

Vol. 19 - Num. 75
Original Papers
Thyroid diseases in adolescents with type 1 diabetes mellitus
M.ª Carmen Valdés Alonsoa, José M.ª Basain Valdésa, Lucía Llopiz Herrerab, Adriana Li de la Rosac, Aimée Álvarez Álvarezd
aServicio de Endocrinología. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
bServicio de Pediatría. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
cServicio de Laboratorio. Hospital Pediátrico Docente Juan Manuel Márquez. La Habana. Cuba.
dServicio de Laboratorio. Instituto Nacional de Endocrinología. La Habana. Cuba.
Reference of this article: Valdés Alonso MC, Basain Valdés JM, Llopiz Herrera L, Li de la Rosa A, Álvarez Álvarez A. Thyroid diseases in adolescents with type 1 diabetes mellitus. Rev Pediatr Aten Primaria. 2017;19:249-57.
Published in Internet: 11-09-2017 - Visits: 14336
Abstract
Introduction: the type 1 diabetes mellitus is related with thyroid alterations. Objective: to determine the behaviour of thyroid diseases in pediatric patients with type 1 diabetes mellitus.
Material and method: descriptive cross-sectional study in 56 adolescents with diagnostic of type 1 diabetes mellitus assisted in the service of Endocrinology of the Juan Manuel Márquez hospital in the period between October 2015 and October 2016. The variables in study were: age, sex, time of evolution of the diabetes mellitus, nutritional state, thyroid function and autoimmune thyroid disease. The qualitative variables were statistically sescribed by absolute and relative frequencies; the association among the categorical variables was explored with the χ2 test and Fisher's exact probability. In all the statistical tests, it was considered a significance level of alpha equal to 0.05.
Results: 46.29% of the studied patients presented autoimmune thyroid disease; of them, 33.33% were female. The highest degree of thyroid dysfunction was present in older patients (36.0%), with normal weigh (68.0%) and time of evolution of the diabetes mellitus among 5-9 years (52.0%). 32.0% vs 80.0% of the patients presented antithyroglobulin antibodies and antithyroperoxidase antibodies respectively, being related this last one with the age and the time of evolution of the diabetes mellitus.
Conclusions: thyroid dysfunction was presented in the patients with autoimmune thyroid disease related to the age and the time of evolution of the type 1 diabetes mellitus. The antithyroperoxidase antibodies were related with the age and the time of evolution of type 1 diabetes mellitus.
Keywords
● Autoimmune thyroiditis ● Diabetes mellitus type 1 ● Thyroid diseasesINTRODUCTION
Type 1 diabetes mellitus (T1D) is the most prevalent endocrine chronic disease in the paediatric age group, and the second most frequent in children in developed countries following asthma.1 It is a heterogeneous syndrome characterised by chronic hyperglycaemia of a multifactorial aetiology that results from changes in the secretion and/or activity of insulin affecting the metabolism of carbohydrates, lipids and proteins, and presents with acute life-threatening complications in the short-term and with chronic, severe, disabling and potentially fatal complications in the long-term.2 The key point in the pathophysiology of T1D is absolute insulin deficiency, which predisposes the individual to ketoacidosis. This deficiency is due to the autoimmune destruction of the β cells of the pancreas3 and is diagnosed most frequently between ages 10 and 14 years, which suggests an association with the endocrine changes that take place in puberty; however, in the past 20 years there has been evidence of an increase in its incidence in children aged 0 to 4 years, which may be due to changes in lifestyle in this population or to the introduction of diagnostic methods that are more sensitive, although it could also be associated with viral infection by Coxsackievirus, Epstein-Barr virus or rubella, among others.4
Similarly to T1D, thyroid abnormalities are frequent in adolescence, and their prevalence is increasing. Although in most cases, for instance those of diffuse goitre, patients present with normal thyroid function, hypo- or hyperthyroidism are not infrequent and are commonly underdiagnosed in this age group.5
Among the thyroid abnormalities, subclinical hypothyroidism (elevated thyroid-stimulating hormone [TSH] with normal triiodothyronine [T3] and free and total thyroxine [T4] levels) is often not diagnosed, although its reported prevalence has been rising due to increased screening in risk populations (with obesity, hyperlipidaemia, diabetes mellitus, etc) and the relatively recent TSH test. Most cases are idiopathic and are identified by routine tests in the absence of associated manifestations or triggers. In the remaining cases, autoimmune thyroiditis is the most common cause.6
The most frequent aetiology of acquired hypothyroidism is chronic lymphocytic thyroiditis (autoimmune, Hashimoto disease), with a 2:1 female to male ratio, followed by endemic goitre due to iodine deficiency. Cases with a pituitary or hypothalamic aetiology are very rare.5 Autoimmune thyroiditis is an inflammatory process of the thyroid characterised by the presence of goitre, circulating antibodies and histologic changes. This disease is most frequent in children and adolescents and is associated with certain class II HLA antigens (DR3, DR4 and DR5 alleles), some of which are present in T1D. Autoimmune thyroiditis is associated with other autoimmune processes, such as T1D (20%), adrenal insufficiency, hypoparathyroidism and chromosomal disorders such as Down syndrome (4.3%) and Turner syndrome (3.8%). It is a feature of type I and II autoimmune polyendocrine syndromes, the former of which is more prevalent in children.7
The association of diabetes mellitus with thyroid disorders is found more frequently in patients with a genetic predisposition, for instance HLA-DR3 haplotype carriers. A considerable percentage of patients with T1D test positive for antithyroid antibodies. Up to 50% of these patients progress to autoimmune thyroid disease, most frequently primary hypothyroidism, which is found in 2% to 5% of patients with T1D.8
Autoimmune hyperthyroidism has also been associated with T1D, although with a considerably lower prevalence of 1% to 2%. In the case of primary hypothyroidism, this increase seems to be associated with the presence of dyslipidaemia, high diastolic blood pressure and endothelial dysfunction.8
Despite the frequent association of T1D and autoimmune thyroid disease, few studies have been conducted on the prevalence of this comorbidity in Spain and other countries.8
The aim of this study was to establish patterns in thyroid disorders in adolescents with T1D managed at the Hospital Pediátrico Docente Juan Manuel Márquez (Havana, Cuba) between 2015 and 2016.
MATERIALS AND METHODS
We conducted a cross-sectional descriptive study in 54 patients of both sexes with a diagnosis of T1D based on the criteria established by the World Health Organization (n = 54) managed at the endocrinology department of the Hospital Pediátrico Docente Juan Manuel Márquez (Havana, Cuba) between October 2015 and October 2016. We excluded patients treated with immunosuppressants and/or with intercurrent disease. The variables under study were: age, sex, duration of T1D, nutritional status, thyroid function and autoimmune thyroid disease. We collected the following data from the medical records of the patients: age, sex and duration of T1D. All patients underwent anthropometric measurements of their weight and height, followed by determination of TSH, total T4, and antithyroglobulin and antithyroperoxidase antibody levels. Based on their measured weight and height, patients were placed in the corresponding Cuban weight-for-height percentile table for their sex9,10 to obtain their percentile, which was interpreted according to the criteria established for Cuba. Test samples were obtained by venipuncture at the clinical laboratory after 12 hours of fasting. Hormone levels (TSH, total T3 and T4) were measured at the laboratory of the hospital by solid-phase radioimmunoassay, while antibody levels (antithyroglobulin and antithyroperoxidase) were measured at the Instituto Nacional de Endocrinología (National Institute of Endocrinology) by means of electrochemiluminescence immunoassay.
To process the data, we entered them in a digital database using Excel® 2003 worksheets. Qualitative and quantitative variables converted to an ordinal scale were described statistically by means of absolute and relative frequencies. We studied the association between categorical variables using the χ2 and Fisher exact tests. We set the α level of significance for all tests at 0.05.
We ensured that the study complied with ethical standards with the following: 1) Use of written informed consent forms explaining to each patient, parent and/or legal guardian the relevance of the research; 2) the study respected the integrity of participants and ensured the confidentiality of all the collected data, and 3) the Scientific Council and the Research Ethics Committee of the Hospital Pediátrico Docente Juan Manuel Márquez approved the study presented here.
RESULTS
Table 1 shows the distribution of autoimmune thyroid disease in patients with T1D by age and sex. We found that 25 patients with T1D (46.29%) had autoimmune thyroid disease, of who 18 (33.33%) were female.
| Table 1. Distribution of autoimmune thyroid disease in patients with type 1 diabetes mellitus by age and sex | ||||||||
|---|---|---|---|---|---|---|---|---|
| Age (years) | With autoimmune thyroid disease (n = 25) | Without autoimmune thyroid disease (n = 29) | ||||||
| Male | Female | Male | Female | |||||
| n | %* | n | %* | n | %* | n | %* | |
| 10-12 (n = 18) | 1 | 1.85 | 4 | 7.41 | 8 | 14.81 | 5 | 9.26 |
| 13-15 (n = 18) | 2 | 3.70 | 6 | 11.11 | 7 | 12.96 | 3 | 5.56 |
| 16-18 (n = 18) | 4 | 7.41 | 8 | 14.81 | 5 | 9.26 | 1 | 1.85 |
| Total (n = 54) | 7 | 12.96 | 18 | 33.33 | 20 | 37.04 | 9 | 16.67 |
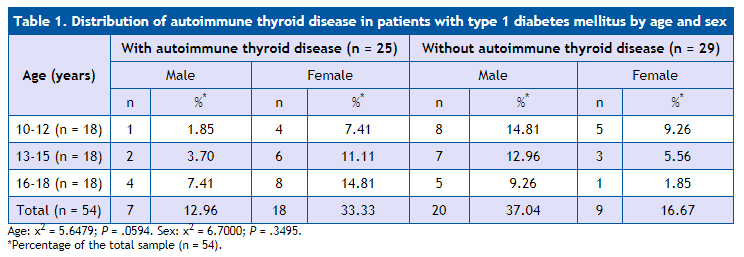
Table 2 compares thyroid function in patients with autoimmune thyroid disease by age and sex. In the comparison by age, we found that older patients had a greater degree of thyroid dysfunction compared to younger patients, with 9 (36.0%) of the 13 patients with hypothyroidism aged more than 16 years, 4 (16.0%) aged 13 to 15 years, and none aged 10 to 12 years. When it came to sex, there was a predominance of female patients, who amounted to 17 of these patients (68.0%).
| Table 2. Thyroid function in patients with autoimmune thyroid disease by age and sex | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | Thyroid function | |||||||||||
| Normal function | Subclinical hypothyroidism | Hypothyroidism | ||||||||||
| Male | Female | Male | Female | Male | Female | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| 10-12 (n = 5) | 2 | 8.0 | 1 | 4,0 | 1 | 4.0 | 1 | 4.0 | - | - | - | - |
| 13-15 (n = 8) | 1 | 4.0 | - | - | 1 | 4.0 | 2 | 8.0 | 1 | 4.0 | 3 | 12.0 |
| 16-18 (n = 12) | - | - | - | - | - | - | 3 | 12.0 | 2 | 8.0 | 7 | 28.0 |
| Total | 3 | 12.0 | 1 | 4,0 | 2 | 8.0 | 6 | 24.0 | 3 | 12.0 | 10 | 40.0 |
| 4 (16.0) | 8 (32.0) | 13 (52.0) | ||||||||||
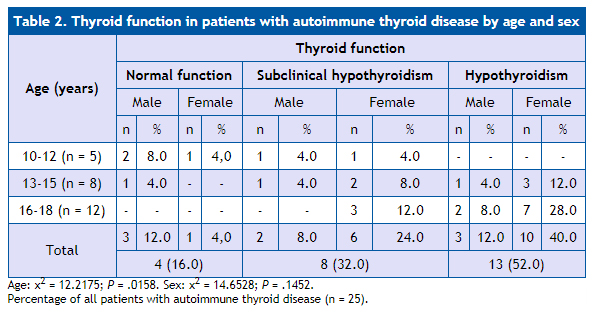
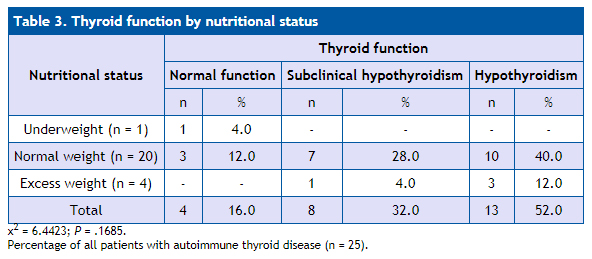
Table 3 presents current thyroid functioning in patients by nutritional status. The majority of patients, amounting to 20 (80.0%), had normal weight, and 10 of them (40.0%) presented with hypothyroidism.
| Table 3. Thyroid function by nutritional status | ||||||
|---|---|---|---|---|---|---|
| Nutritional status | Thyroid function | |||||
| Normal function | Subclinical hypothyroidism | Hypothyroidism | ||||
| n | % | n | % | n | % | |
| Underweight (n = 1) | 1 | 4.0 | - | - | - | - |
| Normal weight (n = 20) | 3 | 12.0 | 7 | 28.0 | 10 | 40.0 |
| Excess weight (n = 4) | - | - | 1 | 4.0 | 3 | 12.0 |
| Total | 4 | 16.0 | 8 | 32.0 | 13 | 52.0 |
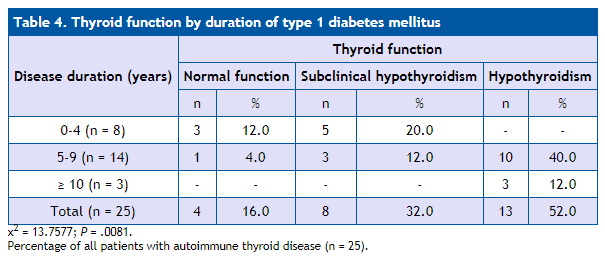
As regards the duration of T1D and current thyroid functioning, for which data are shown in Table 4, we found a significant association in the differences in these two variables (P = .0081), with the degree of thyroid impairment increasing with longer duration of T1D.
| Table 4. Thyroid function by duration of type 1 diabetes mellitus | ||||||
|---|---|---|---|---|---|---|
| Disease duration (years) | Thyroid function | |||||
| Normal function | Subclinical hypothyroidism | Hypothyroidism | ||||
| n | % | n | % | n | % | |
| 0-4 (n = 8) | 3 | 12.0 | 5 | 20.0 | - | - |
| 5-9 (n = 14) | 1 | 4.0 | 3 | 12.0 | 10 | 40.0 |
| ≥ 10 (n = 3) | - | - | - | - | 3 | 12.0 |
| Total (n = 25) | 4 | 16.0 | 8 | 32.0 | 13 | 52.0 |
The distribution of antithyroid antibodies by age in the studied sample of patients with T1D is shown in Table 5. We only found a significant association with age for antithyroperoxidase antibodies (P = .0008).
| Table 5. Distribution of antithyroid antibodies by age in patients with type 1 diabetes mellitus | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | Antithyroid antibodies | |||||||||||
| Antithyroglobulin (n = 25) | Antithyroperoxidase (n = 25) | Both (n = 25) | ||||||||||
| Positive | Negative | Positive | Negative | Positive | Negative | |||||||
| n | %* | n | % | n | %* | n | %* | n | %* | n | %* | |
| 10-12 (n = 5) | 3 | 12.0 | 2 | 8.0 | 1 | 4.0 | 4 | 16.0 | 1 | 11.11 | 1 | 11.11 |
| 13-15 (n = 8) | 2 | 8.0 | 6 | 24.0 | 8 | 32.0 | - | - | 1 | 11.11 | - | - |
| 15-18 (n = 12) | 3 | 12.0 | 9 | 36.0 | 11 | 44.0 | 1 | 4.0 | 4 | 44.44 | 2 | 22.22 |
| Total |
8 | 32.0 | 17 | 68.0 | 20 | 80.0 | 5 | 20.0 | 6 | 66.67 | 3 | 33.33 |
| χ2 = 2.2518; P = .3244 | χ2 = 14.2708; P = .0008 | χ2 = 0.7500; P = .6873 | ||||||||||
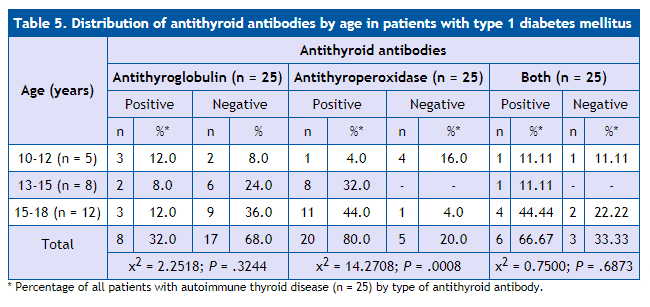
Table 6 shows the distribution of antithyroid antibodies by sex in patients with T1D. We found that there were no statistically significant differences in antithyroid antibodies based on sex. There was a greater proportion of female patients with positive antithyroid antibody test results compared to male patients.
| Table 6. Distribution of antithyroid antibodies by sex in patients with type 1 diabetes mellitus | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Antithyroid antibodies | |||||||||||
| Antithyroglobulin | Antithyroperoxidase | Both | ||||||||||
| Positive | Negative | Positive | Negative | Positive | Negative | |||||||
| n | %* | n | %* | n | %* | n | % | n | %* | n | %* | |
| Male (n = 8) | 4 | 16.0 | 4 | 16.0 | 7 | 28.0 | 1 | 4.0 | 4 | 44.44 | 2 | 22.22 |
| Female (n = 17) | 4 | 16.0 | 13 | 52.0 | 13 | 52.0 | 4 | 16.0 | 2 | 22.22 | 1 | 11.11 |
| Total (n = 25) | 8 | 32.0 | 17 | 78.0 | 20 | 80.0 | 5 | 20.0 | 6 | 66.67 | 3 | 33.33 |
| χ2 = 1.7029; P = .1919 | χ2 = 0.4416; P = .5064 | χ2 = 0.0000; P = 1.0000 | ||||||||||

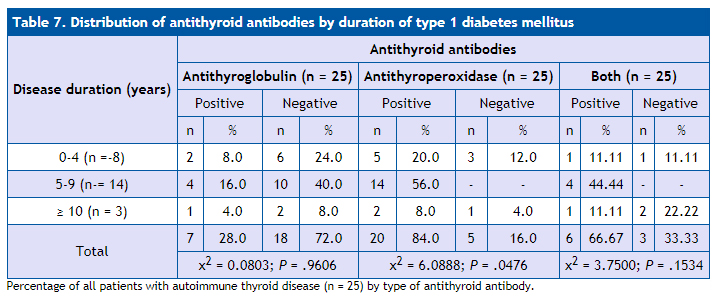
Table 7 shows the distribution of antithyroid antibodies based on the duration of T1D in the patients under study. We did not find an association between positive results for antithyroglobulin antibodies or both antibodies and the duration of T1D. When we analysed the antithyroperoxidase antibody results, we observed that its levels were significantly greater (P = .0476) with greater duration of T1D (100% of patients with T1D duration of 5 to 9 years tested positive for these antibodies, as did 66.67% of patients with 10 or more years of T1D).
| Table 7. Distribution of antithyroid antibodies by duration of type 1 diabetes mellitus | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Disease duration (years) | Antithyroid antibodies | |||||||||||
| Antithyroglobulin (n = 25) | Antithyroperoxidase (n = 25) | Both (n = 25) | ||||||||||
| Positive | Negative | Positive | Negative | Positive | Negative | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| 0-4 (n =-8) | 2 | 8.0 | 6 | 24.0 | 5 | 20.0 | 3 | 12.0 | 1 | 11.11 | 1 | 11.11 |
| 5-9 (n-= 14) | 4 | 16.0 | 10 | 40.0 | 14 | 56.0 | - | - | 4 | 44.44 | - | - |
| ≥ 10 (n = 3) | 1 | 4.0 | 2 | 8.0 | 2 | 8.0 | 1 | 4.0 | 1 | 11.11 | 2 | 22.22 |
| Total | 7 | 28.0 | 18 | 72.0 | 20 | 84.0 | 5 | 16.0 | 6 | 66.67 | 3 | 33.33 |
| χ2 = 0.0803; P = .9606 | χ2 = 6.0888; P = .0476 | χ2 = 3.7500; P = .1534 | ||||||||||
DISCUSSION
Type 1 diabetes is often associated to other diseases of immune aetiology, the most prevalent of which is autoimmune thyroid disease. Both are endocrine gland diseases caused by the stimulation of organ-specific T-cells. The association of these two diseases is most frequently found in patients with a genetic predisposition, such as carriers of the HLA-DR3 haplotype, among who an important number of those with T1D test positive for antithyroid antibodies. Of the latter, up to 50% progress to autoimmune thyroid diseases, most frequently to primary hypothyroidism, which is found in 2% to 5% of patients with T1D.8 Chronic autoimmune thyroiditis is characterised by the presence of specific antithyroid antibodies in serum, which are detected in 10% to 12% of the general population and in 3% to 50% of children with T1D depending on the degree of thyroid dysfunction.11,12
The study by Baena8 showed a high prevalence of autoimmune thyroid disease in patients with T1D (17%). However, this result is similar to the findings reported by other authors11,12 in international studies, most of them performed in the paediatric population, in which the prevalence of autoimmune thyroid disease ranges between 15.8 and 43.7%.8 The study by Rivera11 showed that out of all the patients with diabetes, there was a higher proportion of the female sex of 52.6% (P < .019) and a significant predominance of adolescents, who amounted to 52.6% (P < .001), which is consistent with the national 12,13 and international14,15 literature, which supports the findings of that study. In the study by Rivera,11 nine patients, or 9.3%, received a diagnosis of autoimmune thyroid disease, a majority of who were adolescents. Of the nine patients with autoimmune thyroid disease, six had Hashimoto thyroiditis in the euthyroid phase, and three in the hypothyroid phase, which diverges from the findings of Briceño et al.12 at the national level and Barker et al.15 at the international level, who find a statistically significant predominance of hypothyroidism.
In a study of 90 patients with T1D, Baena et al.8 found that 17.8% of the total had a known autoimmune thyroid disease which corresponded, in order of decreasing frequency, to primary hypothyroidism (9.9%), subclinical hypothyroidism (7.1%) and Graves disease (0.8%). In the study by Miraval León,16 the most frequent thyroid disorder was clinical hypothyroidism, with a prevalence of 84.4%, which was higher than the prevalence reported in other studies14,16 but consistent with the international medical literature.17
The percentage of subclinical hypothyroidism in patients that underwent a hormone screen was 2.5%, lesser than that reported in other studies.14,16 Johnson et al.18 reported a prevalence of up to 50%, and Gronich17 found a percentage of subclinical hypothyroidism of 8.6% in Australian women, despite the fact that this was not the thyroid disorder found most frequently in the study.
In the study conducted in our hospital, we found that hypothyroidism was the most frequent autoimmune thyroid disease, followed by subclinical hypothyroidism in adolescent and in female patients, which was consistent with the reviewed medical literature. We found no cases of increased thyroid activity (hyperthyroidism).
As for the association with the nutritional status of patients with T1D, which was analysed by Rivera,11 77.2% had normal weight, 6.2% obesity, 6.2% chronic malnutrition, 5.2% overweight and 5.2% acute malnutrition. This was consistent with the description at the national level of Briceño et al.,12 whose study of the distribution of nutritional status based on the presence of thyroid disease showed that out of 9 female patients with thyroiditis, 7 had normal weight. Kordonouri et al.14 found no differences in growth or weight between patients with and without autoimmune thyroiditis. In the study conducted in our hospital, the majority of patients had normal weight, although part of them had hypothyroidism. This was consistent with what had been described in the reviewed medical literature.
In terms of the duration of T1D, the study by Rivera11 found a duration of at least 4 years in the majority of patients, which corresponded to 44.3%; of the 9 patients under study, 6 had a thyroid disorder, Hashimoto thyroiditis, in the euthyroid phase in 3 and the hypothyroid phase in the other 3. This diverged from the findings of the nationwide study by Martín,13 which found that diabetes mellitus had been diagnosed less than 3 years prior in more than half of the patients (51.2%), but was consistent with the findings of Kordonouri14 and Barker,15 who reported a longer duration of diabetes mellitus in patients with autoimmune thyroid disease. However, in opposition to other works,12,14,15 the study by Baena8 did not find an association between duration of diabetes and the presence of autoimmune thyroid disorder; although it did find an increased prevalence of autoimmune thyroid disease in female patients (24.6% compared to 10.8% of male patients). This study found a significant difference, with an increased prevalence of thyroid dysfunction with increasing T1D duration.
Positive detection of specific antithyroid antibodies has been reported in a larger proportion of paediatric patients with T1D compared to the general population, with the percentage of positive results ranging from 7% to 40%. Antithyroid antibody titres are higher in patients with more years of T1D. The main antibodies that mediate the autoimmune thyroid response are the following: antithyroglobulin, anti-TSH receptor, anti-thyroid hormone and antithyroperoxidase. The latter is found in every type of autoimmune thyroid disease, reaching the highest titres in Hashimoto thyroiditis, even in cases in which tests for other antithyroid antibodies are negative. This antigen (antithyroperoxidase antigen) targets thyroid peroxidase, an enzyme that catalyses the iodination of tyrosine residues in thyroglobulin and that is located both in the cytoplasm and in the apical membrane of thyroid cells. These antibodies are responsible for the complement-dependent cytotoxicity observed in thyroiditis.19 In relation to this, we ought to highlight the study by Kordonouri14 that included 7097 patients with T1D, with a mean age of 12 years, a 15.8% prevalence of thyroid disease and a 21.6% prevalence of positive antithyroid antibody detection.
It is well known that in patients with T1D, the main marker of risk of future thyroid disease is the development of antithyroid antibodies (antithyroperoxidase, antithyroglobulin and thyroid-stimulating immunoglobulins).8 Thus, there is evidence that patients who test positive for antithyroid antibodies have a risk up to 18 times greater of future thyroid disease, although primary hypothyroidism can also occur in up to 20% to 30% of patients with negative results for antithyroid antibodies; the study by Baena8 obtained very similar data, with 25.6% of patients with autoimmune thyroid disease having negative antithyroid antibody test results. On the other hand, while it seems that the prevalence of thyroid disease increases with age and with duration of diabetes, there is no published evidence of an increased prevalence in patients with poor metabolic control, although few studies have analysed this association. Barker15 conducted a study that found that antithyroid antibody test results were most frequent in female patients (58%; P < .0001) and adolescents (16.1 years; P < .0013).
In the study by Rivera,11 of the patients that underwent measurement of antithyroperoxidase levels, only 6 (11.2%) had positive results, of who 4 (66.7%) had Hashimoto thyroiditis in the euthyroid phase and 2 (33.3%) in the hypothyroid phase. At the national level, Briceño12 obtained similar findings in relation to antithyroid antibodies, which were negative in 126 patients (86.3%) and positive in 12.7%. At the international level, Glastras20 found positive antithyroperoxidase antibodies in 13 out of 166 patients (7.8%); 6 of the 13 patients (46.2%) who tested positive for antithyroperoxidase antibodies at the time of diagnosis developed thyroid disease, compared to only 3.6% of patients with negative results; the study by Baena8 found different results, with only 41.1% of patients testing positive for antithyroperoxidase antibodies and 25.6% testing negative; there were no data for the remaining 33.3% of patients.
When it came to antithyroid antibody tests in our study, the results were only positive and associated with the duration of autoimmune thyroid disease for antithyroperoxidase levels, which was not the case for antithyroglobulin levels or the detection of both antibodies, for which we did not find a statistically significant association with the duration of disease. There was a higher proportion of the female sex in patients with positive antithyroperoxidase results, although this predominance was not statistically significant our results were similar to those reported in the reviewed medical literature.
CONCLUSIONS
We found autoimmune thyroid disease in adolescents with type 1 diabetes mellitus.
Thyroid dysfunction in adolescents with autoimmune thyroid disease manifested with clinical and subclinical hypothyroidism and was associated with age and duration of T1D.
The presence of antithyroperoxidase antibodies was associated with age and duration of T1D, but not with sex. We found no association between antithyroglobulin levels and any of the variables under study.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation or publication of this article.
ABBREVIATIONS
T1D: type 1 diabetes mellitus • T3: triiodothyronine • T4: thyroxine • TSH: thyroid-stimulating hormone.
REFERENCES
- Camacho B, Manzanares A, Espino R. Debut de diabetes mellitus tipo 1 en el área hospitalaria de Valme. Vox Paediatr. 2012;19:9-13.
- Asenjo S, Muzzo S, Pérez MV, Ugarte F, Willshaw ME. Consenso en el diagnóstico y tratamiento de la diabetes tipo 1 del niño y del adolescente. Rev Chil Pediatr. 2007;78:534-41.
- Soltész G. La diabetes en niños: tendencias cambiantes dentro de una epidemia emergente. Diabetes Voice. 2007;52:13-5.
- Braverman Bronstein A, Rendón Macías ME, Iglesias Leboreiro J, Bernárdez Zapata I, Antillón Ferreira C. Características clínicas y de laboratorio en niños con diabetes mellitus. Rev Mex Pediatr. 2013;80;200-5.
- Curell Aguilá N. Hipotiroidismo en adolescentes. Adolescere. 2013;12:24-31.
- Chueca Guindulain M, Berrade Zubiri S, Dura Travé T, Oyarzábal Irigoyen M. Hipotiroidismo subclínico en la infancia y adolescencia. Rev Esp Endocrinol Pediatr. 2014;5:49-57.
- Valdés Alonso MC. Síndrome poliglandular autoinmune. In: Coto Hermosilla C. Reumatología Pediátrica. Havana: Editorial Ciencias Médicas; 2012. p. 412-36.
- Baena MG, Carral F, Roca MM, Cayón M, Ortego J, Aguilar-Diosdado M. Prevalencia de la enfermedad tiroidea autoinmune en pacientes con diabetes mellitus tipo 1. Av Diabetol. 2010;26:42-6.
- Jordan JR. Desarrollo humano en Cuba. Havana: Editorial Científico-Técnica; 1979.
- Esquivel M, Rubí A. Curvas nacionales de peso y talla. Su interpretación y uso en la valoración del estado nutricional. Rev Cubana Pediatr. 1985;57:377-83.
- Rivera N. Enfermedad tiroidea autoinmune en pacientes con diabetes mellitus tipo 1. Consulta de Endocrinología Pediátrica. Hospital de Niños Dr. Jorge Lizarraga. Valencia, junio 2009-2012. Valencia, Venezuela: Universidad de Carabobo; 2013.
- Briceño Y, Paoli M, Maulino N, Gaffaro L, Marcano H, Pérez M. Dislipidemia y disfunción tiroidea en niños y adolescentes con diabetes mellitus tipo1: relación con el control metabólico e índice de masa corporal. Rev Venez Endocrinol Metab. 2009;7:23-8.
- Martín R. Frecuencia de trastornos de la función tiroidea en escolares y adolescentes con diabetes mellitus Consulta de Endocrinología. Hospital Pediátrico Dr. Agustín Zubillaga. Barquisimeto, Venezuela: Universidad Centro Occidental Lisandro Alvarado; 2007.
- Kordonouri O, Klinghammer A, Lang EB, Gruters-Kieslich A, Grabert M, Holl RW. Thiyroid autoimmunity in children and adolescents with type 1 diabetes: a multicenter survey. Diabetes Care. 2002;25:1346-50.
- Barker JM, Yu J, Yu L, Wang J, Miao D, Bao F, et al. Autoantibody “subspecificity” in type 1 diabetes: risk for organ specific autoimmunity clusters in distinct groups. Diabetes Care. 2005;28:850-5.
- Miraval León LJ. La disfunción tiroidea en pacientes con diabetes mellitus tipo 2. Hospital Nacional Dos de Mayo 2013-2015. Thesis. Lima: Universidad Nacional Mayor de San Marcos; 2016.
- Gronich N, Deftereos SN, Lavi I, Persidis AS, Abernethy DR, Rennert G. Hypothyroidism is a risk factor for new-onset diabetes: a cohort study. Diabetes Care. 2015;38:1657-64.
- Johnson J. Diabetes control in thyroid disease. Diabetes Spectrum. 2006;19:148-53.
- Rivero Escalante H, Dorantes Álvarez LM, García Morales L, Coyote Estrada N, Martínez Duncker C, Palafox Vázquez H, et al. Frecuencia de enfermedad tiroidea autoinmune en niños con diabetes mellitus tipo 1. Bol Med Hosp Infant Mex. 2001;58:627-34.
- Glastras SJ, Craig ME, Verge CF, Chan AK, Cusumano JM, Donaghue KC. The role of autoimmunity at diagnosis of type 1 diabetes in the development of thyroid and celiac disease and microvascular complications. Diabetes Care. 2005;28:2170-5.
Comments
This article has no comments yet.