
Vol. 21 - Num. 82
Originales
¿Cuánto saben de lactancia los sanitarios del área materno-infantil? Estudio de los 14 hospitales públicos de Castilla y León
M.ª José González Veredaa, M.ª Rosario Bachiller Luqueb, Ana Dorado Díazc, Pilar Martín Pérezc, Tomás Maté Enríquezd, Virtudes Niño Martíne
aMatrona. CS Circular . Valladolid. España.
bPediatra. CS Pilarica Circular. Valladolid. España.
cTécnico en Estadística. Consejería de Sanidad. Valladolid. España.
dGerencia de Atención Primaria de Valladolid Este. Valladolid. España.
eEnfermera. CS La Victoria. Valladolid. España.
Correspondencia: MJ González . Correo electrónico: gonverma@gmail.com
Cómo citar este artículo: González Vereda MJ, Bachiller Luque MR, Dorado Díaz A, Martín Pérez P, Maté Enríquez T, Niño Martín V. ¿Cuánto saben de lactancia los sanitarios del área materno-infantil? Estudio de los 14 hospitales públicos de Castilla y León. Rev Pediatr Aten Primaria. 2019;21:133-46.
Publicado en Internet: 06-06-2019 - Número de visitas: 25880
Resumen
Introducción: la lactancia materna es un objetivo prioritario en salud pública. Los profesionales sanitarios que trabajan en el área materno-infantil de los centros hospitalarios deben poseer un adecuado nivel de conocimientos de lactancia materna.
Material y métodos: estudio descriptivo trasversal realizado durante enero-febrero de 2015 utilizando el cuestionario validado ECola, que se adapta a ginecólogos, matronas y enfermería. Para los técnicos auxiliares de enfermería (TCAE) se utiliza el cuestionario de Temboury Molina MC, modificado por los autores. La población de estudio fueron todos los profesionales sanitarios del área materno-infantil de los 14 hospitales públicos de Castilla y León.
Resultados: en total se recibieron 724 cuestionarios (61,0%). Considerando aceptable el 70% de aciertos (16,8 puntos), los profesionales de enfermería presentan un nivel de conocimientos en lactancia bueno (18,19) y significativamente superior (p <0,05) a los médicos (17,01). Las matronas han presentado la media de aciertos mayor (20,03). Los ginecólogos, con 15,24 puntos, poseen un nivel inferior al recomendable. Los TCAE, con 16,93 puntos, manifiestan conocimientos suficientes, pero en el límite inferior. Se observaron diferencias significativas entre los distintos centros hospitalarios. Globalmente, el nivel de conocimientos de los profesionales del área materno-infantil de los hospitales públicos de Castilla y León es suficiente (17,54).
Conclusiones: el nivel de conocimientos de los profesionales del área materno-infantil en global es aceptable. Algunas categorías profesionales presentan carencias en aspectos trascendentales para el adecuado manejo de la lactancia materna. Se debe considerar la necesidad de implementar formación en lactancia en los currículos formativos, especialmente ginecólogos y TCAE.
Palabras clave
● Conocimiento ● Enfermería ● Lactancia materna ● Matronas ● Médicos ● Técnicos auxiliares en enfermeríaINTRODUCCIÓN
La Estrategia Mundial para la Alimentación del Lactante y del Niño Pequeño (EMALYP) fue desarrollada por la Organización Mundial de la Salud (OMS) y el Fondo de las Naciones Unidas para la Infancia (UNICEF), aprobada por la Asamblea Mundial de la Salud y apoyada por la Junta Ejecutiva de UNICEF en 2002. Esta reafirmó la importancia de promover y apoyar la lactancia materna exclusiva durante los primeros seis meses de vida y mantenerla hasta los dos años, completada con una alimentación sana, segura, apropiada y factible1.
Existen multitud de estudios en España2-5 y en otros países6-9 que hacen una descripción de los factores que van asociados a la prevalencia de la lactancia materna, y en todos se recoge la importancia del profesional sanitario que está en contacto con la madre, tanto en el embarazo como en el parto y posparto.
El primer y probablemente más importante paso para promocionar la lactancia materna consiste en mejorar los conocimientos y las actitudes de los profesionales sanitarios. Estos deben ser capaces de ayudar a las madres a iniciar la lactancia materna y resolver las dudas o problemas que se presenten durante el amamantamiento10. La educación de los progenitores antes y después del parto parece esencial para el éxito de la lactancia11.
Toda lactancia que se pierde por falta de formación de los profesionales es un fracaso del sistema sanitario. Hasta ahora en España no disponíamos de ninguna herramienta validada para estimar los conocimientos en lactancia materna. El riguroso trabajo realizado por Gómez Fernández-Vegue y Menéndez Orenga nos ofrece un valioso instrumento para validar los conocimientos y habilidades en lactancia materna12. La Iniciativa para la Humanización al Nacimiento y la Lactancia (IHAN) elaboró una encuesta para valorar los conocimientos y las necesidades formativas de los profesionales sanitarios respecto a la lactancia materna13, difundida a mediados del 2015, pero no se disponen en la actualidad de datos sobre su utilización en ningún centro hospitalario.
La realidad con respecto a la lactancia materna en Castilla y León es que el 82,7% de las madres inician lactancia materna exclusiva pero solo el 27,1% (intervalo de confianza del 95% [IC 95]: 21,8 a 39,9) la mantienen hasta los seis meses14. No se dispone en Castilla y León de datos sobre conocimientos de los profesionales sanitarios en lactancia.
MATERIAL Y MÉTODOS
Diseño: estudio descriptivo trasversal realizado durante los meses de enero y febrero de 2015.
Población de estudio: todos los profesionales sanitarios de todas las categorías (pediatras, ginecólogos, matronas, enfermería, técnicos auxiliares de enfermería (TCAE) que trabajan en el área materno-infantil de los 14 hospitales de la Gerencia Regional de Salud de la Comunidad Autónoma de Castilla y León (SACYL): 1187 profesionales sanitarios. Se decide encuestar a toda la población de estudio para tener datos de cada hospital.
Métodos: se utilizaron como instrumento de medida dos modelos de cuestionarios:
Cuestionario 1: se trata de la Encuesta sobre Conocimientos en Lactancia Materna (ECola)12, validado para pediatras y MIR de Pediatría. Fue adaptado con la colaboración de los autores, para ginecólogos, matronas y enfermería. Se pidió autorización a los autores y quedó finalmente redactado en 42 preguntas.
Los datos del profesional están recogidos desde la pregunta 1 a la 8. El cuestionario está validado con 24 preguntas puntuables (de la 9 a la 33 incluidas, excepto la pregunta 30, que no se valoró por ser una pregunta abierta). Las preguntas acertadas se valoraron con 1 punto. Los 24 puntos corresponderían a un 100% de aciertos. En el cuestionario se recogen otras preguntas no evaluables (de la pregunta 34 a la 42), relacionadas con actitudes de los profesionales con respecto a la lactancia, que no se han analizado en este estudio.
El cuestionario explora sobre distintas áreas básicas de conocimientos y habilidades en lactancia materna: fisiología de la lactancia, salud pública, problemas de los primeros días, problemas tardíos, evaluación de la toma, condicionantes maternos y actitudes.
Cuestionario 2: este cuestionario fue diseñado por Temboury Molina en el año 200310 para evaluar los conocimientos sobre el manejo de la lactancia materna entre los MIR de Pediatría de España. Por su diseño sencillo y por explorar las áreas de conocimiento que se consideraron importantes, se utilizó para los TCAE con pequeñas adaptaciones. El cuestionario quedó redactado en 29 preguntas. Los datos sociodemográficos se recogen en las preguntas 1 a la 4. Las preguntas de la 5 a la 28 se puntúan los aciertos con 1 punto cada una. La pregunta 29, por ser de respuesta libre, no se valora.
Se exploran áreas básicas de conocimiento sobre lactancia: ventajas de la lactancia natural, peligros de la lactancia artificial, mecanismos de secreción láctea y de succión, habilidades para manejar adecuadamente el inicio y mantenimiento de la lactancia, evaluación de las tomas, manejo de las dificultades y normas del hospital sobre lactancia.
Procedimiento: el acceso a los profesionales se facilitó mediante una carta enviada desde la Dirección General de Salud Pública a los gerentes, directores médicos, directores de enfermería y supervisores de las áreas materno-infantiles de todos los hospitales de Castilla y León. Asimismo, se contactó con la Asociación Castellanoleonesa de Matronas (ASCALEMA) para designar una persona responsable del estudio en cada centro. Los cuestionarios se elaboraron en formato papel de manera anónima y se cumplimentó durante las reuniones de equipo o en las sesiones clínicas, con firma concomitante de consentimiento informado.
Para el análisis de los resultados se utilizó el paquete estadístico versión SPSS: IBM SPSS Statistics Versión 22.0.0.0.
RESULTADOS
Datos sociodemográficos
El perfil de los participantes por categoría profesional en el cuestionario 1 es: 13,3% de neonatólogos, 18,6% de ginecólogos, 24,8% de matronas, 19,7% de enfermería de planta de puerperio, 19,5% de enfermería de planta de neonatos. En su mayoría, son mujeres (87,1%), con una edad media de 43,6 años (±10,6), con hijos (62,5%) y experiencia en lactancia (59,2%).
En el cuestionario 2, el perfil de los participantes TCAE es mujer (95,8%), con una edad media de 53,1 años (±7,5), con hijos (78,8%), la mayoría tienen dos hijos (61,1%).
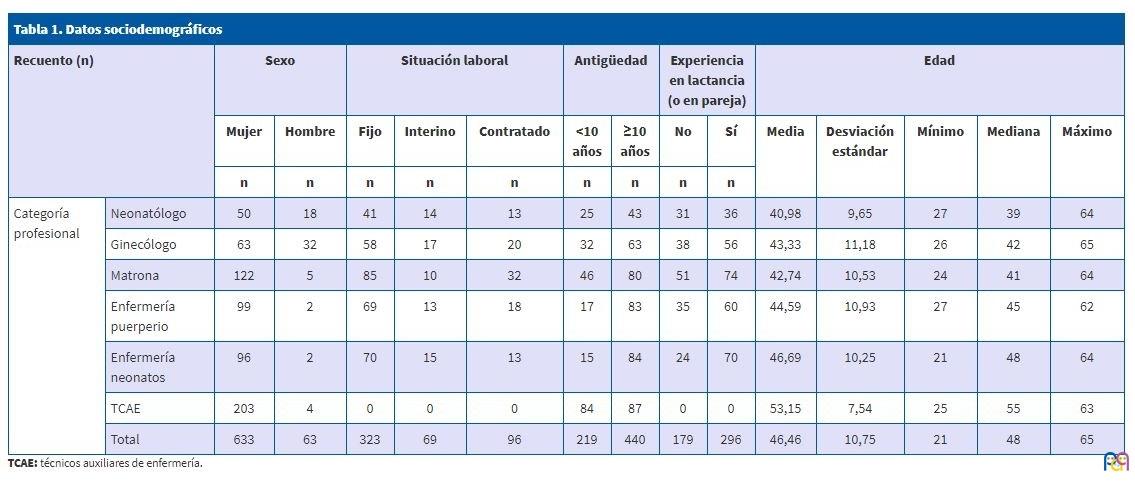
Algunos encuestados no contestan a algunas preguntas del perfil sociodemográfico (Tabla 1).
| Tabla 1. Datos sociodemográficos | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Recuento (n) | Sexo | Situación laboral | Antigüedad | Experiencia en lactancia (o en pareja) | Edad | ||||||||||
| Mujer | Hombre | Fijo | Interino | Contratado | <10 años | ≥10 años | No | Sí | Media | Desviación estándar | Mínimo | Mediana | Máximo | ||
| n | n | n | n | n | n | n | n | n | |||||||
| Categoría profesional | Neonatólogo | 50 | 18 | 41 | 14 | 13 | 25 | 43 | 31 | 36 | 40,98 | 9,65 | 27 | 39 | 64 |
| Ginecólogo | 63 | 32 | 58 | 17 | 20 | 32 | 63 | 38 | 56 | 43,33 | 11,18 | 26 | 42 | 65 | |
| Matrona | 122 | 5 | 85 | 10 | 32 | 46 | 80 | 51 | 74 | 42,74 | 10,53 | 24 | 41 | 64 | |
| Enfermería puerperio | 99 | 2 | 69 | 13 | 18 | 17 | 83 | 35 | 60 | 44,59 | 10,93 | 27 | 45 | 62 | |
| Enfermería neonatos | 96 | 2 | 70 | 15 | 13 | 15 | 84 | 24 | 70 | 46,69 | 10,25 | 21 | 48 | 64 | |
| TCAE | 203 | 4 | 0 | 0 | 0 | 84 | 87 | 0 | 0 | 53,15 | 7,54 | 25 | 55 | 63 | |
| Total | 633 | 63 | 323 | 69 | 96 | 219 | 440 | 179 | 296 | 46,46 | 10,75 | 21 | 48 | 65 | |
Tasa de respuesta
Se recibieron en total 724 cuestionarios (el 61,0% del total de profesionales de Castilla y León). Al cuestionario 1 respondieron 512 profesionales (60,5% de participación) y al cuestionario 2 contestaron 212 (62,2% de participación) (Tabla 2).
| Tabla 2. Diferencias en la participación según categoría profesional médico/enfermería | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Recuento | Sexo | Tipo de contrato | Antigüedad | Experiencia en lactancia (o en pareja) | Edad | |||||||||||
| Mujer | Hombre | Valor de p, médicos, enfermería | Fijo | Interino | Contratado | Valor de p, médicos, enfermería | Menos de 10 años | 10 o más años | Valor de p, médicos, enfermería | No | Sí | Valor de p, médicos, enfermería | Media | Valor de p, médicos, enfermería |
||
| n | n | n | n | n | n | n | n | n | ||||||||
| Profesión | Médicos | 113 | 50 | p = 0,0000 | 99 | 31 | 33 | p = 0,0866 | 57 | 106 | p = 0,227 | 69 | 92 | p = 0,110 | 42,36 | p = 0,045 |
| Enfermería | 317 | 9 | 224 | 38 | 63 | 78 | 247 | 110 | 204 | 44,46 | ||||||
| TCAE | 203 | 4 | 0 | 0 | 0 | 84 | 87 | 0 | 0 | 53,15 | ||||||
| Total | 633 | 63 | 323 | 69 | 96 | 219 | 440 | 179 | 296 | 46,46 | ||||||

Se observan diferencias estadísticamente significativas según el sexo y la edad, son más jóvenes los médicos y es predominante el sexo femenino.
No se observan diferencias estadísticamente significativas según tipo de contrato, experiencia, y antigüedad.
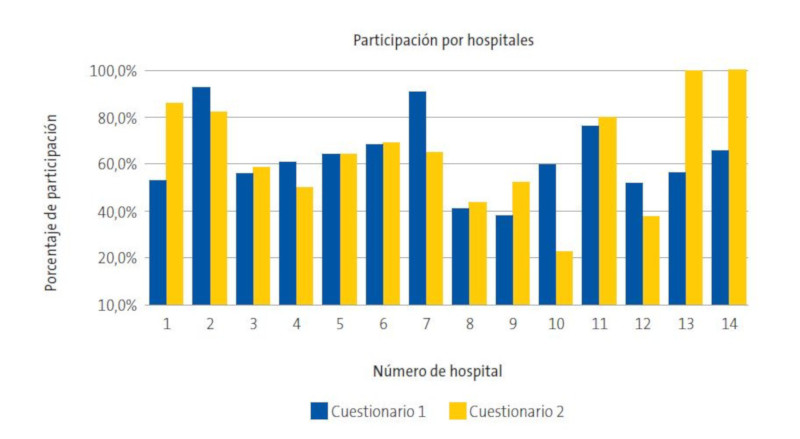
Variabilidad de la participación de los hospitales públicos de Castilla y León
Se observa una variabilidad significativa (p <0,05) en la tasa de respuesta entre los distintos hospitales. En la mayoría de los hospitales (9/14), responden a la encuesta entre el 50 y 70% del personal del área materno-infantil (Fig. 1).
| Figura 1. Participación por hospitales |
|---|
 |

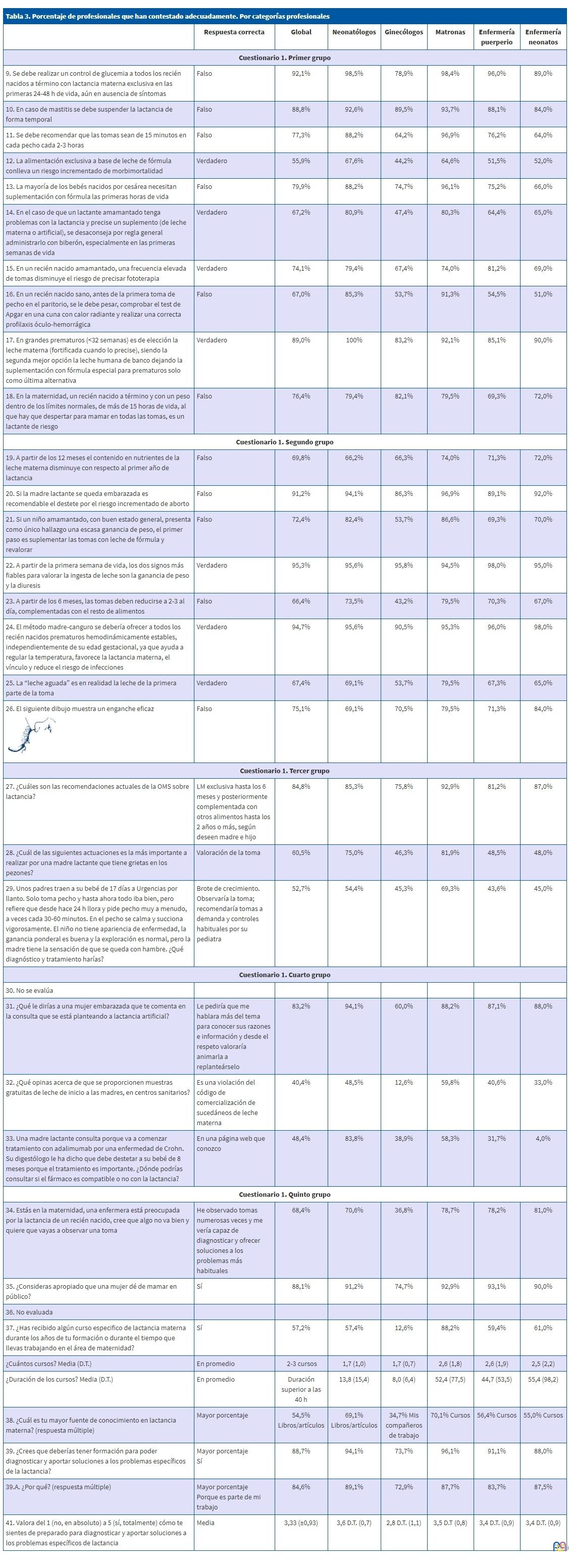
Análisis de las preguntas de los cuestionarios
Se incluyen en las Tablas 3 y 4.
| Tabla 3. Porcentaje de profesionales que han contestado adecuadamente. Por categorías profesionales | |||||||
|---|---|---|---|---|---|---|---|
| Respuesta correcta | Global | Neonatólogos | Ginecólogos | Matronas | Enfermería puerperio | Enfermería neonatos | |
| Cuestionario 1. Primer grupo | |||||||
| 9. Se debe realizar un control de glucemia a todos los recién nacidos a término con lactancia materna exclusiva en las primeras 24-48 h de vida, aún en ausencia de síntomas | Falso | 92,1% | 98,5% | 78,9% | 98,4% | 96,0% | 89,0% |
| 10. En caso de mastitis se debe suspender la lactancia de forma temporal | Falso | 88,8% | 92,6% | 89,5% | 93,7% | 88,1% | 84,0% |
| 11. Se debe recomendar que las tomas sean de 15 minutos en cada pecho cada 2-3 horas | Falso | 77,3% | 88,2% | 64,2% | 96,9% | 76,2% | 64,0% |
| 12. La alimentación exclusiva a base de leche de fórmula conlleva un riesgo incrementado de morbimortalidad | Verdadero | 55,9% | 67,6% | 44,2% | 64,6% | 51,5% | 52,0% |
| 13. La mayoría de los bebés nacidos por cesárea necesitan suplementación con fórmula las primeras horas de vida | Falso | 79,9% | 88,2% | 74,7% | 96,1% | 75,2% | 66,0% |
| 14. En el caso de que un lactante amamantado tenga problemas con la lactancia y precise un suplemento (de leche materna o artificial), se desaconseja por regla general administrarlo con biberón, especialmente en las primeras semanas de vida | Verdadero | 67,2% | 80,9% | 47,4% | 80,3% | 64,4% | 65,0% |
| 15. En un recién nacido amamantado, una frecuencia elevada de tomas disminuye el riesgo de precisar fototerapia | Verdadero | 74,1% | 79,4% | 67,4% | 74,0% | 81,2% | 69,0% |
| 16. En un recién nacido sano, antes de la primera toma de pecho en el paritorio, se le debe pesar, comprobar el test de Apgar en una cuna con calor radiante y realizar una correcta profilaxis óculo-hemorrágica | Falso | 67,0% | 85,3% | 53,7% | 91,3% | 54,5% | 51,0% |
| 17. En grandes prematuros (<32 semanas) es de elección la leche materna (fortificada cuando lo precise), siendo la segunda mejor opción la leche humana de banco dejando la suplementación con fórmula especial para prematuros solo como última alternativa | Verdadero | 89,0% | 100% | 83,2% | 92,1% | 85,1% | 90,0% |
| 18. En la maternidad, un recién nacido a término y con un peso dentro de los límites normales, de más de 15 horas de vida, al que hay que despertar para mamar en todas las tomas, es un lactante de riesgo | Falso | 76,4% | 79,4% | 82,1% | 79,5% | 69,3% | 72,0% |
| Cuestionario 1. Segundo grupo | |||||||
| 19. A partir de los 12 meses el contenido en nutrientes de la leche materna disminuye con respecto al primer año de lactancia | Falso | 69,8% | 66,2% | 66,3% | 74,0% | 71,3% | 72,0% |
| 20. Si la madre lactante se queda embarazada es recomendable el destete por el riesgo incrementado de aborto | Falso | 91,2% | 94,1% | 86,3% | 96,9% | 89,1% | 92,0% |
| 21. Si un niño amamantado, con buen estado general, presenta como único hallazgo una escasa ganancia de peso, el primer paso es suplementar las tomas con leche de fórmula y revalorar | Falso | 72,4% | 82,4% | 53,7% | 86,6% | 69,3% | 70,0% |
| 22. A partir de la primera semana de vida, los dos signos más fiables para valorar la ingesta de leche son la ganancia de peso y la diuresis | Verdadero | 95,3% | 95,6% | 95,8% | 94,5% | 98,0% | 95,0% |
| 23. A partir de los 6 meses, las tomas deben reducirse a 2-3 al día, complementadas con el resto de alimentos | Falso | 66,4% | 73,5% | 43,2% | 79,5% | 70,3% | 67,0% |
| 24. El método madre-canguro se debería ofrecer a todos los recién nacidos prematuros hemodinámicamente estables, independientemente de su edad gestacional, ya que ayuda a regular la temperatura, favorece la lactancia materna, el vínculo y reduce el riesgo de infecciones | Verdadero | 94,7% | 95,6% | 90,5% | 95,3% | 96,0% | 98,0% |
| 25. La “leche aguada” es en realidad la leche de la primera parte de la toma | Verdadero | 67,4% | 69,1% | 53,7% | 79,5% | 67,3% | 65,0% |
| 26. El siguiente dibujo muestra un enganche eficaz
|
Falso | 75,1% | 69,1% | 70,5% | 79,5% | 71,3% | 84,0% |
| Cuestionario 1. Tercer grupo | |||||||
| 27. ¿Cuáles son las recomendaciones actuales de la OMS sobre lactancia? | LM exclusiva hasta los 6 meses y posteriormente complementada con otros alimentos hasta los 2 años o más, según deseen madre e hijo | 84,8% | 85,3% | 75,8% | 92,9% | 81,2% | 87,0% |
| 28. ¿Cuál de las siguientes actuaciones es la más importante a realizar por una madre lactante que tiene grietas en los pezones? | Valoración de la toma | 60,5% | 75,0% | 46,3% | 81,9% | 48,5% | 48,0% |
| 29. Unos padres traen a su bebé de 17 días a Urgencias por llanto. Solo toma pecho y hasta ahora todo iba bien, pero refiere que desde hace 24 h llora y pide pecho muy a menudo, a veces cada 30-60 minutos. En el pecho se calma y succiona vigorosamente. El niño no tiene apariencia de enfermedad, la ganancia ponderal es buena y la exploración es normal, pero la madre tiene la sensación de que se queda con hambre. ¿Qué diagnóstico y tratamiento harías? | Brote de crecimiento. Observaría la toma; recomendaría tomas a demanda y controles habituales por su pediatra | 52,7% | 54,4% | 45,3% | 69,3% | 43,6% | 45,0% |
| Cuestionario 1. Cuarto grupo | |||||||
| 30. No se evalúa | |||||||
| 31. ¿Qué le dirías a una mujer embarazada que te comenta en la consulta que se está planteando a lactancia artificial? | Le pediría que me hablara más del tema para conocer sus razones e información y desde el respeto valoraría animarla a replanteárselo | 83,2% | 94,1% | 60,0% | 88,2% | 87,1% | 88,0% |
| 32. ¿Qué opinas acerca de que se proporcionen muestras gratuitas de leche de inicio a las madres, en centros sanitarios? | Es una violación del código de comercialización de sucedáneos de leche materna | 40,4% | 48,5% | 12,6% | 59,8% | 40,6% | 33,0% |
| 33. Una madre lactante consulta porque va a comenzar tratamiento con adalimumab por una enfermedad de Crohn. Su digestólogo le ha dicho que debe destetar a su bebé de 8 meses porque el tratamiento es importante. ¿Dónde podrías consultar si el fármaco es compatible o no con la lactancia? | En una página web que conozco | 48,4% | 83,8% | 38,9% | 58,3% | 31,7% | 4,0% |
| Cuestionario 1. Quinto grupo | |||||||
| 34. Estás en la maternidad, una enfermera está preocupada por la lactancia de un recién nacido, cree que algo no va bien y quiere que vayas a observar una toma | He observado tomas numerosas veces y me vería capaz de diagnosticar y ofrecer soluciones a los problemas más habituales | 68,4% | 70,6% | 36,8% | 78,7% | 78,2% | 81,0% |
| 35. ¿Consideras apropiado que una mujer dé de mamar en público? | Sí | 88,1% | 91,2% | 74,7% | 92,9% | 93,1% | 90,0% |
| 36. No evaluada | |||||||
| 37. ¿Has recibido algún curso especifico de lactancia materna durante los años de tu formación o durante el tiempo que llevas trabajando en el área de maternidad? | Sí | 57,2% | 57,4% | 12,6% | 88,2% | 59,4% | 61,0% |
| ¿Cuántos cursos? Media (D.T.) | En promedio | 2-3 cursos | 1,7 (1,0) | 1,7 (0,7) | 2,6 (1,8) | 2,6 (1,9) | 2,5 (2,2) |
| ¿Duración de los cursos? Media (D.T.) | En promedio | Duración superior a las 40 h | 13,8 (15,4) | 8,0 (6,4) | 52,4 (77,5) | 44,7 (53,5) | 55,4 (98,2) |
| 38. ¿Cuál es tu mayor fuente de conocimiento en lactancia materna? (respuesta múltiple) | Mayor porcentaje | 54,5% Libros/artículos | 69,1% Libros/artículos | 34,7% Mis compañeros de trabajo | 70,1% Cursos | 56,4% Cursos | 55,0% Cursos |
| 39. ¿Crees que deberías tener formación para poder diagnosticar y aportar soluciones a los problemas específicos de la lactancia? | Mayor porcentaje Sí |
88,7% | 94,1% | 73,7% | 96,1% | 91,1% | 88,0% |
| 39.A. ¿Por qué? (respuesta múltiple) | Mayor porcentaje Porque es parte de mi trabajo |
84,6% | 89,1% | 72,9% | 87,7% | 83,7% | 87,5% |
| 41. Valora del 1 (no, en absoluto) a 5 (sí, totalmente) cómo te sientes de preparado para diagnosticar y aportar soluciones a los problemas específicos de lactancia | Media | 3,33 (±0,93) | 3,6 D.T. (0,7) | 2,8 D.T. (1,1) | 3,5 D.T (0,8) | 3,4 D.T. (0,9) | 3,4 D.T. (0,9) |

| Tabla 4. Porcentaje de profesionales (TCAE) que han contestado cada pregunta | |||
|---|---|---|---|
| Verdadero | Falso | No contesta | |
| 5. La leche materna es el alimento de mejor calidad para el recién nacido, siempre que la madre no esté desnutrida | 83,5% | 15,6% | 0,9% |
| 6. Durante el segundo año de vida, la leche materna es de muy baja calidad | 16,0% | 80,2% | 3,9% |
| 7. Si la madre está tomando cualquier medicación, se debe suspender la lactancia | 5,7% | 90,1% | 4,2% |
| 8. Cuando el recién nacido amantado llora de hambre, se le debe complementar con biberón | 52,8% | 43,4% | 3,8% |
| 16. La primera toma debe de ser inmediatamente después del parto | 90,6% | 7,5% | 1,9% |
| 17. El suero glucosado es necesario para evitar la hipoglucemia del recién nacido | 16,5% | 81,6% | 1,9% |
| 18. Dando el pecho con más frecuencia, disminuye el riesgo de ictericia | 59,0% | 38,7% | 2,4% |
| 19. Muchos niños necesitan biberón los primeros días hasta que a la madre le sube la leche | 54,2% | 43,9% | 1,9% |
| 20. Hay que dar el pecho cada vez que el bebé lo pida | 96,2% | 2,8% | 0,9% |
| 21. Los chupetes interfieren y dificultan la lactancia materna | 60,4% | 37,3% | 2,4% |
| 22. El recién nacido debe permanecer día y noche con la madre | 81,6% | 17,0% | 1,4% |
| 23. La primera toma debe ser al menos 3 horas después del parto | 26,9% | 71,2% | 1,9% |
| 24. En caso de mastitis hay que suprimir la lactancia | 24,1% | 73,6% | 2,4% |
| 25. Hay que lavar el pecho antes y después de cada toma | 53,8% | 44,8% | 1,4% |
| 26. No es recomendable dar el pecho si la madre es portadora de hepatitis B | 38,2% | 54,2% | 7,5% |
| 27. Si el niño tiene diarrea hay que suspender unos días la lactancia | 6,1% | 92,5% | 1,4% |
| 28. En gemelos no se debe recomendar la lactancia materna | 3,8% | 95,8% | 0,5% |

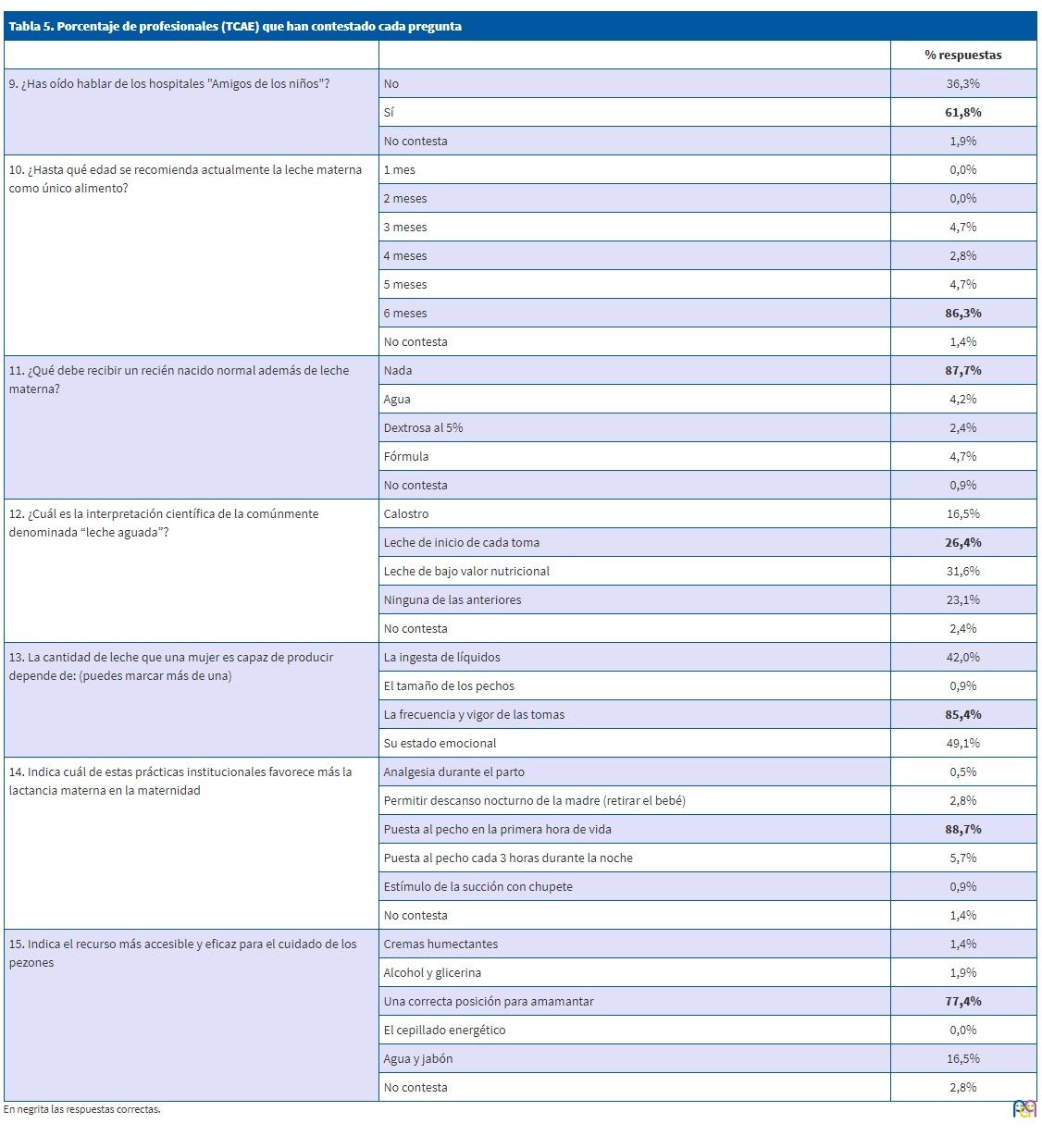
Nivel de conocimientos según la categoría profesional
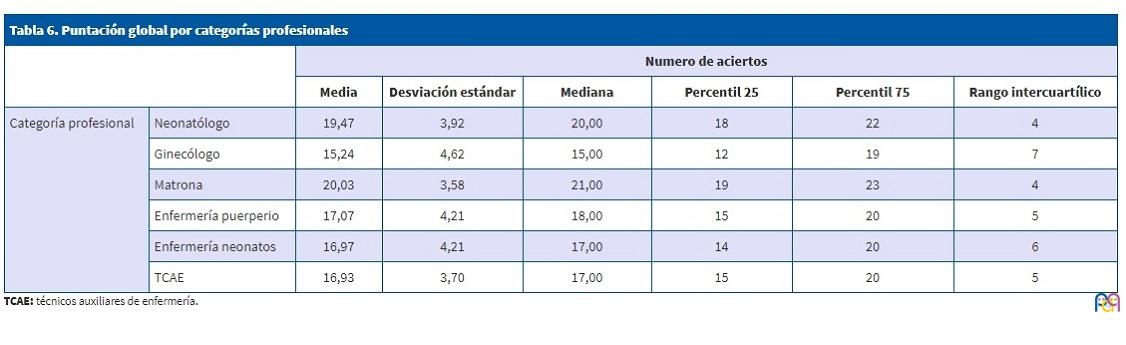
Para analizar el nivel de conocimientos se ha tomado como referencia el 70% de aciertos (16,8 puntos) como el puntaje recomendable. Se han seguido para este estándar las recomendaciones de los autores de las encuestas12, que categorizaron las puntuaciones como: <50% muy insuficiente, 50-70% insuficiente, 70-85% bien, >85% excelente. También el estudio de Canadá consideró el nivel de 70% como aceptable18. Los neonatólogos, matronas, profesionales de enfermería de la planta de puerperio y los TCAE presentan niveles aceptables. Los ginecólogos no superan el nivel mínimo recomendable (Tablas 5 y 6,Figura 2).
| Tabla 5. Porcentaje de profesionales (TCAE) que han contestado cada pregunta | ||
|---|---|---|
| % respuestas | ||
| 9. ¿Has oído hablar de los hospitales "Amigos de los niños"? | No | 36,3% |
| Sí | 61,8% | |
| No contesta | 1,9% | |
| 10. ¿Hasta qué edad se recomienda actualmente la leche materna como único alimento? | 1 mes | 0,0% |
| 2 meses | 0,0% | |
| 3 meses | 4,7% | |
| 4 meses | 2,8% | |
| 5 meses | 4,7% | |
| 6 meses | 86,3% | |
| No contesta | 1,4% | |
| 11. ¿Qué debe recibir un recién nacido normal además de leche materna?
|
Nada | 87,7% |
| Agua | 4,2% | |
| Dextrosa al 5% | 2,4% | |
| Fórmula | 4,7% | |
| No contesta | 0,9% | |
| 12. ¿Cuál es la interpretación científica de la comúnmente denominada “leche aguada”? | Calostro | 16,5% |
| Leche de inicio de cada toma | 26,4% | |
| Leche de bajo valor nutricional | 31,6% | |
| Ninguna de las anteriores | 23,1% | |
| No contesta | 2,4% | |
| 13. La cantidad de leche que una mujer es capaz de producir depende de: (puedes marcar más de una) | La ingesta de líquidos | 42,0% |
| El tamaño de los pechos | 0,9% | |
| La frecuencia y vigor de las tomas | 85,4% | |
| Su estado emocional | 49,1% | |
| 14. Indica cuál de estas prácticas institucionales favorece más la lactancia materna en la maternidad | Analgesia durante el parto | 0,5% |
| Permitir descanso nocturno de la madre (retirar el bebé) | 2,8% | |
| Puesta al pecho en la primera hora de vida | 88,7% | |
| Puesta al pecho cada 3 horas durante la noche | 5,7% | |
| Estímulo de la succión con chupete | 0,9% | |
| No contesta | 1,4% | |
| 15. Indica el recurso más accesible y eficaz para el cuidado de los pezones | Cremas humectantes | 1,4% |
| Alcohol y glicerina | 1,9% | |
| Una correcta posición para amamantar | 77,4% | |
| El cepillado energético | 0,0% | |
| Agua y jabón | 16,5% | |
| No contesta | 2,8% | |
| Tabla 6. Puntación global por categorías profesionales | |||||||
|---|---|---|---|---|---|---|---|
| Numero de aciertos | |||||||
| Media | Desviación estándar | Mediana | Percentil 25 | Percentil 75 | Rango intercuartílico | ||
| Categoría profesional | Neonatólogo | 19,47 | 3,92 | 20,00 | 18 | 22 | 4 |
| Ginecólogo | 15,24 | 4,62 | 15,00 | 12 | 19 | 7 | |
| Matrona | 20,03 | 3,58 | 21,00 | 19 | 23 | 4 | |
| Enfermería puerperio | 17,07 | 4,21 | 18,00 | 15 | 20 | 5 | |
| Enfermería neonatos | 16,97 | 4,21 | 17,00 | 14 | 20 | 6 | |
| TCAE | 16,93 | 3,70 | 17,00 | 15 | 20 | 5 | |
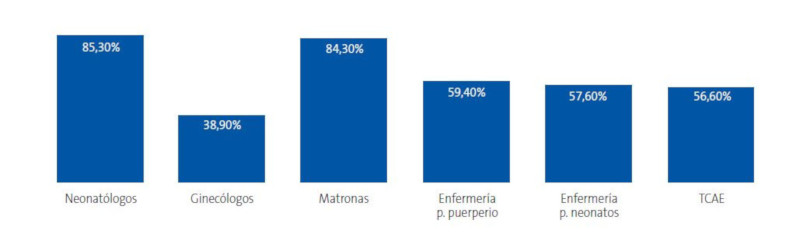
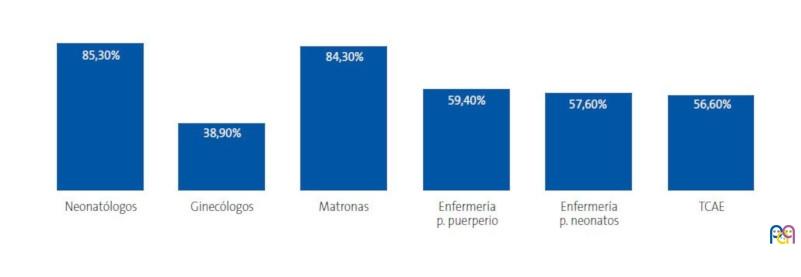
| Figura 2. Porcentaje de profesionales que superan el 70% de aciertos |
|---|
 |
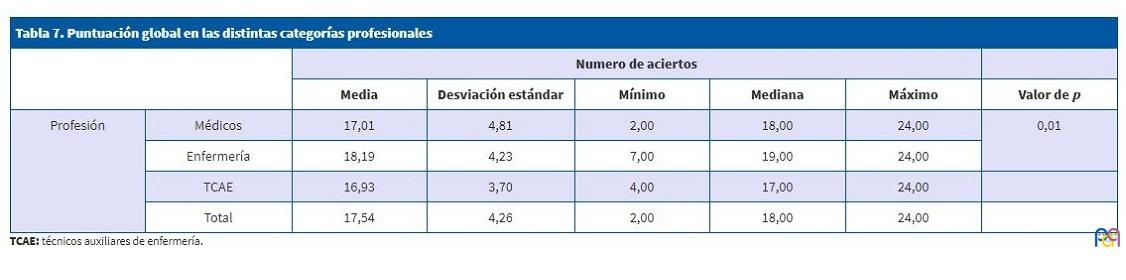
Se observa en la Tabla 7 una diferencia significativa del nivel de aciertos entre profesionales médicos y de enfermería (p = 0,01).
| Tabla 7. Puntuación global en las distintas categorías profesionales | |||||||
|---|---|---|---|---|---|---|---|
| Numero de aciertos | |||||||
| Media | Desviación estándar | Mínimo | Mediana | Máximo | Valor de p | ||
| Profesión | Médicos | 17,01 | 4,81 | 2,00 | 18,00 | 24,00 | 0,01 |
| Enfermería | 18,19 | 4,23 | 7,00 | 19,00 | 24,00 | ||
| TCAE | 16,93 | 3,70 | 4,00 | 17,00 | 24,00 | ||
| Total | 17,54 | 4,26 | 2,00 | 18,00 | 24,00 | ||
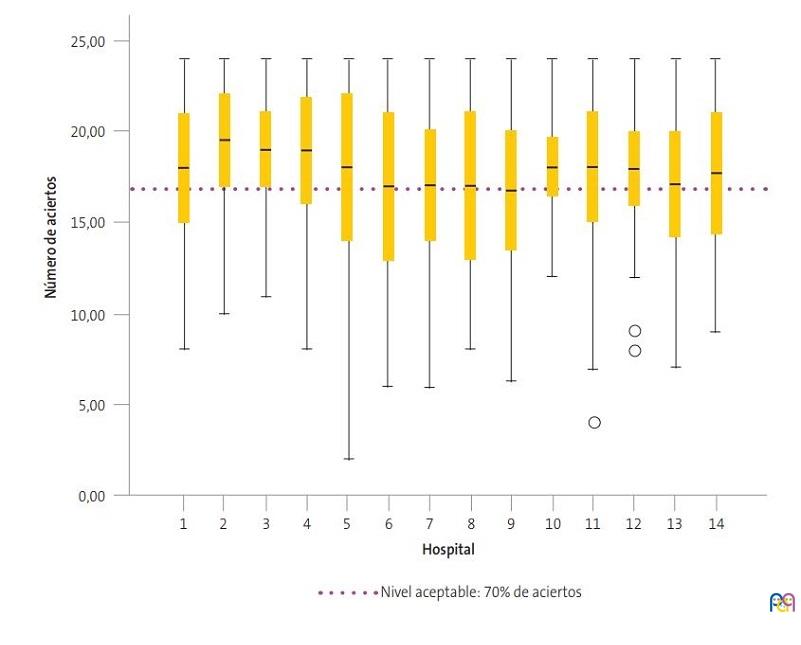
Hay diferencias en general en el número de aciertos entre los hospitales (p = 0,033). Hay diferencias en el número de aciertos (del hospital 7 con el 2, del hospital 9 con el 2, etc.) (Figura 3).
| Figura 3. Número de aciertos en cada hospital |
|---|
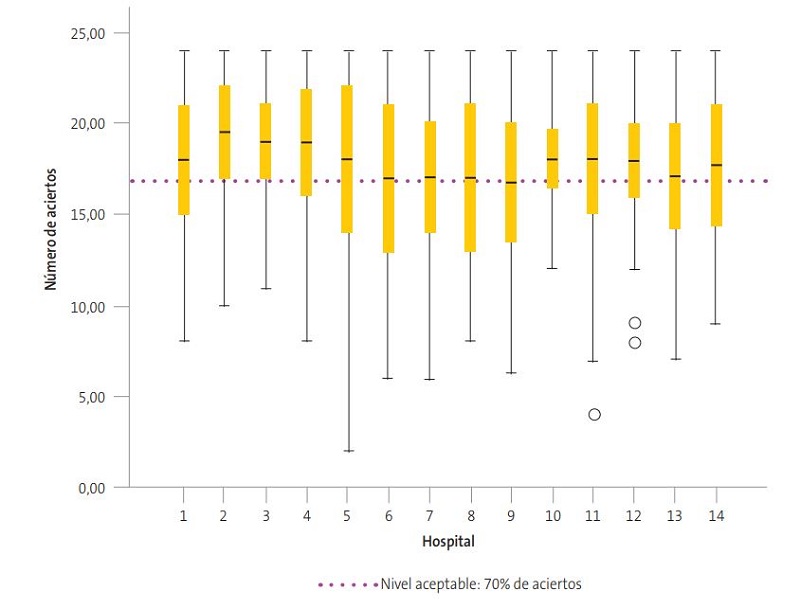 |
DISCUSIÓN
La posibilidad de realizar la encuesta de conocimientos en lactancia materna de nuestro estudio en la totalidad de los profesionales del área materno-infantil de hospitales públicos de SACYL, partiendo de la base de datos real de estos servicios, la alta participación (60,9%), y el método de realización de la encuesta (en papel y dirigida en reuniones de equipo) hace que los resultados nos ofrezcan una situación muy fidedigna de los conocimientos en este tema.
No hemos encontrado estudios en España de estas características, en las que se documenten en varios estamentos profesionales, y en la totalidad de los profesionales del área materno-infantil de los hospitales públicos de una comunidad autónoma. En la revisión bibliográfica sí se documentan estudios dirigidos a distintos perfiles sanitarios: residentes de Pediatría10, pediatras y residentes de Pediatría12, médicos de familia de Tenerife15, y profesionales sanitarios de un área de salud de la Comunidad Valenciana16, sin aparecer en la bibliografía estudios comparativos entre los distintas categorías.
En el estado de Sonora (México)17, con un sistema de salud muy distinto al nuestro, han realizado un estudio similar utilizando un cuestionario basado en el de Temboury10 que incluía también a residentes de Pediatría y Ginecología. El método de aplicación del cuestionario fue realizado por estudiantes de nutrición, y se hizo de manera aleatoria a médicos y enfermería (327 encuestas). Dicho estudio concluía también en el déficit de conocimientos esenciales entre los profesionales, aunque observaba que los residentes de Pediatría obtenían mejores resultados, que se podían justificar por la formación previa en cursos y reuniones académicas.
En el estudio llevado a cabo en Canadá para evaluar los conocimientos, creencias y actitudes de pediatras, médicos de familia y residentes del último año de Pediatría y familia18, el nivel de puntuación de los médicos fue inferior al 70% (que definieron como aceptable) mientras que los residentes de Pediatría superaron el 70%.
Para obtener mejores resultados en lactancia materna e implementar soluciones a los problemas planteados por las madres es preciso conocer la situación previa del nivel de conocimientos. Persiguiendo estos mismos objetivos, y después de iniciado nuestro estudio, IHAN España en el año 2015, publica un documento “Monitorización de la formación en atención a la lactancia materna mediante encuestas a profesionales”13, en el que propone una herramienta de monitorización para valorar el grado de formación y las necesidades formativas y recomienda realizar encuestas a profesionales con periodicidad anual proponiendo unos tamaños de muestra para los distintos hospitales según el número de camas. Esta propuesta de la IHAN aún no ha obtenido resultados publicados.
Los resultados obtenidos nos hacen reflexionar sobre distintos aspectos. Las matronas y los neonatólogos en más de un 80% tienen el nivel “bueno” de conocimientos, sin embargo, solo un 39% de los ginecólogos presentan este nivel, y el resto de las categorías profesionales no lo poseen en más de un 40% de los casos. Por tanto, en las dos terceras partes de las categorías profesionales que están en contacto con las madres que inician la lactancia, un porcentaje considerable de profesionales no poseen los conocimientos definidos como “buenos”, en nuestro estudio.
Se observa en nuestro trabajo la falta de formación en rutinas y habilidades hospitalarias en los TCAE, profesionales que realizan funciones importantes en esta área. Estos no dan la suficiente importancia a la introducción de biberones (p8 y p19), las dificultades de la lactancia y el uso de chupetes (p21), la importancia que tiene el contacto piel con piel precoz y la primera toma (p23) y algo tan básico como puede ser el recomendar erróneamente el lavado del pecho antes y después de la toma p25 (44,8%). Casi la mitad de estos profesionales no llegan al nivel definido como bueno.
Todos estos datos nos llevan a reflexionar en la necesidad de incidir en formación en lactancia materna en todas las categorías profesionales y especialmente en los ginecólogos, cuya cercanía en la asistencia de las madres en el inicio de la lactancia es fundamental. El nivel de conocimiento en esta categoría es el menor de todas.
En las preguntas 19, 21, 23, y 25 del cuestionario 1 es posible afirmar que, a pesar de las campañas realizadas, aún no se valora suficientemente la importancia de la lactancia materna exclusiva durante seis meses y su mantenimiento hasta los dos años o más, complementada con el resto de los alimentos. Tampoco en la necesidad de realizar un acompañamiento a las madres lactantes en las dificultades que se pudieran presentar a lo largo de este periodo.
Los resultados obtenidos nos confirman el frecuente desconocimiento del código de comercialización de sucedáneos y de las herramientas que podrían ayudar a la compatibilidad de la lactancia con la clínica diaria, como podría ser el conocimiento de la página web e-lactancia.org u otras aplicaciones electrónicas, y que influyen directamente en la prevalencia de la lactancia materna.
Todos los profesionales de las áreas materno-infantiles de los hospitales de Castilla y León son conscientes de su falta de formación específica en lactancia materna, y casi el 90% la considera importante para poder diagnosticar y aportar soluciones a los problemas específicos de la lactancia, que considera parte de su trabajo (p39).
Al revisar los currículos formativos publicados del grado de Medicina en la Universidad de Valladolid19,20 y distintas especialidades, nos encontramos con que los estudiantes de medicina solo se forman en fisiología de la lactancia y los ginecólogos en su periodo formativo MIR no poseen ningún apartado en el que se especifique la necesidad de formación en lactancia materna fisiológica, aunque sí en la patología mamaria puerperal21. Los TCAE, en su currículo formativo publicado, no dedican ningún apartado a lactancia materna22.
Entre los objetivos del aprendizaje que reciben los pediatras23, profesionales de enfermería24-27, matronas28 y EIR de Pediatría29 aparece la formación en lactancia materna, aunque con distinto nivel de profundidad. Los resultados obtenidos en este trabajo se relacionan claramente con el nivel de formación previo de los profesionales y se orientan a la necesidad de mejorar los conocimientos, habilidades y competencias de las distintas categorías sanitarias. Habría que incidir en la formación en lactancia especialmente en perfiles profesionales que no reciben la formación adecuada, como ginecólogos y TCAE.
El nivel de conocimientos del personal del área materno-infantil de Castilla y León en el año 2015, según se documenta en nuestro trabajo, presenta debilidades en aspectos trascendentales para el adecuado manejo de la lactancia: se ignoran conocimientos y habilidades básicos que condicionan la misma, se realizan recomendaciones que no favorecen la lactancia (retrasar la primera toma, horarios rígidos, el uso de chupetes y biberones), y cuando se presentan dificultades se limitan a retirar la lactancia, sin tener en cuenta los deseos de la madre y el bienestar del recién nacido. Al definir 16,8 puntos (el 70% de los aciertos) como la puntuación “bien”, observamos que son los neonatólogos, matronas, y profesionales de enfermería de la planta de puerperio/neonatos y TCAE los que llegarían a este nivel. Los ginecólogos tendrían una puntuación “insuficiente”.
La lactancia materna no es un tema de profesionales de enfermería, ni de aquellos a los “que les guste el tema”, sino que, por la importancia que tiene en la promoción de la salud pública, corresponde a los políticos y gestores sanitarios, que son los que han de organizar políticas educativas adecuadas en los distintos currículos profesionales y diseñar programas de formación conjuntos en las áreas materno-infantiles de todos los centros hospitalarios, que incluyan a todas las categorías profesionales implicadas en el cuidado de la mujer y recién nacido (neonatólogos, ginecólogos, matronas, profesionales de enfermería y TCAE). En definitiva, mejorar las tasas de prevalencia en lactancia materna en nuestra Comunidad precisa invertir en formación específica en lactancia materna.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
ASCALEMA: Asociación Castellanoleonesa de Matronas · ECola: Encuesta sobre Conocimientos en Lactancia Materna · EMALYP: Estrategia Mundial para la Alimentación del Lactante y del Niño Pequeño · IC 95: intervalo de confianza del 95% · IHAN: Iniciativa para la Humanización al Nacimiento y la Lactancia · OMS: Organización Mundial de la Salud · SACYL: Gerencia Regional de Salud de la Comunidad Autónoma de Castilla y León · TCAE: técnicos auxiliares de enfermería · Unicef: Fondo de las Naciones Unidas para la Infancia.
AGRADECIMIENTOS
A todas las personas que con su trabajo y su apoyo han contribuido a la realización de este proyecto.
BIBLIOGRAFÍA
- Aguayo Maldonado J, Cañedo Argüelles CA, Arena Ansótegui J, Canduela Martínez V, Flores Antón B, Gómez Papí A, et al. IHAN Calidad en la asistencia profesional al nacimiento y la lactancia. Informes, estudios e investigación 2011. Madrid: Ministerio de Sanidad, Política Social e Igualdad; 2011.
- Estévez-González M, Martell Cebrián D, Medina Santana R, García Villanueva E, Saavedra Santana P. Factores relacionados con el abandono de la lactancia materna. Anal Esp Pediatr. 2002;56:144-51.
- Barriuso Lapresa LM, Sánchez-Valverde Visus F, Romero Ibarra C, Vitoria Comerzana JC. Epidemiología de la lactancia materna en el centro-norte de España. An Esp Pediatr. 1999;50:237-243.
- Aguayo Maldonado J, Pasadas del Amo S, Ramírez Troyano A, Rello Yubero C, Martínez Rodríguez MT, Bonal Pitz P. La lactancia materna en Andalucía: resultados del estudio de prevalencia de la lactancia materna en Andalucía y los factores asociados a su duración en el primer año de vida. Sevilla: Junta de Andalucía, Consejería de Salud; 2005.
- Hernández-Aguilar M, Muñoz-Guillén A, Lasarte-Velillas JJ, García-Vera C, Díaz-Marijuan C, Martín-Calama J. La lactancia materna en la Comunidad Valenciana: Análisis multivariante de una encuesta a 6400 lactantes. Rev Pediatr Aten Primaria. 2004;6:19-37.
- Gartner LM, Morton J, Lawrence RA, Naylor AJ, O’Hare D, Schanler RJ, et al. Breastfeeding and the use of human milk. Pediatrics. 2005;115:496-506.
- Merewood A, Mehta SD, Chamberlain LB, Philipp BL, Bauchner H. Breastfeeding rates in US baby-friendly hospitals: results of a national survey. Pediatrics. 2005;116:628-34.
- Zakarija-Grković I, Burmaz T. Effectiveness of the UNICEF/WHO 20-hour course in improving health professionals’ knowledge, practices, and attitudes to breastfeeding: a before/after study of 5 maternity facilities in Croatia. Croat Med J.2010;51:396-405.
- Cattaneo A, Buzzetti R. Effect on rates of breast feeding of training for the baby friendly hospital initiative. BMJ. 2001;323:1358-62.
- Temboury Molina MC. Informe sobre el conocimiento de los residentes de Pediatría en el manejo de la lactancia materna. An Pediatr (Barc). 2003;58:263-7.
- Hernández Aguilar MT, Aguayo Maldonado J. La lactancia materna. Cómo promover y apoyar la lactancia materna en la práctica pediátrica. Recomendaciones del Comité de Lactancia de la AEP. An Pediatr (Barc). 2005;63:340-56.
- Gómez Fernández-Vegue M, Menéndez Orenga M. Validación de un cuestionario sobre conocimientos y habilidades en lactancia materna. An Pediatr (Barc). 2015;83:387-96.
- Monitorización de la formación en atención a la lactancia mediante encuestas a profesionales. En: UNICEF - Buscar con Google. Disponible en https://bit.ly/2Roca9k
- Sacristán Martín AM, Lozano Alonso JE, Gil Costa M, Vega Alonso AT, Red Centinela Sanitaria de Castilla y León. Situación actual y factores que condicionan la lactancia materna en Castilla y León. Rev Pediatr Aten Primaria. 2011;13:33-46.
- Monge Zamorano, M, Garrido Martín, M. Conocimientos de los residentes de medicina de familia de Tenerife sobre la lactancia materna. BSCP Can Ped. 2007;31:7-1.
- Palomares Jimeno MJ, Labordena Barceló C, Sanantonio Valdearcos F, Agramunt Soler G, Nácher Fernández A, Palau Fuster G. Opiniones y conocimientos básicos sobre lactancia materna en el personal sanitario. Rev Pediatr Aten Primaria. 2001;3:393-402.
- Valenzuela H, Gabriel J, Trujillo EA, Lares AAO, Sánchez GAM, Hernández GÁ. Saberes de médicos y enfermeras de un hospital, acerca de las bondades de la lactancia. Rev Mex Pediatr. 2014;81:56-60.
- Pound CM, Williams K, Grenon R, Aglipay M, Plint AC. Breastfeeding knowledge, confidence, beliefs, and attitudes of Canadian physicians. J Hum Lact. 2014;30:298-309.
- Guía docente de la asignatura Obstetricia y Ginecología. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/478/46294/1/Documento.pdf
- Guía docente de la asignatura Pediatría. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/478/46306/1/Documento.pdf
- Ministerio de Sanidad y Política Social. Orden SAS/1350/2009, de 6 de mayo, por la que se aprueba y publica el programa formativo de la especialidad de Obstetricia y Ginecología. En: Boletín Oficial del Estado [en línea] [consultado el 24/05/2019]. Disponible en www.boe.es/buscar/doc.php?id=BOE-A-2009-8882
- Ministerio de Educación y Ciencia. Real Decreto 558/1995, de 7 de abril, por el que se establece el currículo del ciclo formativo de grado medio correspondiente al título de Técnico en Cuidados Auxiliares de Enfermería. En: Boletín Oficial del Estado [en línea] [consultado el 24/05/2019]. Disponible en www.boe.es/buscar/doc.php?id=BOE-A-1995-13592
- Ministerio de Sanidad y Consumo. ORDEN SCO/3148/2006, de 20 de septiembre, por la que se aprueba y publica el programa formativo de la especialidad de Pediatría y sus Áreas Específicas. En: Boletín Oficial del Estado [en línea] [consultado el 24/05/2019]. Disponible en https://boe.vlex.es/vid/formativo-Pediatría-especificas-23787972
- Proyecto docente de Enfermería en la Infancia y Adolescencia. Campus Soria. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/476/46227/1/Documento.pdf
- Proyecto docente de Enfermería en la Infancia y Adolescencia. Campus Valladolid. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/475/46182/1/Documento.pdf
- Proyecto docente de la asignatura Enfermería en salud sexual y reproductiva. Campus de Soria. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/476/46229/1/Documento.pdf
- Proyecto docente de la asignatura Enfermería en salud sexual y reproductiva. Campus Valladolid. En: Universidad de Valladolid [en línea] [consultado el 24/05/2019]. Disponible en https://alojamientos.uva.es/guia_docente/uploads/2017/475/46184/1/Documento.pdf
- Ministerio de Sanidad y Política Social. Orden SAS/1349/2009, de 6 de mayo, por la que se aprueba y publica el programa formativo de la especialidad de Enfermería Obstétrico-Ginecológica (Matrona)… En: Boletín Oficial del Estado [en línea] [consultado el 24/05/2019]. Disponible en www.boe.es/diario_boe/txt.php?id=BOE-A-2009-8881
- Ministerio de Sanidad y Política Social. Orden SAS/1730/2010, de 17 de junio, por la que se aprueba y publica el programa formativo de la especialidad de Enfermería Pediátrica. En: Boletín Oficial del Estado [en línea] [consultado el 24/05/2019]. Disponible en www.boe.es/diario_boe/txt.php?id=BOE-A-2010-10365