
Vol. 19 - Num. 76
Originales
Test rápido de detección de antígeno estreptocócico en faringoamigdalitis: impacto sobre el uso de antibióticos
César García Veraa, Mercedes Cemeli Canob, Esther María Peralta Rufasc, Elvira Romeo Lázarod, María Belén Pina Gadeae
aPediatra. CS José Ramon Muñoz Fernández. Zaragoza. España.
bPediatra. CS Valdespartera-Montecanal. Zaragoza. España.
cMIR-Pediatría. Hospital Universitario Infantil Miguel Servet. Zaragoza. España.
dPediatra. CS San José Norte. Zaragoza. España.
eFarmacéutica de Atención Primaria. Sector Zaragoza II. Servicio Aragonés de Salud. Zaragoza. España.
Correspondencia: C García. Correo electrónico: cgarciavera@gmail.com
Cómo citar este artículo: García Vera C, Cemeli Cano M, Peralta Rufas EM, Romeo Lázaro E, Pina Gadea MB. Test rápido de detección de antígeno estreptocócico en faringoamigdalitis: impacto sobre el uso de antibióticos. Rev Pediatr Aten Primaria. 2017;19:345:54.
Publicado en Internet: 23-11-2017 - Número de visitas: 41057
Resumen
Objetivo: investigar el impacto de la utilización del test rápido de detección de antígeno estreptocócico sobre la prescripción de antibióticos en niños.
Pacientes y métodos: estudio observacional, de cohortes retrospectivo, a partir de los registros clínicos informatizados de 10 cupos de Pediatría de centros de salud de la provincia de Zaragoza (España) en los años 2012 y 2013. Se hace una valoración del tratamiento antibiótico y de las complicaciones en el mes siguiente al episodio de faringoamigdalitis comparando los episodios en los que se realizó test rápido de detección de antígeno estreptocócico con los que no se realizó.
Resultados: de 17 455 episodios registrados, se seleccionaron 851 que cumplían los criterios de inclusión (tres o cuatro criterios de Centor). En los episodios en los que se realizaron test rápidos de detección de antígeno, la reducción en la prescripción antibiótica fue del 42% (reducción absoluta de riesgo: 42%; intervalo de confianza del 95% [IC 95]: 37 a 48; p < 0,001). Comparando el abordaje entre los pediatras que disponían y utilizaban el test (4), con los que no (6), la reducción absoluta de riesgo fue del 29% (IC 95: 24 a 34; p < 0,001). Se presentaron complicaciones infecciosas en el 12% de los tratados y en el 8% de los no tratados (riesgo relativo: 1,49; IC 95: 0,88 a 2,52; p = 0,178). Se prescribió significativamente más penicilina V que amoxicilina cuando se realizó test diagnóstico (riesgo relativo: 1,30; IC 95: 1,10 a 1,55; p = 0,004).
Conclusiones: en la práctica clínica, el uso de una prueba rápida de detección de antígeno en pacientes pediátricos preseleccionados por criterios clínicos de faringoamigdalitis estreptocócica contribuye de forma determinante al uso racional de antibióticos.
Palabras clave
● Antibióticos ● Evaluación de medicamentos ● Faringitis ● Niño ● Test rápidosINTRODUCCIÓN
Para el abordaje de la faringoamigdalitis (FA) pediátrica en Atención Primaria, la mayoría de las guías de práctica clínica más recientes1-8 recomiendan que únicamente se traten con antimicrobianos las confirmadas como estreptocócicas (FAS). Salvo alguna excepción, que recomienda que en función de la gravedad del cuadro clínico se trate o no sin diagnóstico etiológico9,10, el resto proponen el uso de test rápidos de detección de antígeno estreptocócico (TRDA) o, en su defecto, la utilización del cultivo tradicional. Esta propuesta diagnóstica normalmente va condicionada a la elección de pacientes con unos mínimos criterios clínicos que sugieran que la FA es estreptocócica. Es decir, el objetivo es iniciar tratamiento antibiótico solamente cuando se confirma la sospecha clínica de que estamos ante una FAS mediante TRDA o cultivo.
Ningún signo o síntoma aislado de FAS tiene el suficiente cociente de probabilidad positivo como para variar la probabilidad posprueba a un nivel satisfactorio11-13. Por esta razón, los criterios clínicos servirían para elegir a los pacientes a los que aplicar las pruebas diagnósticas, de manera que no cualquier paciente con algunos signos y síntomas de FA es candidato a la prueba diagnóstica. Se proponen un conjunto de datos mínimos, que en bastantes ocasiones se agrupan en escalas de predicción clínica, de las que las más utilizadas y validadas14 para la edad pediátrica son las de Centor15 y la modificada, a partir de esta, por McIsaac16.
Muy pocos estudios, sin embargo, se han hecho sobre el rendimiento de los TRDA en pacientes preseleccionados, en la realidad de las consultas. Ayanruoh, en 2009, publica un estudio realizado a pacientes que acuden a un Servicio de Urgencias de un hospital de Nueva York y demuestra que la implantación del procedimiento diagnóstico supone una reducción de un 50% aproximadamente en la prescripción de antibióticos en los procesos de FA17. Otro amplísimo estudio poblacional estadounidense con datos del National Ambulatory Medical Care Survey (NAMCS) de 1995 a 2003 mostró una reducción significativa en el porcentaje de prescripción de antibiótico asociada al uso de test diagnóstico. Entre los casos codificados como amigdalitis, faringitis u odinofagia estreptocócica se prescribió antibiótico en el 57% de los que se realizó test frente a un 73% en los que no se realizó18. En Atención Primaria, salvo estudios de pruebas diagnósticas valorando los diferentes TRDA, hay pocas investigaciones que valoren su impacto real una vez implantados. De la Flor estima una reducción del 54,5% en la prescripción de antibióticos en procesos de FAS pediátrica con su utilización en población pediátrica de Barcelona19.
El objetivo de este estudio es, a partir de registros clínicos, comprobar la utilidad real del TRDA en Atención Primaria pediátrica, valorando su impacto sobre el consumo de antibióticos y las complicaciones próximas al episodio según se haya tratado o no.
MATERIAL Y MÉTODOS
El estudio se ha realizado a partir de la población infantil de la provincia de Zaragoza (España). Se trata de un estudio observacional, analítico, de cohortes, retrospectivo, con los datos recogidos en una muestra aleatoria de los registros clínicos informatizados de diez cupos de Pediatría de Atención Primaria. Aleatoriamente (un funcionario que desconocía el estudio, mediante lista de números aleatorios) se escogieron las poblaciones pediátricas asignadas a cinco cupos pediátricos que los años 2012 y 2013 disponían de TRDA como herramienta diagnóstica en la consulta y otros cinco asignadas a pediatras que no disponían del test. Dos poblaciones eran rurales y ocho urbanas. La historia clínica en el servicio público de salud de Aragón (a la que pertenece la ciudad de Zaragoza, España) está informatizada, de manera que se puede acceder a los episodios clínicos de cada paciente, sea cual sea el estamento sanitario público que le atendió (Atención Primaria, hospitales, servicios de urgencias…). Esto permite recabar información de los diferentes episodios e incluso posibilita valorar la evolución, lo que ha permitido obtener datos sobre las posibles complicaciones de los procesos investigados.
Se recogió información en los diez cupos de los episodios de FA que cumplían 3-4 criterios de Centor durante los años 2012 y 2013. La escala de Centor15 puntúa de 0 a 4 según la presencia de los siguientes criterios: fiebre > 38 °C, exudado amigdalar, adenopatías subangulomandibulares protuyentes y ausencia de tos. El programa de historia clínica informatizada disponible (OMI-AP®) codifica los diagnósticos asociados al episodio en función de la Clasificación Internacional de Atención Primaria (CIAP2)20. Se revisaron todos los diagnósticos atendidos por el pediatra titular de cada grupo de pacientes asignados (faringitis/faringoamigdalitis, amigdalitis, infección respiratoria tracto superior; códigos CIAP2 R72, R76 y R74, respectivamente). Se incluyeron para el análisis posterior los episodios de estos diagnósticos que cumplieran tres o cuatro criterios de Centor, que hubieran sido abordados por el pediatra titular de ese cupo y que no pertenecieran a pacientes con alguna patología de base o tratamiento inmunosupresor que condicionase un manejo diferente de la FA. Quedaron excluidos los episodios en los que se justificó la no realización de test diagnóstico (imposibilidad de toma de muestra, tratamiento antibiótico reciente y cardiopatía). Asimismo, se recogieron los diagnósticos registrados en el mes siguiente, que pudieran ser considerados como complicación infecciosa por la ausencia de tratamiento, y los potencialmente secundarios al tratamiento.
Variables principales fueron la prescripción o no de antibioterapia y la presencia o no de complicaciones en el mes siguiente del inicio del episodio valorado. Variables secundarias fueron: sexo, edad, población rural o urbana, test diagnóstico, presencia o ausencia de cada uno de los criterios de Centor, puntuación de Centor, y antibiótico prescrito.
El TRDA disponible fue el mismo para todos los centros. Se trata de un test de técnica inmunocromatográfica en casete (Alere TestPack Strep A®, con sensibilidad del 97,6% [IC 95: 93,1 a 99,5] y especificidad del 98,4% [IC 95: 95,9 a 99,6], según datos facilitados por el fabricante), realizado a partir del hisopado adecuado de amígdalas y faringe. Cuando se precisó cultivo, se enviaron las muestras desde los centros de Atención Primaria en condiciones y medio de transporte adecuadas para práctica de cultivo tradicional en dos centros hospitalarios (laboratorios de Microbiología del Hospital Universitario Miguel Servet y del Hospital Royo Villanova, Zaragoza, España).
Para el análisis de las variables, de las cualitativas se calcularon las frecuencias en porcentajes, con sus IC 95. Para las cuantitativas se calcularon las medidas de tendencia central y de dispersión en función de que cumplieran los criterios de normalidad. Se realizó el test de Kruskal-Wallis para comprobar si había diferencias entre las medianas de la edad de los diferentes cupos, al comprobar que la variable edad no seguía una distribución normal. Para la variable utilización de antibiótico entre los episodios en los que se realiza test diagnóstico y los que no, se calcularon el riesgo relativo (RR) y la reducción absoluta de riesgo (RAR) con sus IC 95. También se calculó el RR de complicaciones infecciosas inmediatas (en el primer mes tras el diagnóstico del episodio), potencialmente relacionadas con el tratamiento antibiótico o su ausencia, en tratados y no tratados.
El estudio formó parte del proyecto “Actualización y evaluación del protocolo de faringoamigdalitis aguda en la edad pediátrica del sector Zaragoza II”, seleccionado en el año 2014 como uno de los Programas de Apoyo a las Iniciativas de Mejora de la Calidad en Salud (proyecto número 314) del Servicio Aragonés de Salud (Servicio de Salud Pública de Aragón, España). Para su aceptación, superó los filtros éticos exigidos (autorización para la obtención retrospectiva de datos de los registros informatizados, y compromiso de la debida anonimización que hiciera imposible identificar a los pacientes o a los profesionales titulares de las poblaciones pediátricas revisadas). Así mismo el Director de Atención Primaria del Servicio Aragonés de Salud firmó una autorización expresa para la extracción retrospectiva de datos de las historias clínicas informatizadas.
RESULTADOS
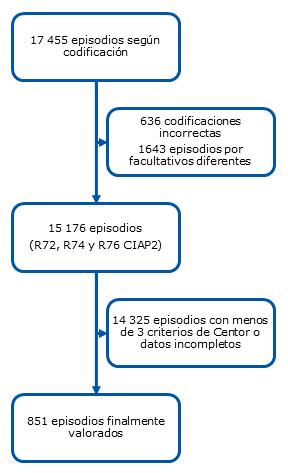
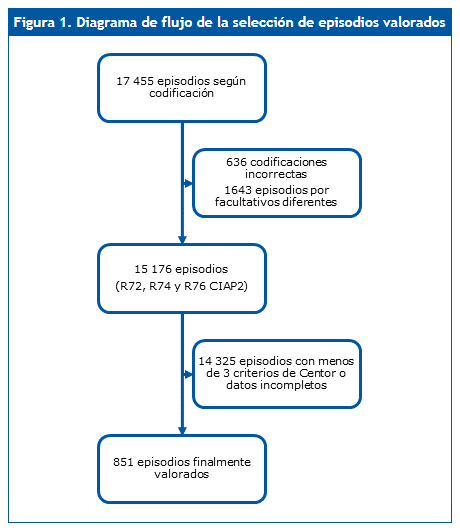
Tras la revisión de 17 455 episodios correspondientes a las codificaciones antes descritas en los diez cupos, 851 episodios cumplieron los criterios válidos para el análisis (Fig. 1). Las aportaciones de episodios de cada uno de los cupos oscilaron desde 39 hasta 163. En uno de los cupos, el pediatra disponía de TRDA pero no lo utilizaba. En total, los centros que utilizaban TRDA aportaron 435 casos, y los que no 416 (Tabla 1).
| Figura 1. Diagrama de flujo de la selección de episodios valorados |
|---|
 |
| Tabla 1. Principales características de los diferentes cupos analizados en función de la utilización del test rápido de antígeno estreptocócico (TRDA) | |||||
|---|---|---|---|---|---|
| Cupo | Episodios Centor 3-4 | Mediana edad (RIC) | Confirmación diagnóstica | Tratamiento antibiótico | Complicaciones* |
| 1 | 52 | 8,75 años (5,17 a 9,94) |
96%a | 54% | 12% |
| 2 | 94 | 5,72 años (3,58 a 9,23) |
86%a | 47% | 18% |
| 3 | 107 | 6,27 años (4,56 a 8,72) |
73%a | 65% | 10% |
| 4 | 163 | 7,38 años (4,50 a 9,69) |
70%a | 74% | 6% |
| 5 | 40 | 3,58 años (1,44 a 8,10) |
0%b | 97% | 10% |
| 6 | 39 | 4,61 años (2,74 a 6,53) |
0%c | 97% | 3% |
| 7 | 101 | 6,17 años (3,79 a 7,79) |
11%c | 82% | 10% |
| 8 | 114 | 6,19 años (4,28 a 8,98) |
8%c | 98% | 18% |
| 9 | 72 | 6,38 años (4,67 a 8,57 |
51%c | 83% | 14% |
| 10 | 69 | 7,91 años (3,69 a 8,77) |
0%c | 100% | 7% |
| Total | 851 | 6,38 años (4,08 a 8,99) |
45% | 78% | 11% |

En global, no se realizó test diagnóstico en 471 casos (55,4%). En los centros que disponían del test y lo utilizaban, se realizó una prueba diagnóstica (TRDA) en el 78% de episodios con 3-4 criterios de Centor, mientras que en los que no disponían o no utilizaban test rápido se practicó estudio etiológico (cultivo) en el 12,4% de casos. Del total de casos en los que se practicó prueba diagnóstica (378) un 51,6% fueron positivos a Streptococcus pyogenes. Del total de TRDA negativos en mayores de tres años, solamente uno de cada tres se confirmó mediante realización de cultivo posterior. En dos casos de TRDA negativo el cultivo posterior fue positivo, en los 52 restantes TRDA negativos en que se hizo cultivo de confirmación, este resultó negativo.
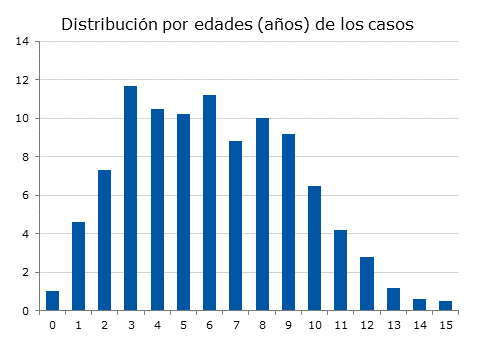
La Fig. 2 muestra la distribución de casos por edades (distribución no normal, test de Kolmogorov-Smirnov: distribución máxima de 0,053; p = 0,017). La mediana de la edad fue de 6,38 años y el rango intercuartílico 4,08 a 8,99 años. Hubo casos desde diez meses de edad a 15 años y 11 meses. El 48% de episodios fueron en mujeres y 52% en varones.
| Figura 2. Distribución porcentual del total de casos estudiados por años de edad |
|---|
 |

La Tabla 1 muestra las principales características de los casos para cada facultativo. No hubo diferencias estadísticamente significativas en la distribución de la edad entre los diferentes cupos (test de Kruskal-Wallis). Los centros que no disponían de TRDA pudieron realizar alguna otra prueba diagnóstica, tal y como sucedió en el caso del facultativo número 9, que solicitó cultivo en la mitad de sus casos. Se incluye también en la tabla el porcentaje de casos en cada centro en los que se realizó prueba diagnóstica, el porcentaje de casos en los que se realizó prescripción antibiótica y el porcentaje de casos en los que se registraron complicaciones infecciosas en el mes siguiente.
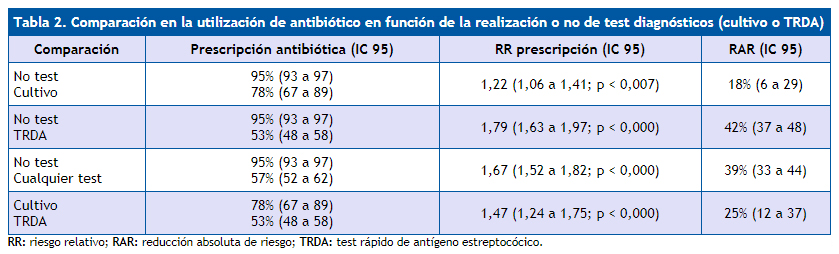
En la Tabla 2 se analizan los porcentajes de prescripción de antibióticos en función de que se realizara algún test diagnóstico, en forma de RR y RAR para cada comparación. Para el total de episodios, la mayor reducción en la prescripción se dio con la utilización de TRDA (RR si no se utilizó test frente a su uso: 1,79 [IC 95: 1,63 a 1,97]; p < 0,000), lo que supone una reducción absoluta de prescripción antibiótica cuando se utiliza el test frente a su no utilización de un 42% (IC 95: 37 a 48). La utilización del cultivo también supuso una reducción significativa en la utilización de antibióticos: RAR del 18% (IC 95: 6 a 29).
| Tabla 2. Comparación en la utilización de antibiótico en función de la realización o no de test diagnósticos (cultivo o TRDA) | |||
|---|---|---|---|
| Comparación | Prescripción antibiótica (IC 95) | RR prescripción (IC 95) | RAR (IC 95) |
| No test Cultivo |
95% (93 a 97) 78% (67 a 89) |
1,22 (1,06 a 1,41; p < 0,007) | 18% (6 a 29) |
| No test TRDA |
95% (93 a 97) 53% (48 a 58) |
1,79 (1,63 a 1,97; p < 0,000) | 42% (37 a 48) |
| No test Cualquier test |
95% (93 a 97) 57% (52 a 62) |
1,67 (1,52 a 1,82; p < 0,000) | 39% (33 a 44) |
| Cultivo TRDA |
78% (67 a 89) 53% (48 a 58) |
1,47 (1,24 a 1,75; p < 0,000) | 25% (12 a 37) |
En un análisis más próximo a la realidad de cada profesional, se compararon los cupos que no disponían o no utilizaban TRDA y los que sí lo tenían y utilizaban (seis cupos frente a cuatro). El porcentaje de prescripción fue del 92% entre los primeros (IC 95: 90 a 95) y del 63% entre los segundos (IC 95: 59 a 68); RR: 1,46 (IC 95: 1,35 a 1,58; p < 0,000); RAR: 29% (IC 95: 24 a 34).
Del total de casos con TRDA negativo (160), fueron tratados con antibiótico ocho (5%). Del total de casos con cultivo negativo (22), 13 recibieron antibiótico (59%), en la mayoría porque se instauró a la espera del resultado y al conocer este con bastante retraso, no se suspendió.
Hubo efectos adversos relacionados con el tratamiento antibiótico en el 2% de los casos tratados (la mayoría digestivos).
Se produjeron procesos infecciosos en el mes siguiente al diagnóstico potencialmente relacionados con tratar o dejar sin tratar el episodio en el 12% de los que recibieron antibioterapia (IC 95: 10 a 15), y en el 8% de los que no la recibieron (IC 95: 4 a 12). El riesgo fue mayor en el grupo tratado, aunque sin significación estadística: RR de 1,49 (IC 95: 0,88 a 2,52; p = 0,178).
La prescripción de penicilina V potásica (PCN V) y amoxicilina supuso el 93% de prescripciones antibióticas (42 y 51% respectivamente). Cuando se utilizó test diagnóstico, fue significativamente más probable recetar PCN V que amoxicilina (RR: 1,30; IC 95: 1,10 a 1,55; p = 0,004). Se prescribió un antibiótico considerado inadecuado (injustificadamente diferente a PCN V, amoxicilina o macrólido) en el 5% de episodios en los que no se hizo prueba diagnóstica frente al 3% de episodios en los que se hizo TRDA: RR 1,86 (IC 95: 0,72 a 4,79; p = 0,271).
DISCUSIÓN
Son múltiples los estudios que se han llevado a cabo sobre la utilidad diagnóstica de los TRDA en las consultas de Pediatría21-24. Por ello, cada vez hay más consenso entre las guías de práctica clínica en recomendar su utilización en pacientes seleccionados mediante unos mínimos criterios clínicos, y solamente tratar con antibioterapia a aquellos con resultado positivo1-8,25. Sin embargo, son muy pocas las investigaciones que se han publicado sobre la utilidad del test en la práctica clínica real.
Sabemos que cuando no se aplican pruebas diagnósticas en la FA en niños, la tendencia a la prescripción de antibióticos es muy elevada, tanto como de un 70-90%18,26,27, cifra injustificada si tenemos en cuenta que la probabilidad de etiología bacteriana es, a esta edad, de aproximadamente un 35%28. Los TRDA son herramientas útiles a la cabecera del enfermo, que han permitido precisar el diagnóstico en esta entidad y que han demostrado efectividad para mejorar la adecuación terapéutica. Aun con la limitación de no distinguir entre el estado de portador y el paciente enfermo (tampoco lo hace el cultivo tradicional), se ha estimado que un resultado positivo en pacientes con criterios clínicos favorables al diagnóstico puede ofrecer una probabilidad posprueba de hasta el 96%24.
Los escasos estudios que han valorado la utilidad del test en la práctica clínica en niños ofrecen cifras muy importantes en la reducción de prescripción antibiótica. Ya comentado, el de Ayanruoh, en un Servicio de Urgencias, estima una reducción del 50% en la prescripción cuando se utiliza el test17. Maltezou, en niños de Grecia, constata una reducción del 44%27 en un estudio de validación del TRDA. En España no hay estudios en niños de utilización del test en la práctica real: De la Flor hace una estimación de la reducción del tratamiento antibiótico de un 54,5% en función de los resultados obtenidos al aplicar el test, pero no sobre la práctica clínica real19; Contessotto calcula en un 50% la reducción de prescripción comparando dos estudios29,30 y Regueras muestra que en niños con sospecha de FAS la utilización del test disminuye la prescripción en un 29,5% de casos31. Cohen, en una revisión reciente sobre este tema que incluye dos de los estudios comentados17,27, valora en un 30% la reducción en el uso de antibiótico en estas entidades si se utiliza el test32.
En nuestra serie, si comparamos los datos globales entre los episodios en los que se usó el TRDA y los que no se hizo prueba diagnóstica, la reducción en la prescripción fue del 42%, marcando una diferencia importante con el cultivo, ya que en los casos en los que se había realizado solo este, la disminución en el uso de antibióticos fue bastante menor (18%). No obstante, más representativo de la realidad parece comparar lo que realmente sucedió entre los profesionales que realizaban test (prescripción antibiótica en el 63% de episodios) y los que no (92% de prescripciones), con una reducción en este caso de la prescripción de un 29%. Esta cifra se aproxima más a la serie de Linder18, o a los resultados que sintetiza Cohen32, y probablemente sea porque estamos ante pacientes preseleccionados por cumplir tres o cuatro criterios de Centor, en los que la prevalencia es mayor. Es posible que el ahorro en la prescripción fuese superior si el test se aplicase a pacientes con menos criterios de Centor, pero, por el contrario, el gasto en el test sería mayor y habría que considerar que la sensibilidad del test decrece cuando hay menos de tres criterios33-36. En una reciente publicación sobre datos de niños atendidos en Urgencias de un hospital madrileño, el uso del test parece esencial para lograr una mejor adecuación a las recomendaciones de las principales guías37.
Un aspecto relevante en esta revisión ha sido que nos ha permitido comprobar que no hay más complicaciones infecciosas en los días siguientes al episodio en los casos no tratados. Incluso el riesgo fue menor en los que no recibieron antibioterapia frente a los que sí la recibieron (el 8 frente a 12% de casos, respectivamente), aunque sin significación estadística.
Como fortalezas del estudio, pensamos que, al utilizar los registros clínicos, el estudio desvela lo que se hace realmente en la clínica. En este caso, además, la posibilidad de seguir la evolución de cada paciente e incluso de valorar los efectos secundarios del tratamiento o las infecciones posteriores al existir una historia clínica unificada en nuestro sistema de salud, permite atenuar los sesgos de información y de memoria.
Limitaciones de nuestro estudio son las subyacentes a un estudio realizado de forma retrospectiva sobre registros clínicos (en este caso informatizados). En general, la mayoría de datos principales se registraron, pero al no existir un registro específico para los síntomas y signos clínicos, existe un sesgo en la recogida de información cometido por parte del clínico que completa el registro, tendiendo a incluir el hallazgo que sí existe, pero con mayor probabilidad de no hacer constar el que no existe. En la historia clínica informatizada concreta, los síntomas y signos de la enfermedad diagnosticada no tienen una plantilla específica que los incluya, dejando a cada facultativo que los registre de forma libre, lo que puede determinar sesgos de detección.
CONCLUSIONES
El estudio confirma que, en la práctica clínica en Atención Primaria, el uso de TRDA supone una importante reducción en la prescripción de antibióticos en los procesos de FA pediátrica. Esta mejor adecuación en el abordaje de la FAS pediátrica permite disminuir costes directos y previene la aparición de resistencias, principalmente a otras bacterias que tan frecuentemente colonizan la nasofaringe de los niños y que son sometidas a presión antibiótica en cada tratamiento. Además, parece que la no realización de tratamiento antibiótico no deriva en incremento de complicaciones de tipo infeccioso inmediatas al episodio.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
FINANCIACIÓN
El soporte técnico para las historias clínicas informatizadas de los pacientes y los centros de atención sanitaria pertenecen al Servicio Aragonés de Salud, que autorizó, a través de su director de Atención Primaria, la realización de esta investigación. El resto del trabajo no ha requerido financiación, pero sí la generosa colaboración de los firmantes del artículo.
ABREVIATURAS
CIAP: Clasificación Internacional de Atención Primaria • FA: faringoamigdalitis • FAS: faringoamigdalitis estreptocócicas • IC 95: intervalo de confianza del 95% • PCN V: penicilina V potásica • RAR: reducción absoluta de riesgo • RR: riesgo relativo • TRDA: test rápidos de detección de antígeno estreptocócico.
BIBLIOGRAFÍA
- Management of the individual with GAS pharyngitis. Group A Streptococcal Sore Throat Management Guideline. En: Heart Foundation of New Zealand [en línea] [consultado el 21/11/2017]. Disponible en www.ttophs.govt.nz/vdb/document/1056
- Snellman L, Adams W, Anderson G, Godfrey A, Gravley A, Johnson K, et al. Diagnosis and treatment of respiratory illness in children and adults. En: Agency for Healthcare Research and Quality [en línea] [consultado el 21/11/2017]. Disponible en www.guideline.gov/summaries/summary/43792/diagnosis-and-treatment-of-respiratory-illness-in-children-and-adults
- Michigan Medicine Quality Departament. Guidelines for Clinical Care Ambulatory. Pharyngitis. En: Michigan Quality Improvement Consortium [en línea] [consultado el 21/11/2017]. Disponible en www.med.umich.edu/1info/FHP/practiceguides/pharyngitis/pharyn.pdf
- Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-82.
- Chiappini E, Principi N, Mansi N, Serra A, De Masi S, Camaioni A, et al. Management of acute pharyngitis in children: summary of the Italian National Institute of Health guidelines. Clin Ther. 2012;34:1442-58.
- ESCMID Sore Throat Guideline Group, Pelucchi C, Grigoryan L, Galeone C, Esposito S, Huovinen P, et al. Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18:1-28.
- Chiappini E, Regoli M, Bonsignori F, Sollai S, Parretti A, Galli L, et al. Analysis of different recommendations from international guidelines for the management of acute pharyngitis in adults and children. Clin Ther. 2011;33:48-58.
- Gerber MA, Baltimore RS, Eaton CB, Gewitz M, Rowley AH, Shulman ST, et al. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics. Circulation. 2009;119:1541-51.
- Management of sore throat and indications for tonsillectomy. A national clinical guideline. En: SIGN Scottish Intercollegiate Guidelines Network [en línea] [consultado el 21/11/2017]. Disponible en www.sign.ac.uk/assets/sign117.pdf
- NICE Short Clinical Guidelines Technical Team (2008). Respiratory tract infections –antibiotic prescribing. Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. En: National Institute for Health and Clinical Excellence [en línea] [consultado el 21/11/2017]. Disponible en www.nice.org.uk/guidance/cg69/resources/respiratory-tract-infections-selflimiting-prescribing-antibiotics-975576354757
- Cohen JF, Cohen R, Levy C, Thollot F, Benani M, Bidet P, et al. Selective testing strategies for diagnosing group A streptococcal infection in children with pharyngitis: a systematic review and prospective multicentre external validation study. CMAJ. 2015;187:23-32.
- Le Marechal F, Martinot A, Duhamel A, Pruvost I, Dubos F. Streptococcal pharyngitis in children: a meta-analysis of clinical decision rules and their clinical variables. BMJ Open. 2013;3. pii: e001482.
- Shaikh N, Swaminathan N, Hooper EG. Accuracy and precision of the signs and symptoms of streptococcal pharyngitis in children: a systematic review. J Pediatr. 2012;160:487-93.
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172:847-52.
- Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-46.
- McIsaac WJ, Kellner JD, Aufricht P, Vanjaka A, Low DE. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA. 2004;291:1587-95. Erratum in: JAMA. 2005;294:2700.
- Ayanruoh S, Waseem M, Quee F, Humphrey A, Reynolds T. Impact of rapid streptococcal test on antibiotic use in a pediatric emergency department. Pediatr Emerg Care. 2009;25:748-50.
- Linder JA, Bates DW, Lee GM, Finkelstein JA. Antibiotic treatment of children with sore throat. JAMA. 2005;294:2315-22.
- De la Flor J, Parellada N. Utilització sistemàtica de tests de diagnòstic ràpid en una consulta de Pediatría d’atenció primària. Pediatr Catalana. 2009;69:75-84.
- Comité Internacional de Clasificación de la WONCA. Clasificación Internacional de la Atención Primaria segunda edición. CIAP-2. Barcelona: Masson; 1999.
- Ruiz-Aragón J, Rodríguez R, Molina JM. Evaluación de los métodos rápidos para la detección de Streptococcus pyogenes. Revisión sistemática y metanálisis. An Pediatr (Barc). 2010;72:391-402.
- Lean WL, Arnup S, Danchin M, Steer AC. Rapid diagnostic tests for group A streptococcal pharyngitis: a meta-analysis. Pediatrics. 2014;134:771-81.
- Stewart EH, Davis B, Clemans-Taylor BL, Littenberg B, Estrada CA, Centor RM. Rapid antigen group A streptococcus test to diagnose pharyngitis: a systematic review and meta-analysis. PLoS One. 2014;9:e111727.
- Esparza Olcina MJ, García Vera C. ¿Qué utilidad tiene el test rápido de detección del estreptococo en la consulta de Pediatría? Evid Pediatr. 2016;12:3.
- Van Brusselen D, Vlieghe E, Schelstraete P, De Meulder F, Vandeputte C, Garmyn K, et al. Streptococcal pharyngitis in children: to treat or not to treat? Eur J Pediatr. 2014;173:1275-83.
- Ochoa C, Vilela M, Cueto M, Eiros JM, Inglada L; Grupo Español de Estudio de los Tratamientos Antibióticos. Adecuación del tratamiento de la faringoamigdalitis aguda a la evidencia científica. An Pediatr (Barc). 2003;59:31-40.
- Maltezou HC, Tsagris V, Antoniadou A, Galani L, Douros C, Katsarolis I, et al. Evaluation of a rapid antigen detection test in the diagnosis of streptococcal pharyngitis in children and its impact on antibiotic prescription. J Antimicrob Chemother. 2008;62:1407-12.
- Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010;126:e557-64.
- Contessotto C, Cámara M, Avilés MJ, Ojeda JM, Cascales I, Rodríguez F. Empleo racional de los antibióticos en Pediatría: impacto de la aplicación de un test rápido de detección de estreptococo beta-hemolítico del grupo A en la faringoamigdalitis aguda. An Esp Pediatr. 2000;52:212-9.
- Contessotto C, Andreu J, Gómez M, Cascales I, Gutiérrez JD, Valverde J, et al. Sobreutilización de antibióticos en Pediatría de base. ¿Malpraxis frecuente? An Esp Pediatr. 1996;84:50.
- Regueras G, Santos PM, Villa L, Pérez A, Arbesú E, Barreiro L, et al. Utilidad de una técnica antigénica rápida en el diagnóstico de la faringoamigdalitis por Streptococcus pyogenes. An Pediatr (Barc). 2012;77:193-9.
- Cohen J, Levy C, Chalumeau M, Bidet P, Cohen R. Rapid antigen detection tests for group A streptococcus in children with pharyngitis. Arch Pediatr. 2014;21:S78-83.
- García Vera C, Afayate Miguélez S, Bengoa Gorosabel A, Cocho Gómez P. Test de detección rápida en infecciones ORL y respiratorias: utilidad en la consulta. Rev Pediatr Aten Primaria Supl. 2014;23:49-59.
- Edmonson MB, Farwell KR. Relationship between the clinical likelihood of group A streptococcal pharyngitis and the sensitivity of a rapid antigen-detection test in a pediatric practice. Pediatrics. 2005;115:280-5.
- Hall MC, Kieke B, Gonzales R, Belongia EA. Spectrum bias of a rapid antigen detection test for group A beta-hemolytic streptococcal pharyngitis in a pediatric population. Pediatrics. 2004;114:182-6.
- Cohen JF, Chalumeau M, Levy C, Bidet P, Benani M, Koskas M, et al. Effect of clinical spectrum, inoculum size and physician characteristics on sensitivity of a rapid antigen detection test for group A streptococcal pharyngitis. Eur J Clin Microbiol Infect Dis. 2013;32:787-93.
- Piñeiro Pérez R, Hernández Martín D, Carro Rodríguez MA, Casado Verrier E, Reques Cosme R, Carabaño Aguado I. Adecuación del diagnóstico y tratamiento de la faringoamigdalitis aguda a las guías actuales. Rev Pediatr Aten Primaria. 2016;18:317-24.