


Clinical presentation and treatment of children hospitalised due to influenza from the 2012 to the 2016 season
Marciano Sánchez Baylea, Enrique Villalobos Pintob, M.ª Araceli Manso Cuevasc, Laura Palomino Pérezc, Ester de Juan Bitriac
aPediatra. Fundación para la Investigación, Estudio y Desarrollo de la Salud Pública. Madrid. España.
bSección de Pediatría Hospitalaria. Hospital Infantil Universitario Niño Jesús. Madrid. España.
cMIR-Pediatría. Hospital Infantil Universitario Niño Jesús. Madrid. España.
Correspondence: E Villalobos. E-mail: evillalobospinto@yahoo.es
Reference of this article: Sánchez Bayle M, Villalobos Pinto E, Manso Cuevas MA, Palomino Pérez L, de Juan Bitria E. Clinical presentation and treatment of children hospitalised due to influenza from the 2012 to the 2016 season. Rev Pediatr Aten Primaria. 2018;20:e61-e67.
Published in Internet: 10-09-2018 - Visits: 18621
Abstract
Objective: to analyse the demographic and clinical characteristics and the use of oseltamivir in children admitted with influenza to a tertiary care children’s hospital.
Patients and methods: we conducted a descriptive observational study of all patients aged 0 to 18 years admitted in every December-to-May epidemic season between 2012 and 2016 with a microbiological diagnosis of influenza.
Results: we reviewed the cases of 166 patients. The percentage of influenza admissions out of the total admissions during the seasons under study between 2.03% and 9.69%. The highest number of admissions occurred in the second to last season under study (p < .0001). Children with infection by influenza A were younger compared to those with influenza B (2.45 vs. 3.88 years, p < .0001), and we found no significant differences between serotypes in the sex distribution, mean length of stay or need for antibiotherapy or bronchodilators. A total of 96 children (57.83%) received oseltamivir, 75 of them in the 2015-2016 season. We found no differences in the characteristics of children treated with oseltamivir compared to those that were not. The mean length of stay was 0.89 days overall and was greater in children treated with the antiviral drug, with p-values that neared the threshold for significance in the entire sample (p = .052); the length of stay was 1.8 days longer in the 2015-2016 season (p = .039). We did not find significant differences between patients that received oseltamivir and patients that did not in the percentage that developed pneumonia or the percentage that required admission to the paediatric intensive care unit.
Conclusions: the percentage of children admitted with influenza virus was substantial and increased in the last season. Children with an influenza A diagnosis were younger compared to children with influenza B. Our study did not find advantages in the use of oseltamivir.
Keywords
● Influenza A virus ● Influenza B virus ● OseltamivirINTRODUCTION
Infection by influenza viruses (influenza, or the flu) is common in the Spanish paediatric population and usually has a mild presentation, although it is also associated with a wide range of complications of variable severity in previously healthy and immunocompetent children. Most cases of the flu cluster in outbreaks during the winter months, producing a significant health care burden that is managed mainly at the outpatient level, although the flu, along with infection by respiratory syncytial virus (RSV), is the main reason for hospital admission this time of year.
In recent years, there has been an increase in the use of neuraminidase inhibitors for treatment of influenza. Patients in which their use is indicated include hospitalised patients, children with underlying chronic disease, immunosuppressed patients or patients with severe or complicated disease.
At present, there is little evidence on the clinical effect of oseltamivir, and few of the studies have been conducted in the paediatric population. Furthermore, the findings of published studies are inconsistent. This may be partly due to the modest clinical effects of these antivirals and a lack of homogeneous criteria for the diagnosis, treatment and need for hospital admission in influenza.
Due to all of the above and the significant impact of this disease, both social and economic, our aim was to review the characteristics of children hospitalised due to influenza in recent years and the effectiveness of treatment with oseltamivir in these patients.
MATERIALS AND METHODS
We conducted a retrospective study in which we reviewed all the cases of hospitalization due to influenza virus infection in the Hospital Infantil Universitario Niño Jesús (Madrid, Spain) during the flu seasons (December-May) from 2012-2013 to 2016-2017.
The microbiological evaluation consisted in rapid antigen tests for detection of influenza virus A and B antigens in nasopharyngeal aspirate samples and, in some cases, subsequent testing by polymerase chain reaction (PCR). The rapid viral antigen detection method can produce a diagnosis within minutes or hours with a sensitivity of 53% and a specificity of 94%, which in turn allows rapid clinical decision making. Reverse transcription PCR allows diagnosis within 1 to 8 hours, with a sensitivity and specificity near 99%.1
We collected data for the following variables in these patients: age, sex, influenza virus serotype, reason for admission, additional diagnostic tests (such as blood tests or chest X-ray), associated complications (such as pneumonia or acute otitis media), admission to paediatric intensive care unit (PICU), length of stay and need for treatment with antibiotics or bronchodilators.
We performed a descriptive and comparative statistical analysis with the software SPSS® version 15.0 to analyse differences between groups. We compared qualitative variables by means of the χ2 test, and quantitative variables by means of the Mann-Whitney U test, as they did not follow a normal distribution (normality tested by means of Kolmogorov-Smirnov test). We defined statistical significance as a p-value of less than 0.05.
RESULTS
During the period under study, a total of 166 children were admitted to hospital due to influenza virus infection confirmed by either rapid antigen testing or PCR. Most cases (119/149) were caused by influenza A virus (71.68%), 46 by influenza B virus (27.71%) and 1 corresponded to a coinfection by both serotypes.
The number of children admitted due to influenza varied between seasons: in the 2012-2013 season there were 23 admissions, amounting to 2.69% of the total admissions and 4.43% of admissions due to respiratory disease in the months of the epidemic season; in the 2013-2014 season, there were 20 admissions, amounting to 2.71% of the total admissions and 3.85% of the admissions due to respiratory disease; in 2014-2015 there were 17 admissions, which were 2.03% of the total and 2.43% of respiratory disease admissions; and in 2015-2016 there were 89 admissions, amounting to 9.69% of the total and 11.22% of respiratory disease admissions, and also to 53.61% of the total of influenza-related admissions found in our study, which was a significantly higher proportion compared to the other seasons (p < .0001). Lastly, in the 2016-17 season, 17 children were admitted with influenza (3.71% of respiratory disease admissions and 2.83% of total admissions).
Children with infection by influenza A virus were younger compared to children infected by influenza B virus (mean age, 2.45 years vs 3.88 years; p .003). We did not find statistically significant differences between the influenza A and the influenza B cases in the sex distribution, mean length of stay, need of antibiotics or need of bronchodilators (Table 1). When we compared data for these variables, we excluded the case of coinfection by both influenza virus serotypes.
| Table 1. Comparison of variables by influenza type | ||||
|---|---|---|---|---|
| Influenza A virus | Influenza B virus | P | ||
| Total | 119 | 46 | ||
| Season | 2012-2013 | 14 | 8 | |
| 2013-2014 | 19 | 1 | ||
| 2014-2015 | 14 | 3 | ||
| 2015-2016 | 57 | 32 | ||
| 2016-2017 | 15 | 2 | ||
| Sex | Male | 66 | 20 | NS |
| Female | 53 | 26 | ||
| Age | 2,45 DE 2,74 |
3,88 DE 3,70 |
0,0003 | |
| Length of stay (days) | 5,63 DE 3,08 |
6,36 DE 4,08 |
NS | |
| Pneumonia | 39 DE 32,77% |
9 DE 19,56% |
||
| Oseltamivir | 68 DE 57,14% |
29 DE 63,04% |
||

The cases occurred in 86 boys (51.8%) and 79 girls, and we found no differences in the sex distribution based on the causative serotype. The mean age of the children admitted for influenza was 2.86 years (standard deviation [SD]: 3.05). There were 59 children aged less than 12 months, which corresponded to 35.54% of the total.
A chest X-ray was performed during the hospital stay in 90 children (54.54%), revealing pneumonia in 48 of them (53.33%), who amounted to 28.91% of the total patients with influenza. A blood sample was collected and a complete blood count performed in 130 children (78.31%), of who 82 (63.07%) were treated with antibiotic drugs. A total of 91 children (55.15%) received antibiotherapy at some point, 48 for treatment of pneumonia and 5 for treatment of otitis. Bronchodilators were also given to 62 patients (37.34 %). A total of 11 patients (6.62%) required admission to the PICU, which was more frequent in patients aged less than 12 months (11.86% in infants aged less than 12 months compared to 3.84% of older children, a statistically significant difference: p .054).
The length of stay was slightly longer in patients with pneumonia (0.7 days longer; p .016) and in patients admitted to the PICU (4 days longer; p < .0001). We found no statistically significant differences in length of stay based on age.
A total of 96 patients (57.83%) received oseltamivir during their hospital stay. The mean age of patients that received oseltamivir was lower compared to those that did not, although the difference was not statistically significant. In the 2012-2013 and 2013-2014 seasons, none of the children received oseltamivir, compared to 10 out of the 17 patients in the 2014-2015 season (58.8%), 75 of the 89 patients in the 2015-2016 season (84.3%) and 12 of the 17 patients in the 2016-2017 season (70.58%). We did not find statistically significant differences in the children that received oseltamivir compared to those that did not in the incidence of pneumonia (32.29% versus 24.63%, respectively) or admission to the PICU (8.33% versus 4.34%). A blood test was performed in 79 of the 96 patients treated with oseltamivir (82.29%), while 53 underwent a chest X-ray (55.20%), leading to diagnosis of pneumonia in 31 (32.29%). However, as many as 61 of the 96 patients that received oseltamivir also received antibiotics (63.54%). The main findings are summarised in Table 2.
| Table 2. Comparison of study variables based on whether patients were or not treated with oseltamivir | |||||
|---|---|---|---|---|---|
| Oseltamivir | P | ||||
| Yes | No | ||||
| Total | 96 | 69 | |||
| Season | 2012-2013 | 23 | 0 0% |
23 100% |
|
| 2013-2014 | 20 | 0 0% |
20 100% |
||
| 2014-2015 | 17 | 10 59% |
7 41% |
||
| 2015-2016 | 89 | 75 84% |
14 16% |
||
| 2016-2017 | 17 | 12 70,58% |
5 29,41% |
||
| Sex | Male | 86 | 44 51,11% |
42 | NS |
| Female | 79 | 46 58,22% |
33 | ||
| Age | 2,62 DE 3,01 |
3,2 DE 3,19 |
NS | ||
| Length of stay (days) | 6,19 DE 3,57 |
5,30 DE 3,07 |
0,052 | ||
| Pneumonia | 48 | 31 32,29% |
17 24,63% |
NS | |
| PICU admission | 11 | 7 7,29% |
3 4,34% |
NS | |
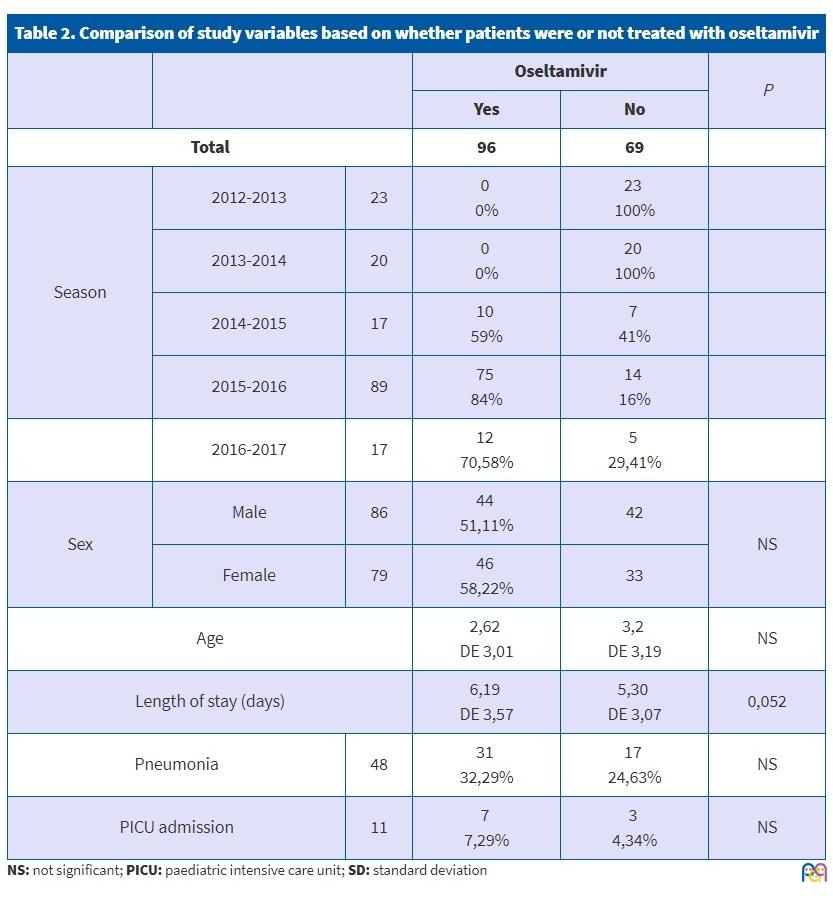
The mean length of stay was slightly longer in the patients that received oseltamivir compared to those that did not (0.89 days), with a p-value near the threshold for statistical significance (p = .052). We also found no significant difference in the mean age of the patients treated with oseltamivir. The mean length of stay of children treated with oseltamivir in the 2015-2016 season was 1.8 days longer compared to children not treated with it (p = .039).
DISCUSSION
The general population and paediatricians perceive influenza in children as a mild illness without important repercussions. This may be partly explained by the dearth of paediatric studies on the clinical presentation and complications of this disease. However, it is known that respiratory infections cause significant morbidity in children, particularly in the younger subset. And influenza not only involves infection of the respiratory tract, but is also associated with many of the most common respiratory complications in childhood, such as acute otitis media or pneumonia.
We studied a total of 166 patients admitted to our hospital with influenza in the 2012-2013 through 2016-2017 epidemic seasons (December-May). Most admissions took place in the cold-weather months, although sporadic cases may occur outside the epidemic season.2 For this reason, we restricted the period under study to the epidemic seasons. In these periods, we found a clear predominance of serotype A over serotype B, with a progressive increase in the prevalence of the latter in recent years. This was consistent with epidemiological studies on influenza.3 The incidence was highest in the 2015-2016 season, when the proportion of hospital admissions was also the highest in our study: 9.69% of total admissions and 11.22% of admissions due to respiratory illness, percentages that were consistent with other published reviews.4,5 One of the reasons for this increase in admissions may be the increased detection of the virus due to technological advances and the performance of these tests in all patients admitted with respiratory illness, in adherence with the recommendation of the Centers for Disease Control and Prevention (CDC).6 We also found that in this epidemic season, there was an overall increase in length of stay compared to other seasons, but with a lower incidence peak, so that the cumulative incidence of admissions for influenza remained stable. The proportion of patients with complications and the mean length of stay were also greater in patients with infection by influenza A virus, although these differences were not statistically significant.
Previous studies have shown that sex is not associated with the probability of admission due to influenza, whereas age is. In our study, we found a higher number of admissions in children of an age to attend child care or school (2-10 years), a group with a significant role in influenza transmission due to the quick spread of the virus in schools and child care centres. Attack rates are highest in children, reaching up to 40% in pre-schoolers and 30% in school-aged children, with potential secondary infection of parents and siblings. The findings of our study were consistent with those of the previous literature.4,5,7
The higher number of admissions in children aged less than 3 years, especially in infants aged less than 12 months, may also be due to coinfection by RSV, although we did not find evidence of this in our study.4,5 The literature describes a higher incidence of complications in this age group, which is why these patients may be treated with these novel antiviral agents. In our sample, 35.34% of admissions occurred in patients aged less than 12 months, and the proportion of patients admitted to the PICU was also significantly greater in this age group compared to older children (p = .03).
Respiratory complications of influenza are relatively frequent and are often the reason for admission or a prolonged length of stay. The complications commonly described in the medical literature, in order of decreasing frequency, are acute bronchitis (in up to 30% of the total cases of influenza), pneumonia and asthma exacerbations. In our series, pneumonia was a complication found in 28.91% of cases of influenza, which was similar to the proportions described in previously published reviews.7-9 The presence of pneumonia in children with influenza was associated with a significant increase in the mean length of stay of 0.7 days (p = 0,016). Other complications in our sample were acute otitis media (3.01% in our sample, compared to 10%-30% in other studies, varying between series) and acute sinusitis (18% of the overall paediatric population with infection by influenza virus).
The use of antivirals for treatment of influenza is currently being debated. During the 2009 pandemic, there was a generalised increase in their use, although it has since been decreasing gradually. The mechanisms of action of these drugs are still unclear, as is their availability, so it is difficult to determine which subset of patients would most benefit from this treatment.10 The medical literature reports that it is more effective in the first hours from onset, when the viral load has yet to peak. It is more beneficial the earlier it is administered (< 48 hours). If more than 48 hours have elapsed since onset, it may still be beneficial in patients that have been hospitalised, with severe or complicated disease or at higher risk of complications.
In paediatrics, the first-line antiviral agent is oseltamivir, a neuraminidase inhibitor. In the 2015-2016 season, treatment in our hospital adhered to the 2011 recommendations of the CDC, according to which oseltamivir was indicated in patients with immunosuppressed status, undergoing chronic treatment with acetylsalicylic acid, with lung disease, heart disease or severe chronic disease, or requiring hospital admission.6 Nevertheless, the decision to use oseltamivir must be made on a case-to-case basis. The proportion of patients that received oseltamivir in the first two seasons under study had been zero, and it climbed to 85% by this last season. The main reason for this substantial increase was the implementation of the new guidelines for diagnosis and management, which were introduced in our hospital in the last season.
Other studies have reported that oseltamivir reduces the duration of fever and other symptoms within 24 hours, as well as the risk of complications.1,11,12 Yet others have reported data that disagreed, with statistically significant results showing no decrease in the risk of acute otitis media or sinusitis in children or adults.1 Some authors have reported a decrease in length of stay in asthmatic patients, but not in the rest.10 As we mentioned above, the effect of oseltamivir is stronger the earlier it is administered, so some studies have only studied its effect in cases diagnosed and treated with it within 48 hours from onset.13 On the other hand, numerous adverse effects have been described in association with this drug (vomiting, headache, dizziness, renal side effects, etc), and it has also been reported that its use does not reduce the incidence of flu-related complications, leading to the recommendation that it not be used save in exceptional cases.3
In most patients that visit the emergency room, influenza is not diagnosed within 48 hours from onset (as management at the outpatient level or at home with antipyretic agents has been usually attempted beforehand), and the timing of rapid antigen detection testing also varies between patients. These are barriers to early treatment of infection and may reduce the potential effectiveness of antiviral medication. In our case series, 57.83% of all patients received oseltamivir. We found a longer mean length of stay (by 0.89 days) in children treated with oseltamivir, a difference that was greatest in the 2015-2016 season, when the length of stay was 1.8 days longer in children that received it compared to children that did not; 29 of those treated with oseltamivir had pneumonia and 16 did not, although some of these patients already had pneumonia at admission. Of the 11 patients that required admission to the PICU, 8 were being treated with oseltamivir and 3 were not. As we mentioned above, these results are inconsistent with those of some of the previously published studies, in which use of oseltamivir is associated with decreases in length of stay and the incidence of complications.
In our study, we did not register the timing of oseltamivir initiation, except for the last season (2016-2017), in which treatment started within 48 hours from onset of symptoms in only 5 of the 12 treated cases (41.66%). Future studies should assess the efficacy of oseltamivir in patients with delayed diagnosis (> 48 hours after onset) that fulfil other criteria, such as requiring hospital admission or presence of underlying chronic disease. This would be relevant in terms of avoiding the use of an expensive drug that is not publicly funded and of questionable effectiveness.
Since this was a descriptive study on hospitalised patients only, we could not compare the efficacy of the drug in patients of similar characteristics that did not require admission. Furthermore, the need for hospital admission suggests that this is a subset of the population that is more vulnerable and likely to develop complications, or perhaps that there may have already been complications at the time of admission. The small sample size is another limitation. Therefore, future studies of a larger scope are still needed.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
CDC: Centers for Disease Control and Prevention ● PCR: polymerase chain reaction ● PICU: Paediatric intensive care unit ● RSV: respiratory syncytial virus ● SD: standard deviation
REFERENCES
- Lafond KE, Nair H, Rasooly MH, Valente F, Booy R, et al. Global role and burden of influenza in pediatric respiratory hospitalizations, 1982-2012: a systematic analysis. PLoS Med. 2016;13:e1001977.
- Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev. 2014;(4):CD008965.
- Cruz-Cañete M, Moreno-Pérez D, Jurado-Ortiz A, García-Martín FJ, López-Siles J. Olalla-Martín L. El virus de la gripe en Pediatría. Un motivo de hospitalización. Enferm Infecc Microbiol Clin. 2007;25:177-83.
- Weil-Olivier C. Gripe estacional infantil. FMC Pediatr. 2015;50:1-19.
- Dawood FS, Chaves SS, Pérez A. Complications and associated bacterial coinfections among children hospitalized with seasonal or pandemic influenza, United States, 2003-2010. J Infect Dis. 2014;209:686-94.
- Arístegui Fernández J. Gripe en Pediatría. Pediatr Integral. 2015;19:694-701.
- Ros Aranal I, Navarra Vicente B. Características clínicas y actuaciones en los niños ingresados por gripe en cuatro periodos epidémicos gripales (2002-2006). An Pediatr (Barc). 2008;68(1):24-9.
- Arostegi Kareaga N, Montes M, Pérez-Yarza EG, Sardón O, Vicente D, Cilla G. Características clínicas de los niños hospitalizados por infección por virus Influenza. An Pediatr (Barc). 2005;62:5-12.
- Vilà de Muga M, Torre Monmany N, Asensio Carretero S, Travería Casanovas FJ, Martínez Mejías A, Coll Sibina MT, et al. Características clínicas de la gripe A H1N1 2009: estudio multicéntrico. An Pediatr (Barc). 2011;75:6-12.
- Buñuel Álvarez JC, González de Dios J. Evidencias de la pandemia por virus influenza A (H1N1). An Pediatr (Barc). 2009;71:379-82.
- Heinonen S, Silvennoinen H, Lehtinen P, Vainionpää R, Vahlberg T, Ziegler T, et al. Early oseltamivir treatment of influenza in children 1-3 years of age: a randomized controlled trial. Clin Infect Dis. 2010;51:887-94.
- Informe de Vigilancia de la Gripe en España. Temporada 2015-2016 (desde la semana 40/2015 hasta la semana 20/2016). Sistema de Vigilancia de la Gripe en España. En: Instituto de Salud Carlos III [en línea] [consultado el 25/07/2018]. Disponible en www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/fd-enfermedades/gripe.shtml.
- Centers for Disease Control and Prevention. Antiviral agents for the treatment and chemoprophylaxis of influenza recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. 2011;60:7-9.
- Rude D. Myths in emergency medicine: still prescribing osetalmivir? Emerg Med News. 2017;39:41.
Comments
JEBlanco commented on 09/10/2018 at 10:38:
Interesante y arduo trabajo. Os animo a revisar los historiales de nuevo, anotando las fechas y horas de inicio de tratamiento para responder a la pregunta clave de si el inicio precoz o no permite ver algún cambio evolutivo. Por otro lado sería interesante tratar de clasificar los pacientes según algún criterio estandarizado (¿Pulmonary Score?, SatO2, Frecuencia respiratoria) para tratar de ver si hubo diferencias al recibir el tto con oseltamivir respecto a los que no lo recibieron. Gracias por mostrar nuestra realidad asistencial. ¡Enhorabuena por vuestro trabajo!