

Vol. 19 - Num. 76
Original Papers
Rapid streptococcal antigen detection test in pharyngitis: impact in antibiotic use
César García Veraa, Mercedes Cemeli Canob, Esther María Peralta Rufasc, Elvira Romeo Lázarod, María Belén Pina Gadeae
aPediatra. CS José Ramon Muñoz Fernández. Zaragoza. España.
bPediatra. CS Valdespartera-Montecanal. Zaragoza. España.
cMIR-Pediatría. Hospital Universitario Infantil Miguel Servet. Zaragoza. España.
dPediatra. CS San José Norte. Zaragoza. España.
eFarmacéutica de Atención Primaria. Sector Zaragoza II. Servicio Aragonés de Salud. Zaragoza. España.
Correspondence: C García. E-mail: cgarciavera@gmail.com
Reference of this article: García Vera C, Cemeli Cano M, Peralta Rufas EM, Romeo Lázaro E, Pina Gadea MB. Rapid streptococcal antigen detection test in pharyngitis: impact in antibiotic use. Rev Pediatr Aten Primaria. 2017;19:345:54.
Published in Internet: 23-11-2017 - Visits: 27593
Abstract
Objective: to investigate the impact of rapid streptococcal antigen detection test use on antibiotic prescription in children.
Patients and methods: observational, retrospective cohort study, based on the computer data from 10 pediatric health centre cohorts in Zaragoza (Spain) from 2012 and 2013. The prescription of antibiotics and complications in the ensuing month are compared according to whether a rapid antigen diagnostic test was carried out or not.
Results: 851 cases met the inclusion criteria (3-4 Centor criteria) from a pre-selection of 17,455. In those cases where the rapid antigen test was performed a reduction in prescriptions of 42% (absolute risk reduction 42%; 95% confidence interval [95 CI]: 37 to 48; p < 0.001) was observed. On comparing the approach among pediatricians who had the test available (4) and those who did not (6) a decrease of 29% (absolute risk reduction 29%; 95 CI: 24 to 34; p < 0.001) was noted. Ensuing infectious complications did not vary (12% in treated, 8% in untreated; relative risk 1.49; CI 95: 0.88 to 2.52; p = 0.178). The prescription of penicillin V was significantly more likely than that of amoxicillin when a diagnostic test was used (relative risk 1.30; 95 CI: 1.10 to 1.55; p = 0.004).
Conclusions: in clinical practice the use of the rapid antigen test in pediatric patients pre-selected through clinical criteria was a determining factor in the reduction of the inappropriate use of antibiotics.
Keywords
● Antibiotics ● Child ● Drug evaluation ● Pharyngitis ● Rapid testsINTRODUCTION
When it comes to the management of paediatric pharyngitis in the primary care setting, most recent clinical practice guidelines1-8 recommend that antibiotherapy be restricted to confirmed cases of streptococcal pharyngitis. Although there are a few exceptions that recommend treatment based on the severity of symptoms whether an aetiological diagnosis has been made or not,9,10 all others propose the use of a rapid antigen detection test (RADT) for streptococcus or, should it not be available, traditional culture. This recommendation is usually made on the condition that the patient has met a minimum set of criteria suggestive of a streptococcal aetiology. Thus, the ultimate goal is to initiate antibiotherapy only when the clinical suspicion of streptococcal pharyngitis is confirmed by either RADT or culture.
No sign or symptom of streptococcal pharyngitis in isolation has a high enough positive likelihood ratio to achieve a satisfactory post test-probability.11-13 Consequently, clinical criteria can only be useful in determining which patients are eligible for diagnostic tests, so that they are not performed in all patients presenting with any sign or symptom of pharyngitis. The use of a minimum set of data has been proposed; these data are often grouped in clinical prediction rules, of which the most widely used and validated14 in the paediatric age group are the Centor criteria15 and Centor criteria modified by McIsaac.16
Very few studies, however, have assessed the diagnostic yield of RADTs in preselected patients in everyday clinical practice. In 2009, Ayanruoh published a study of patients that visited the emergency department of a hospital in New York that showed that the introduction of rapid testing was associated with a reduction of approximately 50% in antibiotic prescription in pharyngitis cases.17 Another large population-based study in the United States that used data from the National Ambulatory Medical Care Survey (NAMCS) from 1995 to 2003 found a significant reduction in the proportion of antibiotic prescription associated to the use of diagnostic testing. This study found that in cases with diagnosis codes for pharyngitis, tonsillitis or streptococcal sore throat, antibiotics were prescribed in only 57% of tested children compared to 73% of untested children.18 With the exception of studies focused on diagnostic testing that evaluated different RADTs, few studies have been conducted in primary care settings to assess their actual impact after their introduction in everyday clinical practice. De la Flor estimated a reduction of 54.5% in the prescription of antibiotics in cases of suspected streptococcal pharyngitis when this test was used in the paediatric population of Barcelona.19
The aim of this study was to review electronic health records in order to assess the actual usefulness of RADT in the everyday practice of primary care paediatrics, evaluating its impact on antibiotic use and complications occurring soon after the episode of pharyngitis, based on whether the patient had or not received treatment.
MATERIALS AND METHODS
The study focused on the paediatric population of the province of Zaragoza (Spain). We conducted a retrospective observational analytic cohort study of data collected from the electronic health records corresponding to a random sample of 10 primary care paediatrics caseloads. A civil servant that was not acquainted with the study used a random number list to select the paediatric populations (caseloads) assigned to 5 paediatric clinics with access to RADT as a diagnostic test in 2012 and 2013, and another 5 caseloads managed by paediatricians that did not have access to this test. Two caseloads corresponded to clinics in rural areas and eight to clinics in urban areas. Medical health records in the public health system of the autonomous community of Aragon in Spain (which includes the city of Zaragoza) are kept in an electronic database, so that information on the episodes of disease experienced by each patient can be accessed regardless of the public health setting where the patient was managed (primary care centre, hospital, emergency department…). This allows access to information for different episodes and even assessment of patient outcomes, so we were able to obtain data on the potential complications of the episodes under study.
We collected data from the 10 caseloads for the pharyngitis episodes recorded in 2012 and 2013 that met 3 or 4 Centor criteria. The Centor score15 can range from 0 to 4 based on the presence of the following criteria: fever > 38°C, tonsillar exudate, swollen and tender anterior cervical nodes and absence of cough. In the current regional primary care electronic health records system (OMI-AP®), the diagnoses for each episode of disease are coded according to the International Classification of Primary Care (ICPC-2).20 We reviewed all cases with a relevant diagnosis managed by the paediatrician in charge of each selected caseload (streptococcal sore throat, acute tonsillitis, acute upper respiratory infection; ICPC-2 codes R72, R76 and R74, respectively). In the subsequent analysis, we included the episodes diagnosed with any of these codes that met 3 or 4 Centor criteria, managed by the paediatrician in charge of the caseload, and occurring in patients with no underlying disease or not under immunosuppressive therapy, factors that would require a different approach to the management of pharyngitis. We excluded episodes where there was a justifiable reason to not perform the diagnostic test (collection of a sample was not possible, recent antibiotic treatment or heart disease). We also retrieved diagnoses made in these patients in the month following the episode that could be indicative of an infectious complication due to lack of treatment or a complication resulting from treatment.
The primary variables were prescription of antibiotics or lack thereof, and the presence or absence of complications in the month following the onset of the episode. Secondary variables included sex, age, rural or urban setting, diagnostic test, presence or absence of each of the Centor criteria, Centor score and prescribed antibiotic.
The available RADT was the same in every clinic. It was an immunochromatographic assay in cassette format (Alere TestPack Strep A®, with a sensitivity of 97.6% [95 CI: 93.1 to 99.5] and a specificity of 98.4% [95 CI: 95.9 to 99.6], as reported by the manufacturer), performed on suitable throat swab specimens. When culture was required, samples were submitted from primary care centres in the appropriate media and under appropriate conditions for performance of traditional culture in one of two possible hospitals (microbiology laboratories of the Hospital Universitario Miguel Servet and the Hospital Royo Villanova, Zaragoza, Spain).
We summarised qualitative variables as percentages with their corresponding 95 CI, and quantitative variables using appropriate measures of central tendency and dispersion based on whether or not they followed a normal distribution. We used the Kruskal-Wallis test to check whether there were significant differences in median age between caseloads, as the age variable did not follow a normal distribution. To analyse the use of antibiotics comparing episodes where a diagnostic test was used versus episodes where it was not, we calculated the relative risk (RR) and the absolute risk reduction (ARR) with their 95 CIs. We also calculated the RR of immediate infectious complications (defined as those occurring within one month from diagnosis) potentially associated with the use or lack of use of antibiotherapy in treated and untreated patients.
This study was conducted in the framework of the project “Evaluation and Updating of the protocol for the management of paediatric acute pharyngitis in the Zaragoza II health district,” which was selected in 2014 for one of the grant programmes of the public health system of Aragon (Department of Health of Aragon, Spain) to support initiatives for improving health care quality (project No. 314). To participate in this programme, the project met the necessary ethical criteria (consent for retrospective electronic data collection, and anonymization of data to ensure the confidentiality of the patients and providers included in the reviewed caseloads). The Director of Primary Care of the Public Health System of Aragon also signed an express authorisation for the retrospective extraction of data from the electronic health records database.
RESULTS
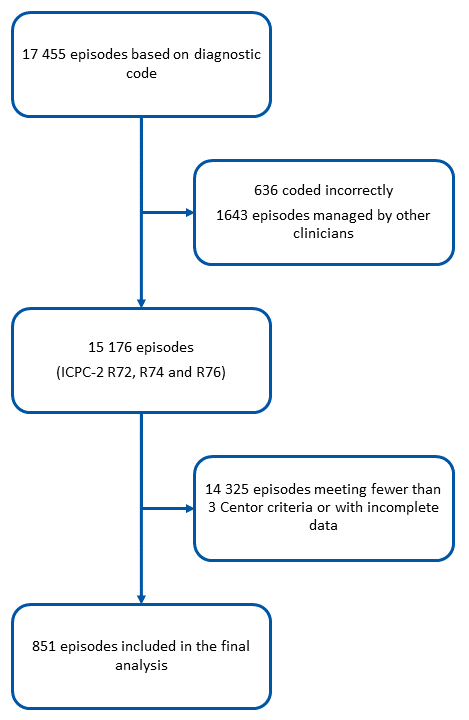
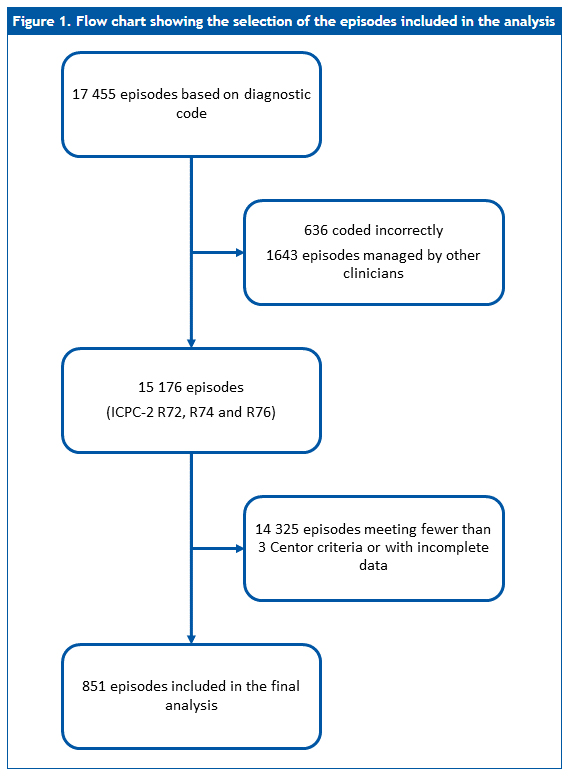
After reviewing 17 455 episodes corresponding to the previously listed codes in the 10 caseloads, we found 851 episodes that met the criteria for inclusion in the analysis (Figure 1). The episodes contributed by each caseload ranged from 39 to 163. In one of the caseloads, the paediatrician in charge had access to the RADT but did not use it. In total, the clinics that used the RADT contributed 435 cases, and the clinics that did not contributed 416 (Table 1).
| Figure 1. Flow chart showing the selection of the episodes included in the analysis |
|---|
 |
|
Table 1. Main characteristics of the different caseloads under study based on the use of the rapid antigen detection test (RADT) for streptococcus |
|||||
|---|---|---|---|---|---|
| Caseload | Episodes meeting 3-4 Centor criteria | Median age (IQR)* | Confirmed diagnosis | Antibiotic treatment | Complications** |
| 1 | 52 | 8.75 years (5.17 to 9.94) |
96%a | 54% | 12% |
| 2 | 94 | 5.72 years (3.58 to 9.23) |
86%a | 47% | 18% |
| 3 | 107 | 6.27 years (4.56 to 8.72) |
73%a | 65% | 10% |
| 4 | 163 | 7.38 years (4.50 to 9.69) |
70%a | 74% | 6% |
| 5 | 40 | 3.58 years (1.44 to 8.10) |
0%b | 97% | 10% |
| 6 | 39 | 4.61 years (2.74 to 6.53) |
0%c | 97% | 3% |
| 7 | 101 | 6.17 years (3.79 to 7.79) |
11%c | 82% | 10% |
| 8 | 114 | 6.19 years (4.28 to 8.98) |
8%c | 98% | 18% |
| 9 | 72 | 6.38 years (4.67 to 8.57 |
51%c | 83% | 14% |
| 10 | 69 | 7.91 years (3.69 to 8.77) |
0%c | 100% | 7% |
| Total | 851 | 6.38 years (4.08 to 8.99) |
45% | 78% | 11% |
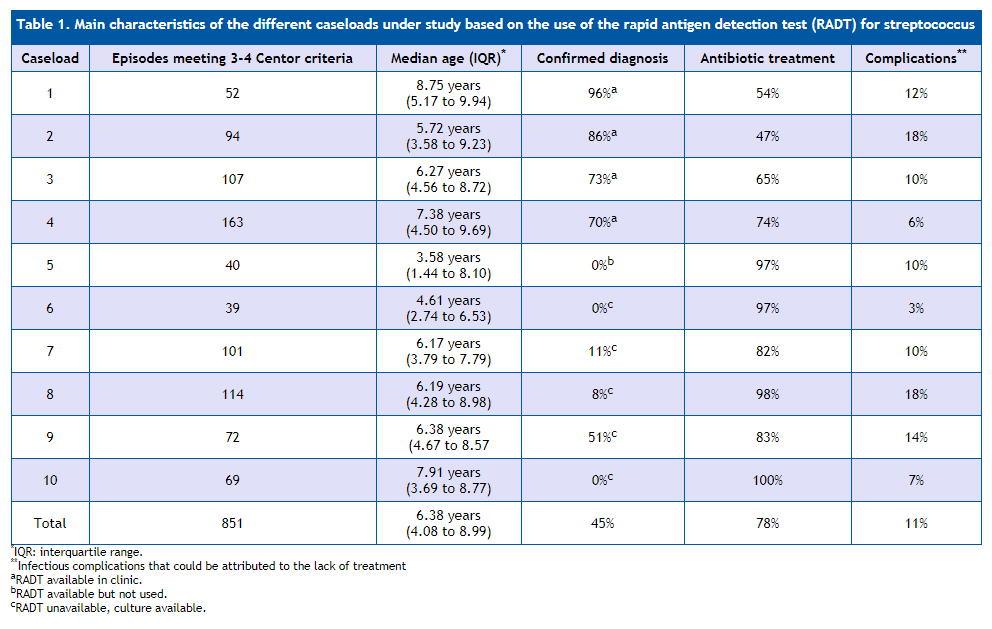
In the overall sample, no diagnostic test was performed in 471 cases (55.4%). In the subset of clinics where the test was available and used, a diagnostic test (RADT) was performed in 78% of episodes that met 3-4 Centor criteria, while in the clinics that did not have access or did not use the rapid test, culture was performed in 12.4% of episodes meeting the criteria. Of the total cases where a diagnostic test was performed (378), the results were positive for Streptococcus pyogenes in 51.6%. Out of all cases where the results of the RADT were negative, a culture was subsequently performed for confirmation in only one third. Among the total cases with negative RADT results where culture was performed for confirmation, the results of culture were positive in 2 and negative in the remaining 52.
Figure 2 shows the age distribution of the included cases (non-normal distribution, Kolmogorov-Smirnov test: maximum deviation of 0.053; P = .017). The median age was 6.38 years and the interquartile range 4.08 to 8.99 years. Cases occurred in patients aged 10 months to 15 years and 11 months. Forty-eight percent occurred in girls and 52% in boys.
| Figure 2. Percent distribution by years of age of the total cases under study |
|---|
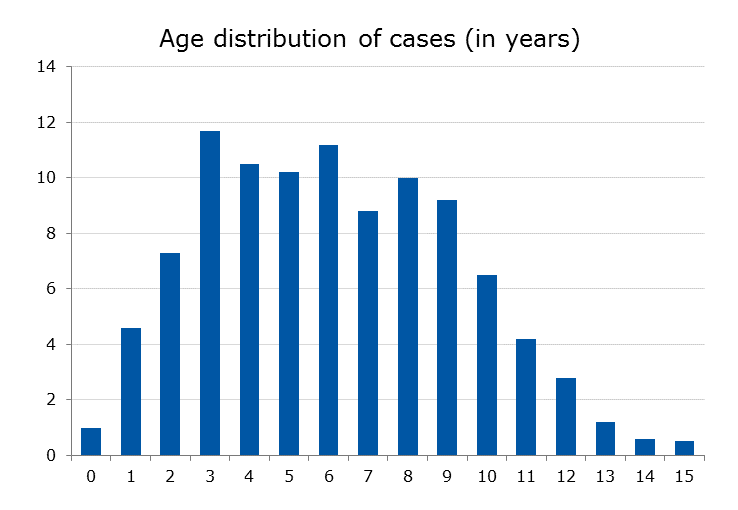 |
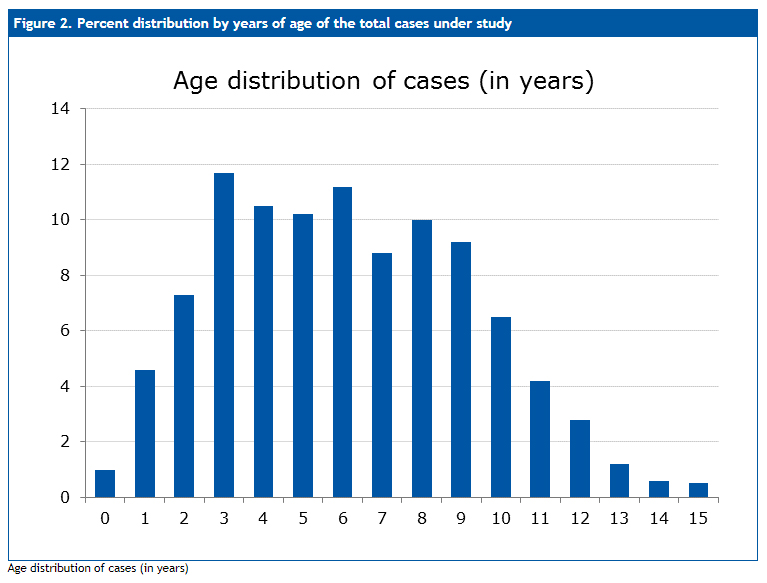
Table 1 shows the main characteristics of the cases managed by each paediatrician. There were no statistically significant differences in age distribution between caseloads (Kruskal-Wallis test). The clinics that did not have access to the RADT had access to alternative diagnostic tests, as was the case of paediatrician no. 9, who ordered a culture in half of the cases. The table also includes the percentage of cases in each clinic where a diagnostic test was performed, the percentage of cases where antibiotherapy was prescribed, and the percentage of cases in which infectious complications were documented in the month that followed diagnosis.
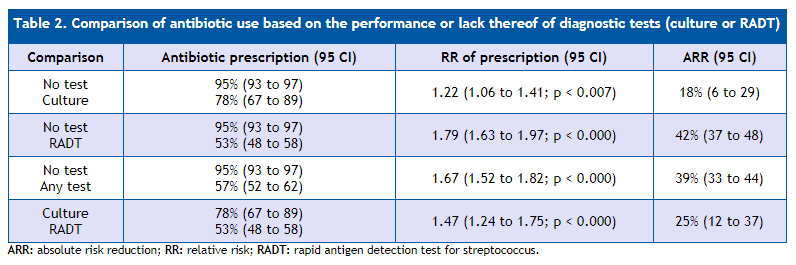
Table 2 analyses the proportion of antibiotic prescription based on whether patients did or did not undergo diagnostic testing, expressed as the RR and ARR for each comparison. Overall, we found the greatest reduction in antibiotic prescription in episodes where the RADT had been used (RR for not using vs using the test: 1.79 [95 CI: 1.63 to 1.97]; P < .000), which amounts to an absolute reduction of antibiotic prescription of 42% when the test is used compared to when it is not (95 CI: 37 to 48). The use of culture was also associated with a significant reduction in antibiotic use: ARR of 18% (95 CI: 6 to 29).
|
Table 2. Comparison of antibiotic use based on the performance or lack thereof of diagnostic tests (culture or RADT) |
|||
|---|---|---|---|
| Comparison | Antibiotic prescription (95 CI) | RR of prescription (95 CI) | ARR (95 CI) |
| No test Culture |
95% (93 to 97) 78% (67 to 89) |
1.22 (1.06 to 1.41; p < 0.007) | 18% (6 to 29) |
| No test RADT |
95% (93 to 97) 53% (48 to 58) |
1.79 (1.63 to 1.97; p < 0.000) | 42% (37 to 48) |
| No test Any test |
95% (93 to 97) 57% (52 to 62) |
1.67 (1.52 to 1.82; p < 0.000) | 39% (33 to 44) |
| Culture RADT |
78% (67 to 89) 53% (48 to 58) |
1.47 (1.24 to 1.75; p < 0.000) | 25% (12 to 37) |
In an analysis that took into account the specific circumstances of each paediatrician, we compared the caseloads of clinics where the RADT was either unavailable or not used, and those of clinics where the RADT was available and also used (six and four caseloads, respectively). The percentage of cases where antibiotherapy was prescribed was of 92% in the former (95 CI: 90 to 95) compared to 63% in the latter (95 CI: 59 to 68); RR: 1.46 (95 CI: 1.35 to 1.58; P < .000); ARR: 29% (95 CI: 24 to 34).
Of the total cases where the RADT was negative (160), 8 (5%) were treated with antibiotics. Of the total of cases where the culture was negative (22), 13 (59%) were treated with antibiotics, in most cases because empirical treatment was initiated while awaiting the results, and not discontinued due to the long time elapsed until results became available.
Adverse events were reported in 2% of the cases treated with antibiotics (most of them gastrointestinal).
Infectious complications in the month following the diagnosis that may have resulted from antibiotherapy or else from lack of treatment were documented in 12% of cases treated with antibiotics (95 CI: 10 to 15) and 8% of untreated cases (95 CI: 4 to 12). The risk was greater in the treated group, although the difference was not statistically significant: RR of 1.49 (95 CI: 0.88 to 2.52; P = .178).
Penicillin V potassium (PCN VK) and amoxicillin amounted to 93% of antibiotic prescriptions (42% and 51%, respectively). The use of a diagnostic test was associated with a higher probability of PCN VK prescription compared to amoxicillin (RR: 1.30; 95 CI: 1.10 to 1.55; P = .004). An antibiotic that would be considered inappropriate (an unjustified alternative to PCN VK, amoxicillin or a macrolide) was prescribed in 5% of episodes where a diagnostic test was not performed compared to 3% of episodes where a RADT was performed: RR of 1.86 (95 CI: 0.72 to 4.79; P = .271).
DISCUSSION
Many studies have assessed the usefulness of RADTs in paediatrics clinics for the purpose of diagnosis.21-24 As a consequence, there is an increasing agreement among clinical practice guidelines in recommending their use in patients previously selected based on a minimum set of clinical criteria and advising that antibiotherapy be restricted to patients with positive results.1-8,25 However, few studies have assessed the actual usefulness of rapid testing in everyday clinical practice.
We know that when diagnostic tests are not used in paediatric cases of pharyngitis, there is a high probability of antibiotic prescription of up to 70-90%,18,26,27 a proportion that is unwarranted if we consider that the probability of a bacterial aetiology in this age group is approximately 35%.28 Rapid antigen detection tests are useful bedside tools that have allowed a more accurate diagnosis of this disease and proven effective to improve the therapeutic approach. Although they are limited in that they cannot differentiate between carriage and active disease (a limitation that also applies to traditional culture), it is estimated that the post-test probability of a positive result in a patient with clinical criteria suggestive of a streptococcal aetiology may be as high as 96%.24
The few studies that have assessed the usefulness of rapid testing in children in clinical practice have reported significant reductions in antibiotic prescription. The study mentioned above by Ayanruoh, conducted in an emergency department, estimated a 50% reduction in prescription with the use of the test.17 Maltezou, in study conducted in children in Greece to validate the RADT, found a reduction of 44%.27 In Spain, no studies had been performed to assess the use of the test in everyday clinical practice: de la Flor estimated a reduction in antibiotic treatment of 54.5% based on the results obtained with the test, but not on actual clinical practice,19 Contessotto estimated a reduction of 50% by comparing two different studies,29,30 and Regueras showed that in children with suspected streptococcal pharyngitis, use of rapid testing reduced unnecessary prescription by at least 29.5%.31 In a recent review on this subject that included two of the studies mentioned above,17,27 Cohen estimated a 30% reduction in the use of antibiotics associated with the use of the test.32
In our series, the comparison of all episodes where RADT was used versus all episodes where testing was not performed found a 42% reduction in antibiotic prescription in the former, evincing a considerable difference compared to culture, as the reduction of antibiotic prescription in cases where only culture had been used was significantly lower (18%). However, a comparison of the actual figures in clinicians that used the test (prescription in 63% of episodes) versus those who did not (prescription in 92% of episodes) may be more illustrative of the status quo, showing a reduction in prescription with the use of the test of 29%. This percentage is close to the one found in the series published by Linder18 or the results summarised by Cohen,32 and may be due to the test having been performed in preselected patients that met 3 or 4 Centor criteria, in who the actual prevalence is higher. It is possible that the savings in antibiotic prescription would be greater if the test were applied to patients with fewer Centor criteria, but on the other hand the costs associated with testing would be higher, and it would be necessary to consider that the sensitivity is lower in patients meeting fewer than 3 criteria.33-36 A recently published analysis of data on children managed in the emergency department of a hospital in Madrid suggests that the use of the test is essential to improve adherence to the recommendations of the main clinical guidelies.37
A relevant aspect of our review is that it allowed us to ascertain that the incidence of infectious complications in the days following diagnosis was not higher in untreated cases. The risk was actually lower in patients not treated with antibiotics compared to patients that received them (8% versus 12% of cases, respectively), although the difference was not statistically significant.
One of the strengths of the study, in our opinion, is that the use of data from medical records shows what is actually done in everyday clinical practice. In this particular case, it also allowed us to assess the outcomes in each patient and even detect adverse events associated with treatment or subsequent infections, as out public health system has a unified medical records database, which reduces the risk of information and recall bias.
Some of the limitations of our study were those intrinsic to a retrospective review of medical records (in this case, electronic health records). Generally speaking, most of the important data were documented, but since a form specifically designed to document the clinical signs and symptoms was not used, there was a source of bias in the clinicians that entered the data in the records, as usually they record the manifestations that are present, but are less likely to specifically document manifestations that are absent. The health records system used in these clinics does not have a specific template for the documentation of clinical manifestations, which are entered as free text by each clinician, which may have led to detection bias.
CONCLUSIONS
Our study confirms that in everyday clinical practice in primary care, the use of the RADT for streptococcus is associated with a significant reduction in antibiotic prescription in paediatric cases of pharyngitis. This improvement in the appropriate management of streptococcal pharyngitis in the paediatric age group can reduce direct health care costs and prevent the development of antimicrobial resistance, especially in other bacteria that frequently colonise the upper respiratory tract of children and that are subjected to selective pressure with each antibiotic exposure. Furthermore, our data suggest that the lack of antibiotic treatment is not associated with an increase in the incidence of infectious complications in the first weeks after the episode.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
FUNDING
The electronic health records of patients and primary care centres belong to the Department of Health of Aragon, which authorised, through its Primary Care director, the performance of this study. The study did not otherwise require any additional funding, although it did require the generous collaboration of the authors signing this article.
ABBREVIATIONS
ARR: absolute risk reduction • CI: confidence interval • ICPC: International Classification of Primary Care • PCN VK: penicillin V potassium • RADT: rapid antigen detection test • RR: relative risk.
REFERENCES
- Management of the individual with GAS pharyngitis. Group A Streptococcal Sore Throat Management Guideline. In: Heart Foundation of New Zealand [online] [accessed 21/11/2017]. Available at www.ttophs.govt.nz/vdb/document/1056
- Snellman L, Adams W, Anderson G, Godfrey A, Gravley A, Johnson K, et al. Diagnosis and treatment of respiratory illness in children and adults. In: Agency for Healthcare Research and Quality [online] [accessed 21/11/2017]. Available at www.guideline.gov/summaries/summary/43792/diagnosis-and-treatment-of-respiratory-illness-in-children-and-adults
- Michigan Medicine Quality Departament. Guidelines for Clinical Care Ambulatory. Pharyngitis. In: Michigan Quality Improvement Consortium [online] [accessed 21/11/2017]. Available at www.med.umich.edu/1info/FHP/practiceguides/pharyngitis/pharyn.pdf
- Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-82.
- Chiappini E, Principi N, Mansi N, Serra A, De Masi S, Camaioni A, et al. Management of acute pharyngitis in children: summary of the Italian National Institute of Health guidelines. Clin Ther. 2012;34:1442-58.
- ESCMID Sore Throat Guideline Group, Pelucchi C, Grigoryan L, Galeone C, Esposito S, Huovinen P, et al. Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18:1-28.
- Chiappini E, Regoli M, Bonsignori F, Sollai S, Parretti A, Galli L, et al. Analysis of different recommendations from international guidelines for the management of acute pharyngitis in adults and children. Clin Ther. 2011;33:48-58.
- Gerber MA, Baltimore RS, Eaton CB, Gewitz M, Rowley AH, Shulman ST, et al. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics. Circulation. 2009;119:1541-51.
- Management of sore throat and indications for tonsillectomy. A national clinical guideline. In: SIGN Scottish Intercollegiate Guidelines Network [online] [accessed 21/11/2017]. Available at www.sign.ac.uk/assets/sign117.pdf
- NICE Short Clinical Guidelines Technical Team (2008). Respiratory tract infections –antibiotic prescribing. Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. In: National Institute for Health and Clinical Excellence [online] [accessed 21/11/2017]. Available at www.nice.org.uk/guidance/cg69/resources/respiratory-tract-infections-selflimiting-prescribing-antibiotics-975576354757
- Cohen JF, Cohen R, Levy C, Thollot F, Benani M, Bidet P, et al. Selective testing strategies for diagnosing group A streptococcal infection in children with pharyngitis: a systematic review and prospective multicentre external validation study. CMAJ. 2015;187:23-32.
- Le Marechal F, Martinot A, Duhamel A, Pruvost I, Dubos F. Streptococcal pharyngitis in children: a meta-analysis of clinical decision rules and their clinical variables. BMJ Open. 2013;3. pii: e001482.
- Shaikh N, Swaminathan N, Hooper EG. Accuracy and precision of the signs and symptoms of streptococcal pharyngitis in children: a systematic review. J Pediatr. 2012;160:487-93.
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172:847-52.
- Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-46.
- McIsaac WJ, Kellner JD, Aufricht P, Vanjaka A, Low DE. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA. 2004;291:1587-95. Erratum in: JAMA. 2005;294:2700.
- Ayanruoh S, Waseem M, Quee F, Humphrey A, Reynolds T. Impact of rapid streptococcal test on antibiotic use in a pediatric emergency department. Pediatr Emerg Care. 2009;25:748-50.
- Linder JA, Bates DW, Lee GM, Finkelstein JA. Antibiotic treatment of children with sore throat. JAMA. 2005;294:2315-22.
- De la Flor J, Parellada N. Utilització sistemàtica de tests de diagnòstic ràpid en una consulta de Pediatría d’atenció primària. Pediatr Catalana. 2009;69:75-84.
- Comité Internacional de Clasificación de la WONCA. Clasificación Internacional de la Atención Primaria segunda edición. CIAP-2. Barcelona: Masson; 1999.
- Ruiz-Aragón J, Rodríguez R, Molina JM. Evaluación de los métodos rápidos para la detección de Streptococcus pyogenes. Revisión sistemática y metanálisis. An Pediatr (Barc). 2010;72:391-402.
- Lean WL, Arnup S, Danchin M, Steer AC. Rapid diagnostic tests for group A streptococcal pharyngitis: a meta-analysis. Pediatrics. 2014;134:771-81.
- Stewart EH, Davis B, Clemans-Taylor BL, Littenberg B, Estrada CA, Centor RM. Rapid antigen group A streptococcus test to diagnose pharyngitis: a systematic review and meta-analysis. PLoS One. 2014;9:e111727.
- Esparza Olcina MJ, García Vera C. ¿Qué utilidad tiene el test rápido de detección del estreptococo en la consulta de Pediatría? Evid Pediatr. 2016;12:3.
- Van Brusselen D, Vlieghe E, Schelstraete P, De Meulder F, Vandeputte C, Garmyn K, et al. Streptococcal pharyngitis in children: to treat or not to treat? Eur J Pediatr. 2014;173:1275-83.
- Ochoa C, Vilela M, Cueto M, Eiros JM, Inglada L; Grupo Español de Estudio de los Tratamientos Antibióticos. Adecuación del tratamiento de la faringoamigdalitis aguda a la evidencia científica. An Pediatr (Barc). 2003;59:31-40.
- Maltezou HC, Tsagris V, Antoniadou A, Galani L, Douros C, Katsarolis I, et al. Evaluation of a rapid antigen detection test in the diagnosis of streptococcal pharyngitis in children and its impact on antibiotic prescription. J Antimicrob Chemother. 2008;62:1407-12.
- Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010;126:e557-64.
- Contessotto C, Cámara M, Avilés MJ, Ojeda JM, Cascales I, Rodríguez F. Empleo racional de los antibióticos en Pediatría: impacto de la aplicación de un test rápido de detección de estreptococo beta-hemolítico del grupo A en la faringoamigdalitis aguda. An Esp Pediatr. 2000;52:212-9.
- Contessotto C, Andreu J, Gómez M, Cascales I, Gutiérrez JD, Valverde J, et al. Sobreutilización de antibióticos en Pediatría de base. ¿Malpraxis frecuente? An Esp Pediatr. 1996;84:50.
- Regueras G, Santos PM, Villa L, Pérez A, Arbesú E, Barreiro L, et al. Utilidad de una técnica antigénica rápida en el diagnóstico de la faringoamigdalitis por Streptococcus pyogenes. An Pediatr (Barc). 2012;77:193-9.
- Cohen J, Levy C, Chalumeau M, Bidet P, Cohen R. Rapid antigen detection tests for group A streptococcus in children with pharyngitis. Arch Pediatr. 2014;21 Suppl 2:S78-83.
- García Vera C, Afayate Miguélez S, Bengoa Gorosabel A, Cocho Gómez P. Test de detección rápida en infecciones ORL y respiratorias: utilidad en la consulta. Rev Pediatr Aten Primaria Supl. 2014;23:49-59.
- Edmonson MB, Farwell KR. Relationship between the clinical likelihood of group A streptococcal pharyngitis and the sensitivity of a rapid antigen-detection test in a pediatric practice. Pediatrics. 2005;115:280-5.
- Hall MC, Kieke B, Gonzales R, Belongia EA. Spectrum bias of a rapid antigen detection test for group A beta-hemolytic streptococcal pharyngitis in a pediatric population. Pediatrics. 2004;114:182-6.
- Cohen JF, Chalumeau M, Levy C, Bidet P, Benani M, Koskas M, et al. Effect of clinical spectrum, inoculum size and physician characteristics on sensitivity of a rapid antigen detection test for group A streptococcal pharyngitis. Eur J Clin Microbiol Infect Dis. 2013;32:787-93.
- Piñeiro Pérez R, Hernández Martín D, Carro Rodríguez MA, Casado Verrier E, Reques Cosme R, Carabaño Aguado I. Adecuación del diagnóstico y tratamiento de la faringoamigdalitis aguda a las guías actuales. Rev Pediatr Aten Primaria. 2016;18:317-24.
Comments
This article has no comments yet.