
Vol. 23 - Num. 92
Originales
Seguridad de las actividades extraescolares en tiempos de pandemia por SARS-CoV-2. Estudio prospectivo en población pediátrica
Ana Rodríguez Varelaa, Alicia Martínez Sebastiánb, Pedro Dongo Floresb, Carla A. Pérez Paretsc, Beatriz Mansilla Roigb
aServicio de Urgencias de Pediatría. Hospital Universitario Doctor Peset. Valencia. España.
bMIR-Pediatría. Servicio de Pediatría. Hospital Universitario Doctor Peset. Valencia. España.
cMIR-Pediatría. Servicio de Pediatría. Hospital Universitario Doctor Peset . Valencia. España.
Correspondencia: A Rodríguez . Correo electrónico: rodriguez_anaval@gva.es
Cómo citar este artículo: Rodríguez Varela A, Martínez Sebastián A, Dongo Flores P, Pérez Parets CA, Mansilla Roig B. Seguridad de las actividades extraescolares en tiempos de pandemia por SARS-CoV-2. Estudio prospectivo en población pediátrica. Rev Pediatr Aten Primaria. 2021;23:375-81.
Publicado en Internet: 15-11-2021 - Número de visitas: 10538
Resumen
Introducción: la epidemia de la enfermedad por coronavirus 2019 ha obligado a implementar diferentes medidas para mitigar el impacto de un aumento inevitable de casos de COVID-19, como fue el cierre de los colegios. A su reapertura, dado que la actividad deportiva en la infancia y adolescencia es clave para su óptimo desarrollo, nos planteamos: ¿son seguras las actividades extraescolares deportivas en tiempos de COVID?
Material y métodos: estudio observacional descriptivo longitudinal. Se siguió a 717 escolares deportistas y monitores de una asociación deportiva municipal que participaron en alguna de las actividades deportivas ofrecidas durante el periodo de septiembre a diciembre del año 2020. Ante un caso positivo, se contactó con la familia, cumplimentando la hoja de recogida de datos y realizando seguimiento de los menores.
Resultados: de los 679 escolares deportistas y 38 adultos monitores estudiados, únicamente se registró un caso de infección por virus SARS-CoV-2. El caso fue un jugador de baloncesto de 13 años por un contacto familiar, la sintomatología fue leve y tanto él como su grupo de convivencia estable mantuvieron 10 días de cuarentena sin aparición de nuevos casos positivos.
Conclusiones: nuestros resultados indican que si la práctica deportiva se realiza en grupos controlados, en medios optimizados y respetando las normas sanitarias, pueden ser espacios seguros para nuestra población pediátrica, con una baja tasa de transmisión del virus SARS-CoV-2. No hemos observado ningún brote en nuestra muestra habiendo implantado las medidas preventivas oportunas y siendo los niños excelentes cumplidores de las mismas. No obstante, es importante disponer de un registro preciso del alumnado existente para el rastreo de contactos e incidir tanto en las medidas generales de prevención como en las específicas para actividades deportivas para minimizar los riesgos.
Palabras clave
● Deporte ● Extraescolares ● Pediatría ● SARS-CoV-2 ● SeguridadINTRODUCCIÓN
La emergencia y expansión del virus SARS-CoV-2 llegó a España el 31 de enero con el primer caso confirmado correspondiente a un ciudadano alemán, convirtiéndose en un gran desafío para nuestro país, así como una emergencia de Salud Pública de carácter internacional.
El día 9 de septiembre de 2020, fecha de comienzo del estudio que presentamos, según datos del Ministerio de Sanidad y la Dirección General de Salud Pública, había un total de 543 379 casos confirmados por PCR o IgM en el territorio español, de los que 29 253 correspondían a la Comunidad Valenciana (a fecha del 09/09), siendo la sexta comunidad española más afectada por detrás de Madrid, Cataluña, Andalucía, País Vasco y Castilla y León respectivamente, de los cuales 537 casos se encontraban hospitalizados, posicionándose España como líder europeo en número de contagios, en segundo lugar solo por detrás de Rusia1.
Esto ha hecho implementar grandes medidas preventivas promoviendo el distanciamiento social, limitando el número de personas en reuniones, así como la obligatoriedad del uso de la mascarilla y la restricción del horario de apertura de numerosos locales de ocio en las diferentes comunidades autónomas. Se han promocionado y reforzado las mismas medidas preventivas coincidiendo con en el inicio del año escolar, que tuvo lugar el 7 de septiembre en la Comunidad Valenciana. Para evitar la transmisión y expansión del virus, tanto en la escuela como en las actividades extraescolares y deportivas, se han implantado diversas medidas llevadas a cabo por los centros que trabajan con menores, como la medición de la temperatura al inicio de la actividad, uso obligatorio de la mascarilla en cualquier espacio dentro del recinto deportivo, limitación de los contactos creando grupos independientes conocidos como “burbuja”, aumento de la ventilación en espacios cerrados, clausura de los espacios comunes como vestuarios o duchas, uso frecuente de gel desinfectante y lavado de manos, entre otras, que han resultado exitosas en la población pediátrica según proponemos en el siguiente estudio.
El éxito experimentado en la población pediátrica, debido en gran medida a las acciones anteriormente descritas, es potenciado por las características particulares de la población infantil, que hacen que los niños sufran una forma más leve de enfermedad causada por los coronavirus, en el que se encuentra incluido el SAR-CoV-2, y que ya se pudo constatar en las epidemias de síndrome respiratorio agudo severo (SARS) y síndrome respiratorio de Oriente Medio (MERS), en las que, como en la actual pandemia, pocos casos de infección en el paciente pediátrico fueron reportados en comparación con la población adulta. Su transmisión de humano a humano principalmente se produce por vía respiratoria (gotitas respiratorias o aerosoles, según recientes estudios)2, aunque este también puede transmitirse por contacto con objetos contaminados, como juguetes y picaportes, que se verían minimizados con el uso de las medidas preventivas que habitualmente se ponen en marcha en los lugares donde los niños realizan sus actividades bajo estrecha supervisión de los docentes3. Los niños infectados pueden estar asintomáticos o tener fiebre, tos seca y fatiga; algunos pacientes experimentan síntomas gastrointestinales, que incluyen malestar abdominal, náuseas, vómitos, dolor abdominal y diarrea. La mayoría tienen manifestaciones clínicas leves y suelen tener buen pronóstico. Por lo general, se recuperan dentro de las dos primeras semanas después del inicio de la enfermedad3. Cuando son sintomáticos, los niños propagan el virus en proporciones similares a los adultos y pueden infectar a otros de manera similar, motivo por el cual no pueden asistir al ámbito escolar o a sus actividades extraescolares, permaneciendo en aislamiento en domicilio hasta que la infección se resuelva4. A pesar de las medidas anteriormente descritas, los brotes en las escuelas pueden ocurrir y ser difícil de detectar debido a la relativa ausencia de síntomas en los niños5,6. Por nuestra parte, no hemos objetivado ningún brote en nuestra muestra habiendo implantado las medidas preventivas oportunas en la nuestra población pediátrica y siendo los niños excelentes cumplidores de las mismas.
Presentamos un estudio realizado en un centro deportivo de la Comunidad Valenciana entre los meses de septiembre y diciembre de 2020 coincidiendo con el inicio del curso escolar en una población entre 3 y 19 años que ha realizado diferentes actividades extraescolares deportivas con las medidas preventivas enumeradas anteriormente, tanto en ambientes abiertos, como en cerrados, para estudiar si estos espacios constituyen lugares seguros para nuestra población pediátrica o por si de lo contrario constituyen un entorno eficaz de propagación del virus.
MATERIAL Y MÉTODOS
Diseño del estudio: estudio observacional descriptivo longitudinal.
Población de estudio: el estudio se realizó a 717 escolares deportistas y monitores de una asociación deportiva municipal (ACDSAB) situada en San Antonio de Benagéber, Valencia, que participaron en alguna de las actividades deportivas ofrecidas durante el periodo de septiembre a diciembre del año 2020.
Metodología: ante un caso positivo comunicado por el responsable COVID del centro deportivo, el pediatra responsable del estudio contactó con la familia, cumplimentando la hoja de recogida de datos y realizando seguimiento de los menores.
La hoja de recogida de datos se divide en tres apartados:
- Datos generales: fecha de notificación del caso, datos demográficos del deportista (edad, sexo), deporte practicado, grupo al que pertenecía, medidas preventivas llevadas a cabo durante la actividad.
- Datos clínicos como: síntomas de presentación y duración de los mismos, diagnóstico de detección de coronavirus (realizado mediante reacción en cadena de la polimerasa [PCR], antígeno o serología), patología de base del paciente, ingreso hospitalario.
- Datos de contactos/trazabilidad: contactos confirmados positivos y detección del ámbito de los contactos positivos (asociación deportiva, familia, colegio, otros), periodo de aislamiento, caso de reinfección.
Se rastreó a los contactos tanto familiares como del ámbito deportivo, determinando la fecha de inicio de la trasmisión, valorando así la trazabilidad de la infección del virus.
Asimismo, se valoraron otros factores como los síntomas ocasionados, gravedad y duración de la sintomatología, aislamiento domiciliario o ingreso y coinfección con otras patologías.
Análisis estadístico: el análisis estadístico ha sido realizado con el paquete estadístico SPSS® Statistics versión 19.0. Las variables cuantitativas continuas se han expresado como medias y desviaciones estándar y las categóricas como frecuencias absolutas y porcentajes.
Aspectos éticos: antes de la realización del estudio, la investigadora principal se reunió con la dirección del centro deportivo, que se mostró colaboradora en todo momento. Se entregó una hoja de información y autorización a los tutores legales de los deportistas, así como a los alumnos mayores de 12 años, que fue firmada previamente a la participación en este estudio. Los datos de los menores y las familias han sido codificados con claves específicas que han sido custodiadas por los responsables del estudio, respetando la confidencialidad de los datos y el anonimato según determina la Ley Orgánica de Protección de Datos 3/2018, 5 de diciembre. El proyecto ha sido revisado y autorizado por el Comité de Ética de Investigación Clínica del Hospital Universitario Doctor Peset.
RESULTADOS
Se incluyeron 717 personas en el estudio (65% varones), pertenecientes a la asociación deportiva municipal ACDSAB, situada en San Antonio de Benagéber (Valencia). De estas, 679 eran escolares deportistas y 38 adultos monitores de actividades deportivas.
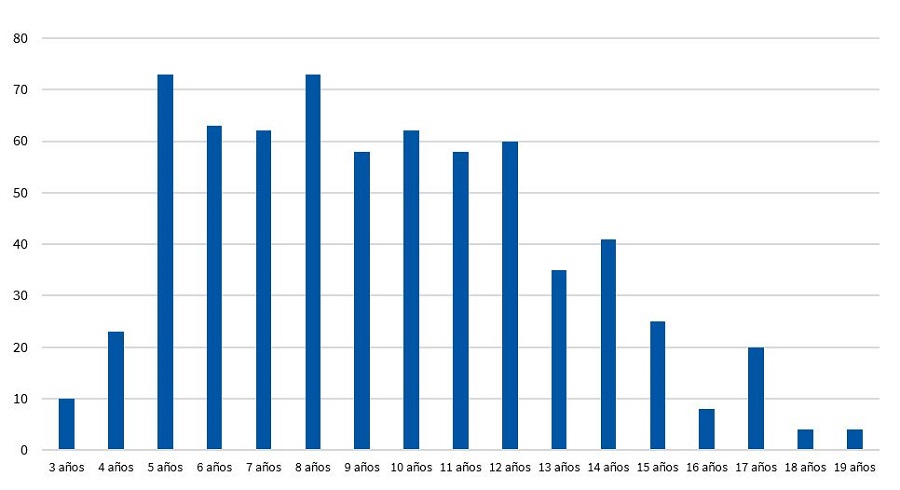
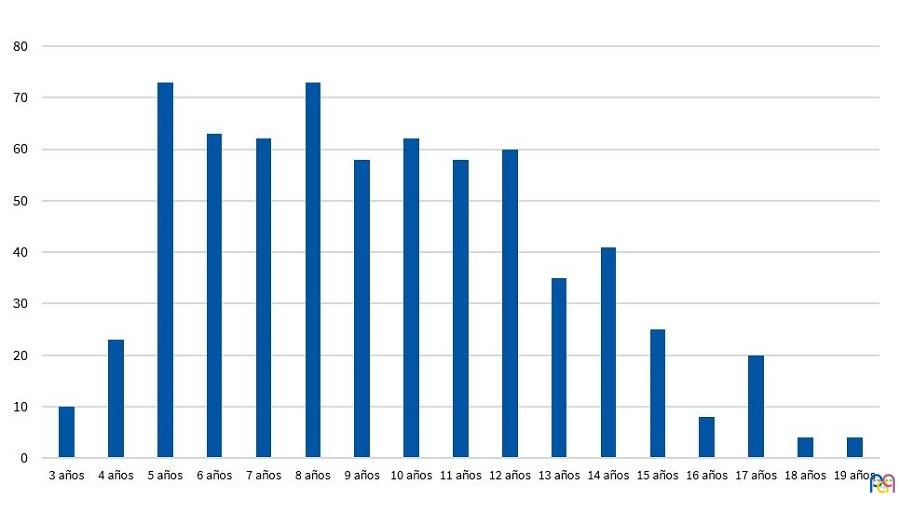
El grupo de edad de los escolares abarcaba de los 3 a los 19 años, repartidos tal y como se representa en la Fig. 1. El 15,8% eran menores de cinco años, y un 29% adolescentes mayores de 12 años. La media de edad de los escolares fue de 9,4 años, con una mediana de 9.
| Figura 1. Número total de deportista participantes en el estudio según edad |
|---|
 |
Se repartían en actividades practicadas al aire libre: futbol el 33%; tenis el 20%; baloncesto el 17%; patinaje el 5,2%; y futbol sala el 2,5%; y otras en espacios cerrados: karate el 13%; capoeira el 4,5%; baile el 3,5%; y deporte multidisciplinar el 1,5%.
Durante los cuatro meses de seguimiento (de septiembre a diciembre 2020), se registró un único caso de infección por virus SARS-CoV-2 en la muestra estudiada. El caso fue un varón de 13 años que practicaba baloncesto y que formaba parte de un grupo de convivencia estable (GCE) con su equipo. El contagio fue por contacto familiar, presentando como síntomas tos y mucosidad de 24 horas de duración, con aparición de anosmia a los cuatro días de inicio del cuadro. Se detectó mediante prueba rápida de antígeno, no precisó ingreso hospitalario y mantuvo diez días de aislamiento. Como antecedentes de interés, hay que destacar asma extrínseca de buena evolución, sin tratamiento de base.
Dado que pertenecía a un grupo de convivencia estable, se realizó aislamiento a los componentes de su equipo de baloncesto, con los que había entrenado 24 horas antes de la positividad de la prueba de detección de coronavirus. El aislamiento del grupo y del menor se realizó durante diez días y no presentaron síntomas ninguno de los implicados en el grupo afectado, por lo que no fue necesario la realización pruebas de detección de coronavirus en ninguno de ellos.
Los demás equipos de esta disciplina realizaron sus entrenamientos habituales, y el grupo afectado se reincorporó a la disciplina deportiva tras el confinamiento preventivo.
En las demás actividades deportivas no hubo constancia de ningún caso positivo que implicaran tomar medidas en los demás compañeros, dado que no cumplían los criterios de contacto estrecho, ya sea por cumplir las medidas de prevención adecuadas o por ser su último contacto con el grupo deportivo más de 72 horas antes del inicio de la clínica.
DISCUSIÓN
La positividad de un único menor entre los 679 deportistas y 38 monitores que conformaban la muestra estudiada se traduce en una incidencia de 1/717 (0,0014) en el periodo de cuatro meses que duró el estudio. Esto parece implicar que si la práctica deportiva se realiza en grupos controlados, en medios optimizados para la misma y respetando las normas sanitarias para frenar la expansión del virus, podemos conseguir una baja transmisión de la enfermedad aún en situaciones en las que las medidas de distancia interpersonal y uso de mascarilla no siempre pueden ser aplicadas de forma óptima. Sin embargo, serán necesarios más estudios para confirmar estos resultados.
El único caso confirmado fue el de un adolescente de 13 años que realizaba baloncesto como actividad deportiva. El hecho de que no se confirmasen contactos positivos en compañeros implica que las medidas aplicadas fueron efectivas. El contagio se produjo en el ámbito familiar (el abuelo y el padre del escolar comenzaron con sintomatología en días previos al paciente; el abuelo se realizó una PCR para detectar SARS-CoV-2 que resultó positiva). Tal y como sugieren los datos actuales de transmisión del virus, es probable que una parte considerable de los contagios tengan que ver con la transmisión entre familiares y contacto social entre adultos.
El último entrenamiento del adolescente positivo para SARS-CoV-2 con el grupo fue 24 horas antes del resultado de la prueba, lo cual convirtió al GCE en contactos estrechos y provocó el aislamiento de este durante diez días, según las normas vigentes dictadas por Salud Pública. Durante estos diez días, ningún menor presentó síntomas, por lo que no se realizó la PCR a ninguno de ellos, volviendo a la actividad deportiva habitual tras el aislamiento. Cabe destacar que tampoco ninguno de los 38 monitores resultó positivo.
Respecto al análisis de la actividad deportiva, las recomendaciones generales emitidas por la Consellería de Sanitat Valenciana7, además de hacer hincapié en medidas generales de prevención, incluyen medidas específicas a llevar a cabo en las actividades extraescolares para hacerlas lo más seguras posibles. Entre estas, destacan la llamada a la responsabilidad de padres y tutores a la hora revisar el estado de salud de los niños y adolescentes deportistas previo a acudir a la actividad, la importancia de evitar aglomeraciones a la entrada y salida de las actividades, de garantizar la ventilación de las instalaciones en el caso de que la actividad física no sea al aire libre, de evitar el uso de vestuarios y duchas, así como la desinfección del material deportivo y el espacio utilizado. Se hace hincapié en la necesidad de disponer de un registro preciso del alumnado existente para que, en el caso de detectar un contagio, el rastreo de contactos pueda hacerse de forma eficiente. También se hace referencia a la importancia de mantener la distancia interpersonal y limitar las actividades físicas que supongan contacto físico entre los niños y adolescentes deportistas, favoreciendo, aún en los deportes que impliquen contacto directo, rutinas de entrenamiento individuales durante la mayor parte de la actividad. En deportes en los que su práctica conlleva un contacto estrecho con imposibilidad de mantener la distancia interpersonal de al menos 1,5 metros y en los que, por su intensidad, el uso de mascarilla podría dificultar entrenamientos y competiciones8,9 se realizó una organización mediante GCE. Los escolares miembros de los GCE podrán socializar y jugar entre sí sin tener que mantener la distancia interpersonal de forma estricta ni usar mascarilla. Estos grupos están conformados por un máximo de 20 escolares (pudiéndose ampliar excepcionalmente a 25) y su objetivo es optimizar la trazabilidad y la gestión de los casos de contagios y, al mismo tiempo, permitir la interacción algunas veces imprescindible en el ámbito escolar. El personal docente y no docente que no forme parte del GCE e interaccione con él, deberá llevar mascarilla y mantendrá la distancia interpersonal10.
En lo que se refiere al único positivo confirmado, la práctica deportiva del baloncesto en concreto implica unas características especiales ya que, a pesar de ser realizada al aire libre, consta de contacto directo regular entre los participantes, así como contacto regular de todos ellos con la superficie de balones utilizados durante entrenamientos y partidos que no es posible desinfectar tras cada contacto. El hecho de que ninguno de los compañeros de actividad extraescolar del adolescente infectado fuese contagiado, así como la ausencia de positivos para SARS-CoV-2 en relación con los contactos durante la práctica deportiva, implica que la responsabilidad del personal y, sobre todo, de padres, deportistas y monitores a la hora de cumplir las medidas anteriormente referidas, fue fundamental, disminuyendo la posibilidad de transmisión del virus.
El hecho de que no se produjeran más contagios en la actividad deportiva realizada en espacios cerrados que en la realizada en abiertos, implica que estas conclusiones son también aplicables a este último tipo de actividades deportivas, a priori con más riesgo (deportes de contacto y realizados en ambientes cerrados), e implica la posibilidad de mantener tanto clases de educación física como actividades extraescolares con prácticas deportivas variadas, incluyendo aquellas en las que las medidas de distancia interpersonal son más difíciles de aplicar, frente a la posibilidad de reducir la oferta a la práctica deportiva al aire libre y en deportes concretos.
Por último, el hecho de que no se encontraran diferencias en la tasa de contagio en niños y adolescentes deportistas de diferentes edades implica también la posibilidad de mantener las actividades extraescolares en todas las franjas de edad, incluyendo en ellas a los escolares de menor edad en los que a veces aplicar de forma óptima medidas como el distanciamiento social puede ser complicado y que los menores de seis años están exentos de llevar mascarilla.
Es importante incidir en que esto será así siempre y cuando estas actividades se realicen de forma supervisada y se respeten de la forma más estricta posible las medidas generales sanitarias implementadas según evidencia científica para frenar la expansión del virus11. Esto, según nuestro punto de vista, es fundamental, ya que la actividad deportiva en infancia y adolescencia es clave para su óptimo desarrollo, disminuyendo la incidencia de patologías prevalentes como la obesidad, previniendo el sedentarismo y favoreciendo el desarrollo de habilidades sociales y de valores como la responsabilidad y el trabajo en equipo. Entendemos que una mayor oferta conseguirá una mayor adhesión. Son necesarios sin embargo más estudios para confirmar estos resultados, de gran importancia de cara a orientar la práctica deportiva extraescolar en colegios e institutos.
Como limitaciones del estudio, destacamos principalmente el hecho de que nos consta al menos un menor que fue positivo para SARS-CoV-2 y, al indicársele desde Sanidad Pública que no cumplía criterios de contacto estrecho con sus compañeros de actividad deportiva (la prueba diagnóstica fue positiva más de 48 horas después de la última vez que había realizado actividad deportiva con el resto de menores deportistas) no informaron al club de dicho positivo ni se realizó aislamiento de los compañeros, aunque también destacamos que la indicación de que ningún menor con síntomas sospechosos de infección por SARS-CoV-2 o al que se le hubiese indicado aislamiento preventivo por contacto estrecho acudió a realizar actividades extraescolares deportivas.
CONCLUSIONES
Nuestros resultados indican que, si la práctica deportiva se realiza en grupos controlados, en medios optimizados y respetando las normas sanitarias, pueden ser espacios seguros, no habiendo grandes diferencias entre los espacios abiertos y los cerrados bien ventilados, para nuestra población pediátrica con una baja tasa de transmisión del virus SARS-CoV-2.
No hemos observado ningún brote en nuestra muestra, habiendo implantado las medidas preventivas oportunas y siendo los niños excelentes cumplidores de las mismas.
No obstante, es importante disponer de un registro preciso del alumnado existente para que, en el caso de detectar un contagio, el rastreo de contactos pueda hacerse de forma eficiente e incidir tanto en las medidas generales de prevención como en las específicas para actividades deportivas para minimizar los riesgos.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
GCE: grupo de convivencia estable · MERS: síndrome respiratorio de Oriente Medio · PCR: reacción en cadena de la polimerasa · SARS: síndrome respiratorio agudo severo.
AGRADECIMIENTOS
Agradecemos a todo el personal laboral y directivo de la asociación deportiva municipal ACDSAB, de en San Antonio de Benagéber (Valencia, España) y a los niños deportistas y a sus familias la participación en el presente estudio.
BIBLIOGRAFÍA
- Actualización n.º 203. Enfermedad por el coronavirus (COVID-19) (datos consolidados a las 14:00 horas del 09.09.2020). En: Ministerio de Sanidad [en línea] [consultado el 11/11/2021]. Disponible en www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_203_COVID-19.pdf
- Paules CI, Marston HD, Fauci AS. Coronavirus infections ‒ More than just the common cold. JAMA. 2020;323:707-8.
- Cao Q, Chen YC, Chen CL, Chiu CH. SARS-CoV-2 infection in children: Transmission dynamics and clinical characteristics. J Formos Med Assoc. 2020;119:670-3.
- COVID-19 in children and the role of school settings in COVID-19 transmisión – Draft Technical Report - 31 July 2020. European Centre for Disease Prevention and Control; 2020.
- Panovska-Griffiths J, Kerr CC, Stuart RM, Mistry D, Klein DJ, Viner RM, et al. Determining the optimal strategy for reopening schools, the impact of test and trace interventions, and the risk of occurrence of a second COVID-19 epidemic wave in the UK: a modelling study. Lancet Child Adolesc Health. 2020;4:817-27.
- Medeiros GCBS, Nunes ACF, Azevedo KPM, de Oliveira Segundo VH, Santos GM, Mata ÁNS, et al. The Control and Prevention of COVID-19 Transmission in Children: A Protocol for Systematic Review and Meta-analysis. Medicine (Baltimore). 2020;99:e21393.
- Protocol de mesures de Prevenció i Higiene Sanitària en les Activitats Extraescolars. En: GVA; Conselleria de Sanitat Universal i Salut Pública [en línea] [consultado el 11/11/2021]. Disponible en https://coronavirus.san.gva.es/documents/469630/873868/Protocolo+Actividades+Extraescolares+Cas.pdf/b445f8c4-dfa4-f650-802f-2876a5d7e948?t=1634302727152
- Davis BA, Tsen LC. Wearing an N95 Respiratory Mask: An Unintended Exercise Benefit? Anesthesiology. 2020;133:684-6.
- Pifarre F, Dulanto D, Grazioli G, de Yzaguirre I, Maura I. COVID-19 and masks in sports. Apunts Sports Med. 2020;55:143-5.
- Actualización del protocolo de protección y prevención frente a la transmisión y contagio del sars-cov-2 para centros educativos que impartan enseñanzas no universitarias en el curso 2020-21 . En: GVA; Conselleria d’Educació Cultura i Sport [en línea] [consultado el 11/11/2021]. Disponible en https://ceice.gva.es/documents/161634256/174782899/Protocolo/927f90ba-7d23-4559-b8bc-9d3ef95898a8
- Chen P, Mao l, Nassis GP, Harmer P, Ainsworth BE, Li F. Returning Chinese school-aged children and adolescents to physical activity in the wake of COVID-19: actions and precautions. J Sport Health Sci. 2020;9:322-4.