

Presentación clínica y tratamiento de los niños hospitalizados por gripe durante cinco temporadas
Marciano Sánchez Baylea, Enrique Villalobos Pintob, M.ª Araceli Manso Cuevasc, Laura Palomino Pérezc, Ester de Juan Bitriac
aPediatra. Fundación para la Investigación, Estudio y Desarrollo de la Salud Pública. Madrid. España.
bSección de Pediatría Hospitalaria. Hospital Infantil Universitario Niño Jesús. Madrid. España.
cMIR-Pediatría. Hospital Infantil Universitario Niño Jesús. Madrid. España.
Correspondencia: E Villalobos. Correo electrónico: evillalobospinto@yahoo.es
Cómo citar este artículo: Sánchez Bayle M, Villalobos Pinto E, Manso Cuevas MA, Palomino Pérez L, de Juan Bitria E. Presentación clínica y tratamiento de los niños hospitalizados por gripe durante cinco temporadas. Rev Pediatr Aten Primaria. 2018;20:e61-e67.
Publicado en Internet: 10-09-2018 - Número de visitas: 26009
Resumen
Objetivo: estudiar las características clínicas y demográficas, así como el uso de oseltamivir, de los niños hospitalizados por gripe en un hospital pediátrico terciario.
Pacientes y métodos: estudio descriptivo observacional de niños entre 0 y 18 años ingresados en las temporadas de diciembre a mayo de 2012 a 2017 con diagnóstico confirmado microbiológicamente de gripe.
Resultados: se han estudiado 166 pacientes. El porcentaje de ingresos sobre el total de ingresados en las mismas fechas osciló entre el 2,03 y el 9,69%. El mayor número de ingresos fueron en la penúltima temporada de estudio (p <0,0001). Los niños diagnosticados de gripe A presentaron una edad menor que los que lo fueron de gripe B (2,45 frente a 3,88 años, p <0,0001), no encontrándose diferencias significativas en cuanto al sexo, los días de estancia media, la necesidad de antibioterapia o de broncodilatadores. Recibieron tratamiento con oseltamivir un total de 96 niños (57,83%), 75 de ellos en la temporada 2015-2016. No se encontraron diferencias en las características de los niños que lo recibieron frente a los que no. La estancia media global fue 0,89 días mayor en aquellos niños que recibieron el antiviral, diferencia casi significativa en el total de la muestra (p = 0,052), durante la temporada 2015-2016 la duración fue 1,8 días mayor (p = 0,039). No se encontraron diferencias significativas en cuanto al porcentaje de pacientes con neumonía ni de los que precisaron ingreso en la Unidad de Cuidados Intensivos Pediátricos entre los tratados respecto a los no tratados.
Conclusiones: el porcentaje de niños ingresados por gripe es importante, habiéndose incrementado en la última temporada. Los niños diagnosticados con gripe A tienen una edad significativamente menor que los que presentaron gripe B. En nuestro caso no se encontraron ventajas en el tratamiento con oseltamivir.
Palabras clave
● Oseltamivir ● Virus de la influenza A ● Virus de la influenza BINTRODUCCIÓN
La infección por virus influenza o gripe está ampliamente distribuida en nuestro entorno en la población pediátrica, habitualmente con una sintomatología banal, aunque también incluye un amplio rango de complicaciones de gravedad variable en niños sanos e inmunocompetentes. La gripe se distribuye de forma epidémica mayoritariamente en los meses de invierno, de tal manera que supone una importante carga asistencial que es manejada en su mayoría de forma ambulatoria, a pesar de ello constituye, junto al virus respiratorio sincitial (VRS), la principal causa de ingreso durante esta época.
En los últimos años se está constatando un aumento en el uso de los inhibidores de la neuraminidasa para el tratamiento de la gripe, siendo alguna de sus indicaciones el manejo de niños hospitalizados, niños con patología crónica de base, inmunodeprimidos o pacientes con cuadros graves o complicados.
En la actualidad hay escasas evidencias acerca del efecto clínico del oseltamivir y pocos estudios disponibles realizados en la edad pediátrica. Además, existen resultados contradictorios en los diferentes estudios. Esto puede estar influido por los modestos resultados clínicos de estos antivirales y la falta de criterios unificados de diagnóstico, ingreso y tratamiento de la gripe.
Por todo esto y debido al importante impacto de esta patología, tanto su repercusión económica como social, el objetivo de este estudio es revisar las características de los niños hospitalizados por gripe en los últimos años y el rendimiento del tratamiento con oseltamivir en estos pacientes.
MATERIAL Y MÉTODOS
Se trata de un estudio descriptivo retrospectivo mediante la revisión de todos los casos ingresados con el diagnóstico de infección por virus influenza en el Hospital Infantil Universitario Niño Jesús (Madrid, España) en las temporadas de diciembre a mayo de 2012-2013 a 2016-2017.
El estudio microbiológico consistió en la detección de los antígenos del virus influenza A y B en el aspirado nasofaríngeo a través de test rápidos antigénicos y, en algunos casos, la posterior determinación por reacción en cadena de la polimerasa (PCR). La técnica de detección de antígenos víricos permite un diagnóstico en minutos u horas con una sensibilidad del 53% y una especificidad del 94%. Esto te permite una toma rápida de decisiones. La RT-PCR permite el diagnóstico en 1-8 horas, con una sensibilidad y especificidad cercanas al 99%1.
Las variables recogidas de estos pacientes fueron: edad, sexo, serotipo de virus influenza, motivo de ingreso, realización de pruebas complementarias (como analítica sanguínea o radiografía de tórax), complicaciones asociadas (como neumonía u otitis media aguda), ingreso en la Unidad de Cuidados Intensivos Pediátricos (UCIP), tiempo de estancia y necesidad de instaurar tratamiento antibiótico o con broncodilatadores.
Se ha realizado un análisis estadístico descriptivo y comparativo con el programa SPSS® versión 15.0 para estudiar diferencias entre subgrupos. La comparación de las variables cualitativas se llevó a cabo con las pruebas de χ2. La comparación de las variables cuantitativas se realizó con la prueba U de Mann-Whitney, al no tener una distribución paramétrica (determinado por el test de Kolmogorov-Smirnov). Se consideraron significativos valores de p <0,05.
RESULTADOS
Durante el periodo de estudio un total de 166 pacientes fueron hospitalizados debido a una infección por virus influenza confirmada virológicamente mediante test rápido o PCR. La mayor parte de estos (119/149) estaban causados por virus influenza A (71,68%), 46 casos se debían a virus influenza B (27,71%) y un caso a la coinfección por ambos serotipos.
El número de niños hospitalizados por virus influenza varió entre las distintas temporadas: en la temporada 2012/2013 hubo un total de 23 ingresos, suponiendo el 2,69% del total de ingresos en los meses estudiados de esa temporada y el 4,43% de los ingresos respiratorios; en la temporada 2013/2014 hubo 20, que supuso el 2,71% del total de ingresos y el 3,85% de los respiratorios; en la temporada 2014/2015 hubo 17, el 2,03% del total y el 2,43% de los respiratorios; en la temporada 2015/2016 hubo 89, que ascendió al 9,69% del total de ingresos y al 11,22% de los respiratorios, lo que además supone el 53,61% del total de ingresos por gripe de nuestro estudio, siendo significativamente mayor que en el resto de temporadas (p <0,0001). Finalmente, en la temporada 2016-17 ingresaron 17 niños (el 3,71% de los respiratorios y el 2,83% del total de los ingresos).
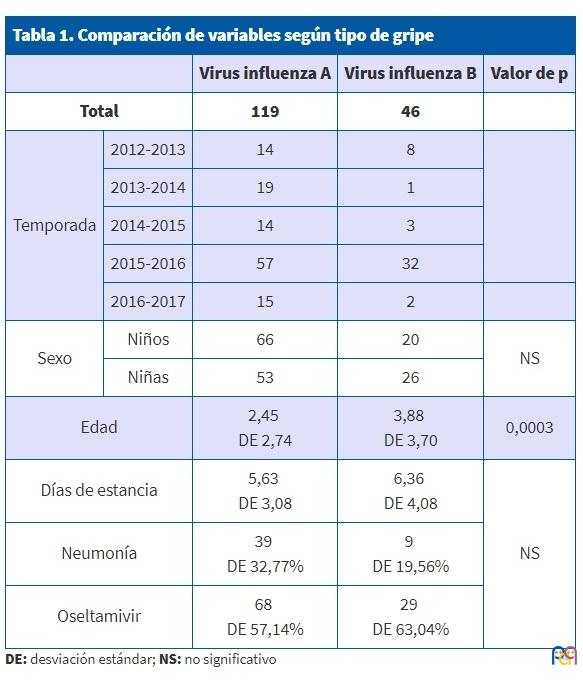
Los niños infectados con virus influenza serotipo A presentan una edad media inferior que aquellos con virus influenza B (2,45 años frente a 3,88 años, p = 0,003). No se han encontrado diferencias significativas entre los distintos serotipos de virus influenza en cuanto al sexo, los días de estancia media, la necesidad de antibioterapia o de broncodilatadores (Tabla 1). En la comparación de estas variables hemos excluido al paciente con la coinfección por ambos serotipos de virus influenza.
| Tabla 1. Comparación de variables según tipo de gripe | ||||
|---|---|---|---|---|
| Virus influenza A | Virus influenza B | Valor de p | ||
| Total | 119 | 46 | ||
| Temporada | 2012-2013 | 14 | 8 | |
| 2013-2014 | 19 | 1 | ||
| 2014-2015 | 14 | 3 | ||
| 2015-2016 | 57 | 32 | ||
| 2016-2017 | 15 | 2 | ||
| Sexo | Niños | 66 | 20 | NS |
| Niñas | 53 | 26 | ||
| Edad | 2,45 DE 2,74 |
3,88 DE 3,70 |
0,0003 | |
| Días de estancia | 5,63 DE 3,08 |
6,36 DE 4,08 |
NS | |
| Neumonía | 39 DE 32,77% |
9 DE 19,56% |
||
| Oseltamivir | 68 DE 57,14% |
29 DE 63,04% |
||
Los casos se correspondieron a 86 niños (51,8%) y 79 niñas, sin encontrar diferencias según el sexo entre los distintos serotipos de virus influenza. La edad media de los niños hospitalizados fue de 2,86 años (desviación estándar [DE]: 3,05). Hubo 59 niños menores de 12 meses, que se corresponde al 35,54% del total.
Se realizó radiografía de tórax durante el ingreso a 90 niños (54,54%), que fue diagnóstica de neumonía en 48 de ellos (53,33%), correspondiendo al 28,91% del total de pacientes con gripe. A 130 niños se les realizó una analítica sanguínea con hemograma (78,31%) y de ellos 82 recibieron antibiótico (63,07%). Un total de 91 niños recibieron antibiótico en algún momento (55,15%), 48 de ellos por diagnóstico de neumonía y cinco por otitis. En 62 casos (37,34 %) se asociaron broncodilatadores. Un total de 11 casos precisaron ingreso en la UCIP (6,62%), siendo más frecuente en menores de 12 meses (11,86% en menores de 12 meses frente a 3,84% en mayores de esa edad, diferencia casi significativa: p = 0,054).
Los pacientes diagnosticados de neumonía tuvieron una estancia media algo mayor que el resto (0,7 días más, p = 0,016) al igual que aquellos que ingresaron en la UCIP (cuatro días más, p <0,0001), sin diferencias significativas en cuanto a la edad.
Durante la estancia hospitalaria recibieron tratamiento con oseltamivir un total de 96 casos (57,83%). La edad media es menor en el grupo de niños que recibieron oseltamivir, sin diferencias significativas. En las temporadas 2012-2013 y 2013-2014 ningún niño fue tratado con oseltamivir, mientras que lo recibieron diez de los 17 casos de la temporada 2014-2015 (58,8%), 75 de los 89 casos de la temporada 2015-2016 (84,3%) y 12 de los 17 en 2016-17 (70,58%). No se han encontrado diferencias en la presencia de neumonía entre los niños que recibieron oseltamivir frente a los que no (32,29% frente al 24,63%, respectivamente), tampoco en los ingresos en UCIP (8,33%, frente a 4,34%). En 79 de los 96 casos que recibieron oseltamivir (82,29%) se realizó analítica sanguínea, en 53 (55,20%) radiografía, diagnosticándose neumonía en 31 de ellos (32,29%). Sin embargo, hasta 61 de los 96 pacientes tratados con oseltamivir recibieron antibiótico (63,54%). Los principales datos están recogidos en la Tabla 2.
| Tabla 2. Comparación de las variables estudiadas en función de si recibieron tratamiento con oseltamivir | |||||
|---|---|---|---|---|---|
| Oseltamivir | Valor de p | ||||
| Sí | No | ||||
| Total | 96 | 69 | |||
| Temporada | 2012-2013 | 23 | 0 0% |
23 100% |
|
| 2013-2014 | 20 | 0 0% |
20 100% |
||
| 2014-2015 | 17 | 10 59% |
7 41% |
||
| 2015-2016 | 89 | 75 84% |
14 16% |
||
| 2016-2017 | 17 | 12 70,58% |
5 29,41% |
||
| Sexo | Niños | 86 | 44 51,11% |
42 | NS |
| Niñas | 79 | 46 58,22% |
33 | ||
| Edad | 2,62 DE 3,01 |
3,2 DE 3,19 |
NS | ||
| Días de distancia | 6,19 DE 3,57 |
5,30 DE 3,07 |
0,052 | ||
| Neumonía | 48 | 31 32,29% |
17 24,63% |
NS | |
| Ingreso en UCIP | 11 | 7 7,29% |
3 4,34% |
NS | |
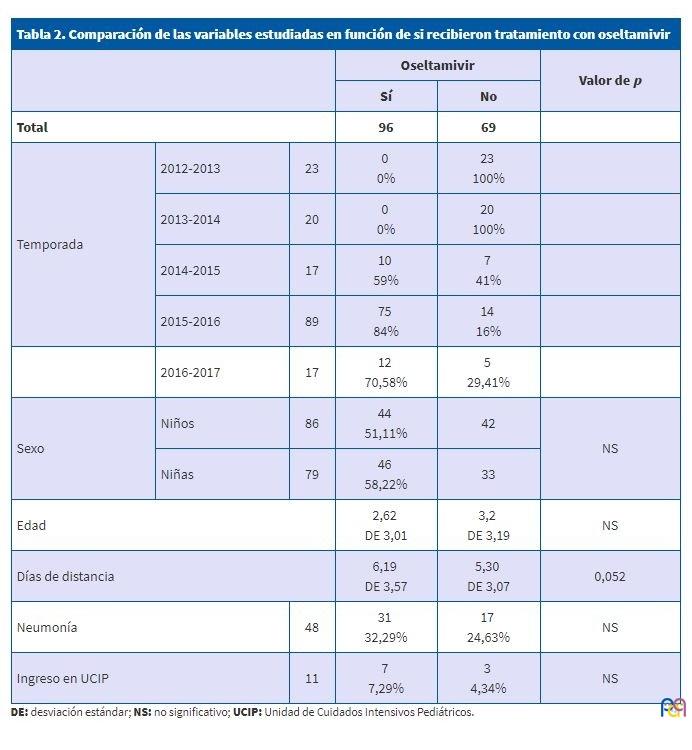
La estancia media fue ligeramente mayor en el total de niños tratados con oseltamivir que en aquellos que no lo recibieron (0,89 días), con una diferencia casi significativa (p = 0,052). Tampoco se ven diferencias en cuanto a la edad media de niños que fueron tratados con oseltamivir. La duración media del ingreso en los niños tratados con oseltamivir durante la temporada 2015/2016 fue 1,8 días mayor que la de aquellos que no lo recibieron (p = 0,039).
DISCUSIÓN
La percepción de la gripe, tanto de la población general como de los pediatras, es que es una enfermedad banal en niños, sin repercusiones importantes. Esto se explica en parte por el escaso número de estudios pediátricos sobre la clínica y las complicaciones de esta entidad. Sin embargo, se sabe que las infecciones respiratorias causan una gran morbilidad en niños, que es mayor en los de menor edad. Y la gripe no solo implica la infección de las vías respiratorias, sino que asocia muchas de las complicaciones respiratorias más comunes en la infancia, como puede ser la otitis media aguda o la neumonía.
En nuestro centro hemos estudiado un total de 166 pacientes hospitalizados con diagnóstico de gripe entre las temporadas de diciembre a mayo y de 2012-2013 a 2016-2017. La mayoría de los ingresos se dan en los meses fríos, aunque pueden ocurrir casos esporádicos fuera de onda epidémica2. Por este motivo nuestro periodo de estudio se ha reducido a las temporadas de epidemia. Durante el tiempo de estudio se observa un claro predominio de la infección por virus influenza A sobre el B, viéndose un aumento progresivo de este último a lo largo de estos años. Esto coincide con los estudios epidemiológicos de la gripe3. La temporada 2015-2016 abarca el mayor número de ingresos del estudio, además supone un porcentaje significativamente mayor del número de ingresos hospitalarios de esa temporada: el 9,69% del total y el 11,22% de los respiratorios, cifra que se corresponde con otras revisiones4,5. Uno de los motivos del aumento de ingresos puede ser la mayor detección por el avance de las técnicas diagnósticas y por la realización de estas a todo paciente con patología respiratoria que ingresa, según las recomendaciones de los Centers for Disease Control and Prevention (CDC)6. También se ha estudiado que en esta época epidémica ha habido un aumento de la duración global respecto años anteriores, pero con un menor pico de casos, manteniéndose de este modo la tasa de incidencia acumulada de ingresos por gripe. La tasa de complicaciones y la estancia media es mayor en los pacientes infectados por virus influenza A, aunque las diferencias no han sido significativas.
Tal y como muestran otros estudios, el sexo no influye en la probabilidad de ingreso por gripe, mientras que sí lo hace la edad. En nuestro estudio hemos observado un mayor número de ingresos en escolares (2-10 años), ya que es un grupo importante de transmisión del virus influenza por la rápida expansión vírica en colegios y guarderías. Los niños presentan las tasas máximas de ataque, hasta un 40% en preescolares y un 30% en niños de edad escolar, con extensión secundaria a los padres y hermanos. Los hallazgos obtenidos en nuestra muestra se corresponden a los datos de otras publicaciones4,5,7.
En niños menores de tres años, en especial en menores de 12 meses, el aumento del número de ingresos también puede deberse a la coinfección con el VRS, lo que no se ha observado en nuestro estudio4,5. Se ha descrito que en este grupo de edad son más frecuentes las complicaciones, motivo por el cual son objeto de tratamiento con los nuevos antivirales. En nuestra muestra un 35,34% del total de ingresos eran pacientes menores de 12 meses, presentando un porcentaje de ingreso en UCIP significativamente mayor que en mayores de esta edad (p = 0,03).
Las complicaciones respiratorias de la infección por virus influenza son relativamente frecuentes y son las que determinan en muchos casos el ingreso o su prolongación. En la literatura médica se describen por orden de frecuencia: bronquitis aguda (hasta en un 30% de población total con gripe), neumonía y exacerbación del asma. En nuestra serie la neumonía se presentó como complicación en un 28,91% de los casos de gripe, que se corresponde a un porcentaje similar en otras revisiones previas7-9. Esto ha supuesto un aumento significativo de la estancia media hospitalaria en 0,7 días en los niños que asociaron neumonía a la infección por gripe (p = 0,016). Otras complicaciones han sido la otitis media aguda (3,01% en nuestra muestra, frente al 10 al 30% en otros estudios, dependiendo de las series) y sinusitis aguda (18% de la población pediátrica global con infección por virus influenza).
El uso de antivirales para la gripe está en discusión. Durante la pandemia del 2009 hubo un aumento generalizado en el uso de ese medicamento, aunque posteriormente se ha ido reduciendo. Todavía no están claros los mecanismos de acción del fármaco, así como de su disponibilidad, por este motivo es difícil determinar el grupo de pacientes que más se beneficiaría de este10. La literatura médica describe que es más eficaz en las primeras horas, cuando la carga viral todavía no está en su pico más alto. Presenta mayor beneficio cuanto antes se administre (<48 horas). Una vez que han pasado más de 48 horas del comienzo de la clínica, puede encontrarse beneficio en pacientes hospitalizados, cuadros graves y complicados o pacientes con mayor riesgo de complicaciones.
En Pediatría, el antivírico de elección es el oseltamivir, inhibidor de la neuraminidasa. En la temporada 2015/2016 en nuestro centro se han seguido las recomendaciones de los CDC descritas en 2011, cuyas indicaciones para el tratamiento con oseltamivir incluyen: pacientes inmunodeprimidos, en tratamiento crónico con ácido acetil salicílico, neumópatas, cardiópatas, con patología crónica grave de base y aquellos que requieran ingreso6. Aun así, cada caso se ha de evaluar. El porcentaje de tratamiento fue nulo en las dos primeras temporadas del estudio y ha ascendido al 85% en esta última. El principal motivo de este importante incremento ha sido la implementación de las nuevas guías diagnóstico-terapéuticas seguidas durante la última temporada.
En otros estudios se ha referido que el oseltamivir reduce duración de la fiebre y otros síntomas en 24 horas, así como el riesgo de complicaciones1,11,12. Otros estudios difieren con esto, obteniendo resultados significativos en la no disminución del riesgo de otitis media aguda y sinusitis, tanto en niños como en adultos10. En algunos estudios destacan que la reducción del tiempo de estancia en el hospital se ve disminuida únicamente en pacientes asmáticos y no en el resto10. Como ya se ha comentado, el efecto es mayor cuanto más precozmente se administre, de modo que en algunos estudios este efecto solo se ha estudiado diagnosticando y administrando el fármaco en las primeras 48 horas13. Por otro lado, se han señalado numerosos efectos adversos del fármaco (vómitos, cefaleas, mareos, efectos renales adversos, etc.) y que no disminuye las complicaciones de la gripe y se ha propugnado su no utilización salvo en situaciones excepcionales3.
El diagnóstico de gripe, en la mayoría de los casos que acuden a Urgencias, no siempre se realiza en las primeras 48 horas (ya que previamente se intenta el manejo ambulatorio o en domicilio con antitérmicos) y el tiempo en que se realiza test rápido de gripe en pacientes también es variable. Esto dificulta el tratamiento precoz de la infección, y podría reducir la potencial eficacia de los antivirales. En nuestra serie se trataron con oseltamivir el 57,83% del total de los casos. Se observó una duración mayor de la estancia media de hospitalización (0,89 días) en los niños tratados con oseltamivir y esta fue mayor en la temporada 2015/2016, con una cifra de hasta 1,8 días más respecto a los no tratados; 29 de los niños tratados con oseltamivir tuvieron neumonía y 16 no, aunque algunos de ellos ya la presentaban antes del ingreso. De los 11 casos que requirieron ingreso en la UCIP, ocho recibían tratamiento con oseltamivir y tres no. Como se ha comentado previamente, estos resultados parecen discrepar de algunos de los estudios publicados, en los que el oseltamivir disminuye el tiempo de estancia media y las complicaciones.
En nuestro estudio no se ha registrado el momento de inicio del oseltamivir, excepto en la última temporada (2016-2017) en la que solo cinco de los 12 casos tratados (41,66%) lo fueron antes de las 48 horas del inicio de los síntomas. Se deben realizar estudios posteriores que evalúen la eficacia del oseltamivir en pacientes con diagnóstico diferido (>48 horas de sintomatología) pero que cumplen otras condiciones, como precisar ingreso o presentar patología crónica de base. Esto es interesante de cara a evitar el uso de un fármaco caro, no financiado y de dudosa eficacia.
Al ser un estudio descriptivo y solo de pacientes ingresados, no hemos podido comparar la eficacia del fármaco en aquellos de características parecidas que no precisaran ingreso. Además, el hecho de ingresar implica que sea una población más frágil y susceptible de complicaciones o que ya las presentaran. El tamaño muestral es otra de las principales limitaciones. Se precisan por lo tanto estudios posteriores más amplios.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
CDC: Centers for Disease Control and Prevention ● DE: desviación estándar ● PCR: (reacción en cadena de la polimerasa) ● UCIP: Unidad de Cuidados Intensivos Pediátricos ● VRS: virus respiratorio sincitial.
BIBLIOGRAFÍA
- Lafond KE, Nair H, Rasooly MH, Valente F, Booy R, et al. Global role and burden of influenza in pediatric respiratory hospitalizations, 1982-2012: a systematic analysis. PLoS Med. 2016;13:e1001977.
- Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev. 2014;(4):CD008965.
- Cruz-Cañete M, Moreno-Pérez D, Jurado-Ortiz A, García-Martín FJ, López-Siles J. Olalla-Martín L. El virus de la gripe en Pediatría. Un motivo de hospitalización. Enferm Infecc Microbiol Clin. 2007;25:177-83.
- Weil-Olivier C. Gripe estacional infantil. FMC Pediatr. 2015;50:1-19.
- Dawood FS, Chaves SS, Pérez A. Complications and associated bacterial coinfections among children hospitalized with seasonal or pandemic influenza, United States, 2003-2010. J Infect Dis. 2014;209:686-94.
- Arístegui Fernández J. Gripe en Pediatría. Pediatr Integral. 2015;19:694-701.
- Ros Aranal I, Navarra Vicente B. Características clínicas y actuaciones en los niños ingresados por gripe en cuatro periodos epidémicos gripales (2002-2006). An Pediatr (Barc). 2008;68:24-9.
- Arostegi Kareaga N, Montes M, Pérez-Yarza EG, Sardón O, Vicente D, Cilla G. Características clínicas de los niños hospitalizados por infección por virus Influenza. An Pediatr (Barc). 2005;62:5-12.
- Vilà de Muga M, Torre Monmany N, Asensio Carretero S, Travería Casanovas FJ, Martínez Mejías A, Coll Sibina MT, et al. Características clínicas de la gripe A H1N1 2009: estudio multicéntrico. An Pediatr (Barc). 2011;75:6-12.
- Buñuel Álvarez JC, González de Dios J. Evidencias de la pandemia por virus influenza A (H1N1). An Pediatr (Barc). 2009;71:379-82.
- Heinonen S, Silvennoinen H, Lehtinen P, Vainionpää R, Vahlberg T, Ziegler T, et al. Early oseltamivir treatment of influenza in children 1-3 years of age: a randomized controlled trial. Clin Infect Dis. 2010;51:887-94.
- Informe de Vigilancia de la Gripe en España. Temporada 2015-2016 (desde la semana 40/2015 hasta la semana 20/2016). Sistema de Vigilancia de la Gripe en España. En: Instituto de Salud Carlos III [en línea] [consultado el 25/07/2018]. Disponible en www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/fd-enfermedades/gripe.shtml.
- Centers for Disease Control and Prevention. Antiviral agents for the treatment and chemoprophylaxis of influenza recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. 2011;60:7-9.
- Rude D. Myths in emergency medicine: still prescribing osetalmivir? Emerg Med News. 2017;39:41.