
Vol. 20 - Num. 78
Originales
Evaluación del desarrollo de un grupo de recién nacidos prematuros frente a niños nacidos a término
M.ª Laura Casado Sáncheza, Ángeles Gutiérrez Garcíab, Jesús Ruiz Contrerasc
aPediatra. CS San Blas. Parla. Madrid. España.
bDepartamento de Didáctica y Teoría de la Educación. Facultad de Formación de Profesorado y Educación. Universidad Autónoma de Madrid. Madrid.
cServicio de Pediatría. Hospital Universitario 12 de Octubre. Universidad Complutense de Madrid. Madrid. España.
Correspondencia: ML Casado. Correo electrónico: cs.mlaura@yahoo.es
Cómo citar este artículo: Casado Sánchez ML, Gutiérrez García A, Ruiz Contreras J. Evaluación del desarrollo de un grupo de recién nacidos prematuros frente a niños nacidos a término. Rev Pediatr Aten Primaria. 2018;20:121-31.
Publicado en Internet: 04-04-2018 - Número de visitas: 24908
Resumen
Introducción: actualmente, los recién nacidos prematuros representan el 10% de los nacimientos en España, justificando un 50% de la discapacidad infantil, con un presunto riesgo aumentado de alteraciones en comparación con los nacidos a término. El presente estudio trata de determinar si tienen mayor probabilidad de retraso del desarrollo que estos.
Pacientes y métodos: se han incluido 58 niños menores de seis años de un centro de salud madrileño, que nacieron con 34 o más semanas y menos de 37 de edad gestacional (prematuros tardíos), cuyos controles pareados nacieron a término. Para detectar la existencia de retraso del desarrollo se utilizó el inventario de desarrollo de Battelle.
Resultados: no se encontraron diferencias en las medias de la puntuación total de ambas poblaciones, ni por áreas de desarrollo ni con respecto a las desviaciones típicas (-1,0, -1,5 y -2) frente a no desviación. Veinticuatro de los niños (20,69%) mostraron algún grado de desviación frente a lo considerado un desarrollo normal, de los que 14 (58,3%) no tenían sospecha de retraso. La prevalencia de retrasos se sitúa en 0,224 para los términos y en 0,207 para los prematuros tardíos.
Conclusiones: no se encuentran diferencias en la prevalencia de retrasos entre ambas poblaciones. Dado que en más del 50% de los niños en los que se demostró algún grado de retraso no existía sospecha previa del mismo, se demuestra la necesidad de aplicar protocolos de escrutinio del retraso psicomotor en las visitas del niño sano en Atención Primaria para un diagnóstico precoz.
Palabras clave
● Discapacidades del desarrollo ● Indicadores de desarrollo ● Nacimiento a término ● Recién nacido prematuroINTRODUCCIÓN
La creciente población de niños prematuros de las unidades neonatales ha hecho aparecer nuevos problemas sanitarios1, como los posibles retrasos en el desarrollo. Ello ha conducido a la búsqueda de terapias anticipatorias para minimizar las secuelas de la prematuridad2.
Hay estudios que han demostrado que, a menor edad gestacional, mayor es la morbilidad2. Sin embargo, el aumento de prematuros tardíos puede también tener un riesgo aumentado de alteraciones en el neurodesarrollo e incluso psiquiátricas o de comportamiento durante la vida adulta3,4 en comparación con nacidos a término.
Actualmente, los prematuros representan el 8-10% de los nacimientos en España, justificando un 75% de la mortalidad perinatal y un 50% de la discapacidad infantil5.
El retraso o retardo del desarrollo o retraso psicomotor significa una demora o lentitud en la secuencia normal de adquisición de los hitos del desarrollo sin base patológica, en contraposición al trastorno o alteración del desarrollo, que presupone una perturbación, cambio en la esencia o patrón anormal del desarrollo6.
Diversos estudios han mostrado que los retrasos del desarrollo obedecen a causas muy variadas, como los riesgos maternos (patología mental, infecciosa, tóxica; adolescente o mayor de 35-40 años), los riesgos del niño (desnutrición tras el nacimiento, agentes nocivos como el plomo, infecciones, enfermedades genéticas, ventilación mecánica, exanguinotransfusión…), la falta de cuidado o negligencia en el mismo, antecedentes familiares, etc.7,8, y que el diagnóstico y la intervención precoz con el fin de evitarlas o disminuir sus efectos ofrece mejores resultados a corto, medio y largo plazo9.
Se ha postulado que muchos niños prematuros de entre 34 y 37 semanas de edad gestacional tienen alteraciones del desarrollo identificables desde Atención Primaria. El presente estudio trata de determinar si tienen mayor probabilidad de retraso del desarrollo que los nacidos a término.
PACIENTES Y MÉTODOS
Se planteó un estudio observacional, transversal y analítico, en el centro de salud San Blas, en Parla (Madrid).
Población de estudio
Se han incluido niños de entre 0 y 6 años, atendidos en la consulta de Pediatría del centro de salud referido, que nacieron entre las 34 y las 37 semanas de edad gestacional (prematuros tardíos). Sus controles pareados nacieron a término (37 semanas o más de gestación), del mismo sexo y una fecha de nacimiento lo más próxima posible (precedente o siguiente niño a término del mismo sexo más cercano en fecha de nacimiento; a igualdad de condiciones entre precedente y siguiente, se eligió al siguiente por arbitrariedad). Todos han nacido entre el 1 de junio de 2009 y el 31 de mayo de 2015.
Para calcular el tamaño de la muestra se aplicó la fórmula para diferencias de medias. Se realizó un test bilateral, con un nivel de confianza 1-α del 95% y un poder estadístico del 80%. Se consideró que existía una diferencia clínicamente importante del desarrollo cuando hubo una desviación de 3,5 meses en la consecución de los hitos del desarrollo con respecto al patrón normal. Se tuvo en cuenta la desviación típica global control de otros estudios españoles que arrojó una varianza estimada de 18410. De este modo, se obtuvo un tamaño muestral de 58 pares de niños a término y prematuros tardíos. Este mismo resultado se corrobora mediante el programa estadístico Epidat® 4.1 del Servicio Gallego de Salud11.
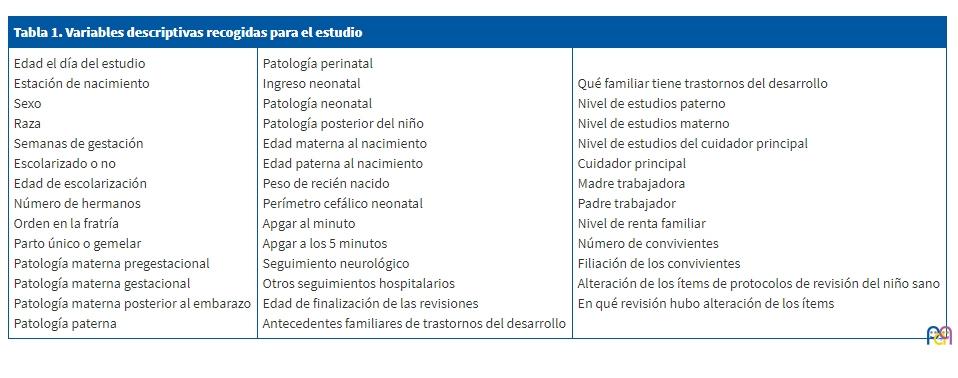
Los prematuros que estudiar se ordenaron por fecha de nacimiento ascendente. Se les numeró correlativamente y se aleatorizaron con la ayuda de una aplicación generadora de número aleatorios (http://nosetup.org/php_on_line/numero_aleatorio_2). Según el tamaño muestral calculado anteriormente, se tomaron solo 58 casos para el estudio (muestra total de los 129 niños), tras comparar las variables de la población total de prematuros y homogeneizar las variables descriptivas detalladas en la Tabla 1, que se recogieron en un formulario web confeccionado para el estudio12. Para detectar la existencia de retraso del desarrollo se utilizó el inventario de desarrollo de Battelle13, considerado como el gold standard para detectar problemas del desarrollo preescolar y del inicio escolar14,15.
| Tabla 1. Variables descriptivas recogidas para el estudio | ||
|---|---|---|
| Edad el día del estudio Estación de nacimiento Sexo Raza Semanas de gestación Escolarizado o no Edad de escolarización Número de hermanos Orden en la fratría Parto único o gemelar Patología materna pregestacional Patología materna gestacional Patología materna posterior al embarazo Patología paterna |
Patología perinatal Ingreso neonatal Patología neonatal Patología posterior del niño Edad materna al nacimiento Edad paterna al nacimiento Peso de recién nacido Perímetro cefálico neonatal Apgar al minuto Apgar a los 5 minutos Seguimiento neurológico Otros seguimientos hospitalarios Edad de finalización de las revisiones Antecedentes familiares de trastornos del desarrollo |
Qué familiar tiene trastornos del desarrollo Nivel de estudios paterno Nivel de estudios materno Nivel de estudios del cuidador principal Cuidador principal Madre trabajadora Padre trabajador Nivel de renta familiar Número de convivientes Filiación de los convivientes Alteración de los ítems de protocolos de revisión del niño sano En qué revisión hubo alteración de los ítems |
El inventario de desarrollo de Battelle cuenta con una prueba de cribado con un alto grado de correlación con la batería completa (0,96, excepto para el área cognitiva, que es de 0,92)13, que fue la que se aplicó a cada niño, independientemente de la edad, posibilitando una comparación homogénea16. Dicha prueba evalúa mediante 96 ítems las habilidades o hitos fundamentales del niño en las áreas personal y social, adaptativa, motora, de comunicación y cognitiva, de 0 a 8 años.
El resultado se expresa como puntuación total y desviación típica (-1,0 -1,5, -2,0 o sin desviación), que indicaría posible retraso13,17.
Para eliminar sesgos, se añade al cuestionario el nivel de estudios y socioeconómico de los padres.
Análisis estadístico
Para variables cualitativas se utilizó el test de la χ2 de Pearson o el test exacto de Fisher. Para variables cuantitativas con distribución normal, la prueba t de Student para muestras independientes en la comparación de los valores medios con un intervalo de confianza del 95%; cuando los grupos comparados fueron más de dos, se aplicó ANOVA de un factor con las correcciones de Bonferroni, Tukey y Scheffe. Las alternativas no paramétricas fueron la U de Mann-Whitney o Kruskal-Wallis.
Se consideró estadísticamente significativo un valor p <0,05, con significación exacta a dos caras (bilateral).
Los datos de los prematuros se analizaron según sus edades cronológica y corregida hasta los dos años. La prevalencia se expresa entre 0 y 1.
Se realizó a partir de la tabla Excel® obtenida del formulario web, con el paquete estadístico IBM SPSS® Statistics 22.
Se obtuvo la evaluación favorable tanto del Comité Ético de Investigación Clínica del Hospital Universitario de Getafe como de la Comisión Local de Apoyo a la Investigación Sur de Madrid. Se pasó una hoja informativa a los tutores y se obtuvo su consentimiento informado.
RESULTADOS
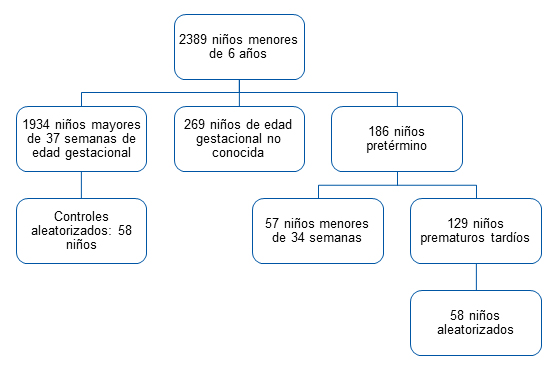
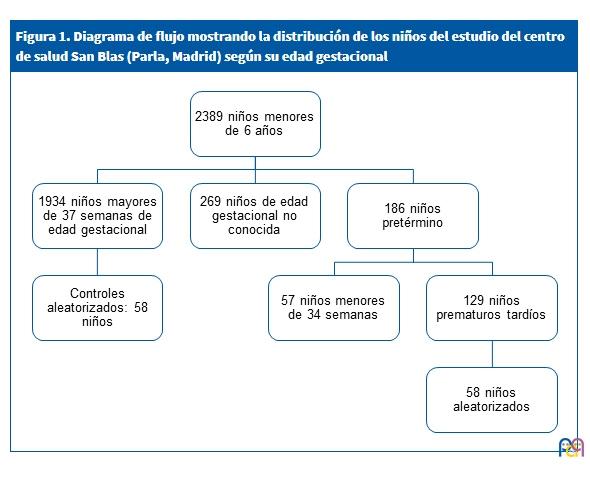
Los nacidos entre el 1 de junio de 2009 y el 31 de mayo de 2015, adscritos a 30 de junio de 2015 al centro, fueron 2389 niños.
Niños prematuros
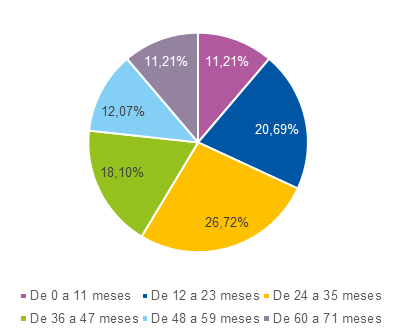
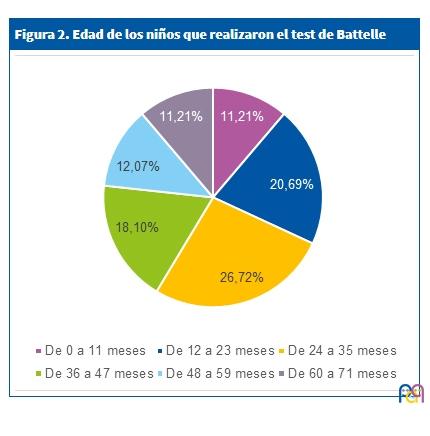
Se identificaron 129 prematuros tardíos, de los que se tomaron 58 aleatoriamente, que correspondieron al 31,2% de los prematuros del centro y al 44,96% de los tardíos. El diagrama de flujo de la Fig. 1 clarifica la distribución de los niños de acuerdo con su edad gestacional y la Fig. 2 muestra la distribución porcentual de la edad de los niños que realizaron el test de Battelle.
| Figura 1. Diagrama de flujo mostrando la distribución de los niños del estudio del centro de salud San Blas (Parla, Madrid) según su edad gestacional |
|---|
 |
| Figura 2. Edad de los niños que realizaron el test de Battelle |
|---|
 |
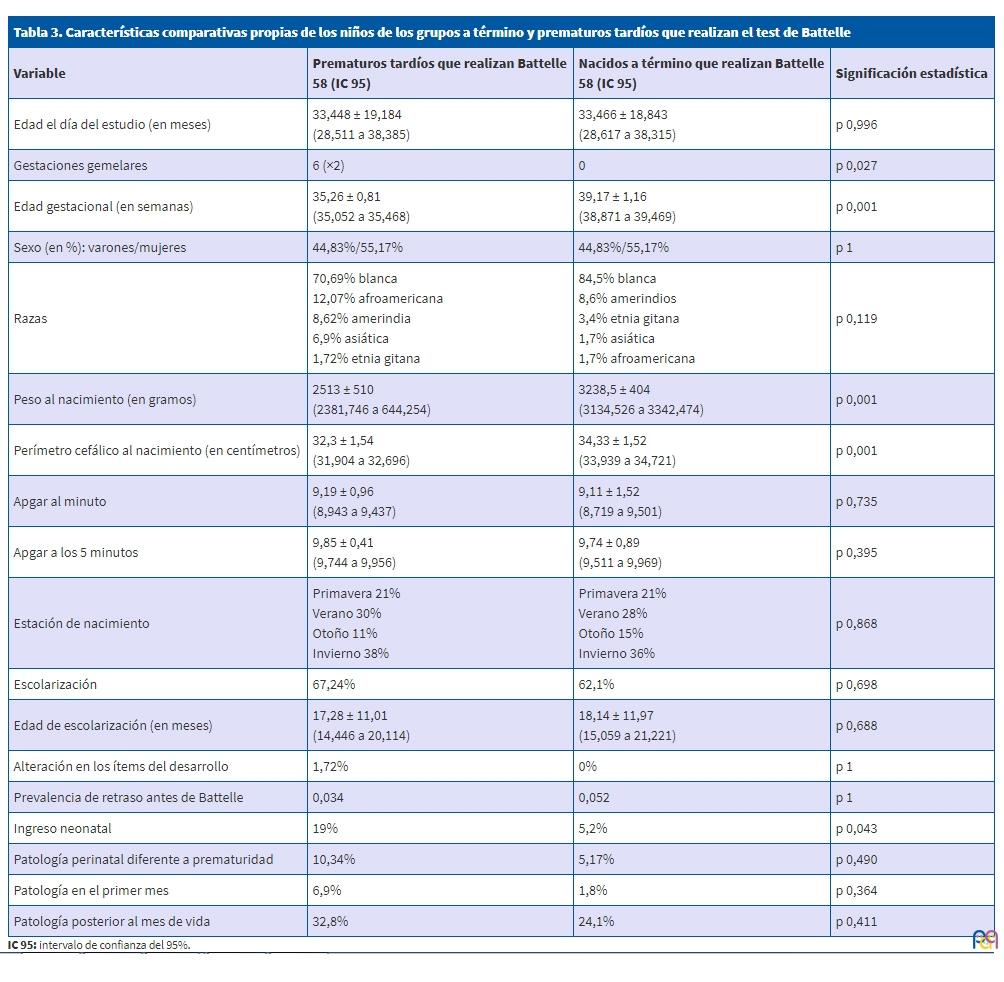
Las poblaciones de los 58 prematuros tardíos incluidos y la total de prematuros fueron similares en cuanto a las variables descriptivas de la Tabla 1. En las revisiones del niño sano, solo uno de los 58 presentó alteraciones en los ítems de desarrollo, un 1,72% de la muestra. Otro presentó dificultades evolutivas sin estar alterados los ítems del desarrollo, estimándose con estos datos una prevalencia de retrasos en los prematuros de 0,034. En cuanto a antecedentes familiares de retraso, solo uno fue un familiar cercano (hermana).
Los progenitores eran sanos, excepto por patología gravídica de origen endocrinológico.
Nacidos a término
La distribución de los nacidos a término por semanas de gestación siguió una curva de Gauss con un mayor porcentaje de nacidos a las 39 semanas.
Un niño presentaba un retraso simple del lenguaje y otros dos sospecha de retraso. Por tanto, la prevalencia de retrasos era de 0,052. Un único caso tenía un familiar directo con retraso diagnosticado (padre).
Tampoco sus progenitores presentaban patología, excepto la endocrinológica, mayoritariamente diabetes gestacional.
Comparación entre poblaciones
En la Tabla 2 se comparan las variables socioeconómicas de las familias de los grupos de estudio, mientras que en la Tabla 3 se comparan las variables entre los prematuros y los nacidos a término en los que se realizó el test de Battelle. Ambas poblaciones fueron similares en características demográficas. Las únicas diferencias significativas fueron la patología gestacional materna y las relacionadas con la prematuridad: la edad gestacional, gestaciones gemelares, ingreso neonatal y peso y perímetro cefálico al nacimiento.
| Tabla 2. Características sociales y familiares comparativas de los grupos a término y prematuros tardíos que realizan el test de Battelle | |||
|---|---|---|---|
| Variable | Prematuros tardíos que realizan Battelle 58 (IC 95) |
Nacidos a término que realizan Battelle 58 (IC 95) |
Significación estadística |
| Edad materna | 31,66 ± 5,61 (30,216 a 33,104) |
31,88 ± 4,91 (30,616 a 33,144) |
p 0,823 |
| Edad paterna | 33,83 ± 6,55 (32,144 a 35,516) |
34,39 ± 4,85 (33,142 a 35,638) |
p 0,602 |
| Renta declarada (en euros) | 24816 ± 16953 (20542,966 a 29179,034) |
29307,27 ± 17447 (24817,099 a 33797,441) |
p 0,162 |
| Número de hermanos | 1,16 ± 1,099 (0,877 a 1,443) |
0,83 ± 0,752 (0,636 a 1,024) |
p 0,062 |
| Orden en la fratría | 1,91 ± 0,978 (1,658 a 2,162) |
1,63 ± 0,645 (1,464 a 1,796) |
p 0,071 |
| Número de convivientes | 3,362 ± 1,2523 (3,040 a 3,684) |
3,069 ± 1,2685 (2,743 a 3,395) |
p 0,213 |
| Antecedentes familiares | 17,24% | 17,2% | p 1 |
| Patología pregestacional materna | 13,8% | 17,3% | p 0,798 |
| Patología gestacional materna | 48,3% | 27,6% | p 0,035 |
| Patología materna posterior al embarazo | 20,7% | 15,5% | p 0,630 |
| Patología paterna | 6,9% | 12,1% | p 0,528 |
| Madre trabajadora/en paro | 57%/43% | 55%/45% | p 1 |
| Padre trabajador/en paro | 81%/17% | 91%/9% | p 0,177 |
| Cuidador principal la madre (en exclusividad) | 94,8% (69%) | 93,1% (65,5%) | p 1 (p 0,843) |
| Estudios maternos | Sin estudios 3,4% Primarios 25,9% Secundarios 48,3% Universitarios 20,7% NS/NC 1,7% |
Sin estudios 1,7% Primarios 37,9% Secundarios 36,2% Universitarios 22,4% Máster 1,7% |
p 0,454 |
| Estudios primarios maternos en % | 25,9% | 37,9% | p 0,232 |
| Estudios paternos | Sin estudios 1,7% Primarios 29,3% Secundarios 48,3% Universitarios 15,5% NS/NC 5,2% |
Sin estudios 1,7% Primarios 36,2% Secundarios 44,8% Universitarios 13,8% NS/NC 3,4% |
p 0,945 |

| Tabla 3. Características comparativas propias de los niños de los grupos a término y prematuros tardíos que realizan el test de Battelle | |||
|---|---|---|---|
| Variable | Prematuros tardíos que realizan Battelle 58 (IC 95) |
Nacidos a término que realizan Battelle 58 (IC 95) |
Significación estadística |
| Edad el día del estudio (en meses) | 33,448 ± 19,184 (28,511 a 38,385) |
33,466 ± 18,843 (28,617 a 38,315) |
p 0,996 |
| Gestaciones gemelares | 6 (×2) | 0 | p 0,027 |
| Edad gestacional (en semanas) | 35,26 ± 0,81 (35,052 a 35,468) |
39,17 ± 1,16 (38,871 a 39,469) |
p 0,001 |
| Sexo (en %): varones/mujeres | 44,83%/55,17% | 44,83%/55,17% | p 1 |
| Razas | 70,69% blanca 12,07% afroamericana 8,62% amerindia 6,9% asiática 1,72% etnia gitana |
84,5% blanca 8,6% amerindios 3,4% etnia gitana 1,7% asiática 1,7% afroamericana |
p 0,119 |
| Peso al nacimiento (en gramos) | 2513 ± 510 (2381,746 a 644,254) |
3238,5 ± 404 (3134,526 a 3342,474) |
p 0,001 |
| Perímetro cefálico al nacimiento (en centímetros) | 32,3 ± 1,54 (31,904 a 32,696) |
34,33 ± 1,52 (33,939 a 34,721) |
p 0,001 |
| Apgar al minuto | 9,19 ± 0,96 (8,943 a 9,437) |
9,11 ± 1,52 (8,719 a 9,501) |
p 0,735 |
| Apgar a los 5 minutos | 9,85 ± 0,41 (9,744 a 9,956) |
9,74 ± 0,89 (9,511 a 9,969) |
p 0,395 |
| Estación de nacimiento | Primavera 21% Verano 30% Otoño 11% Invierno 38% |
Primavera 21% Verano 28% Otoño 15% Invierno 36% |
p 0,868 |
| Escolarización | 67,24% | 62,1% | p 0,698 |
| Edad de escolarización (en meses) | 17,28 ± 11,01 (14,446 a 20,114) |
18,14 ± 11,97 (15,059 a 21,221) |
p 0,688 |
| Alteración en los ítems del desarrollo | 1,72% | 0% | p 1 |
| Prevalencia de retraso antes de Battelle | 0,034 | 0,052 | p 1 |
| Ingreso neonatal | 19% | 5,2% | p 0,043 |
| Patología perinatal diferente a prematuridad | 10,34% | 5,17% | p 0,490 |
| Patología en el primer mes | 6,9% | 1,8% | p 0,364 |
| Patología posterior al mes de vida | 32,8% | 24,1% | p 0,411 |
Resultados del test
No se encontraron diferencias en las medias de la puntuación total de ambas poblaciones, ni por áreas de desarrollo ni con respecto a las desviaciones típicas (-1, -1,5 y -2) frente a no desviación (Tabla 4).
| Tabla 4. Comparación entre poblaciones a término y de prematuros tardíos en cuanto a los resultados globales y parcelados del test de cribado de Battelle por puntuaciones y por desviaciones típicas vs no desviación | |||||||
|---|---|---|---|---|---|---|---|
| Variable (media de puntos) |
Prematuros tardíos que realizan Battelle 58 (IC 95) |
Nacidos a término que realizan Battelle 58 (IC 95) |
Significación estadística | Variable (en número de niños con desviación típica en cada muestra) | Prematuros tardíos que realizan Battelle 58 |
Término que realizan Battelle 58 |
Significación estadística |
| Total del test de Battelle (puntos) | 98,345 ± 43,8 (87,073 a 109,617) |
100,103 ± 42,37 (89,199 a 111,007) |
p 0,826 | Total de test de Battelle con desviaciones típicas | 11 | 13 | p 0,819 |
| Área personal y social | 22,35 ± 10,19 (19,727 a 24,973) |
22,62 ± 9,53 (20,167 a 25,073) |
p 0,883 | Área personal y social | 21 | 17 | p 0,553 |
| Área adaptativa | 21,14 ± 9,72 (18,638 a 23,642) |
21,62 ± 9,64 (19,139 a 24,101) |
p 0,789 | Área adaptativa | 12 | 13 | p 1 |
| Área motora | 19,97 ± 9,16 (17,613 a 22,327) |
20,66 ± 9,16 (18,303 a 23,017) |
p 0,686 | Área motora | 12 | 11 | p 1 |
| Área de comunicación | 17,03 ± 7,27 (15,159 a 18,901) |
17,03 ± 7,18 (15,182 a 18,878) |
p 1 | Área de comunicación | 12 | 17 | p 0,391 |
| Área cognitiva | 17,69 ± 8,42 (15,523 a 19,857) |
18 ± 8,18 (15,895 a 20,105) |
p 0,841 | Área cognitiva | 22 | 15 | p 0,84 |
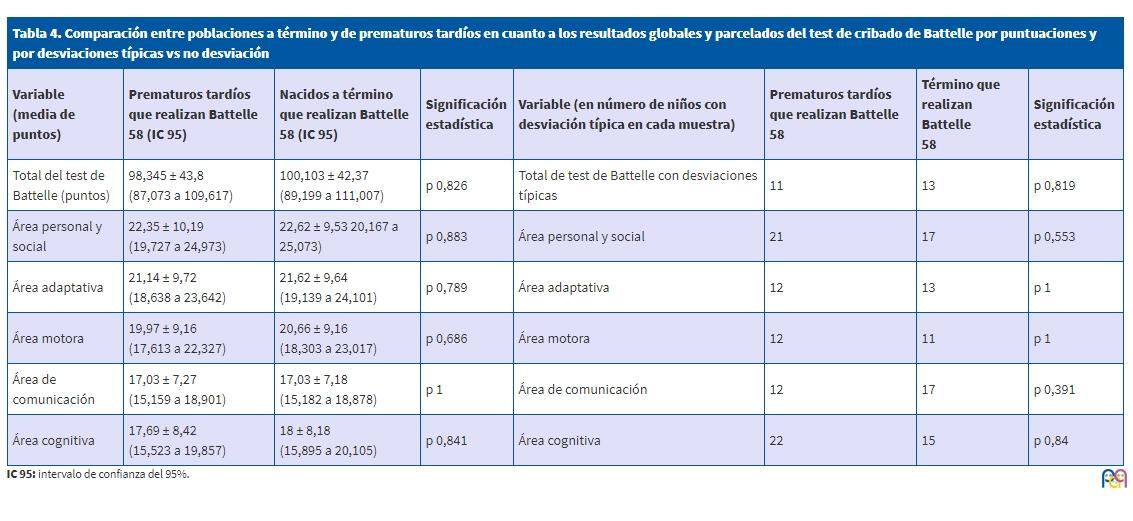
No obstante, en las desviaciones globales se detectaron cinco nacidos a término con una desviación de -2 frente a un prematuro, siete prematuros con -1 desviación frente a cinco nacidos a término, y tres para cada grupo para -1,5 desviaciones. Ante esta observación, se categorizaron los grupos entre niños que obtuvieron desviación -2, -1,5 y -1 frente al resto. Para ello se realizó una comparación entre los niños prematuros y a término en cada categoría de desviaciones, correspondiendo al azar este resultado, pues no existen diferencias estadísticamente significativas entre sendos grupos (p 0,206 para -2 desviaciones, p 1 para -1,5 desviaciones y p 0,762 para -1 desviaciones).
De estos 24 niños, 14 con desviaciones (58,3%) no tenían sospecha de retraso psicomotor.
Asumiendo que el cribado se corresponde con la batería completa, el número y prevalencia de retrasos han aumentado (0,224 para los términos y 0,207 para los prematuros). Solo hubo un caso de un niño que no presentaba alteraciones en el momento del estudio, que sí las había tenido en el pasado, contabilizándose como retraso.
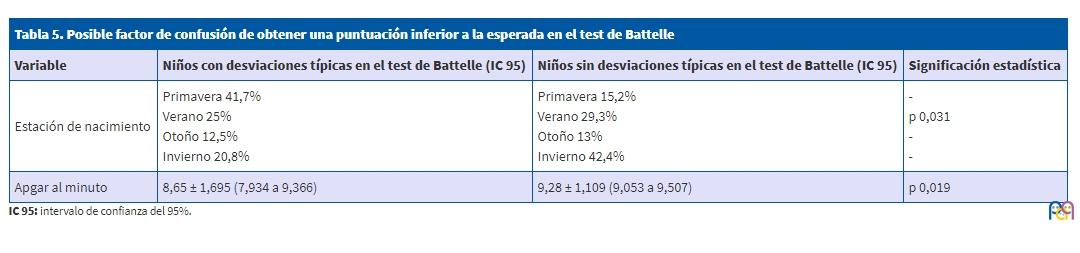
Se han comparado las variables detalladas en la Tabla 1, categorizando a los niños entre los que presentaban desviación frente a no desviación después de realizar la prueba de cribado. Se pretende así identificar factores de riesgo, encontrándose la estación de nacimiento y el Apgar al primer minuto como posibles predisponentes a padecer retraso del desarrollo (Tabla 5).
| Tabla 5. Posible factor de confusión de obtener una puntuación inferior a la esperada en el test de Battelle | |||
|---|---|---|---|
| Variable | Niños con desviaciones típicas en el test de Battelle (IC 95) | Niños sin desviaciones típicas en el test de Battelle (IC 95) | Significación estadística |
| Estación de nacimiento | Primavera 41,7% Verano 25% Otoño 12,5% Invierno 20,8% |
Primavera 15,2% Verano 29,3% Otoño 13% Invierno 42,4% |
p 0,031 |
| Apgar al minuto | 8,65 ± 1,695 (7,934 a 9,366) | 9,28 ± 1,109 (9,053 a 9,507) | p 0,019 |
DISCUSIÓN
El presente estudio es el primero realizado de estas características en población española, comparando retrasos del desarrollo mediante el test de Battelle, entre prematuros tardíos y nacidos a término.
Contradiciendo la literatura médica existente, nuestro estudio demuestra que los prematuros tardíos tienen un desarrollo psicomotor similar al de los nacidos a término18-22. Esta similitud se constata en diferentes edades por debajo de los seis años, tanto en la puntuación total del test, que engloba las habilidades o hitos del niño en las áreas personal y social, adaptativa, motora, de comunicación y cognitiva, como específicamente en cada área, teniendo en cuenta tanto la edad cronológica como la corregida. Nuestros hallazgos se asemejan a los del estudio de Demestre et al. (2016), en el que no se encontraron diferencias en la puntuación global del test ASQ-3 a los 48 meses22.
La prevalencia de retrasos del desarrollo obtenida tras evaluar a los sujetos es muy similar para ambas poblaciones (0,224 para nacidos a término y 0,207 para los prematuros). Estas cifras son ligeramente superiores a las encontradas en Navarra, donde un estudio que evaluó el desarrollo de los niños de 0 a 6 años encontró un 11,2% de retrasos (prevalencia de 0,112), aunque en realidad ese valor corresponde a patologías reales de desarrollo y no incluye simples retrasos en la adquisición de los hitos evolutivos, lo que puede explicar la diferencia porcentual entre los estudios23. Dentro de la misma franja etaria, en Argentina se observó inesperadamente una cifra mucho más alta, un 57% (0,57), hecho que puede ser explicado porque se utilizó una batería de pruebas y exámenes complementarios en varios días para determinar si había patología del desarrollo, y no únicamente una prueba de cribado24. Las muestras parleñas se encuentran entre los datos de ambos trabajos.
Se puede afirmar que la población menor de seis años del centro de salud San Blas presenta un nivel de desarrollo similar entre los niños nacidos después de las 34 semanas de gestación.
Esto no concuerda con estudios previos, realizados en población anglosajona o gala, con otros test de evaluación, valorando en muchas ocasiones únicamente a niños prematuros extremos (criterio de exclusión en este estudio) u otras variables18-22.
Tampoco coincide con la prevalencia hallada en el estudio catalán, que fue de 0,17 en los prematuros tardíos, y de 0,05 en los nacidos a término22. La causa de estas discrepancias no está clara. Por un lado, quizás dicha población no sea comparable a la de nuestro estudio, ya que en el grupo de nacidos a término ellos excluyen a los niños que tuvieron un ingreso neonatal22. Además, el test se pasó entre los 45 y 50 meses y 30 días, no a cualquier edad, como en este estudio, por debajo de los seis años, periodo en el que puede haberse superado un retraso del desarrollo que comenzó en edades más tempranas, o puede no haber comenzado alguna patología de debut más tardío. También puede ocurrir que al utilizarse otros test, no se evalúe exactamente el mismo grado de desarrollo. Es destacable la diferente aplicación de los cuestionarios, pues en el estudio catalán lo rellenaban los padres, incluyéndose nueve cuestiones que respondían de forma subjetiva, frente a la batería de administración directa que se empleó en el presente estudio, a priori más objetiva. Esto podría explicar la menor prevalencia de retrasos del desarrollo hallados en el estudio de Demestre et al. (2016), aunque en niños mayores de 31 meses no parece haber diferencia de estimación de retraso del desarrollo entre el ASQ-3 utilizado por ellos y el inventario de desarrollo de Battelle del presente trabajo25.
Por otro lado, en un centro de salud asturiano se han estudiado unas poblaciones comparables a las del presente trabajo en cuanto a variables descriptivas, como edad gestacional, peso al nacimiento, sexo, patología perinatal y enfermedades posteriores26. Dicho estudio no encuentra diferencias entre el consumo de recursos sanitarios de prematuros y términos, medidos como número de visitas al pediatra y a la enfermera, número de derivaciones a especialistas o pruebas complementarias realizadas26, lo que puede tener como trasfondo un similar grado de patología, como en el presente estudio.
En cualquier caso, habría que buscar concienzudamente y comprobar los motivos por los que la población parleña no sigue los patrones de la mayoría de los estudios publicados.
En un 58,3% de los retrasos diagnosticados con el test no había sospecha previa, confirmándose un infradiagnóstico. Esto pone de manifiesto la necesidad de sensibilizar a padres, profesores y pediatras, para ofrecer una atención individualizada a su patología, así como el uso de test de escrutinio de forma protocolizada en las consultas pediátricas ambulatorias del niño sano.
Aunque el diseño del estudio no es el idóneo para encontrar factores de riesgo de retraso diferentes de la prematuridad, se ha confirmado la puntuación del Apgar al minuto como uno de ellos8.
Un hallazgo relevante del presente estudio es que algunos factores como el nivel socioeconómico, la raza negra, los hábitos tóxicos o las infecciones no se han asociado a mayor riesgo de retraso psicomotor, a diferencia de lo que sucede en otros estudios27. Es posible que el diseño o el tamaño muestral de nuestro estudio no hayan permitido demostrar las diferencias.
Otro hallazgo sorprendente, no reflejado en la bibliografía, es la asociación entre retraso del desarrollo y estación de nacimiento: nacer en primavera se asocia con más sospechas de retraso; el invierno, con menor prevalencia.
La importancia de la estacionalidad en la presentación de algunas enfermedades está demostrada. Existen enfermedades con variación estacional, como más infecciones respiratorias en invierno28; otras, con picos de incidencia en verano (apendicitis, diverticulitis, infarto agudo de miocardio, fibrilación auricular), sin causa aparente de esta variabilidad29. En esta línea se lanza la hipótesis de una posible asociación entre estación de nacimiento y retraso del desarrollo.
Hay estudios que relacionan prematuridad y estacionalidad con resultados contradictorios, aunque no con retraso del desarrollo. Así, en poblaciones como la japonesa se encuentra un incremento de prematuros en verano e invierno30. En la población africana, en julio y octubre31. Otros estudios la relacionan con el inicio de la época seca en Zimbabue, el otoño en Bangladesh o el invierno en Londres32. En otros se correlaciona con factores como edad materna o raza33. Ninguna de estas asociaciones se confirma en el presente trabajo.
Queda por determinar si esta estacionalidad tiene repercusión en el retraso del desarrollo, si depende de la población, de nacer en primavera, o de variables relacionadas con esta estación, que podrían ser detectadas con un análisis multivariante con mayor tamaño muestral.
A pesar de la elaboración minuciosa del estudio, existen ciertas limitaciones que deben tenerse en cuenta a la hora de interpretar los resultados. De entrada, la arbitrariedad de asumir una diferencia clínicamente significativa en ±3,5 meses para el cálculo del tamaño muestral no representa lo mismo en unas edades que en otras. No significa lo mismo tener un retraso del desarrollo de 3,5 meses a la edad de tres meses que a los cinco años. No obstante, la prueba de cribado de Battelle proporciona desviaciones estándar para cada valor etario, lo que corrige este posible sesgo.
Por otro lado, dado que es un estudio descriptivo que no pretende extrapolar sus datos a la población general, no se contempla que la muestra pareada sea representativa de la población general, aunque se comparen los resultados con la bibliografía existente. No obstante, los estrechos intervalos de confianza del 95% que se registraron pueden hacer válidos estos resultados entre poblaciones de similares características. Solo la edad de inicio de escolarización tenía seis meses de intervalo de confianza, ligeramente amplio, para ambos grupos. El resto de las variables se movían en márgenes estrechos.
Por último, en el estudio no se diferencia entre prematuros que tuvieron patología perinatal que favorezca retrasos en el desarrollo (hipoxia perinatal, hemorragia periventricular, etc.) de los que no la tuvieron, como tampoco se tienen en consideración otros factores que pueden ser la causa de retrasos independientemente de la edad gestacional. No obstante, sí se pregunta en el cuestionario, aunque dado el tamaño muestral y el diseño del estudio, no se obtienen datos significativos de estos factores de confusión.
CONCLUSIONES
En conclusión, en nuestro estudio no hay diferencias en la prevalencia de retrasos en los nacidos a término (0,224) frente a los prematuros tardíos (0,207). Dado que en más del 50% de los niños en los que se demostró algún grado de retraso no existía sospecha previa del mismo, nuestro estudio demuestra la necesidad de aplicar protocolos de escrutinio del retraso psicomotor en las visitas del niño sano.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
AGRADECIMIENTOS
A todos aquellos pequeños pacientes y sus familias que colaboraron desinteresadamente en este estudio.
BIBLIOGRAFÍA
- Martínez Gertner M. Eficacia de una breve intervención temprana basada en la evaluación del desarrollo del neonato prematuro: efecto sobre el estrés, la depresión y las percepciones maternas [tesis doctoral]. En: Universitat Autònoma de Barcelona [en línea] [consultado el 03/04/2018]. Disponible en www.tdx.cat/bitstream/handle/10803/32092/mmg1de1.pdf;jsessionid=B5E0D176D4825FD8F37940D2FCF9DD1A.tdx1?sequence=1
- Tosca Segura R. Prematuros extremos: ¿es posible establecer un límite de viabilidad? Anales (Reial Acadèmia de Medicina de la Comunitat Valenciana). 2011;12:1-20.
- Hurtado Suazo JA, García Reymundo M, Calvo Aguilar MJ, Ginovart Galiana G, Jiménez Moya A, Trincado Aguinagalde MJ, et al. Recomendaciones para el manejo perinatal y seguimiento del recién nacido prematuro tardío. An Pediatr (Barc). 2014;81:327.e1-327.e7.
- De Jong M, Verhoeven M, van Baar AL. School outcome, cognitive functioning, and behaviour problems in moderate and late preterm children and adults: a review. Sem Fetal & Neonatal Med. 2012;17:163-9.
- Pallás Alonso CR, Grupo PrevInfad/PAPPS Infancia y Adolescencia. Actividades preventivas y de promoción de la salud para niños prematuros con una edad gestacional menor de 32 semanas o un peso inferior a 1500 g. Del alta hospitalaria a los siete años (1.ª parte). Rev Pediatr Aten Primaria. 2012;14:153-66.
- Contreras MM. Clasificaciones diagnósticas de los trastornos del desarrollo. En: Lejarraga H. Desarrollo del niño en contexto. Buenos Aires: Paidós SAICF; 2004. p. 143-92.
- Lira MI. Factores de riesgo para el desarrollo psicomotor del lactante de nivel socioeconómico bajo. Rev Chil Pediatr. 1994;65:21-7.
- Ramos Sánchez I. Detección y diagnóstico precoz de los trastornos del desarrollo psicomotor. Vox Paediatrica. 2007;15:36-43.
- Guillois B, Castel S, Beunard A, Blaizot X, Creveuil C, Proia-Lelouey N. Efficacité des programmes d’intervention précoce auprès des familles sur le développement neuro-comportemental des enfants prématurés. Arch Pédiatrie. 2013;20:132-3.
- Moraleda Barreno E, Romero López M, Cayetano Menéndez MJ. La prueba de cribado del inventario de desarrollo de Battelle para la detección precoz de alteraciones del desarrollo. An Pediatr (Barc). 2011;75:372-9.
- Hervada X, Naveira G, Santiago MI, Mujica OJ, Vázquez E, Manrique R, et al. Epidat: programa para análisis epidemiológico de datos. Versión 4.1, octubre 2014. En: Xunta de Galicia [en línea] [consultado el 03/04/2018]. Disponible en www.sergas.gal/Saude-publica/EPIDAT
- Casado Sánchez ML. Prematuros tardíos vs a término ¿hay diferencias en cuanto a retrasos del desarrollo? En: Google Forms [en línea] [actualizado el 07/07/2015; consultado el 03/04/2018]. Disponible en http://goo.gl/forms/16bKHCx2hB
- Newborg J, Stock J, Wnek L. Inventario de desarrollo Battelle. Madrid: TEA; 1996.
- Glascoe FP, Martín ED, Humphrey S. A comparative review of developmental screening tests. Pediatrics. 1990;86:547-54.
- Glascoe FP, Byrne KE. The usefulness of the Battelle Developmental Inventory Screening Test. Clin Pediatr (Phila). 1993;32:273-80.
- Berls AT, McEwen IR. Battelle Developmental Inventory. Phys Ther. 1999;79:776-83.
- Glascoe FP. Are overreferrals on developmental screening tests really a problem? Arch Pediatr Adolesc Med. 2001;155:54-9.
- Snider L, Majnemer A, Mazer B, Campbell S, Bos AF. Prediction of motor and functional outcomes in infants born preterm assessed at term. Pediatr Phys Ther. 2009;21:2-11.
- De Kieviet JF, van Elburg RM, Lafeber HN, Oosterlaan J. Attention problems of very preterm children compared with age-matched term controls at school-age. J Pediatr. 2012;161:824-9.
- Brémond M, Blond MH, Chavet-Queru MS, Hémar I, Miret S, Lionnet C, et al. Devenir médical, psychologique et affectif à l’âge d’un an des prématurés indemnes de handicap sévère. Étude prospective cas-témoins. Arch Pédiatr. 1999;6:1163-71.
- Blond MH, Castello-Herbreteau B, Ajam E, Lecuyer AI, Fradet A, Patat C, et al. Devenir médical, cognitif et affectif à l’âge de quatre ans des prématurés indemnes de handicap sévère. Étude prospective cas-témoins. Arch Pédiatr. 2003;10:117-25.
- Demestre X, Schonbaut L, Morillas J, Martínez-Nadal S, Vila C, Raspall F, et al. Riesgo de déficits en el desarrollo en los prematuros tardíos: evaluación a los 48 meses mediante el Ages & Stages Questionnaires®. An Pediatr (Barc). 2016;84:39-45.
- Álvarez Gómez MJ, Soria Aznar J, Galbe Sánchez-Ventura J, Grupo de Pediatría para el Desarrollo de la Asociación Española de Pediatría de Atención Primaria. Importancia de la vigilancia del desarrollo psicomotor por el pediatra de Atención Primaria: revisión del tema y experiencia de seguimiento en una consulta en Navarra. Rev Pediatr Aten Primaria. 2009;11:65-87.
- Pascucci MC, Lejarraga H, Kelmansky D, Álvarez M, Boullón M, Breiter P, et al. Validación de la prueba nacional de pesquisa de trastornos de desarrollo psicomotor en niños menores de 6 años. Rev Chil Pediatr. 2004;75:75-6.
- Rubio-Codina M, Araujo MC, Attanasio O, Grantham-McGregor S. Validez concurrente y viabilidad de pruebas cortas comúnmente usadas para medir el desarrollo infantil temprano en estudios a gran escala: metodología y resultados. En: Banco Interamericano de Desarrollo [en línea] [consultado el 03/04/2018]. Disponible en: https://publications.iadb.org/handle/11319/7823?locale-attribute=es&
- López Martínez A, Mantecón Fernández L, González Álvarez CE, Arias Llorente RP. Consumo de recursos sanitarios en Atención Primaria de los prematuros tardíos. Estudio caso-control en un centro de salud urbano [carta científica]. An Pediatr (Barc). 2015;83:213-5.
- Álvarez Mingorance, P. Morbilidad y secuelas de los niños prematuros en edad escolar [tesis doctoral]. En: Universidad de Valladolid [en línea] [consultado el 03/04/2018]. Disponible en http://uvadoc.uva.es/handle/10324/113
- Llor C, Hernández S. Enfermedad infecciosa en Atención Primaria: estudio prospectivo efectuado durante todo un año. Enferm Infecc Microbiol Clin. 2010;28:222-6.
- Guerrero Guerrero VH. Diverticulitis. Cambiando los paradigmas en el tratamiento. Cir Gen. 2013;35:S41-2.
- Matsuda S, Kahyo H. Seasonality of preterm births in Japan. Int J Epidemiol. 1992;21:91-100.
- Rayco-Solon P, Fulford AJ, Prentice AM. Differential effects of seasonality on preterm birth and intrauterine growth restriction in rural Africans. Am J Clin Nutr. 2005;81:134-9.
- Lee SJ, Steer PJ, Filippi V. Seasonal patterns and preterm birth: a systematic review of the literature and an analysis in a London-based cohort. BJOG. 2006;113:1280-8.
- Cooperstock M, Wolfe RA. Seasonality of preterm births in the collaborative perinatal project: demographic factors. Am J Epidemiol. 1986;124:234-41.