clínicas de los pacientes atendidos en el servicio de Pediatría del centro de salud Goya (Madrid, España) durante el mes de junio del año 2020. Este centro está ubicado en un distrito céntrico de la ciudad. Atiende a una población total de 59 289 ciudadanos, con una población pediátrica de 6545 niños entre 0 y 14 años y 11 meses de edad (Tabla 2).
| Tabla 2. Datos de las consultas del centro de salud Goya (Madrid, España) | |||
|---|---|---|---|
| Población pediátrica | Plantilla de pediatras | Tipo de consulta | |
| 0-2 años | 1176 | 2 pediatras turno de mañana | Pediatra 1: consulta COVID Pediatra 2: consulta no COVID |
| 3-6 años | 1736 | ||
| 7-13 años | 3195 | 2 pediatras turno de tarde | Pediatra 1: consulta COVID Pediatra 2: consulta no COVID |
| 14 años | 438 | ||
| Total | 6545 | 4 pediatras | |
Los criterios de inclusión fueron: edad menor o igual a 14 años y haber recibido asistencia en el centro, ya fuera presencial o telefónica, en el periodo de tiempo mencionado. Inicialmente, los pacientes que habían solicitado cita pero no acudieron fueron incluidos en el análisis de las características demográficas, pero se excluyeron para el estudio del resto de variables de asistencia.
En todos los pacientes que solicitaron asistencia se recogieron características demográficas de edad y sexo. Posteriormente se recogía tanto la actividad asistencial prevista inicialmente como la que finalmente era llevada a cabo por el facultativo.
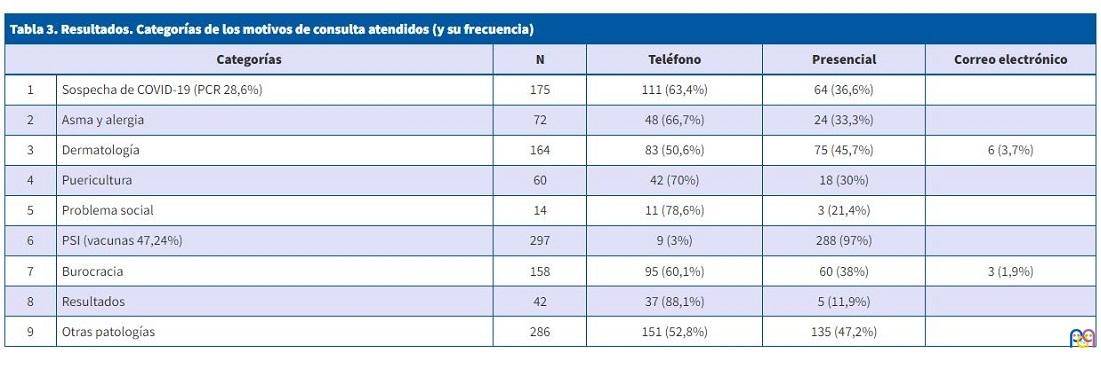
Tras excluir a aquellos que no acudieron a la consulta o no contestaban la llamada (se hacían un mínimo de dos), se clasificaba el motivo de consulta de forma numérica para facilitar su posterior análisis (Tabla 3). De forma adicional se recogían actividades realizadas en la consulta como cumplimentación del calendario vacunal, realización de pruebas diagnósticas, prueba PCR (reacción en cadena de la polimerasa) de coronavirus, o derivación a atención hospitalaria. La categoría de otras patologías se dividió a su vez en los siguientes apartados: gastrointestinal, ORL, genitourinario, alteración de la visión, neurológico, psiquiatría, traumatología, dental y miscelánea.
| Tabla 3. Resultados. Categorías de los motivos de consulta atendidos (y su frecuencia) | |||||
|---|---|---|---|---|---|
| Categorías | N | Teléfono | Presencial | Correo electrónico | |
| 1 | Sospecha de COVID-19 (PCR 28,6%) | 175 | 111 (63,4%) | 64 (36,6%) | |
| 2 | Asma y alergia | 72 | 48 (66,7%) | 24 (33,3%) | |
| 3 | Dermatología | 164 | 83 (50,6%) | 75 (45,7%) | 6 (3,7%) |
| 4 | Puericultura | 60 | 42 (70%) | 18 (30%) | |
| 5 | Problema social | 14 | 11 (78,6%) | 3 (21,4%) | |
| 6 | PSI (vacunas 47,24%) | 297 | 9 (3%) | 288 (97%) | |
| 7 | Burocracia | 158 | 95 (60,1%) | 60 (38%) | 3 (1,9%) |
| 8 | Resultados | 42 | 37 (88,1%) | 5 (11,9%) | |
| 9 | Otras patologías | 286 | 151 (52,8%) | 135 (47,2%) | |
Los datos necesarios para el estudio se obtuvieron de la historia clínica informatizada AP-Madrid. Se utilizó el programa Excel Microsoft Office para organizar los datos. Más tarde se exportaron al programa estadístico XLSTAT2020 para su análisis. Se realizó un análisis descriptivo de las variables. Para variables cuantitativas, los resultados descriptivos se expresaron mediante medidas de tendencia central y de dispersión (mediana y rango, puesto que la media y la desviación típica se hubieran visto muy influenciadas por la presencia de valores extremos, salvo en la descripción del número total de pacientes). Las variables cualitativas se expresaron mediante número y porcentaje.
RESULTADOS
Durante el periodo de estudio fueron atendidos un total de 1321 pacientes. De ellos 640 eran mujeres (48,5%) y 681 varones (51,5%). La mediana de edad fue de 4 años (rango de 3 días-15 años).
No hubo diferencias reseñables en la presión asistencial a lo largo del mes, con una media de 60 pacientes atendidos al día entre los cuatro profesionales. Si comparamos este dato con la presión asistencial media durante el mismo periodo del año 2019 objetivamos una disminución del 34%.
El tipo de consulta realizada fue un 49% (648) visita presencial y el 51% (582) no presencial. De las consultas presenciales 268 fueron en relación con el Programa de Salud Infantil (PSI) y 380 visitas por otras consultas médicas. En cuanto a la atención no presencial 571 se realizaron vía telefónica y 11 consultas por correo electrónico. Hubo 73 pacientes que no contestaron al teléfono. De la atención telefónica 461 (80,7%) fueron solicitadas por el propio paciente y 110 (19,3%) fueron por iniciativa del profesional.
En cuanto al grado de concordancia entre la modalidad de consulta estipulada inicialmente (presencial-telefónica-correo electrónico) y la llevada a cabo finalmente, el tipo de atención inicial se mantenía más en la atención telefónica, 63,6% de concordancia, seguido de las visitas por PSI (60%) y solo un 47,6% en la consulta presencial.
Analizando los motivos de consulta (Tabla 3) se realizó mayoritariamente PSI (23,4% de las consultas). El siguiente grupo de consultas en frecuencia fue aquel que relataban síntomas que coincidían con los posibles descritos en la infección por SARS-CoV-2 (13,8%): fiebre, tos y/o dificultad respiratoria, cefalea, dolor de garganta, diarrea, mialgias, lesiones cutáneas y menos frecuentes anosmia y ageusia. En este grupo se realizó técnica diagnóstica PCR en el 28,6% de los casos. A continuación, las consultas más demandadas fueron dermatológicas (12,9%) seguidas por las consultas en relación con asma y procesos alérgicos (5,7%). Un 12,5%, 158 consultas, fueron por temas administrativos. Del grupo de otras patologías las consultas por orden descendente de frecuencia fueron: problemas gastrointestinales, esfera ORL, genitourinario, alteraciones de la visión, neurológico, problemas psicológicos/psiquiátricos y traumatología.
Respecto a las derivaciones a servicios hospitalarios se realizaron un total de 69 (5,2% de los casos atendidos). Las especialidades mayoritarias en este caso fueron Oftalmología (40,6%), Dermatología (10,1%) y Psiquiatría (8,7%). Solo realizamos una derivación directa al servicio de urgencias, por un cuadro de deshidratación en un lactante en el contexto de una gastroenteritis.
DISCUSIÓN
La pandemia COVID-19 llegó sin ser esperada. Nuestras autoridades sanitarias emitieron recomendaciones para el acceso a los centros sanitarios con el objeto de procurar una atención segura tanto para los pacientes como para los profesionales. Al mismo tiempo debíamos continuar prestando atención sanitaria al resto de patologías y necesidades de nuestra población.
Durante el confinamiento y en lo que compete a la Pediatría de Atención Primaria, disminuyó considerablemente la frecuentación de los pacientes pediátricos, las familias estaban recluidas, los colegios estaban cerrados, y había temor a contagiarse. La mayoría de los centros de salud permanecieron abiertos, estableciendo un filtro de acceso al centro con el fin de separar circuitos de atención de pacientes con posible riesgo COVID de los que no. De forma programada se mantuvo la atención a los lactantes de corta edad y el calendario vacunal de primovacunación. Experimentamos un cambio drástico en la forma de trabajar, buscando en las opciones telemáticas una alternativa a la limitación de la atención presencial impuesta por la COVID-19.
A lo largo del mes de junio, durante la desescalada, debíamos retomar nuestra actividad habitual, pero era preciso continuar con medidas para frenar la pandemia y evitar un nuevo incremento de casos. En el análisis de nuestra actividad durante este periodo vimos un 34% menos de niños que en el mismo periodo del año anterior. Se fue retomando la actividad en la consulta con una presencia equilibrada entre visita presencial (49%) y no presencial (51%). En el análisis de concordancia entre el modelo de consulta estipulada inicialmente y la llevada a cabo finalmente era la actividad presencial la que presentaba un porcentaje menor con un 47,5%, explicado esto porque las visitas solicitadas en agenda como presenciales, se llamaban con anterioridad a la fecha de la consulta y se resolvían por teléfono o por correo electrónico.
En la visita presencial la actividad se repartía entre el PSI (42%) y el resto de los motivos de consulta (58%). La consulta telefónica fue la opción mayoritaria como alternativa a la presencial. De estas un 19% eran establecidas por el profesional, tras reconducir otra modalidad de consulta o para seguimiento evolutivo de pacientes. La consulta por correo electrónico fue minoritaria. Utilizamos el correo corporativo. Fundamentalmente su contenido eran imágenes, así como envío de documentos, informes y resultados de pruebas complementarias. Estas modalidades de consulta que antes de la pandemia eran utilizadas minoritariamente, se convirtieron en un pilar fundamental, resultando en una atención efectiva y bien aceptada por familias y profesionales, aportando cercanía y rapidez de actuación.
Analizando los motivos de consulta mayoritariamente fue el PSI. Se hizo especial esfuerzo en revisar calendarios vacunales y recaptar las vacunaciones no realizadas en el período anterior, ya que datos obtenidos en este sentido, demostraron un claro descenso en la cobertura vacunal durante los meses iniciales de la pandemia17,18.
Respecto a las consultas por síntomas de sospecha COVID, segundo grupo en frecuencia, referir que, durante la primera ola epidémica, en un momento de transmisión comunitaria, no dispusimos de pruebas diagnósticas de infección aguda (PDIA) para la población general sin factores de riesgo en Atención Primaria (AP). Durante el periodo de este estudio los protocolos que manejábamos indicaban realizarla en aquellos pacientes con clara sospecha de infección COVID-1919. Esto suponía un reto, pues muchas infecciones en la población infantil comparten una constelación de síntomas que hace difícil su aproximación diagnóstica. Nos apoyamos en criterios epidemiológicos y de gravedad clínica20. En ese momento solo disponíamos de PCR del SARS-CoV-2 realizada en muestra nasofaríngea. Nuestro porcentaje de 28,8% PCR realizadas pudiera parecer bajo, pero puede estar justificado porque muchos de los síntomas que demandaban al solicitar cita posteriormente en la valoración en consulta no eran consistentes, o el día de la visita ya no los presentaban, o porque tras la valoración del caso establecíamos otro diagnóstico como más probable, todo ello unido a que en ese momento epidemiológico teníamos un descenso en la incidencia de casos y, por tanto, de posible transmisión.
Más allá de la COVID-19 los motivos de consulta más referidos fueron de causa dermatológica y en relación con procesos alérgicos y asma (recordemos que nuestro periodo de estudio fue el mes de junio). No obstante, evidenciamos menor carga de esta patología comparada con temporadas previas. Indudablemente el confinamiento y las medidas de higiene y protección (lavado manos, mascarilla) tuvieron su efecto.
En cuanto a las derivaciones a atención hospitalaria fueron un 5,2%. Las especialidades mayoritarias fueron Oftalmología, Dermatología y Psiquiatría, esta última con un 8,7% de las derivaciones. Al revisar un estudio llevado a cabo en nuestras mismas consultas en el año 2008 respecto al perfil de derivación a atención hospitalaria21, comprobamos que coinciden los dos primeros motivos, pero el tercero en frecuencia entonces fue Traumatología, estando Psiquiatría al final en un grupo minoritario de las especialidades derivadas. Aunque ha pasado tiempo desde entonces y los problemas de salud mental están cada vez más presentes en nuestras consultas, sí constatamos que durante estos meses ha ocurrido un aumento reseñable de consultas por trastornos de ansiedad, fobias, alteraciones del sueño, de la conducta y situaciones vitales descompensadas, sobre todo en niños con trastornos ya diagnosticados como trastorno por déficit de atención (TDAH), trastornos del espectro autista (TEA) y trastornos de conducta alimentaria TCA.
En la Tabla 3 donde analizamos los motivos de consulta y determinamos el modelo de atención prestada, podemos comprobar que el correo electrónico tiene su presencia en consultas dermatológicas y trámites administrativos. Consultas sobre puericultura, problemática social, cuestiones administrativas y comunicación de resultados se realizaron mayoritariamente por vía telemática. La suma de este grupo supone un total de 274 consultas, el 20,7% del total de consultas realizadas. Nos parece importante este dato y así creemos que los circuitos de atención definidos en el centro, así como las agendas de los profesionales, deberían adaptarse para dar cabida a esta actividad en el formato más resolutivo y eficiente.
La pandemia por el SARS-CoV-2 ha supuesto un cambio en nuestra forma de vivir y en nuestra forma de prestar la atención sanitaria en el primer nivel asistencial. Con la premisa de establecer circuitos de atención seguros y eficientes, se ha gestionado de forma directa la demanda de la población, valorando desde el primer momento el motivo de consulta y la posible gravedad o no. Esto supone una atención sanitaria encauzada ya desde su demanda, hecho que se nos antoja deseable no solo para la COVID-19 sino para cualquier demanda de salud planteada. Para ello ha sido imprescindible adaptar la dinámica de los centros tanto en forma como en fondo, más aún en una Atención Primaria acostumbrada a un acceso sin filtro y sin límite.
Filtrar los motivos de consulta, reorientar nuevos roles profesionales, rediseñar agendas, para que sean flexibles y adaptadas, son aspectos que han venido y deben quedarse, pues han demostrado su pertinencia en la mejor gestión de las demandas de salud de nuestra población. La consulta presencial es imprescindible en la interacción con nuestros pacientes y familias, pero puede y debe convivir con la atención no presencial.
Toda situación de crisis es una oportunidad de cambio. El sistema sanitario en general y la Atención Primaria en particular han reorientado sus recursos ante el reto de la COVID-19. El estudio objeto de este artículo presenta una aportación modesta pero real en este sentido, donde la atención no presencial ha adquirido protagonismo y grado de resolución. Creemos que se debe seguir avanzando en esta línea, incorporando herramientas telemáticas que ayuden a los profesionales sanitarios a dar respuesta a las demandas de salud de nuestra población, y conseguir mejoras que permitan una atención primaria sólida, sostenible y adaptada a los tiempos.
CONFLICTO DE INTERESES
Las autoras declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.. Este trabajo no ha contado con ninguna financiación.
ABREVIATURAS
AP: Atención Primaria · ECDC: Centro Europeo para el Control de Enfermedades · OMS: Organización Mundial de la Salud · ORL: otorrinolaringología · PCR: reacción en cadena de polimerasa · PDIA: pruebas diagnósticas de infección aguda PSI: Programa de Salud Infantil · RENAVE: Red Nacional de Vigilancia Epidemiológica · TCA: trastorno de conducta alimentaria · TDAH: trastorno por déficit de atención e hiperactividad · TEA: trastorno del espectro autista.
BIBLIOGRAFÍA
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA. 2020;323:1239-42.
- European Centre for Disease Prevention and Control. An agency of the European Union. En: EDCD [en línea] [consultado el 21/03/2022] Disponible en www.ecdc.europa.eu/en/covid-19-pandemic
- Organización Mundial de la Salud. Brote de enfermedad por coronavirus COVID-19). En: WHO [en línea] [consultado el 21/03/2022] Disponible en www.who.int/es/emergencies/diseases/novel-coronavirus-2019
- Real Decreto 463/2020, de 14 de marzo. Declaración Estado alarma. En: Boletín Oficial del Estado [en línea] [consultado el 21/03/2022] Disponible en www.boe.es/buscar/doc.php?id=BOE-A-2020-3692
- Red Nacional de Vigilancia Epidemiológica (RENAVE). En: Centro Nacional de Epidemiología [en línea] [consultado el 21/03/2022] Disponible en https://cnecovid.isciii.es/
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Información Científica-Técnica. Enfermedad por coronavirus, COVID-19. En: Ministerio de Sanidad [en línea] [consultado el 21/03/2022] Disponible en www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/ITCoronavirus.pdf
- Mehta NS, Mytton OT, Mullins EWS, Fowler TA, Falconer CL, Murhpy OB, et al. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clin Infect Dis. 2020; 71: 2469–79.
- Medeiros GC, Nunes AC, Azevedo KP, Segundo VH, Santos GM, Mata AN, et al. The Control and Prevention of COVID-19 Transmission In Children: A Protocol For Systematic Review And Meta-Analysis. Medicine 2020;99:e21393.
- Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med. 2020;383:334-46.
- García A, Antón J, Martínez-Pajares JD, Giralt G, Gómez B, Tagarro A et al. Documento español de consenso sobre diagnóstico, estabilización y tratamiento del síndrome inflamatorio multisistémico pediátrico vinculado a SARS-CoV-2 (SIM-PedS). An Pediatr. 2021; 94: 116.e1-e11.
- Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 2020;174:882-9.
- Pollán M, Pérez-Gómez B, Pastor-Barriuso R, Oteo J, Hernán MA, Pérez-Olmeda M, et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet. 2020;396:535-44.
- Ministerio de Sanidad. Información por nuevo coronavirus, COVID-19. En: Ministerio de Sanidad, Consumo y Bienestar Social [en línea] [consultado el 21/03/2022] Disponible en www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/home.htm
- Comunicados COVID-19. Normativa y notas de prensa. Repositorio histórico de informes diarios de datos 2020. En: Comunidad de Madrid [en línea] [consultado el 21/03/2022] Disponible en https://www.comunidad.madrid/servicios/salud/comunicados-covid-19-normativa-notas-prensa
- Comunidad de Madrid. Coronavirus. En: Comunidad de Madrid [en línea] [consultado el 21/03/2022] Disponible en www.comunidad.madrid/servicios/salud/coronavirus
- Plan para la transición hacia una nueva normalidad. En: Ministerio de Sanidad [en línea] [consultado el 21/03/2022] Disponible en www.lamoncloa.gob.es/consejodeministros/resumenes/Documents/2020/PlanTransicionNuevaNormalidad.pdf
- Moraga FA, Fernández M, Grande AM, Martínez LI, Moreno D, Pérez JJ. Recuperando las coberturas vacunales perdidas en la pandemia COVID-19. Vacunas. 2020;21:129-35.
- Comité Asesor de Vacunas de la AEP. Objetivo: Recuperar las vacunaciones perdidas por la pandemia de COVID-19. En: Vacunas AEP [en línea] [consultado el 21/03/2022] Disponible en https://vacunasaep.org/profesionales/noticias/vacunaciones-demoradas-COVID-19-recuperacion
- Documento Técnico. Manejo en Atención primaria y domiciliaria del COVID-19. En: Ministerio de Sanidad AEP [en línea] [consultado el 21/03/2022] Disponible en www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Manejo_primaria.pdf
- Documento de manejo clínico del paciente pediátrico y pacientes de riesgo con infección por SARS-CoV-2. En: Asociación Española de Pediatría [en línea] [consultado el 21/03/2022] Disponible en www.aeped.es/noticias/documento-manejo-clinico-paciente-pediatrico-y-pacientes-riesgo-con-infeccion-por-sars-cov2
- Martín Y, Caruana l, Gallego MS, Ruiz S. Derivaciones a especializada desde una consulta de pediatría de atención primaria. Comunicación oral, 57 Congreso de la Asociación Española de Pediatría. An Pediatr. 2008;68:1-378.