
Vol. 19 - Num. 75
Originales
Enfermedades tiroideas en adolescentes con diabetes mellitus tipo 1
M.ª Carmen Valdés Alonsoa, José M.ª Basain Valdésa, Lucía Llopiz Herrerab, Adriana Li de la Rosac, Aimée Álvarez Álvarezd
aServicio de Endocrinología. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
bServicio de Pediatría. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
cServicio de Laboratorio. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
dServicio de Laboratorio. Instituto Nacional de Endocrinología. La Habana. Cuba.
Cómo citar este artículo: Valdés Alonso MC, Basain Valdés JM, Llopiz Herrera L, Li de la Rosa A, Álvarez Álvarez A. Enfermedades tiroideas en adolescentes con diabetes mellitus tipo 1. Rev Pediatr Aten Primaria. 2017;19:249-57.
Publicado en Internet: 11-09-2017 - Número de visitas: 21124
Resumen
Objetivo: determinar el comportamiento de enfermedades tiroideas en pacientes pediátricos con diabetes mellitus tipo 1.
Material y método: estudio descriptivo, transversal, en 56 adolescentes con diagnóstico de diabetes mellitus tipo 1 atendidos en el Servicio de Endocrinología del Hospital Juan Manuel Márquez (La Habana, Cuba) en el periodo de octubre de 2015 a octubre de 2016. Las variables en estudio fueron: edad, sexo, tiempo de evolución de la diabetes mellitus, estado nutricional, función tiroidea y enfermedad tiroidea autoinmune. Las variables cualitativas se describieron estadísticamente mediante frecuencias absolutas y relativas, la asociación entre las variables categóricas se exploró con el test χ2 y la probabilidad exacta de Fisher. En todas las pruebas estadísticas se consideró un nivel de significación de α igual a 0,05.
Resultados: el 46,29% de los pacientes estudiados presentaron enfermedad tiroidea autoinmune; de ellos, el 33,33% eran del sexo femenino. El mayor grado de disfunción tiroidea se presentó en pacientes con mayores edades (36,0%), normopesos (68,0%) y con tiempo de evolución de la diabetes mellitus de entre 5-9 años (52,0%). El 32,0 frente al 80,0% de los pacientes presentaron respectivamente anticuerpos antitiroglobulina y antitiroperoxidasa positivos, relacionándose este último con la edad y el tiempo de evolución de la diabetes mellitus.
Conclusiones: se presentó disfunción tiroidea en los pacientes con enfermedad tiroidea autoinmune relacionado con la edad y el tiempo de evolución de la diabetes mellitus tipo 1. Los anticuerpos antitiroperoxidasa se relacionaron con la edad y el tiempo de evolución de la diabetes mellitus tipo 1.
Palabras clave
● Diabetes mellitus tipo 1 ● Enfermedades de la tiroides ● Tiroiditis autoinmuneINTRODUCCIÓN
La diabetes mellitus tipo 1 (DM1) es la enfermedad crónica endocrinológica más frecuente en la edad pediátrica y la segunda en la infancia después del asma en países desarrollados1. Es un síndrome heterogéneo que se caracteriza por hiperglucemia crónica de origen multifactorial como consecuencia de una alteración en la secreción y/o acción de la insulina, con repercusión en el metabolismo de los carbohidratos, lípidos y proteínas y que desarrolla a corto plazo complicaciones agudas, amenazantes para la vida, y a largo plazo complicaciones crónicas, graves e inhabilitantes, que en ocasiones puede causar la muerte2. El punto cardinal en la fisiopatología de la DM1 es la deficiencia absoluta de insulina, que predispone a la cetoacidosis. Esta deficiencia se debe a una destrucción de origen autoinmune de las células β del páncreas3, diagnosticándose más frecuentemente entre los 10 y 14 años, lo que se considera que puede tener relación con los cambios endocrinos de la pubertad; sin embargo, en los últimos 20 años se ha informado un incremento en la población de entre 0 y 4 años, lo que parece ser debido a los cambios en el estilo de vida de los niños, o bien por incorporación de procedimientos de diagnósticos más sensibles, aunque también pudiera tener relación con infecciones virales por virus de Coxsackie, de Epstein-Barr o rubeola, entre otros4.
De manera similar a la DM1, las alteraciones tiroideas son frecuentes en la adolescencia, y su prevalencia es creciente. Aunque la mayoría de casos, como el bocio difuso, cursan con función tiroidea normal, el hipo- o el hipertiroidismo no son infrecuentes y son, a menudo, infradiagnosticados en este grupo de edad5.
Dentro de las alteraciones tiroideas, el hipotiroidismo subclínico (tirotropina [TSH] elevada, triyodotironina [T3], tiroxina [T4] total y T4 libre normales) a menudo no es diagnosticado, aunque su prevalencia va en aumento debido al creciente cribado en poblaciones de riesgo (obesidad, hiperlipidemias, diabetes mellitus, etc.) y a la determinación relativamente reciente de la TSH. La mayoría son idiopáticos, y se evidencian por controles analíticos rutinarios en ausencia de patología o desencadenantes asociados. En los restantes, la tiroiditis autoinmune es la causa más frecuente6.
La etiología más frecuente del hipotiroidismo adquirido es la tiroiditis linfocitaria crónica (autoinmune, de Hashimoto), con un predominio femenino 2:1, y, en segundo lugar, el bocio endémico por déficit de yodo. Los casos de origen hipofisario o hipotalámico son muy raros5. La tiroiditis autoinmune es un proceso inflamatorio del tiroides caracterizado por presencia de bocio, anticuerpos circulantes y alteraciones histológicas. La enfermedad es más frecuente en la infancia y adolescencia y se asocia a determinados antígenos HLA de la clase II (alelos DR3, DR4 y DR5), algunos presentes en la DM1. La tiroiditis autoinmunitaria se asocia a otros procesos autoinmunes como la DM1 (20%), la insuficiencia suprarrenal, el hipoparatiroidismo y enfermedades cromosómicas como el síndrome de Down (4,3%) y síndrome de Turner (3,8%). Forma parte de los síndromes pluriglandulares autoinmunes tipo I y II, siendo el primero el más frecuente en la infancia7.
La asociación de diabetes mellitus y enfermedades tiroideas se presenta con más frecuencia en pacientes genéticamente predispuestos, como son los portadores del haplotipo HLA-DR3. Un porcentaje importante de pacientes con DM1 presenta anticuerpos antitiroideos positivos. De ellos, hasta un 50% progresa a enfermedad tiroidea autoinmune, fundamentalmente a hipotiroidismo primario, el cual se halla presente en un 2-5% de los pacientes con DM1 8.
El hipertiroidismo de origen autoinmune también se ha asociado con la DM1, aunque con una prevalencia bastante menor, de alrededor del 1-2%. En el caso del hipotiroidismo primario, este incremento parece relacionarse con la presencia de dislipidemia, aumento de la presión arterial diastólica y disfunción endotelial8.
A pesar de la frecuente asociación de DM1 y enfermedad tiroidea autoinmune, son escasos los estudios de prevalencia de ambos procesos en España y otros países8.
El objetivo de la presente investigación fue determinar el comportamiento de las enfermedades del tiroides en adolescentes con DM1 atendidos en el Hospital Pediátrico Docente Juan Manuel Márquez (La Habana, Cuba) en el periodo comprendido de 2015 a 2016.
MATERIAL Y MÉTODOS
Se realizó un estudio descriptivo de corte transversal en 54 pacientes adolescentes con diagnóstico de DM1 según criterios de la Organización Mundial de la Salud (n = 54), de ambos sexos, atendidos en el Servicio de Endocrinología del Hospital Pediátrico Docente Juan Manuel Márquez (La Habana, Cuba) en el periodo comprendido de octubre de 2015 a octubre de 2016. Se excluyeron aquellos pacientes tratados con fármacos inmunosupresores y/o con presencia de otras enfermedades intercurrentes. Las variables en estudio fueron: edad, sexo, tiempo de evolución de la DM1, estado nutricional, función tiroidea y enfermedad autoinmune tiroidea. De las historias clínicas de los pacientes se obtuvieron los siguientes datos: edad, sexo y tiempo de evolución de la DM1. A todos los pacientes se les realizaron las mediciones antropométricas de peso y talla, y posteriormente se les indicó TSH, T4 total, anticuerpos antitiroglobulina y anticuerpos antitiroperoxidasa. A partir de los valores de peso y talla se ubicó al paciente según sexo en la tabla cubana de percentiles de peso para la talla correspondiente9,10 y se determinó el percentil al que correspondía, interpretándose según lo establecido en Cuba. Las muestras de laboratorio fueron obtenidas por punción venosa en el laboratorio clínico, después de 12 horas de ayuno. Las determinaciones hormonales (TSH, T3 y T4 total) fueron realizadas en el laboratorio de dicha institución mediante el principio del análisis inmunorradiométrico en fase sólida; mientras que las determinaciones de los anticuerpos (antitiroglobulina y antiperoxidasa) se realizaron en el Instituto Nacional de Endocrinología mediante técnica de inmunoensayo de electroquimioluminiscencia.
Para el procesamiento de la información, los datos fueron incluidos en una base de datos automatizada con la hoja de cálculo electrónica Excel® 2003. Las variables cualitativas y las variables cuantitativas llevadas a escala ordinal se describieron estadísticamente mediante frecuencias absolutas y relativas. La asociación entre las variables categóricas se exploró con el test χ2 y la probabilidad exacta de Fisher. En todas las pruebas estadísticas se consideró un nivel de significación de α de 0,05.
El estudio estuvo debidamente avalado desde el punto de vista ético por las siguientes razones: 1) se aplicaron planillas de consentimiento informado por escrito, explicándole a cada paciente, padre y/o tutor legal la importancia de la investigación; 2) se respetó la integridad de los participantes en la investigación, asegurando la confidencialidad de todos los datos obtenidos, y 3) el Consejo Científico y el Comité de Ética de la Investigación del Hospital Pediátrico Docente Juan Manuel Márquez avalaron la presente investigación.
RESULTADOS
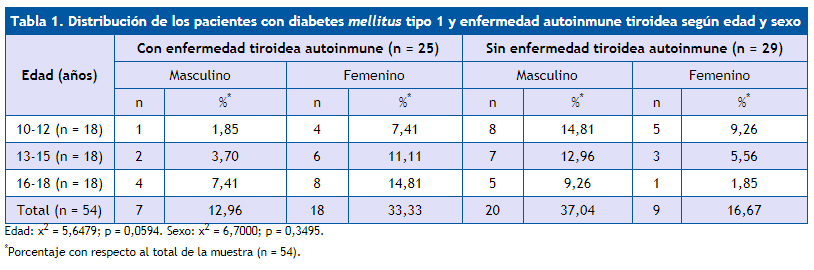
La distribución de los pacientes con DM1 y enfermedad autoinmune tiroidea según edad y sexo se muestran en la Tabla 1. Se observó que 25 (46,29%) pacientes con DM1 presentaron enfermedad tiroidea autoinmune, de los cuales 18 (33,33%) eran del sexo femenino.
| Tabla 1. Distribución de los pacientes con diabetes mellitus tipo 1 y enfermedad autoinmune tiroidea según edad y sexo | ||||||||
|---|---|---|---|---|---|---|---|---|
| Edad (años) | Con enfermedad tiroidea autoinmune (n = 25) | Sin enfermedad tiroidea autoinmune (n = 29) | ||||||
| Masculino | Femenino | Masculino | Femenino | |||||
| n | %* | n | %* | n | %* | n | %* | |
| 10-12 (n = 18) | 1 | 1,85 | 4 | 7,41 | 8 | 14,81 | 5 | 9,26 |
| 13-15 (n = 18) | 2 | 3,70 | 6 | 11,11 | 7 | 12,96 | 3 | 5,56 |
| 16-18 (n = 18) | 4 | 7,41 | 8 | 14,81 | 5 | 9,26 | 1 | 1,85 |
| Total (n = 54) | 7 | 12,96 | 18 | 33,33 | 20 | 37,04 | 9 | 16,67 |
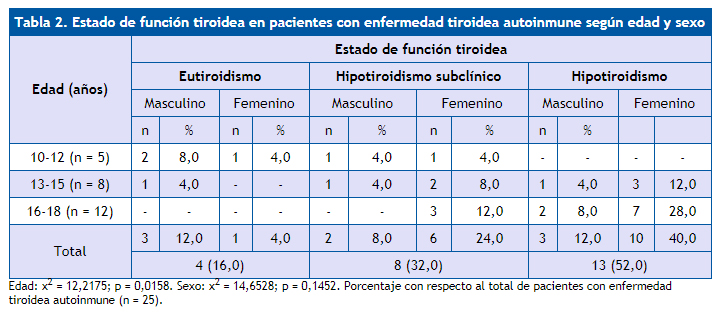
La comparación del estado de la función tiroidea en pacientes con enfermedad tiroidea autoinmune según edad y sexo se muestra en la Tabla 2. Al comparar el estado de la función tiroidea según la edad se encontró que los pacientes con mayores edades presentaron mayor grado de disfunción tiroidea que los pacientes con menores edades, donde, de los 13 pacientes con hipotiroidismo, nueve (36,0%) pacientes eran mayores de 16 años de edad, cuatro (16,0%) tenían entre 13 y 15 años de edad y ningún paciente tenía entre 10 y 12 años de edad. Con respecto al sexo, predominó el sexo femenino, con 17 (68,0%) pacientes.
| Tabla 2. Estado de función tiroidea en pacientes con enfermedad tiroidea autoinmune según edad y sexo | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Edad (años) | Estado de función tiroidea | |||||||||||
| Eutiroidismo | Hipotiroidismo subclínico | Hipotiroidismo | ||||||||||
| Masculino | Femenino | Masculino | Femenino | Masculino | Femenino | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| 10-12 (n = 5) | 2 | 8,0 | 1 | 4,0 | 1 | 4,0 | 1 | 4,0 | - | - | - | - |
| 13-15 (n = 8) | 1 | 4,0 | - | - | 1 | 4,0 | 2 | 8,0 | 1 | 4,0 | 3 | 12,0 |
| 16-18 (n = 12) | - | - | - | - | - | - | 3 | 12,0 | 2 | 8,0 | 7 | 28,0 |
| Total | 3 | 12,0 | 1 | 4,0 | 2 | 8,0 | 6 | 24,0 | 3 | 12,0 | 10 | 40,0 |
| 4 (16,0) | 8 (32,0) | 13 (52,0) | ||||||||||
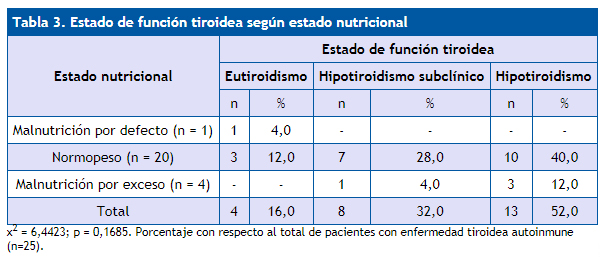
En la Tabla 3 se muestra el estado de la función tiroidea según el estado nutricional. Predominaron los pacientes con normopeso, con un total de 20 (80,0%) pacientes, de los cuales diez (40,0%) pacientes presentaron hipotiroidismo.
| Tabla 3. Estado de función tiroidea según estado nutricional | ||||||
|---|---|---|---|---|---|---|
| Estado nutricional | Estado de función tiroidea | |||||
| Eutiroidismo | Hipotiroidismo subclínico | Hipotiroidismo | ||||
| n | % | n | % | n | % | |
| Malnutrición por defecto (n = 1) | 1 | 4,0 | - | - | - | - |
| Normopeso (n = 20) | 3 | 12,0 | 7 | 28,0 | 10 | 40,0 |
| Malnutrición por exceso (n = 4) | - | - | 1 | 4,0 | 3 | 12,0 |
| Total | 4 | 16,0 | 8 | 32,0 | 13 | 52,0 |
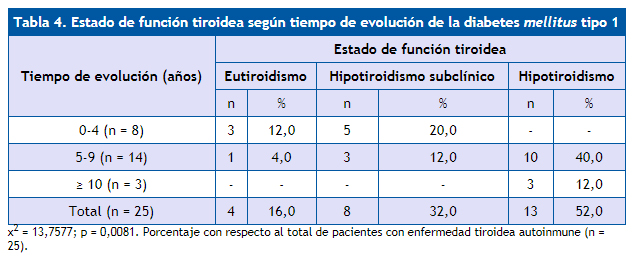
Según el tiempo de evolución de la DM1 y el estado de la función tiroidea, que se muestra en la Tabla 4, se encontró que existen diferencias significativas (p = 0,0081) entre estas dos variables estudiadas, se observó que a mayor tiempo de evolución de la DM1 existió un mayor grado de disfunción tiroidea.
| Tabla 4. Estado de función tiroidea según tiempo de evolución de la diabetes mellitus tipo 1 | ||||||
|---|---|---|---|---|---|---|
| Tiempo de evolución (años) | Estado de función tiroidea | |||||
| Eutiroidismo | Hipotiroidismo subclínico | Hipotiroidismo | ||||
| n | % | n | % | n | % | |
| 0-4 (n = 8) | 3 | 12,0 | 5 | 20,0 | - | - |
| 5-9 (n = 14) | 1 | 4,0 | 3 | 12,0 | 10 | 40,0 |
| ≥ 10 (n = 3) | - | - | - | - | 3 | 12,0 |
| Total (n = 25) | 4 | 16,0 | 8 | 32,0 | 13 | 52,0 |
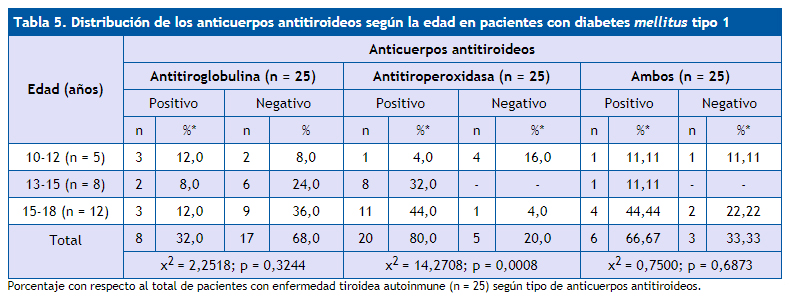
La distribución de los anticuerpos antitiroideos según la edad en los pacientes con DM1 estudiados se muestra en la Tabla 5. Como se observó, solo existen valores significativos en los anticuerpos antitiroperoxidasa (p = 0,0008) en relación con la edad.
| Tabla 5. Distribución de los anticuerpos antitiroideos según la edad en pacientes con diabetes mellitus tipo 1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Edad (años) | Anticuerpos antitiroideos | |||||||||||
| Antitiroglobulina (n = 25) | Antitiroperoxidasa (n = 25) | Ambos (n = 25) | ||||||||||
| Positivo | Negativo | Positivo | Negativo | Positivo | Negativo | |||||||
| n | %* | n | % | n | %* | n | %* | n | %* | n | %* | |
| 10-12 (n = 5) | 3 | 12,0 | 2 | 8,0 | 1 | 4,0 | 4 | 16,0 | 1 | 11,11 | 1 | 11,11 |
| 13-15 (n = 8) | 2 | 8,0 | 6 | 24,0 | 8 | 32,0 | - | - | 1 | 11,11 | - | - |
| 15-18 (n = 12) | 3 | 12,0 | 9 | 36,0 | 11 | 44,0 | 1 | 4,0 | 4 | 44,44 | 2 | 22,22 |
| Total
|
8 | 32,0 | 17 | 68,0 | 20 | 80,0 | 5 | 20,0 | 6 | 66,67 | 3 | 33,33 |
| χ2 = 2,2518; p = 0,3244 | χ2 = 14,2708; p = 0,0008 | χ2 = 0,7500; p = 0,6873 | ||||||||||
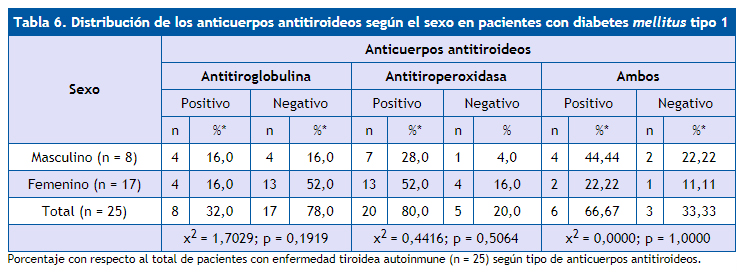
En la Tabla 6 se muestra la distribución de los anticuerpos antitiroideos según el sexo en los pacientes con DM1. Se encontró que no existieron diferencias significativas con respecto a los anticuerpos antitiroideos según el sexo. El sexo femenino mostró el mayor porcentaje con anticuerpos antitiroideos positivos con relación al sexo masculino.
| Tabla 6. Distribución de los anticuerpos antitiroideos según el sexo en pacientes con diabetes mellitus tipo 1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sexo | Anticuerpos antitiroideos | |||||||||||
| Antitiroglobulina | Antitiroperoxidasa | Ambos | ||||||||||
| Positivo | Negativo | Positivo | Negativo | Positivo | Negativo | |||||||
| n | %* | n | %* | n | %* | n | % | n | %* | n | %* | |
| Masculino (n = 8) | 4 | 16,0 | 4 | 16,0 | 7 | 28,0 | 1 | 4,0 | 4 | 44,44 | 2 | 22,22 |
| Femenino (n = 17) | 4 | 16,0 | 13 | 52,0 | 13 | 52,0 | 4 | 16,0 | 2 | 22,22 | 1 | 11,11 |
| Total (n = 25) | 8 | 32,0 | 17 | 78,0 | 20 | 80,0 | 5 | 20,0 | 6 | 66,67 | 3 | 33,33 |
| χ2 = 1,7029; p = 0,1919 | χ2 = 0,4416; p = 0,5064 | χ2 = 0,0000; p = 1,0000 | ||||||||||
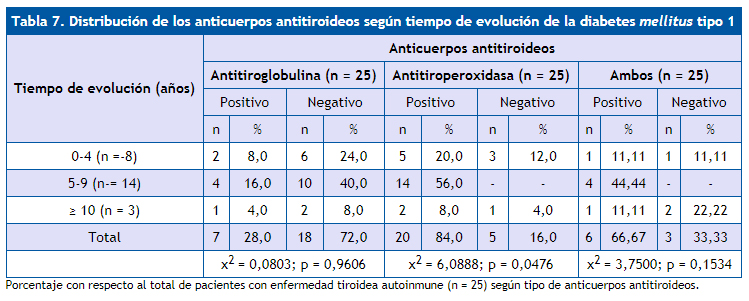
En la Tabla 7 se muestra la distribución de los anticuerpos antitiroideos según tiempo de evolución de la DM1 en los pacientes estudiados. No se encontró asociación entre los anticuerpos antitiroglobulina y ambos anticuerpos positivos con el tiempo de evolución de la DM1. Al analizar los anticuerpos antitiroperoxidasa, se pudo observar que existieron valores más significativos de dichos anticuerpos (p = 0,0476) en relación con el mayor tiempo de evolución de la diabetes mellitus (el 100% de los pacientes entre cinco y nueve años de evolución de la DM1 presentaban estos anticuerpos positivos, mientras que el 66,67% de los diabéticos tipo 1 con diez años o más de evolución de la diabetes presentaron estos anticuerpos positivos.
| Tabla 7. Distribución de los anticuerpos antitiroideos según tiempo de evolución de la diabetes mellitus tipo 1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tiempo de evolución (años) | Anticuerpos antitiroideos | |||||||||||
| Antitiroglobulina (n = 25) | Antitiroperoxidasa (n = 25) | Ambos (n = 25) | ||||||||||
| Positivo | Negativo | Positivo | Negativo | Positivo | Negativo | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| 0-4 (n =-8) | 2 | 8,0 | 6 | 24,0 | 5 | 20,0 | 3 | 12,0 | 1 | 11,11 | 1 | 11,11 |
| 5-9 (n-= 14) | 4 | 16,0 | 10 | 40,0 | 14 | 56,0 | - | - | 4 | 44,44 | - | - |
| ≥ 10 (n = 3) | 1 | 4,0 | 2 | 8,0 | 2 | 8,0 | 1 | 4,0 | 1 | 11,11 | 2 | 22,22 |
| Total | 7 | 28,0 | 18 | 72,0 | 20 | 84,0 | 5 | 16,0 | 6 | 66,67 | 3 | 33,33 |
| χ2 = 0,0803; p = 0,9606 | χ2 = 6,0888; p = 0,0476 | χ2 = 3,7500; p = 0,1534 | ||||||||||
DISCUSIÓN
La DM1 se asocia con cierta frecuencia a otras enfermedades de etiología inmunitaria, siendo la más prevalente la enfermedad tiroidea autoinmune. Ambas son enfermedades de glándulas endocrinas originadas por la estimulación de células T órgano-específicas. La asociación de ambas se presenta con más frecuencia en pacientes genéticamente predispuestos, como son los portadores del haplotipo HLA-DR3, donde un porcentaje importante de pacientes con DM1 presenta anticuerpos antitiroideos positivos. De ellos, hasta un 50% progresa a enfermedad tiroidea autoinmune, fundamentalmente a hipotiroidismo primario, el cual se halla presente en un 2-5% de los pacientes con DM1 8. La tiroiditis crónica autoinmune se caracteriza por la presencia de anticuerpos antitiroideos específicos en suero, los cuales son positivos en el 10-12% en la población general y entre niños con DM1, de acuerdo con el grado de disfunción tiroidea, entre 3 y 50%11,12.
El estudio de Baena8 muestra una elevada prevalencia de enfermedad tiroidea autoinmune en pacientes con DM1 (17%). No obstante, este resultado es similar a los publicados por otros autores11,12 en estudios internacionales, la mayoría de ellos realizados en población pediátrica, en los que la prevalencia de enfermedad tiroidea autoinmune se encuentra entre el 15,8 y el 43,7%8. En el estudio de Rivera11 se obtiene que, del total de pacientes diabéticos, hay una predominancia porcentual del género femenino con un 52,6% (p < 0,019) y con una mayoría significativa de los adolescentes, del 52,6% (p < 0,001), lo cual guarda relación con la bibliografía nacional12,13 e internacional14,15 que apoya dicha investigación. En el estudio de Rivera11 se diagnosticaron nueve pacientes de enfermedad tiroidea autoinmune para un 9,3%, concentrándose mayormente en el grupo de los adolescentes. De las nueve pacientes con enfermedad tiroidea autoinmune, seis presentaban tiroiditis de Hashimoto en fase eutiroidea y tres en fase hipotiroidea, lo cual difiere en lo descrito por Briceño et al.12 a nivel nacional y Barker et al.15 a nivel internacional, que encuentran predominio estadísticamente significativo del hipotiroidismo.
Baena et al.8, en un estudio de 90 pacientes con DM1, encontró que el 17,8% del total de pacientes estudiados presentaban enfermedad tiroidea autoinmune conocida que, por orden de frecuencia, se correspondía con hipotiroidismo primario (9,9%), hipotiroidismo subclínico (7,1%) y enfermedad de Graves (0,8%). En el estudio de Miraval León16, la disfunción tiroidea más frecuente es el hipotiroidismo clínico, con un 84,4%, lo que supera en frecuencia a otros estudios 14,16, pero coincide con la literatura médica internacional17.
El porcentaje de hipotiroidismo subclínico fue del 2,5% de todo aquel con despistaje hormonal, menor en cantidad en comparación con otros estudios14,16. Johnson et al.18 reportan una prevalencia de hasta un 50%, Gronich17 encuentra un 8,6% de casos de hipotiroidismo subclínico en mujeres australianas a pesar de que el hipotiroidismo subclínico no fue la principal alteración tiroidea encontrada.
En el estudio realizado en nuestro hospital se encontró que la enfermedad tiroidea autoinmune que predominó fue el hipotiroidismo, siguiéndole en orden de frecuencia el hipotiroidismo subclínico en pacientes adolescentes y en el sexo femenino, lo cual coincide con lo descrito en la literatura médica revisada. No se presentaron casos de hiperfunción tiroidea (hipertiroidismo).
En relación con el estado nutricional de los pacientes con DM1, que estudia Rivera11, el 77,2% correspondió al tipo eutrófico, el 6,2% a la obesidad, el 6,2% a la desnutrición crónica, el 5,2% al sobrepeso y el 5,2% a la desnutrición aguda. Esto coincide con lo encontrado a nivel nacional por Briceño et al.12, en cuyo estudio la distribución del estado nutricional con respecto a las enfermedades tiroideas refleja que, de las nueve pacientes femeninas con tiroiditis, siete eran eutróficas. En lo descrito por Kordonouri et al.14 no había diferencias respecto al crecimiento o el peso en los pacientes con o sin enfermedad tiroidea autoinmune. En el trabajo que se realizó en nuestro centro predominó el estado nutricional normopeso (eutrófico), aunque un porcentaje de los mismos presentaba hipotiroidismo. Esto se corresponde con lo señalado en la literatura médica revisada.
Según el tiempo de evolución de la DM1, el estudio de Rivera11 demuestra que la mayoría de los pacientes tenía más de cuatro años de evolución de la enfermedad, correspondiendo al 44,3%, habiendo de las nueve pacientes estudiadas, seis con patología tiroidea, de ellas tres con tiroiditis de Hashimoto en fase eutiroidea y tres en fase hipotiroidea. Esto difiere de lo encontrado por Martín13 a nivel nacional donde evidencia que en más de la mitad (51,2%) la diabetes mellitus había sido diagnosticada hacía menos de tres años, pero coincide con Kordonouri14 y Barker15, que señalan una mayor duración de la diabetes mellitus en relación a las pacientes con enfermedad tiroidea autoinmune. No obstante, a diferencia de otros trabajos12,14,15, Baena8 no encuentra una asociación entre el tiempo de evolución de la diabetes y la presencia de enfermedad tiroidea autoinmune en su estudio; sin embargo, sí evidenciamos una elevada prevalencia de enfermedad tiroidea autoinmune en el sexo femenino (la presentaban el 24,6% frente al 10,8% del sexo masculino). En este estudio se demostró diferencia significativa, pues a mayor tiempo de evolución de la DM1 hubo mayor grado de disfunción tiroidea.
La positividad de los anticuerpos específicos contra el tiroides en pacientes con DM1 en edad pediátrica se ha reportado más alto en comparación con la población general, encontrándose positivos entre el 7 y el 40%. Los anticuerpos antitiroideos son más altos en los pacientes con DM1 de más años de evolución de la enfermedad. Los anticuerpos que principalmente median la respuesta autoinmune tiroidea son los siguientes: antitiroglobulina, antirreceptor de tirotropina, antihormona tiroidea, y antitiroperoxidasa. Este último se detecta en todos los tipos de enfermedad tiroidea autoinmune, alcanzando títulos máximos en la tiroiditis de Hashimoto, incluso en aquellos casos que otros anticuerpos antitiroideos son negativos. Este antígeno (antígeno antitiroperoxidasa) está dirigido a la peroxidada tiroidea, una enzima que cataliza la yodación de residuos de tiroxina en tiroglobulina y que se localiza tanto en el citoplasma como en el polo apical de la membrana de las células tiroideas. Estos anticuerpos son los responsables de la citotoxicidad dependiente del complemento observado en las tiroiditis19. Cabe destacar en este sentido el estudio de Kordonouri14 que incluye a 7097 pacientes con DM1, una media de edad de 12 años, una prevalencia de enfermedad tiroidea del 15,8% y una prevalencia de anticuerpos antitiroideos positivos del 21,6%.
Es bien conocido que, en pacientes con DM1, el principal marcador de riesgo para la aparición de enfermedad tiroidea es el desarrollo de anticuerpos antitiroideos (antitiroperoxidasa, antitiroglobulina e inmunoglobulinas estimulantes del tiroides)8. De esta forma, se ha observado que aquellos con anticuerpos antitiroideos positivos presentan un riesgo hasta 18 veces mayor de desarrollar enfermedad tiroidea, si bien el hipotiroidismo primario puede presentarse también hasta en el 20-30% de los pacientes con anticuerpos antitiroideos negativos, Baena8 obtiene datos muy similares en su estudio, en el que el 25,6% de los pacientes con enfermedad tiroidea autoinmune presentaban anticuerpos antitiroideos negativos. Por otro lado, si bien parece que la prevalencia de enfermedad tiroidea aumenta en relación con la edad y con el tiempo de evolución de la diabetes, no se ha documentado una mayor prevalencia en pacientes con mal control metabólico, aunque hay pocos estudios que evalúen esta relación. Barker15 realizó un estudio donde se obtuvo que los pacientes con anticuerpos antitiroideos positivos eran con más frecuencia mujeres (58%; p < 0,0001), adolescentes (16,1 años; p < 0,0013).
En el estudio Rivera11, de los pacientes a los que les realiza determinación de anticuerpos antitiroperoxidasa, solo seis resultaron positivos para un 11,2%, cuatro (66,7%) con tiroiditis de Hashimoto en fase eutiroidea y dos (33,3%) en fase hipotiroidea. En el ámbito nacional, Briceño12 evidencia en relación con los anticuerpos antitiroideos algo similar; en 126 pacientes (86,3%) resultan negativos y positivos en 12,7%. A nivel internacional, Glastras20 detectó anticuerpos antitiroperoxidasa positivos en 13 de 166 pacientes (7,8%); seis de los 13 pacientes (46,2%) con anticuerpos antitiroperoxidasa positivos en el momento del diagnóstico desarrollaron una patología tiroidea, frente a solo el 3,6% con anticuerpos antitiroperoxidasa negativos; datos diferentes se obtuvieron del estudio de Baena8 donde un 41,1% resultaron antitioperoxidasa positivos y un 25,6% negativos; en el 33,3% no se dispuso de datos.
En nuestro estudio, de los anticuerpos antitiroideos, solo los anticuerpos antitiroperoxidasa resultaron positivos y se relacionaron con el tiempo de evolución de la enfermedad tiroidea autoinmune, no así en el caso de los anticuerpos antitiroglobulina o la presencia de ambos anticuerpos, donde no hubo significación estadística con el tiempo de evolución de la enfermedad. El sexo femenino mostró un mayor porcentaje de anticuerpos antitiroperoxidasa positivos, aunque no resultó significativo. Nuestros resultados son similares a los descritos en la literatura médica revisada.
CONCLUSIONES
Existió enfermedad tiroidea autoinmune en los adolescentes con diabetes mellitus tipo 1.
Se presentó disfunción tiroidea en los adolescentes con enfermedad tiroidea autoinmune expresada por hipotiroidismo clínico y subclínico relacionado con la edad y el tiempo de evolución de la DM1.
Los anticuerpos antitiroperoxidasa se relacionaron con la edad y el tiempo de evolución de la diabetes mellitus tipo 1, no así con el sexo. No existió relación de los anticuerpos antitiroglobulina con las variables estudiadas.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
ABREVIATURAS
DM1: diabetes mellitus tipo 1 · T3: triyodotironina · T4: tiroxina · TSH: tirotropina.
BIBLIOGRAFÍA
- Camacho B, Manzanares A, Espino R. Debut de diabetes mellitus tipo 1 en el área hospitalaria de Valme. Vox Paediatr. 2012;19:9-13.
- Asenjo S, Muzzo S, Pérez MV, Ugarte F, Willshaw ME. Consenso en el diagnóstico y tratamiento de la diabetes tipo 1 del niño y del adolescente. Rev Chil Pediatr. 2007;78:534-41.
- Soltész G. La diabetes en niños: tendencias cambiantes dentro de una epidemia emergente. Diabetes Voice. 2007;52:13-5.
- Braverman Bronstein A, Rendón Macías ME, Iglesias Leboreiro J, Bernárdez Zapata I, Antillón Ferreira C. Características clínicas y de laboratorio en niños con diabetes mellitus. Rev Mex Pediatr. 2013;80;200-5.
- Curell Aguilá N. Hipotiroidismo en adolescentes. 2013;12:24-31.
- Chueca Guindulain M, Berrade Zubiri S, Dura Travé T, Oyarzábal Irigoyen M. Hipotiroidismo subclínico en la infancia y adolescencia. Rev Esp Endocrinol Pediatr. 2014;5:49-57.
- Valdés Alonso MC. Síndrome poliglandular autoinmune. En: Coto Hermosilla C. Reumatología Pediátrica. La Habana: Editorial Ciencias Médicas; 2012. p. 412-36.
- Baena MG, Carral F, Roca MM, Cayón M, Ortego J, Aguilar-Diosdado M. Prevalencia de la enfermedad tiroidea autoinmune en pacientes con diabetes mellitus tipo 1. Av Diabetol. 2010;26:42-6.
- Jordan JR. Desarrollo humano en Cuba. La Habana: Editorial Científico-Técnica; 1979.
- Esquivel M, Rubí A. Curvas nacionales de peso y talla. Su interpretación y uso en la valoración del estado nutricional. Rev Cubana Pediatr. 1985;57(7):377-83.
- Rivera N. Enfermedad tiroidea autoinmune en pacientes con diabetes mellitus tipo 1. Consulta de Endocrinología Pediátrica. Hospital de Niños Dr. Jorge Lizarraga. Valencia, junio 2009-2012. Valencia, Venezuela: Universidad de Carabobo; 2013.
- Briceño Y, Paoli M, Maulino N, Gaffaro L, Marcano H, Pérez M. Dislipidemia y disfunción tiroidea en niños y adolescentes con diabetes mellitus tipo1: relación con el control metabólico e índice de masa corporal. Rev Venez Endocrinol Metab. 2009;7:23-8.
- Martín R. Frecuencia de trastornos de la función tiroidea en escolares y adolescentes con diabetes mellitus Consulta de Endocrinología. Hospital Pediátrico Dr. Agustín Zubillaga. Barquisimeto, Venezuela: Universidad Centro Occidental Lisandro Alvarado; 2007.
- Kordonouri O, Klinghammer A, Lang EB, Gruters-Kieslich A, Grabert M, Holl RW. Thiyroid autoimmunity in children and adolescents with type 1 diabetes: a multicenter survey. Diabetes Care. 2002;25:1346-50.
- Barker JM, Yu J, Yu L, Wang J, Miao D, Bao F, et al. Autoantibody “subspecificity” in type 1 diabetes: risk for organ specific autoimmunity clusters in distinct groups. Diabetes Care. 2005;28:850-5.
- Miraval León LJ. La disfunción tiroidea en pacientes con diabetes mellitus tipo 2. Hospital Nacional Dos de Mayo 2013-2015. Tesis. Lima: Universidad Nacional Mayor de San Marcos; 2016.
- Gronich N, Deftereos SN, Lavi I, Persidis AS, Abernethy DR, Rennert G. Hypothyroidism is a risk factor for new-onset diabetes: a cohort study. Diabetes Care. 2015;38:1657-64.
- Johnson J. Diabetes control in thyroid disease. Diabetes Spectrum. 2006;19(3):148-53.
- Rivero Escalante H, Dorantes Álvarez LM, García Morales L, Coyote Estrada N, Martínez Duncker C, Palafox Vázquez H, et al. Frecuencia de enfermedad tiroidea autoinmune en niños con diabetes mellitus tipo 1. Bol Med Hosp Infant Mex. 2001;58:627-34.
- Glastras SJ, Craig ME, Verge CF, Chan AK, Cusumano JM, Donaghue KC. The role of autoimmunity at diagnosis of type 1 diabetes in the development of thyroid and celiac disease and microvascular complications. Diabetes Care. 2005;28:2170-5.