

Experiencia enfermera en la realización de espirometrías en un equipo pediátrico
Sarai Marsiñach Sáncheza, M.ª Carmen Santafé Méndeza, Isabel Gascón Casaredib
aEnfermera de Pediatría. CAP La Marina. Institut Català de la Salut. Barcelona. España.
bPediatra. Unidad de Neumología Pediátrica. Hospital Sant Joan de Déu. Barcelona. España.
Correspondencia: S Marsiñach . Correo electrónico: smarsinachsanchez@gmail.com
Cómo citar este artículo: Marsiñach Sánchez S, Santafé Méndez MC, Gascón Casaredi I. Experiencia enfermera en la realización de espirometrías en un equipo pediátrico. Rev Pediatr Aten Primaria. 2021;23:e137-e145.
Publicado en Internet: 26-10-2021 - Número de visitas: 14667
Resumen
Introducción: en España el asma constituye la segunda causa de morbilidad y enfermedad crónica infantil. Es una de las causas más frecuentes de consulta en el ámbito de la Atención Primaria, y su diagnóstico y tratamiento precoz permiten el control de la enfermedad modificando el curso de esta y la calidad de vida de los pacientes. Objetivo: describir la experiencia en la realización de espirometrías en la población pediátrica e impulsar a otros centros de Atención Primaria la incorporación de esta prueba en su cartera de servicios.
Material y métodos: se realizaron 81 espirometrías a 67 pacientes con edades comprendidas entre los 5 y 14 años, entre enero 2019 y febrero 2020. De las 81 espirometrías, el 16% fueron basales, el 32,1% basales con prueba broncodilatadora (PBD) y el 51,9% con ejercicio y PBD. Se realizaron con un espirómetro Sibelmed Datospir Touch 511-B00-MU1.
Resultados: de las 26 espirometrías con PBD, 15 fueron negativas y 11 positivas. De las 32 espirometrías con ejercicio que se realizaron, 9 fueron positivas respecto a la espirometría basal, y en 23 no se obtuvieron diferencias significativas, pero 5 de ellas si dieron positivo al realizar PBD.
Conclusiones: es posible realizar espirometrías forzadas con resultados de calidad en el ámbito de Atención Primaria pediátrica, si se disponen de recursos materiales y de personal especializado. De esta forma, se contribuye a reducir las listas de espera y favorece un mayor control de la enfermedad.
Palabras clave
● Asma ● Atención Primaria ● Enfermería ● Espirometría ● Niños ● PediatríaINTRODUCCIÓN
Hoy en día en nuestro país el asma constituye la segunda causa de morbilidad y enfermedad crónica infantil, después de la obesidad1. Tiene una prevalencia del 10%, y es más frecuente en las zonas costeras2-4.
Se trata pues, de una patología altamente prevalente en la edad pediátrica, en la que el diagnóstico y tratamiento precoz permiten el control de la enfermedad y ello modifica el curso de esta y la calidad de vida de los pacientes afectos1. Adquiriendo un buen control del asma se evita el deterioro en la función pulmonar, se mejora la calidad de vida, se previene la mortalidad y se reduce el gasto sanitario1,3.
Se trata de una de las causas más frecuentes de consulta en el ámbito de la Atención Primaria, y el coste aproximado es de 535 millones de euros/año en niños asmáticos menores de 16 años en España1,3,5.
El diagnóstico del asma es clínico, basado en una anamnesis y exploración física que nos permitan detectar signos como la presencia de sibilancias, disnea, tos y opresión torácica1,2. Aun así estos síntomas y signos no son específicos de la enfermedad, por lo que las guías clínicas recomiendan la realización de pruebas diagnósticas objetivas como la espirometría forzada2,4.
La espirometría forzada se utiliza para confirmar el diagnóstico, descartar otras enfermedades, cuantificar la gravedad de la enfermedad, observar la respuesta al tratamiento y monitorizar su evolución3,6,7. Además de la espirometría forzada, existen otras técnicas para valorar la función pulmonar en niños como la espirometría forzada con prueba broncodilatadora y las espirometrías con pruebas de provocación bronquial6.
La espirometría con prueba broncodilatadora (PBD) aporta información sobre la reversibilidad de la obstrucción al flujo aéreo, y por tanto es la prueba más útil para el diagnóstico y seguimiento del asma6.
La prueba de provocación bronquial se puede realizar mediante sustancias que actúan directamente en el músculo liso bronquial, o provocando la liberación de mediadores que causan un estrechamiento de la vía aérea, a través del ejercicio, hiperventilación o solución salina hipertónica6.
La prueba de provocación con ejercicio (test de ejercicio o carrera libre) está indicada para la valoración de los síntomas sugerentes de asma relacionados con el ejercicio físico, y es de utilidad para diagnóstico de asma no controlado y el asma de esfuerzo6,8.
Según el último protocolo del Grupo de Vías Respiratorias de la Asociación Española de Pediatría de Atención Primaria, todo niño o adolescente con asma debería tener en su historia clínica los resultados de alguna prueba de función pulmonar. Una a ser posible en la evaluación inicial, otra a los 3-6 meses de iniciar el tratamiento de mantenimiento, y mantenerla actualizada durante el seguimiento al menos una vez al año8.
Antiguamente, la espirometría en la población pediátrica era una prueba escasamente utilizada en Atención Primaria debido a que los niños no realizaban maniobras de respiración voluntaria con la misma eficacia que los adultos y no habían valores de referencia adecuados7,9. Pero en los últimos años se han publicado diversos estudios que indican que en niños a partir de tres o más años se pueden llevar a cabo espirometrías forzadas de calidad, siempre y cuando, se utilice una metodología adecuada, la realice personal entrenado y formado, y se tengan en cuenta valores de referencia adaptados a su edad2,7,9,10.
En los últimos años se está observando un aumento creciente en la utilización de técnicas de exploración funcional ya que facilitan la valoración objetiva del asma. A su vez disminuyen la presión en derivaciones a los centros hospitalarios de referencia de aquellos pacientes con afectación leve de la enfermedad5,8,11.
En diversos estudios, se ha observado que el papel y la implicación del personal de enfermería durante la realización de la espirometría y en el seguimiento del niño y de su familia es clave en el manejo del niño y adolescente con asma. Pero para ofrecer una atención de calidad es necesario disponer de profesionales motivados, bien formados y actualizados, software con motivación adaptada a los niños, y además una estructura y recursos suficientes9,12.
En nuestro centro empezamos a realizar espirometrías en el año 2016 gracias a que una de las pediatras del centro tenía formación especializada en neumología y alergia pediátrica y creó una consulta puente entre la Atención Primaria y la hospitalaria, con el objetivo de ofrecer una mejor calidad asistencial a los pacientes del centro y disminuir el tiempo de espera en las derivaciones hospitalarias. Además, una enfermera tenía experiencia realizando espirometrías en adultos durante varios años y se formó específicamente en la realización de la espirometría en niños, cosa que nos animó a comenzar y continuar realizando este tipo de pruebas en nuestro centro.
El objetivo de nuestro artículo es describir nuestra experiencia en la realización de espirometrías en la población pediátrica e impulsar a otros centros de Atención Primaria la incorporación de esta prueba en su cartera de servicios.
MATERIAL Y MÉTODOS
Participantes
Los niños incluidos en este estudio forman parte de la población asignada al equipo pediátrico la Marina-Magória (Barcelona, España). Los datos han sido recogidos en el periodo de enero de 2019 y febrero de 2020, teniendo en cuenta que durante un mes no se realizaron espirometrías por periodo vacacional.
Durante ese periodo se realizaron 81 espirometrías, de las cuales el 16% (n = 13) fueron basales, el 32,1% (n = 26) basales con PBD, y el 51,9% (n = 42) con ejercicio y PBD.
Se realizaron espirometrías a 67 pacientes, el 58,2% (n = 39) fueron del sexo masculino y el 41,8% (n = 28) femenino. Las edades estuvieron comprendidas entre los 5 y 14 años con una media de edad de 9,5 años.
A un paciente se le realizaron siete espirometrías de control y a nueve pacientes se les realizaron dos espirometrías por diversos motivos.
Los motivos de realización de la técnica fueron: completar el diagnóstico de asma, realizar control de dicha patología, seguimiento del tratamiento, o para el diagnóstico de asma de esfuerzo.
En la mayoría de los casos los pacientes ya contaban en su historia clínica con diagnósticos de asma, disnea, rinitis alérgica, bronquitis agudas obstructivas (BAO), tos, o disnea con el ejercicio.
Procedimiento
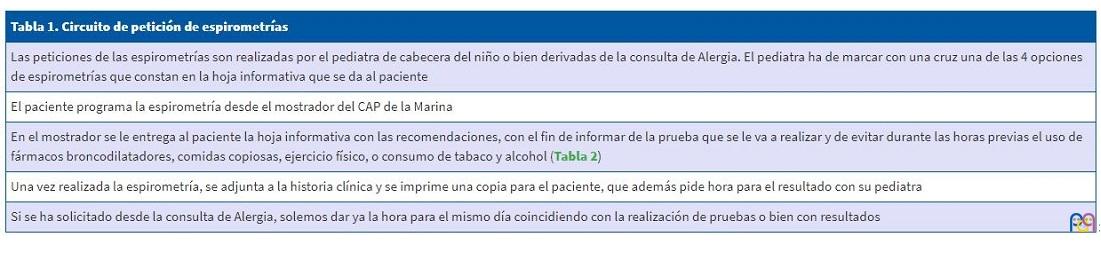
Las espirometrías las solicita el pediatra de referencia o la pediatra encargada de la consulta de alergia de nuestro centro, siguiendo el circuito creado para ello (Tabla 1). Una vez se ha realizado la petición, se programa el día de la espirometría y se entrega una hoja de recomendaciones para el día de la cita a los padres. En esta hoja se dan indicaciones con el fin de evitar durante las horas previas el uso de fármacos broncodilatadores, comidas copiosas, ejercicio físico, tabaco y alcohol, en caso de adolescentes (Tabla 2).
| Tabla 1. Circuito de petición de espirometrías |
|---|
| Las peticiones de las espirometrías son realizadas por el pediatra de cabecera del niño o bien derivadas de la consulta de Alergia. El pediatra ha de marcar con una cruz una de las 4 opciones de espirometrías que constan en la hoja informativa que se da al paciente |
| El paciente programa la espirometría desde el mostrador del CAP de la Marina |
| En el mostrador se le entrega al paciente la hoja informativa con las recomendaciones, con el fin de informar de la prueba que se le va a realizar y de evitar durante las horas previas el uso de fármacos broncodilatadores, comidas copiosas, ejercicio físico, o consumo de tabaco y alcohol (Tabla 2) |
| Una vez realizada la espirometría, se adjunta a la historia clínica y se imprime una copia para el paciente, que además pide hora para el resultado con su pediatra |
| Si se ha solicitado desde la consulta de Alergia, solemos dar ya la hora para el mismo día coincidiendo con la realización de pruebas o bien con resultados |
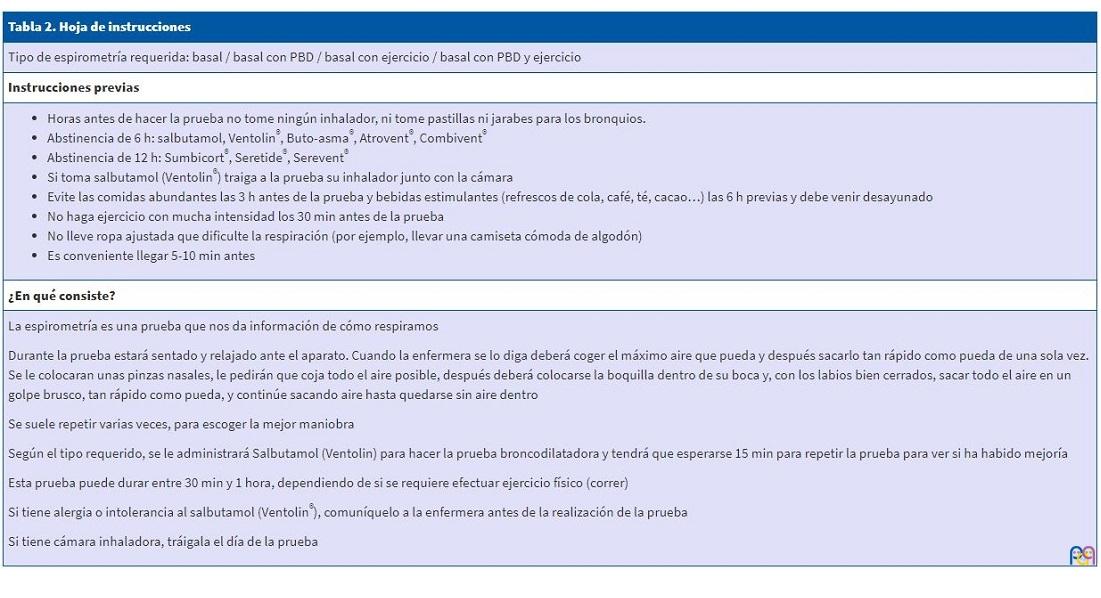
| Tabla 2. Hoja de instrucciones |
|---|
| Tipo de espirometría requerida: basal / basal con PBD / basal con ejercicio / basal con PBD y ejercicio |
| Instrucciones previas |
|
| ¿En qué consiste? |
|
La espirometría es una prueba que nos da información de cómo respiramos Durante la prueba estará sentado y relajado ante el aparato. Cuando la enfermera se lo diga deberá coger el máximo aire que pueda y después sacarlo tan rápido como pueda de una sola vez. Se le colocaran unas pinzas nasales, le pedirán que coja todo el aire posible, después deberá colocarse la boquilla dentro de su boca y, con los labios bien cerrados, sacar todo el aire en un golpe brusco, tan rápido como pueda, y continúe sacando aire hasta quedarse sin aire dentro Se suele repetir varias veces, para escoger la mejor maniobra Según el tipo requerido, se le administrará Salbutamol (Ventolin) para hacer la prueba broncodilatadora y tendrá que esperarse 15 min para repetir la prueba para ver si ha habido mejoría Esta prueba puede durar entre 30 min y 1 hora, dependiendo de si se requiere efectuar ejercicio físico (correr) Si tiene alergia o intolerancia al salbutamol (Ventolin®), comuníquelo a la enfermera antes de la realización de la prueba Si tiene cámara inhaladora, tráigala el día de la prueba |
Todas las espirometrías fueron realizadas en la consulta de espirometría por una enfermera con experiencia en la realización de espirometrías tanto en adultos como en población infantil. Se realizaron los miércoles entre las 8:00 y las 10:00 horas de la mañana.
Para la realización de las espirometrías contamos con un espirómetro Sibelmed Datospir Touch 511-B00-MU1, el software W20S versión 511-BLA-1.06 y una boquilla desechable no deformable. El espirómetro se calibra al inicio de cada sesión con una jeringa de calibración Modelo S300 Volume 3000 con una variabilidad de ±0,5% de precisión. Siguiendo las instrucciones del fabricante, se realizan 1 a 5 ciclos intentando que la insuflación dibuje una curva dentro de las dos áreas marcadas que aparecen en el software del espirómetro.
Los niños entran acompañados de un familiar para que estén más tranquilos, y se intenta crear un ambiente agradable. En nuestro centro las espirometrías se realizan en una de las consultas donde habitualmente se visitan los niños, por tanto, es un entorno familiar con decoración infantil que les aporta confianza y tranquilidad.
Se registra el peso y la talla del paciente, que se miden de forma protocolizada mediante báscula y tallímetro. Los parámetros de edad, sexo y etnia, se introducen automáticamente utilizando los datos del programa informático de uso habitual para las consultas en nuestro centro (ECAP 10.0).
Se realiza una anamnesis acerca del estado del paciente y sobre el consumo de medicamentos u otras circunstancias que puedan interferir o contraindicar la prueba en ese momento (falta de compresión o colaboración, hemoptisis reciente, dolor abdominal, náuseas o vómitos, infecciones respiratorias activas, cirugía ocular o patología de otorrinolaringología).
Además, antes de iniciar la maniobra explicamos el procedimiento al paciente y hacemos una demostración.
En todas las espirometrías forzadas los pacientes han mantenido la sedestación, y no ha sido necesario adoptar otras posturas. Sin embargo, se les ha de motivar para que mantengan la espalda recta, sobre todo durante la maniobra espiratoria, ya que suelen inclinarse hacia adelante.
En la mayoría de los casos se ha podido utilizar la pinza de oclusión nasal, y solo se ha retirado en casos muy concretos debido a que el niño no la ha tolerado.
La estimulación del niño se realiza mediante palabras, lenguaje gestual y corporal, y además el software utilizado contiene un juego de animación en que durante la espiración el niño ha de llegar a la luna con un cohete.
Para realizar la espirometría forzada se explica al niño que en primer lugar ha de inspirar de forma rápida, pero no forzada, intentando coger todo el aire que pueda hasta alcanzar la capacidad pulmonar total (TLC).
Posteriormente ha de introducir la boquilla en la boca sujetándola con los dientes y cerrando los labios en torno a ella. Y sin haber realizado una pausa mayor de 2 segundos, ha de efectuar una espiración enérgica (soplar rápido y fuerte) de forma continua (para expulsar todo el aire contenido en los pulmones) hasta alcanzar el volumen residual (RV).
Al finalizar la espiración, se puede completar la prueba, si se desea el asa inspiratoria, con una inspiración forzada hasta alcanzar la TLC, indicándole al niño que coja aire hacia adentro sin dejar la boquilla hasta la máxima inspiración, pero solo se ha realizado en nuestro centro en una ocasión, a petición del pediatra.
Para considerar la espirometría como correctamente realizada, tenemos en cuenta que se hayan cumplido dos criterios. En primer lugar, el criterio de aceptabilidad, que es subjetivo del técnico que realiza la prueba. El técnico ha de considerar que el esfuerzo realizado por el niño ha sido el adecuado, así como que el inicio, trazado y finalización han sido satisfactorios y que la duración del tiempo espiratorio ha sido al menos de 6 segundos (2-3 segundos en niños pequeños).
En segundo lugar, el criterio de reproducibilidad. Este criterio se cumple cuando los dos mejores valores de la capacidad vital forzada (FVC) y los dos mejores valores del volumen espirado forzado en el primer segundo (FEV1) no difieren entre sí más de 150 ml o más de un 5%. Si la FVC es igual o menor de 1 litro (preescolares de 2-6 años), las diferencias no deben ser mayores a 100 ml.
Habitualmente, una espirometría forzada requiere un mínimo de dos maniobras aceptables en niños y tres en adolescentes, sin un máximo recomendado, aunque en nuestro centro procuramos no realizar más de ocho maniobras en una misma cita. Ha habido alguna ocasión en la que algún niño ha requerido más de ocho maniobras, por tanto, se le ha dejado más tiempo de descanso entre las mismas y se han buscado nuevas estimulaciones para conseguir la colaboración y atención del niño. En el caso de que aun así no se consigan buenas maniobras, se le cita otro día para repetir la prueba.
En la actualidad, es cierto que los espirómetros seleccionan de forma automática la mejor maniobra, pero, de todas formas, la enfermera que realiza la espirometría revisa que la selección sea la adecuada de forma manual.
Los parámetros espirométricos se valoran respecto a la población sana de referencia. En nuestro caso el espirómetro permite seleccionar entre varios valores de referencia y nosotros utilizamos los de Sociedad Española de Neumología y Cirugía Torácica (SEPAR).
Los patrones de las alteraciones espirométricas (tipo obstructivo, restrictivo o mixto), se valoraron siguiendo el protocolo de espirometría forzada del Grupo de Vías Respiratorias de la Asociación Española de Pediatría de Atención Primaria.
Prueba broncodilatadora (PBD)
En nuestro centro, para llevar a cabo la prueba broncodilatadora realizamos una espirometría forzada basal, y posteriormente administramos 400 µg de salbutamol, equivalentes a 4 pulsaciones intercaladas por 30 segundos, que en niños realizamos en una cámara espaciadora. Para poder aprovechar al máximo el tiempo disponible y poder atender a otros pacientes, se invita al niño y a su acompañante a esperar 10-15 minutos en la sala de espera, justo enfrente de la consulta. Una vez trascurrido ese tiempo, se realiza otra espirometría donde se valoran posibles cambios en los parámetros.
Para valorar la respuesta broncodilatadora, observamos el cambio porcentual respecto al valor teórico del FEV1. Se considera positiva una PBD cuando el cambio porcentual del FEV1 es igual o superior al 12% en relación con el valor previo, o del 9% en relación con el valor teórico (≥12% o ≥200 ml) respecto al valor basal en adolescentes y adultos.
Test de ejercicio
La prueba de provocación bronquial con ejercicio trata de demostrar la respuesta obstructiva exagerada con el ejercicio físico.
Previamente a la realización de la prueba se entrega una hoja (Tabla 2) donde aparecen las siguientes recomendaciones: acudir con ropa adecuada para realizar ejercicio físico y sin haber tomado medicación broncodilatadora en las 12 h previas. Además, es necesario que no hayan realizado otro esfuerzo el mismo día, por eso en nuestro caso, por norma general las realizamos a primera hora de la mañana.
Antes de realizarla se interroga al paciente para asegurar que se hayan cumplido las recomendaciones previas y cerciorarnos de que no haya síntomas. Además, se registra la frecuencia cardiaca (FC) y la saturación (SpO2), y se realiza una auscultación en reposo.
Se realiza una primera espirometría basal, en la que la FVC y FEV1 han de ser superiores al 80% de los valores de referencia. De no ser así, un pediatra los ausculta para comprobar el estado de las vías respiratorias, y se realiza la PBD para comprobar si hay reversibilidad de la obstrucción del flujo aéreo respecto a la situación basal.
Dado que en nuestro ambulatorio no se dispone de tapiz rodante o bicicleta ergométrica para realizar el test, la carrera libre la realizan en el parque que hay justo detrás (parque de los Derechos Humanos). Realizan una carrera libre de 6 minutos a una intensidad suficiente para alcanzar una frecuencia cardiaca superior al 85% de la FC máxima para su edad (FC máxima = 210 - edad en años).
La finalización de la carrera ha de ser brusca, sin tiempo de reposo, y en cuanto llegan a la consulta se registran de nuevo la SpO2 y FC, se les ausculta y se realiza la segunda espirometría.
La segunda espirometría se ha de iniciar a los 0-2 minutos de cesar el esfuerzo. En los protocolos indican que hay que repetir las espirometrías de forma seriada a los 5, 10, 15 minutos y opcionalmente a los 20 y 30 minutos, salvo que el FEV1 baje de forma significativa en un tiempo inferior, momento en que se suspende la prueba y se administra un broncodilatador al paciente.
En nuestro centro debido al tipo de espirómetro, tipo de consulta y tiempo disponible, se realiza la segunda espirometría tras la carrera entre los 5 y 10 minutos, ya que revisando la bibliografía actual se observó que la máxima broncobstrucción suele ocurrir entre los 3 y 15 minutos después de finalizar el ejercicio7. Por tanto, realizándola a los 5 y 10 minutos, ya podemos observar con fiabilidad si la broncoobstrucción se produce.
Tanto en la segunda espirometría (al llegar tras la carrera), como en la tercera (10 minutos después del esfuerzo), se registran la FC y la SpO2, además de realizar una auscultación.
La variable espirométrica empleada para valorar la hiperrespuesta es el FEV1, y habitualmente se considera positivo el descenso porcentual del FEV1 tras el ejercicio respecto al valor basal del 12% (>10% en adolescentes y adultos). Hay que destacar que si se obtiene un resultado negativo en el test de carrera libre este no excluye el diagnóstico de asma inducido por el ejercicio.
En el caso de que el FEV1 haya bajado de forma significativa o si el pediatra lo solicita, se realiza una cuarta espirometría con PBD.
Si durante la realización de cualquier prueba ha habido alguna incidencia se deja constancia en la historia clínica del paciente.
RESULTADOS
El total de pacientes atendidos fueron 67 durante dicho periodo de tiempo. Se realizaron 104 citaciones para espirometrías, pero no asistieron a la realización el 18,3% (n = 19) de los niños citados, habitualmente por enfermedad o porque anularon visita por estar de excursión, colonias o exámenes.
Hubo 4 espirometrías que se decidieron reprogramar, ya que en 3 de ellas no se cumplieron los criterios de aceptabilidad y reproducibilidad, ya sea porque el paciente no realizaba bien la técnica o porque se precisaron demasiadas repeticiones. Y en 1 ocasión se suspendió la prueba por problemas técnicos con el espirómetro.
De las diferentes pruebas que se realizan (espirometría forzada, espirometría con prueba de broncodilatación y espirometría con carrera libre), donde mayor absentismo ha habido ha sido en las citas programadas para espirometrías con ejercicio, donde se han ausentado el 9,9% (n = 8) pacientes.
Se realizaron 13 espirometrías basales para el control de asma y para el control del tratamiento de base. En cuanto a las realizadas para el control de la medicación, en la mayoría se observó una mejoría, menos en un paciente que refirió que no cumplía el tratamiento prescrito.
Se realizaron 26 espirometrías con PBD, que fueron derivadas por los pediatras del centro, para confirmar diagnóstico de asma por síntomas y signos clínicos o por repetición de bronquitis agudas obstructivas (BAO).
De las 26 espirometrías con prueba broncodilatadora, 15 dieron una PBD negativa y 11 una PBD positiva.
Se programaron 42 espirometrías con ejercicio, en las que los motivos de derivación por parte de los pediatras del centro fueron presencia de tos, disnea de esfuerzo, cansancio intenso tras ejercicio y/o asma.
De las 42 espirometrías programadas, diez no se pudieron realizar correctamente: dos se aplazaron por técnica incorrecta y ocho por espirometría basal alterada (FVC y FEV1 fueron inferiores al 80%). En estas ocho espirometrías se decidió completar el estudio con una PBD que resulto positiva en siete casos y negativa en uno. En el caso de PBD negativa, no se observó mejoría en los valores de la espirometría, pero se apreció mejoría clínica (los sibilantes previamente auscultados mejoraron).
En nueve de las 32 espirometrías con ejercicio realizadas se observó una disminución de los valores FVC y FEV1 tras el ejercicio inmediato o a los 5-10 minutos, siendo estos pacientes diagnosticados de asma de esfuerzo.
En 23 de las pruebas no había diferencias significativas comparando espirometrías basales con espirometrías con ejercicio. De estas 23, a pesar de que durante el ejercicio no hubo disminución significativa de FVC y FEV1, sí que se obtuvo una PDB positiva sobre la basal en cinco de ellas.
DISCUSIÓN
Este artículo describe la experiencia en la realización de espirometría forzada y prueba de esfuerzo en la población pediátrica en un centro de Atención Primaria.
Hoy en día el principal objetivo en el tratamiento de asma es el control de la enfermedad. Esta patología supone un coste aproximado de 535 millones de euros/año en España. Gran parte de este coste se debe a causas prevenibles como atención en urgencias, ya sea en Atención Primaria como en hospital, e ingresos hospitalarios. Para poder reducir este importe se deberían realizar tanto intervenciones de prevención como de manejo de la enfermedad.
El pediatra de Atención Primaria constituye el primer contacto de la población infantil con el sistema sanitario, y es el encargado, junto con la enfermera de Pediatría, del seguimiento de la población sana además de realizar el control y tratamiento de las enfermedades infantiles crónicas, como el asma.
Por tanto, sería adecuado que los profesionales más próximos al paciente, pudieran realizar un seguimiento más exhaustivo y cercano realizando pruebas funcionales para diagnosticar y controlar el asma. Al acercar las pruebas al domicilio del paciente, creemos que se podría reducir el absentismo habitual a este tipo de pruebas, facilitando que el paciente esté correctamente controlado. En nuestro estudio tuvimos un 23% de absentismo, siendo el 40% de las ausencias en las visitas para realizar test de ejercicio. Nos hubiese gustado poder comparar el absentismo de esta misma prueba en atención especializada o en otros centros de Atención Primaria pero no se han encontrado datos actuales.
En nuestra experiencia hemos conseguido realizar un 95,5% de espirometrías con criterios de calidad en Atención Primaria y en la población preescolar. Es cierto que, es necesario un equipamiento adecuado con técnicas de incentivación apropiadas a la edad, y un personal sanitario formado en espirometrías y en la atención a población pediátrica. En cuanto a la formación del personal creemos que actualmente es insuficiente, y se debería de promover más formación continuada para actualizar conocimientos periódicamente.
Además, para poder garantizar una correcta realización de las espirometrías se necesita tiempo, paciencia y organización para aprovechar al máximo el espacio del que se dispone y los tiempos.
Hay que destacar que la mayoría de nuestros pacientes no tenían experiencia previa en la realización de espirometrías, y el resultado de maniobras adecuadas ha sido gratamente elevado.
El motivo más frecuente, por el que algunas espirometrías requirieron nueva citación, fue que no cumplían los requerimientos de calidad propuestos para aceptar esta exploración.
En cuanto a los errores más frecuentes, la terminación prematura de la maniobra fue el primer motivo y el segundo error fue realizar un esfuerzo inadecuado sin pico de flujo.
A pesar de que los niños tienen muchas menos limitaciones físicas comparados con los adultos o con los adolescentes, prestan menos interés tras un número elevado de maniobras, así que consideramos que hay que repetir la maniobra, siempre y cuando, el niño siga estimulado.
Este estudio descriptivo tiene fortalezas y debilidades.
En cuanto a fortalezas podemos destacar que no hemos encontrado otros estudios similares publicados y realizados en España por profesionales de enfermería y, por tanto, este artículo puede ayudar a dar a conocer nuestra experiencia, y animar a otros centros a realizarla, ya que tanto para los profesionales como para los usuarios es una experiencia muy positiva.
Otro punto fuerte del estudio es que siempre se haya utilizado un mismo equipo de espirometría e interviniendo técnicos bien cualificados.
Además, se dispone de un parque colindante a nuestro centro, hecho que permite que los niños realicen el ejercicio en un entorno sin riesgos.
Del mismo modo, la lectura de las pruebas es llevada a cabo por el mismo equipo que las realiza y por tanto utiliza los mismos criterios, y además también es revisada por el pediatra de referencia del paciente.
En cuando a debilidades o limitaciones, consideramos que en primer lugar es un estudio con una muestra de población pequeña ya que solo se ha realizado con nuestra población de referencia y con los datos del último año. Por tanto, no se puede valorar si el número de espirometrías realizadas es suficiente para poder sacar conclusiones.
Por otro lado, como no se han encontrado otros estudios con una metodología similar, no se ha podido comparar los resultados obtenidos.
CONCLUSIONES
En conclusión, es posible realizar pruebas de función pulmonar como la espirometría forzada, la espirometría forzada con PBD y la provocación bronquial, con resultados de calidad en el ámbito de Atención Primaria pediátrica, siempre y cuando sean realizados por profesionales especializados.
La realización de dicha técnica amplía la cartera de servicios a los usuarios, disminuyendo las derivaciones a centros especializados y, por tanto, las listas de espera. Además, favorece un seguimiento más estrecho de nuestra población asignada, con el fin de conseguir un mayor control de la enfermedad.
Finalmente, con este artículo se quiere contribuir a asentar las bases para adoptar medidas que permitan utilizar los recursos disponibles en los centros de Atención Primaria, y poner en marcha circuitos similares liderados por enfermeras.
CONFLICTO DE INTERESES
Las autoras declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
BAO: bronquitis agudas obstructivas ● FC: frecuencia cardiaca ● FEV1: volumen espirado forzado en el primer segundo ● FVC: capacidad vital forzada ● PBD: prueba broncodilatadora ● RV: volumen residual ● SpO2: saturación transcutánea de oxígeno ● TLC: capacidad pulmonar total.
AGRADECIMIENTOS
Nuestro sincero agradecimiento a todos los compañeros de Equipo Pediátrico La Marina-Magoria y a los residentes médicos y de enfermería, por su apoyo y sus sugerencias en la redacción de este.
BIBLIOGRAFÍA
- Sacristán Martín A, Arribas Santiago C, Camina Gutiérrez A, Machín Rodríguez E, Santos García J. Características del asma infantil en Atención Primaria. Mejora del seguimiento. Rev Pediatr Aten Primaria. 2008;19:593-601.
- GEMA. GEMA 5.0. Guía española para el manejo del asma. En: GEMA [en línea] [consultado el 21/10/2021]. Disponible en www.gemasma.com/
- Asensí Monzó MT, Duelo Marcos M, García Merino Á. Manejo integral del asma en Atención Primaria. AEPap (ed.). Curso Actualización Pediatría 2018. Madrid: Lúa Ediciones 3.0. 2018. p. 489-506.
- Úbeda-Sansano MI, Cano-Garcinuño A, Rueda-Esteban S, Praena-Crespo M. Resources to handle childhood asthma in Spain: The role of plans and guides and the participation of nurses. Allergol Immunopathol (Madr). 2018;46:361-9.
- Blasco Bravo AJ, Pérez-Yarza EG, De Mercado PLY, Perales AB, Díaz Vázquez CA, Moreno Galdó A. Coste del asma en Pediatría en España: un modelo de evaluación de costes basado en la prevalencia. An Pediatr (Barc). 2011;74:145-53.
- Oliva Hernández A, Callejón Callejón A. Espirometría en el niño colaborador. Rev Esp Pediatr. 2012;68:104-13.
- Jat KR. Spirometry in children. Prim Care Respir J. 2013;22:221-9.
- Bercedo Sanz A, Úbeda Sansano I, Juliá Benito J, Praeno Crespo M, Grupo de Vías Respiratorias de la Asociación Española de Pediatría de Atención Primaria. Protocolo de Espirometría. El pediatra de Atención Primaria y la espirometría. En: Respirar.org [en línea] [consultado el 21/10/2021]. Disponible en www.respirar.org/images/pdf/grupovias/Protocolo_espirometria_GVR_2020-finalb.pdf
- Olaguíbel Rivera JM, Álvarez Puebla MJ, Vela Vizcaino C, Cambra Contín K, Uribe San Martín MP, De Esteban Chocarro B. Calidad de la espirometría en preeescolares. An Sist Sanit Navar. 2014;37:81-9.
- Comité de Enfermería de la SEICAP. Espirometría forzada en Pediatría. En: SEICAP [en línea] [consultado el 21/10/2021]. Disponible en www.seicap.es/espirometria-forzada-en-niños_38884.pdf
- García Merino Á, Carvajal Urueña I, Blanco González J. Espirometría básica en Pediatría de Atención Primaria. En: V Reunión anual de la Sociedad Asturiana de Pediatría de Atención Primaria [en línea] [consultado el 21/10/2021]. Disponible en https://cutt.ly/YRbQuXv
- Boqué Genovard M, Zamora Andreu B, Puigserver Sacares B. Estudio de la situación actual en el tratamiento del asma pediátrico en Atención Primaria de Mallorca. Rev Pediatr Aten Primaria. 2007;9:375-84.