
Vol. 22 - Num. 86
Originales
Dermatitis perianal estreptocócica: estudio clínico-epidemiológico de 95 episodios
Jacinto Martínez Blancoa, Laura Míguez Martínb, Noelia Valverde Pérezc
aPediatra. CS El Coto. Gijón. Asturias. España.
bPediatra. Área V. Gijón. Asturias. España.
cMIR-Pediatría. Hospital de Cabueñes. Gijón. Asturias. España.
Correspondencia: J Martínez. Correo electrónico: jacintomartinezblanco@hotmail.com
Cómo citar este artículo: Martínez Blanco J, Míguez Martín L, Valverde Pérez N. Dermatitis perianal estreptocócica: estudio clínico-epidemiológico de 95 episodios. Rev Pediatr Aten Primaria. 2020;22:131-8.
Publicado en Internet: 25-05-2020 - Número de visitas: 39911
Resumen
Introducción y objetivos: analizar las características clínico-epidemiológicas de la dermatitis perianal por estreptococo betahemolítico del grupo A (SBHGA).
Material y métodos: serie de casos con recogida prospectiva de datos durante un periodo de ocho años en una consulta de Pediatría.
Resultados: se diagnosticaron 95 episodios (1/298 consultas) en 76 niños (varones/mujeres: 1,6/1). Edad media 4,5 años. Padecieron más de un episodio 13 pacientes con un total de 19 episodios sucesivos: 10 de ellos en un periodo inferior a 6 meses respecto al anterior (11% del total de episodios). Los motivos de consulta más frecuentes fueron: prurito, sangrado, dolor, estreñimiento y eritema perianal. El tratamiento se realizó por vía tópica en el 70% de los primeros episodios y combinado (tópico y sistémico) en el 68% de los sucesivos. Se constató un fracaso terapéutico inicial en tres episodios. La distribución estacional fue similar a la de faringoamigdalitis y escarlatinas por SBHGA diagnosticadas en el mismo periodo.
Conclusiones: cinco motivos de consulta (prurito, sangrado, dolor, estreñimiento y eritema perianal), solos o combinados, estuvieron presentes en el 92% de los episodios. En solo el 17% de los primeros episodios el eritema perianal fue motivo de consulta. Puede ser tenue, sus bordes no siempre son nítidos y en ocasiones asocia lesiones satélites.
Palabras clave
● Dermatitis perianal ● Dermatitis perianal estreptocócica ● Eritema ● Estreptococo betahemolítico del grupo AINTRODUCCIÓN
Amren et al.1 describen en 1966 una nueva enfermedad asociada al estreptococo (Streptococcus pyogenes) betahemolítico del grupo A (SBHGA), a la que denominan celulitis perianal. En 1987, Kokx et al.2 la denominaron enfermedad perianal estreptocócica, al no tratarse de una celulitis. Montemarano et al.3 publican en 1993 un caso asociado a estafilococo dorado. Diversos autores utilizan el término dermatitis o enfermedad estreptocócica perineal al asociar las infecciones de dicha área.
La dermatitis perianal está causada habitualmente en la infancia por el SBHGA y, en un número menor de ocasiones, por estreptococo betahemolítico de los grupos B, C o G4,5 y por estafilococo dorado (Staphylococcus aureus)3,6, entre otros. Su incidencia se estima entre 1/3007y 1/20001 consultas pediátricas, y puede estar subestimada. Afecta más frecuentemente a varones, con una edad media entre 3 y 5 años8-10.
Su forma de presentación suele ser eritema perianal bien delimitado (90-100%), ocasionalmente con lesiones satélites y con posible afectación interglútea; prurito perianal (50-100% de los casos); dolor rectal o con la defecación (17-50%); deposiciones con sangre (13-50%); estreñimiento (15-50%); fisuras anales (10-50%) e irritabilidad11. Puede estar asociado a: dolor abdominal, psoriasis en gotas, vulvovaginitis, balanopostitis, dermatitis atópica, disuria, secreción perianal y erupción escarlatiniforme12,16. No cursa con afectación sistémica.
Un 30-95% de los pacientes con dermatitis perianal son portadores faríngeos o padecen faringitis estreptocócica. Únicamente un 6% de las faringitis por SBHGA ocurren en portadores perianales17, no siendo posible determinar si la colonización faríngea precede o sigue a la perineal2,18,19. Menos del 1% de niños sanos son portadores perianales de esta bacteria17.
Existen diversas hipótesis respecto al modo de transmisión: agua del baño, transporte gastrointestinal o aéreo, portadores sanos, fómites, autoinoculación. Se han publicado brotes en el ámbito familiar, en guarderías y hospitales4,20,21.
Al diagnóstico se llega por la clínica y la exploración física. La confirmación se realiza bien con test de detección rápida de SBHGA (sensibilidad: 77,9-98%, especificidad: 73-100% para muestras extrafaríngeas9,22), o con cultivo (indicando al laboratorio la utilización de medios adecuados)19,20,23.
El diagnóstico diferencial incluye: dermatitis del pañal, parasitosis intestinal, candidiasis, dermatitis atópica, psoriasis, enfermedad inflamatoria intestinal, histiocitosis, déficit de zinc, liquen escleroso, hemorroides y abuso sexual, entre otros procesos.
El tratamiento da lugar a una mejoría rápida de los síntomas y puede realizarse por vía sistémica, con antibióticos orales (fundamentalmente penicilina o amoxicilina, otras alternativas no han sido evaluadas, excepto en el caso de la cefuroxima24), por vía tópica (ácido fusídico o mupirocina principalmente) o por ambas vías simultáneamente. Las recaídas son frecuentes, especialmente con tratamiento oral exclusivo.
El objetivo principal de este estudio es describir las características clínicas y epidemiológicas de las dermatitis perianales en una consulta de Pediatría de Atención Primaria. El objetivo secundario es valorar su relación temporal con las infecciones faríngeas por SBHGA y la aparición de recidivas.
MATERIAL Y MÉTODOS
Se realizó un estudio observacional prospectivo, longitudinal y descriptivo de la serie de casos de dermatitis perianales SBHGA positivas diagnosticadas entre el 01/04/2011 y el 31/03/2019 en una consulta de Pediatría de un centro de salud en Gijón (Asturias, España) que atiende a niños de entre 0 y 13 años.
Se incluyeron en el estudio aquellos pacientes cuyos motivos de consulta o exploración fueron compatibles con dermatitis perianal y con determinación rápida del antígeno SBHGA (kit OSOM Strep A de Genzyme) en la región perianal positiva, recogiendo: fecha de consulta, número de historia clínica, edad, sexo, motivo de consulta, clínica, exploración, tratamiento y recaídas. La exploración del área perianal fue realizada por el mismo investigador clasificando el eritema en base a su extensión e intensidad: nulo, mínimo (apenas perceptible), leve (escasa extensión e intensidad), moderado (más extenso o intenso que el leve y menos que el intenso) e intenso (muy extenso e intenso).
Se analizó el número de recaídas con test de SBHGA positivo en las sucesivas consultas y dos meses después de finalizada la recogida de casos se procedió a revisar las historias clínicas y contactar telefónicamente con los familiares.
De forma retrospectiva se determinó el número total de consultas (excluidas las sucesivas y telefónicas) así como fechas de consulta, edad y sexo de los pacientes con diagnóstico de faringoamigdalitis o escarlatinas con test SBHGA positivas que fueron atendidos en la referida consulta y en dicho periodo.
Para describir las variables cuantitativas se emplearon la media y la desviación típica, mientras que para las variables cualitativas se recurrió a porcentajes. Para realizar los contrastes de hipótesis se empleó la t de Student (para comparar el comportamiento de una variable cuantitativa en dos grupos) y las tablas de contingencia y el test χ2 de Pearson para estudiar la relación entre variables cualitativas. En el caso de tablas dos por dos se empleó el test exacto de Fisher.
Este estudio fue aprobado por el Comité de Ética en investigación del Principado de Asturias. Se obtuvo el consentimiento informado de los padres o tutores, así como para la toma de fotografías. Al tratarse de un estudio no experimental ni intervencionista, todos los padres consintieron su participación.
RESULTADOS
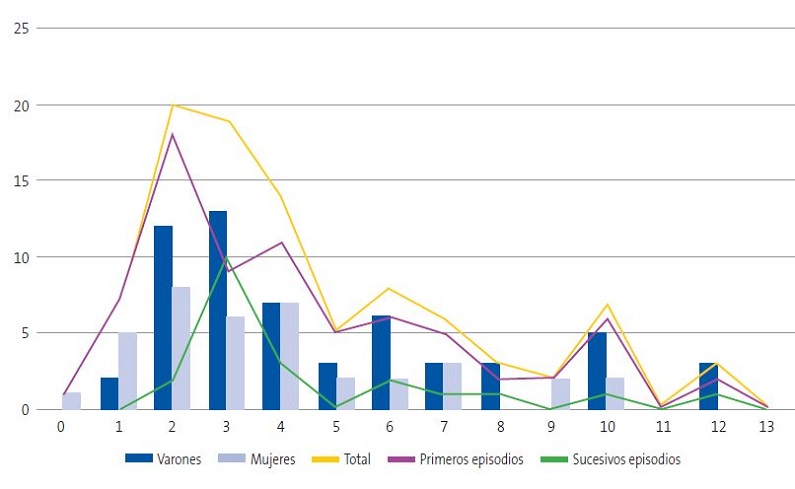
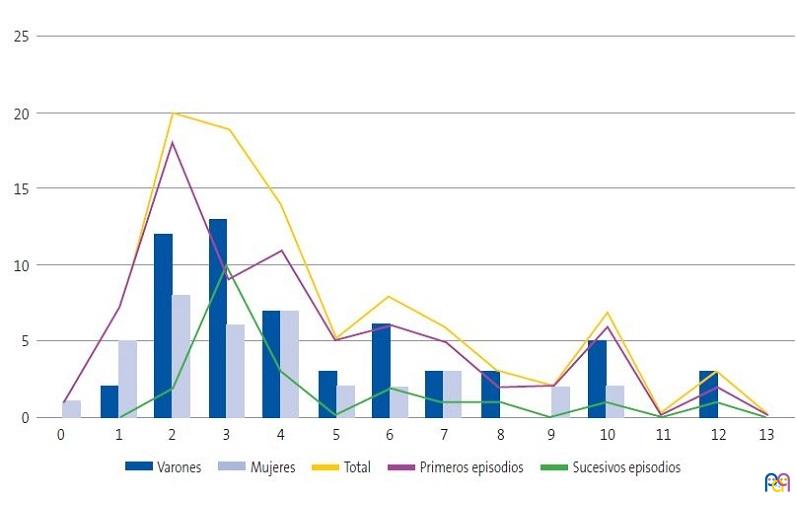
Durante el periodo de estudio (ocho años) se atendieron 28 328 nuevas consultas, siendo diagnosticados 95 episodios de dermatitis perianal (1/298 consultas) mediante test de SBHGA en 76 niños, 62% del sexo masculino y 38% del femenino, diferencia estadísticamente significativa (p = 0,0034) y no encontrándose asociación entre edad y sexo significativa (p = 0,2416) (Fig. 1).
| Figura 1. Distribución de las dermatitis perianales estreptocócicas por edad, sexo y tipo de episodio |
|---|
 |
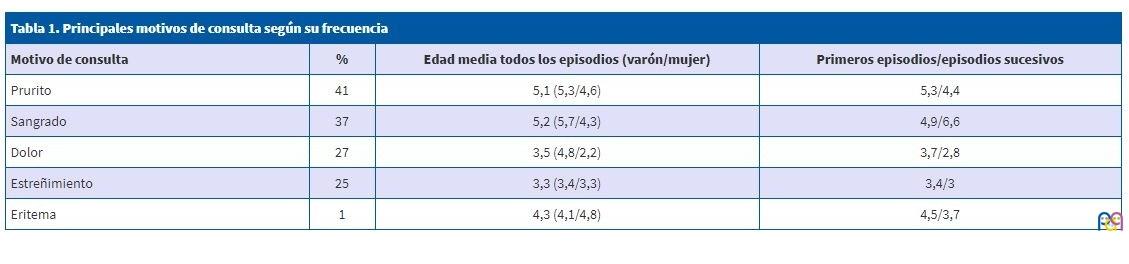
Los motivos de consulta más frecuentes registrados han sido prurito, sangrado con la deposición o perianal, dolor con la deposición o perianal, estreñimiento y eritema (Tabla 1). Con menor frecuencia fisuras (seis episodios), fiebre (todos con odinofagia y test de SBHGA faríngeo positivo), odinofagia, vulvitis-flujo vulvar (cuatro episodios), abdominalgia, descartar parásitos intestinales (tres episodios), disuria (dos episodios), eritema del pañal, balanitis, parafimosis, foliculitis, encopresis, masa, descartar hemorroides (un episodio cada uno).
| Tabla 1. Principales motivos de consulta según su frecuencia | |||
|---|---|---|---|
| Motivo de consulta | Porcentaje | Edad media todos los episodios (varón/mujer) | Primeros episodios/episodios sucesivos |
| Prurito | 41 | 5,1 (5,3/4,6) | 5,3/4,4 |
| Sangrado | 37 | 5,2 (5,7/4,3) | 4,9/6,6 |
| Dolor | 27 | 3,5 (4,8/2,2) | 3,7/2,8 |
| Estreñimiento | 25 | 3,3 (3,4/3,3) | 3,4/3 |
| Eritema | 1 | 4,3 (4,1/4,8) | 4,5/3,7 |
Un total de 63 niños tuvieron un único episodio y 13 (ocho varones y cinco mujeres; 17% del total de episodios) padecieron más de uno (diez pacientes dos episodios; y tres pacientes con tres, cuatro y cinco episodios respectivamente). Se detectaron diez recurrencias en un periodo de tiempo inferior a seis meses del episodio previo (11% del total) y nueve en un periodo superior. Los episodios sucesivos tuvieron lugar entre 24 y 740 días del episodio anterior (media: 265 días).
En los episodios iniciales no hubo relación estadística significativa entre género (χ2 0,0006, p = 0,9803), edad (Welch Two Sample t = 0,641, p = 0,537), o ninguno de los cinco principales motivos de consulta (dolor: p = 0,6771, eritema: p = 1, estreñimiento, p = 0,67771, prurito: p = 0,1368, sangrado: p = 0,1358) y recaída antes de los seis meses.
Relacionando los cinco principales motivos de consulta de los primeros episodios con el género: el eritema perianal se consulta con más frecuencia en el grupo de varones (25,5%) respecto al de mujeres (3,4%) (p = 0,0132); al igual que sucede con el prurito (48,9/24,1%) (p = 0,0523), no existiendo diferencias significativas en el resto (dolor p = 0,3059, estreñimiento p = 0,3059, sangrado p = 1). Si esta relación la establecemos con la edad: se observa que esta es menor cuando el motivo de consulta es estreñimiento (p = 0,0355) y mayor en caso de prurito (p = 0,0038); no habiendo diferencia significativa en el resto (dolor p = 0,1610, sangrado p = 0,3138, eritema p = 0,8714). Analizando el motivo de consulta por sexos y edad, las niñas consultan por dolor a menor edad que los niños (2,2/5,0; p = 0,0019), no habiendo diferencias significativas en el resto (sangrado p = 0,1979, estreñimiento p = 0,7418, prurito p = 0,2547).
La clínica que no fue motivo de consulta consistió en 17 casos más de estreñimiento; cuatro de dolor perianal o al defecar; dos de eritema; tres de sangre en heces o perianal y uno de prurito.
El eritema fue nulo en siete ocasiones, mínimo en 14, leve en 38, moderado en 20 e intenso en 15 (Fig. 2); en una ocasión no quedó constancia de su intensidad. Hubo presencia de lesiones satélites en ocho episodios (Fig. 3), vesículas en tres y límites imprecisos en tres.
| Figura 2. Paciente con eritema intenso |
|---|
 |

| Figura 3. Paciente con lesiones satélites |
|---|
 |

Se registró el tiempo de evolución previo al diagnóstico en 37 episodios, siendo de una semana o inferior en 30; dos semanas en tres; tres semanas en uno y cuatro semanas en tres.
El tratamiento tópico exclusivo se administró en 59 ocasiones (62% del total), 53 de los primeros episodios (70% de dichos casos) y en seis de los sucesivos (32%). Empleando ácido fusídico en 53 ocasiones y mupirocina en seis.
El tratamiento combinado (tópico y sistémico vía oral) se utilizó en 36 ocasiones (38% del total), 23 de los primeros episodios (30%) y 13 de los sucesivos (68%). Administrando amoxicilina y ácido fusídico en 26, amoxicilina y mupirocina en nueve y cefuroxima más mupirocina en una ocasión.
Se precisó cambio en el tratamiento en los tres casos de fracaso terapéutico (3%):
- Episodio número 38: tratamiento: ácido fusídico al que se añade posteriormente amoxicilina por fracaso terapéutico. Al persistir la clínica y el test perianal positivo, se modifica, iniciando cefuroxima y manteniendo el ácido fusídico con control clínico y test negativo. Esta paciente tuvo 3 nuevos episodios a los 21, 29 y 31 meses del inicial.
- Episodio número 75: tratamiento con ácido fusídico, control mediante test positivo. Se añade amoxicilina y ante la persistencia de test positivo se cambia a cerfuroxima. No presentó recurrencias.
- Episodio número 95: quinto episodio. Tratamiento: cefuroxima y mupirocina sin mejoría y persistiendo test positivo. Se cambia antibioterapia oral a amoxicilina y se añade rifampicina los cuatro últimos días (pauta similar a la descrita por Kokx2 para casos persistentes) con control posterior negativo. No se registraron más episodios hasta la actualidad.
Se observaron recurrencias en 15/59 tratamientos tópicos y 4/36 tratamientos combinados.
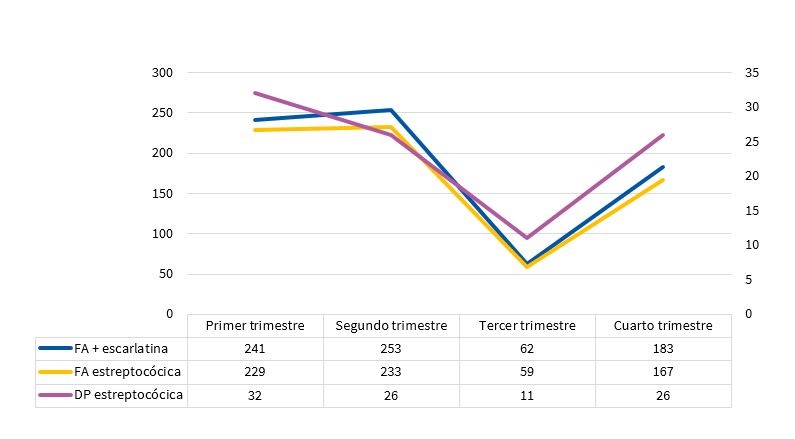
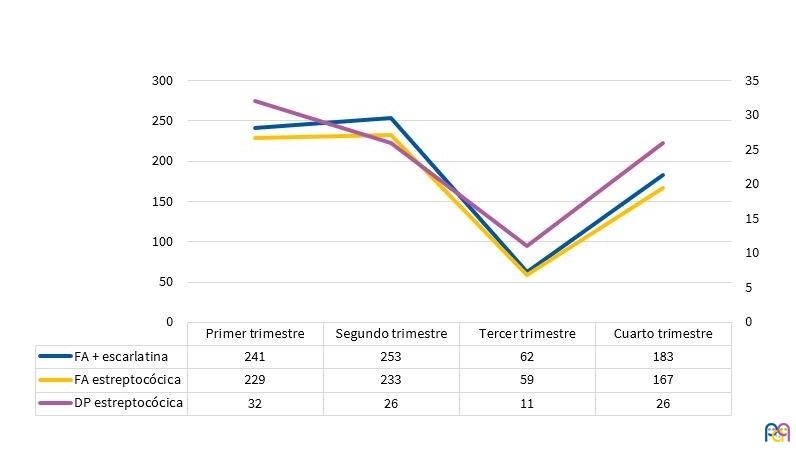
Se constató una preferencia estacional con descenso estadísticamente significativo (p = 0,0174) en el tercer trimestre, siguiendo una distribución similar a la de faringoamigdalitis (p = 0,0000) y faringoamigdalitis más escarlatinas diagnosticadas mediante test de SBHGA en dicho periodo (p = 0,0000) (Fig. 4), con una proporción de 1 dermatitis perianal por SBHGA por cada 7,8 faringoamigdalitis y escarlatinas SBHGA positivas (1/7,3 si no tenemos en cuenta las escarlatinas).
| Figura 4. Distribución estacional de las infecciones estreptocócicas |
|---|
 |
DISCUSIÓN
El principal objetivo de este estudio es la descripción de las características clínico-epidemiológicas de la dermatitis perianal por SBHGA encontrando una frecuencia de casos por primeras consultas similar a lo publicado por Mogielnicky et al. (1/300)7.
Se constató un predominio masculino, tal y como se refiere en la bibliografía, aunque en una proporción inferior a algunas de las publicaciones consultadas8,10 y similar a otras12,13.
La edad media fue similar a lo publicado por otros autores. No se encontraron diferencias en porcentaje en cuanto a la distribución por género entre los primeros episodios y los sucesivos, al igual que Clegg et al.18 y Olson et al.10.
La clínica, sangrado (40%), estreñimiento (48%), prurito (42%; más frecuente en varones), dolor (32%; más frecuente en mujeres) y fisuras (16%), concuerda en porcentaje con las referencias consultadas.
El eritema como motivo de consulta se da en menos del 50% de los casos, coincidiendo Mogielnicky et al.7.
En 21 de 94 ocasiones (22%) el eritema fue nulo o mínimo (motivo por el que puede pasar desapercibido), encontrando lesiones satélites, vesículas o límites imprecisos en pocas ocasiones (13%), lo que no descarta el diagnóstico.
Aunque se requieren más estudios (este no fue diseñado con dicha finalidad), posiblemente el tratamiento tópico exclusivo sea suficiente en la mayoría de los casos (en los dos casos de fracaso terapéutico por vía tópica, el tratamiento combinado posterior fue ineficaz, precisando un nuevo cambio de terapia), con la ventaja añadida de cubrir una posible asociación con otras bacterias.
El número de recurrencias está en el límite inferior de la bibliografía consultada (11-44%), posiblemente por el escaso tiempo medio entre la aparición de los síntomas y el diagnóstico (son factores predictores de recurrencia la mayor duración de los síntomas y existencia de familiares directos con infección estreptocócica13,18) y el no haber utilizado tratamientos orales exclusivos.
La distribución estacional coincide con lo descrito en la literatura médica, siguiendo la de las faringitis EBHGA4,6,25.
El estudio posee ciertas limitaciones: los datos recogidos proceden de una única consulta y la confirmación diagnóstica del cuadro clínico se realizó únicamente con test de SBHGA. El grado de eritema se valoró subjetivamente, aunque siempre por el mismo investigador. El tratamiento se realizó sin asignar grupos dado el carácter meramente observacional del estudio.
CONCLUSIONES
Se encontraron diferencias estadísticas significativas en cuanto a la distribución de las dermatitis por género.
Cinco motivos de consulta (prurito, sangre con la defecación o perianal, dolor perianal o con la defecación, estreñimiento y eritema perianal) solos o combinados, estuvieron presentes en el 92% de los diagnósticos. Relacionando los motivos de consulta en los primeros episodios con el género: el eritema perianal y el prurito se consultan con más frecuencia en el grupo de varones; si los relacionamos con la edad: esta tiende a ser menor cuando el motivo de consulta es estreñimiento y mayor en el caso de prurito. El dolor es motivo de consulta a menor edad en las niñas que en los niños.
El eritema perianal como motivo de consulta tuvo lugar solo en el 17% de los primeros episodios. En la exploración el eritema perianal no siempre está presente o puede ser tenue en una cantidad no despreciable de casos. Sus bordes no siempre son nítidos y pueden observarse lesiones satélites o vesículas por lo que si la clínica es sugestiva debería confirmarse el diagnóstico ya que en caso de ser positivo la evolución es muy favorable con el tratamiento adecuado.
Aunque el estudio no fue diseñado para ello, podría ser inicialmente suficiente el tratamiento tópico exclusivo, dado el escaso número de fracasos y que en dos de ellos fracasó también el primer tratamiento combinado (tópico más oral), no pudiendo sacar conclusiones en cuanto a las recurrencias.
La distribución estacional es similar a la de las faringoamigdalitis estreptocócicas y menor en el tercer trimestre del año.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
SBHGA: estreptococo betahemolítico del grupo A.
AGRADECIMIENTOS
Al profesor Norberto Octavio Corral Blanco (catedrático de estadística de la Universidad de Oviedo), por su contribución en el análisis estadístico de los datos.
BIBLIOGRAFÍA
- Amren DP, Anderson AS, Wannamaker LW. Perianal cellulites associated with group A streptococci. Am J Dis Child. 1966;112:546-52.
- Kokx NP, Comstok JA, Facklam RR. Streptococcal perianal disease in children. Pediatrics. 1987;80:659-63.
- Montemarano AD, James WD. Staphylococcus aureus as a cause of perianal dermatitis. Pediatr Dermatol. 1993;10:259-62.
- Zhang C, Haber RM. The ABCs of perineal streptococcal dermatitis. Case, series and review of the literature. J Cutan Med Surg. 2017;21:102-7.
- Šterbenc A, Seme K, Lah LL, Točkova O, Trop TK, Svent-Kucina, et al. Microbiological characteristics of perianal streptococcal dermatitis: a retrospective study of 105 patients in a 10-year period. Acta Dermatovenerol Alp Pannonica Adriat. 2016;25:73-6.
- Heath C, Desai N, Silverbeg NB. Recent microbiological shifts in perianal bacterial dermatitis: Staphylococcus aureus predominance. Pediatr Dermatol. 2009;26:696-700.
- Mogielnicki NP, Schwartzman JD, Elliott JA. Perineal group Streptococcal disease in a pediatric practice. Pediatrics. 2000;106:276-81.
- Mostafa WZ, Arnaout HH, El-Lawindi MI, El-Abidin YZ. An epidemiologic study of perianal dermatitis among children in Egypt. Dermatol. 1997;14:351-4.
- Cohen R, Levy C, Bonacorsi S, Wollner A, Koskas M, Jung C, et al. Diagnostic accuracy of clinical symptoms and rapid diagnostic test in-group A streptococcal perianal infections in children. Clin Infect Dis. 2015;60:267-70.
- Olson D, Edmonson MB. Outcomes in children treated for perineal group A beta-hemolytic streptococcal dermatitis. Pediatr Infect Dis J. 2011;30:933-6.
- Shouval DS, Schurr D, Nussinovith M. Presentation of perianal group a streptococcal infection as irritability among children. Pediatr Dermatol. 2008;25:568-70.
- Redondo Mateo J, Carrero González PA, Sierra Pérez E. Dermatitis estreptocócica perianal. Actas Dermosifiliogr. 2002;93:243-6.
- Echevarría Fernández M, González Martínez F, Marañón Pardillo R. Factores epidemiológicos implicados en la enfermedad perianal estreptocócica. An Pediatr (Barc). 2009;70:511-2.
- García-Osés I, Martínez de Zabarte Fernández JM, Puig García C, Arnal Alonso JM. Pensando en la dermatitis perianal. Rev Pediatr Aten Primaria. 2015;17:51-5.
- Patrizi A, Costa AM, Fiorillo L, Neri I. Perianal streptococcal dermatitis associated with guttate psoriasis and/or balanoposthitis: a study of five cases. Pediatr Dermatol. 1994;11:168-71.
- Honig PJ. Guttate psoriasis associated with perianal streptococcal disease. J Pediatr. 1988;113:1037-9.
- Asnes RS, Vail D, Grebin B, Sprunt K. Anal carrier rate of group A beta-hemolytic streptococci in children with streptococcal pharyngitis. Pediatrics. 1973;52:438-41.
- Clegg HW, Giftos PM, Anderson WE, Kaplan EL, Johonson DR. Clinical perineal streptococcal infection in children: epidemiologic features, low symptomactic recurrence rateafter trearment and risk factors for recurrence. J Pediatr. 2015;167:687-93.
- Krol AL. Perianal streptococcal dermatitis. Pediatr Dermatol. 1990;7:97-100.
- Herbst RA. Perineal streptococcal dermatitis/disease recognition and management. Am J Clin Dermatol. 2003;4:555-60.
- Barzilai A, Choen HA. Isolation of group A streptococci from childrem with perianal cellulitis and from their siblings. Pediatr Infect Dis J. 1998;17:358-60.
- Clegg HW, Dallas SD, Roddey OF, Martín ES, Swetemburg RL, Koonce EW, et al. Extrapharyngeal group A Streptococcus infection: diagnostic accuracy and utility of rapid antigen testing. Pediatr Infect Dis J. 2003;22:726-31.
- Spear RM, Rothbaum RJ, Keating JP, Blaufuss MC. Perianal streptococcal cellulites. J Pediatr. 1985;107:557-9.
- Meury SN, Erb T, Schaad UB, Heininger U. Randomized, comparative efficacy trial of oral penicillin versus cefuroxime for perianal streptococcal dermatitis in children. J Pediatr. 2008;153:799-802.
- Echevarría Fernández M, López-Menchero Oliva JC, Marañón Pardillo R, Míguez Navarro C, Sánchez Sánchez C, Vázquez López P. Aislamiento de estreptococo betahemolítico del grupo A en niños con dermatitis perianal. An Pediatr (Barc). 2006;64:153-7.