

Estado de ánimo de los adolescentes y su relación con conductas de riesgo y otras variables
Marta Esther Vázquez Fernándeza, M.ª Fe Muñoz Morenob, Ana Fierro Urturic, M Alfaro Gonzálezd, L Molinero Rodrígueze, P Bustamante Marcosf
aPediatra. CS Arturo Eyries. Facultad de Medicina. Universidad de Valladolid. Valladolid. España.
bUnidad de Investigación Biomédica. Hospital Clínico Universitario de Valladolid. Valladolid. España.
cPediatra. CS Pisuerga. Arroyo de la Encomienda. Valladolid. España.
dServicio de Pediatra. Hospital de Medina del Campo. Medina del Campo. Valladolid. España.
ePediatra. CS Casa del Barco. Valladolid. España.
fMIR-MFyC. CS Arturo Eyries. Valladolid. España.
Correspondencia: ME Vázquez. Correo electrónico: mvmarvazfer@gmail.com
Cómo citar este artículo: Vázquez Fernández ME, Muñoz Moreno MF, Fierro Urturi A, Alfaro González M, Molinero Rodríguez L, Bustamante Marcos P. Estado de ánimo de los adolescentes y su relación con conductas de riesgo y otras variables. Rev Pediatr Aten Primaria. 2013;15:219.e75-e84.
Publicado en Internet: 04-09-2013 - Número de visitas: 32669
Resumen
Introducción: la adolescencia es una etapa de la vida en la que se desarrollan nuevas capacidades mentales que permiten a los adolescentes construir sus propias ideas y adoptar estilos de vida. En este trabajo se describen los estados de ánimo y los factores relacionados.
Métodos: se realizó una encuesta a una muestra de 2412 escolares de 13 a 18 años de edad de la provincia de Valladolid, matriculados en centros educativos con segundo, tercero y cuarto de Enseñanza Secundaria Obligatoria y primero y segundo de Bachillerato LOGSE. Se consideraron seis aspectos del estado de ánimo para clasificarlo como positivo o negativo. Se ha analizado, mediante un modelo de regresión logística, la asociación entre los estados de ánimo negativos y los factores sociodemográficos, económicos y las conductas de riesgo.
Resultados: la frecuencia de estado de ánimo negativo fue del 14,9%, más alta en el sexo femenino –16,9% (odds ratio [OR]: 1,63; intervalo de confianza del 95% [IC 95%]: 1,23 a 2,15; p=0,001)– y en los que cursaban segundo de Bachillerato –20,7% (OR: 1,95; IC 95%: 1,29 a 2,97; p=0,002)–.
Se ha encontrado asociación de estados mentales negativos con situaciones familiares distintas a la no convivencia con el padre, la madre y/o hermanos y con no tener trabajo remunerado el padre y la madre. También se relacionan con tener notas peores que la media, agobiarse por no tener conexión a Internet, acceso frecuente a fotos o vídeos de contenido sexual, robar, sentirse maltratado física o psicológicamente, haber sufrido acoso sexual o tener un peso por encima de lo normal.
Como factores de protección estaría tener hermanos, siendo estadísticamente significativa la categoría de dos o más.
Conclusiones: la prevalencia de problemas mentales en adolescentes observada en nuestro estudio es similar de manera global a otros trabajos y menor en el sexo femenino. Diversas variables sociodemográficas, económicas y conductas de riesgo se asocian a estados de ánimo negativos. La valoración de estos aspectos en la consulta puede ser útil para detectar adolescentes de riesgo.
Palabras clave
● Adolescencia ● Conductas de riesgo ● Estados de ánimo ● Factores socioeconómicosINTRODUCCIÓN
La adolescencia es una etapa crítica de la vida porque se inician determinados comportamientos de riesgo. Los cambios físicos y hormonales, junto a las trasformaciones sociales, son factores influyentes1,2. Para poder monitorizar estas conductas con repercusión en la salud se utilizan encuestas de aplicación sistemática que nos permiten obtener datos válidos3.
Aunque la salud mental (de desarrollo, emocional, de conducta…) no se reconoce en muchas ocasiones como un problema de salud que requiere atención médica, el adolescente es especialmente sensible a estos problemas4,5. Existen estudios que han identificado factores demográficos, económicos, condiciones familiares de carencia afectiva o de ausencia de modelos adultos equilibrados, que pueden tener influencia en los estados de ánimo de los adolescentes6,7. Además, estos influyen en el uso de sustancias adictivas, en las prácticas sexuales, en la dieta, en la actividad física, en la experiencia con el acoso o en las conductas violentas8,9. Pese a ello, la relación es compleja y los estudios escasos. Los pediatras y médicos de familia que atendemos a adolescentes no podemos permanecer ajenos a estos aspectos que condicionan el estado de salud, bienestar y las conductas de riesgo. Es importante ayudar a los adolescentes a aprender los mecanismos psicológicos de adaptación que les van a ayudar a relacionarse de forma satisfactoria y a proteger su salud1.
En este artículo se muestran los resultados obtenidos de un estudio sobre hábitos, comportamientos y conductas relacionadas con la salud, realizado en una muestra de estudiantes de 13 a 18 años de edad de la provincia de Valladolid entre marzo y mayo del año 2012, extrayendo datos relacionados con el estado de ánimo de los escolares. El objetivo principal de este trabajo es describir el estado de ánimo de los adolescentes. Los objetivos secundarios son encontrar asociación entre el estado anímico y algunas variables sociodemográficas, hábitos, actitudes y conductas de riesgo analizadas.
MATERIAL Y MÉTODOS
Diseño
Se ha realizado un estudio descriptivo trasversal. La población de estudio han sido los adolescentes de 13 a 18 años de edad de la provincia de Valladolid (España) matriculados en centros educativos con segundo, tercero y cuarto de Enseñanza Secundaria Obligatoria (ESO), primero y segundo de Bachillerato LOGSE.
El número de alumnos obtenido a partir de los listados de la Consejería de Educación, de la Federación Española de Religiosos de la Enseñanza (FERE) y directamente de los colegios privados de Valladolid, fue 18 888 escolares.
La selección de los alumnos se realizó mediante muestreo bietápico por conglomerados, seleccionando aleatoriamente colegios (n=14) en una primera etapa y aulas en la segunda. Posteriormente, se incluyó a todos los estudiantes de las aulas seleccionadas.
El tamaño muestral se calculó para una proporción estimada de un 50% y una precisión del 2,5% en un contraste bilateral, asumiendo un 10% de falta de respuestas, resultando 1566 alumnos. El número final de alumnos encuestados, después de depurar los datos y eliminar encuestas que no estaban cumplimentadas en su totalidad, fue de 2412 adolescentes escolarizados de 13 a 18 años, por lo que se cumplieron ampliamente las cifras de partida.
Se contactó telefónicamente y por correo con los directores de los colegios y se les informó sobre los objetivos y contenidos del estudio, acordando uno o varios días (no precedidos de vacaciones) para la realización de la encuesta entre marzo y mayo de 2012. Tres colegios rehusaron participar sin dar una razón clara. Los colegios notificaron a las familias de los alumnos que se les iba a hacer participar en la encuesta, dando la opción de rechazarlo sin consecuencias.
El equipo investigador fue el encargado de administrar la encuesta. En el 69% de la muestra se utilizó el cuestionario asistido por ordenador y en el resto el cuestionario en formato papel, por no disponer de suficiente número de ordenadores en las aulas de informática. Los datos informáticos quedaron automáticamente recogidos en la base de datos, los realizados en papel fueron introducidos manualmente en la misma.
Los alumnos seleccionados cumplimentaron los cuestionarios de forma personal, avisados previamente de la confidencialidad de los datos y de que no debía existir comunicación entre ellos. La realización de la encuesta fue voluntaria, durante el horario escolar habitual. El tiempo aproximado utilizado para responder fue de 35-40 minutos. El diseño del proyecto fue aprobado por la Comisión de Investigación de la Gerencia de Atención Primaria del Área Oeste de Valladolid.
Recogida de datos
El cuestionario recogía, entre otras, además de preguntas relacionadas con el estado de ánimo de los adolescentes, cuestiones sobre variables sociodemográficas, rendimiento escolar (notas y repetición de curso), tiempo libre (ver la televisión, navegar por Internet), accidentes, tabaco (han fumado alguna vez o a diario), alcohol (han bebido alguna vez o se han emborrachado más de dos veces en los últimos 12 meses), drogas (las han probado o consumen porros a diario), conducta antisocial (hacen novillos o roban cosas), experiencia sobre el maltrato y las relaciones con los demás (maltrato psicológico, físico, acoso o abuso sexual y participación en intimidación a otros), alimentación (fruta a diario y peso por encima de lo normal) y sexualidad (relaciones sexuales con penetración y utilización de la píldora del día después), basadas en las recomendaciones de los programas internacionales10,11, nacionales12,13 y de distintas provincias y comunidades autónomas14-18.
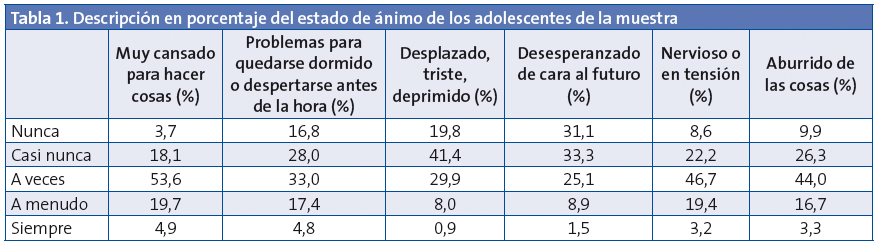
Siguiendo el modelo de Ahonen et al.8, se consideraron seis aspectos del estado de ánimo: a) sentirse cansado; b) tener problemas para dormirse o despertarse; c) desplazado, triste o deprimido; d) desesperanzado de cara al futuro; e) nervioso o en tensión, y f) sentirse aburrido.
Las categorías de respuestas según la escala de Likert fueron: nunca, casi nunca, a veces, a menudo y siempre. Se consideró un estado de ánimo negativo cuando respondía siempre y a menudo en tres o más de los seis ítems, siguiendo el modelo de trabajo catalán, informe FRESC de Barcelona14, adaptado a su vez del estudio HBSC a nivel nacional13.
Análisis estadístico
Las variables cuantitativas se presentan con los valores medios y el intervalo de confianza del 95% (IC 95%) y las cualitativas según su distribución de frecuencias.
Para analizar la asociación entre el estado de ánimo, las características sociodemográficas y los factores de riesgo se ha utilizado el test Chi-cuadrado de Pearson. En el caso de que el número de celdas con valores esperados menores de cinco sean mayores de un 20%, se ha utilizado el test exacto de Fisher o el test Razón de verosimilitud para variables con más de dos categorías.
Las variables que estadísticamente eran significativas a nivel 0,1 en el análisis de regresión logística univariante han sido incluidas en un modelo multivariante ajustando por las variables de confusión.
Los datos han sido analizados con el programa estadístico SPSS® versión 19.0 para Windows®. Los valores de p<0,05 han sido considerados estadísticamente significativos.
RESULTADOS
El número total de encuestas validadas fue de 2412 adolescentes entre 13 y 18 años de la provincia de Valladolid (España).
Las características del estado de ánimo se pueden ver en la Tabla 1. Destaca sobre todo que el 24,6% declara estar siempre o a menudo muy cansado/a para hacer cosas, seguido de nervioso/a o en tensión (22,6%) y de los problemas para quedarse dormido/a o despertarse antes de la hora (22,2%).
La prevalencia de estado de ánimo negativo, considerado como respuesta “siempre o a menudo” en tres o más de los seis aspectos valorados, fue globalmente del 14,9%. La Tabla 2 resume los principales resultados del estado anímico relacionados con las variables sociodemográficas de la población adolescente estudiada. El análisis bivariado de los diversos factores con el estado de ánimo negativo mostró diferencias estadísticamente significativas en función del sexo, el curso, el tipo de colegio, el hábitat del colegio, el tipo de convivencia familiar y el trabajo de los padres fuera de la casa.
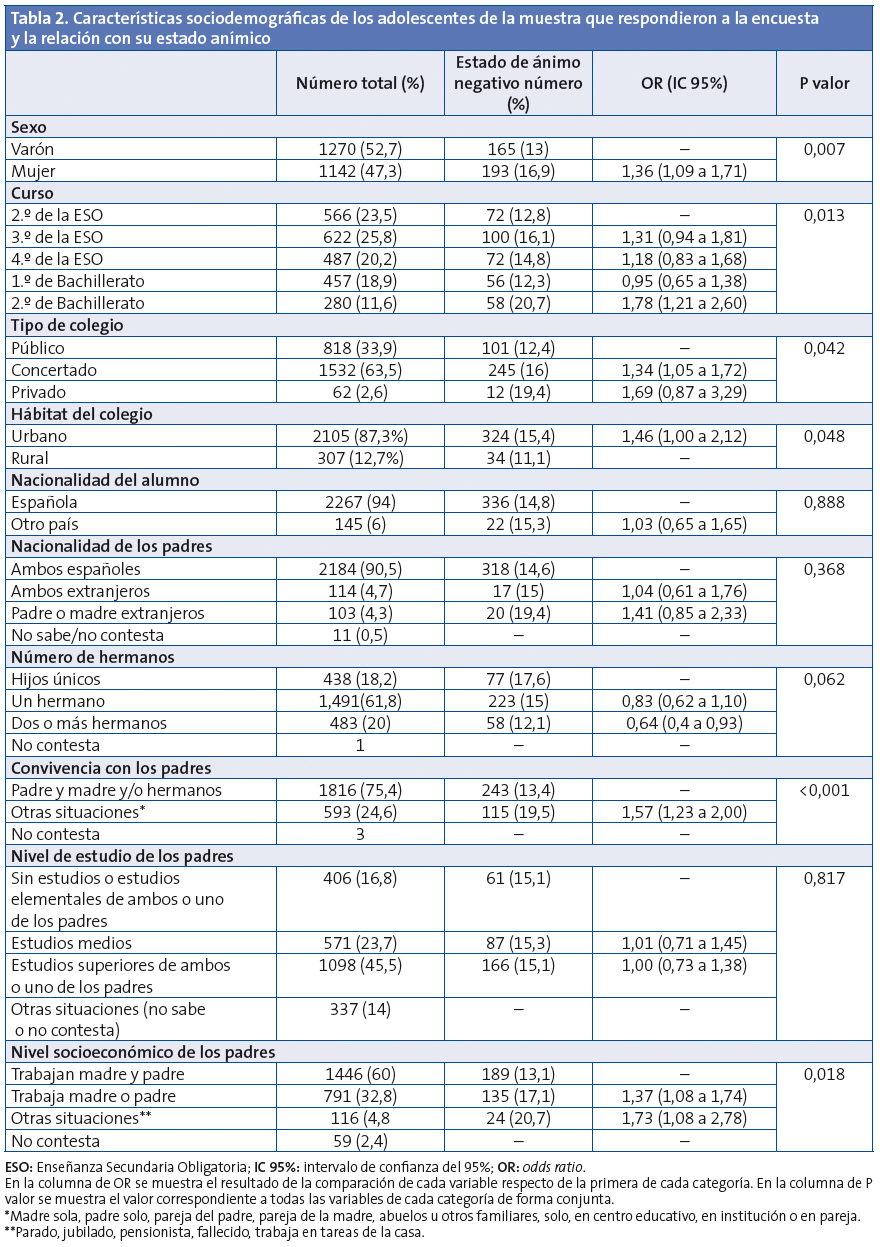
La proporción de niñas que se sentían con tres o más problemas del estado de ánimo fue del 16,9% (odds ratio [OR]: 1,36; IC 95%: 1,09 a 1,71). Los escolares de segundo de Bachillerato fueron los que manifestaron más problemas de ánimo 20,7% (OR: 1,78; IC 95%: 1,22 a 2,60, tomando como referencia los de segundo de la ESO). El colegio privado y el hábitat urbano se asociaron a un incremento del estado de ánimo negativo, alcanzando diferencias estadísticamente significativas (p=0,042 y p=0,048, respectivamente). Por el contrario, factores socioeconómicos de los padres como el trabajo de los dos progenitores y el modelo de convivencia más habitual del padre, la madre y/o hermanos se presentan como factores de menor riesgo para el estado de ánimo negativo. Otro factor adicionalmente vinculado al estado de ánimo negativo es ser hijo único, frente a tener uno, dos o más hermanos. No aparece asociación con la nacionalidad de los padres o del alumno, ni con el nivel de estudio de los padres.
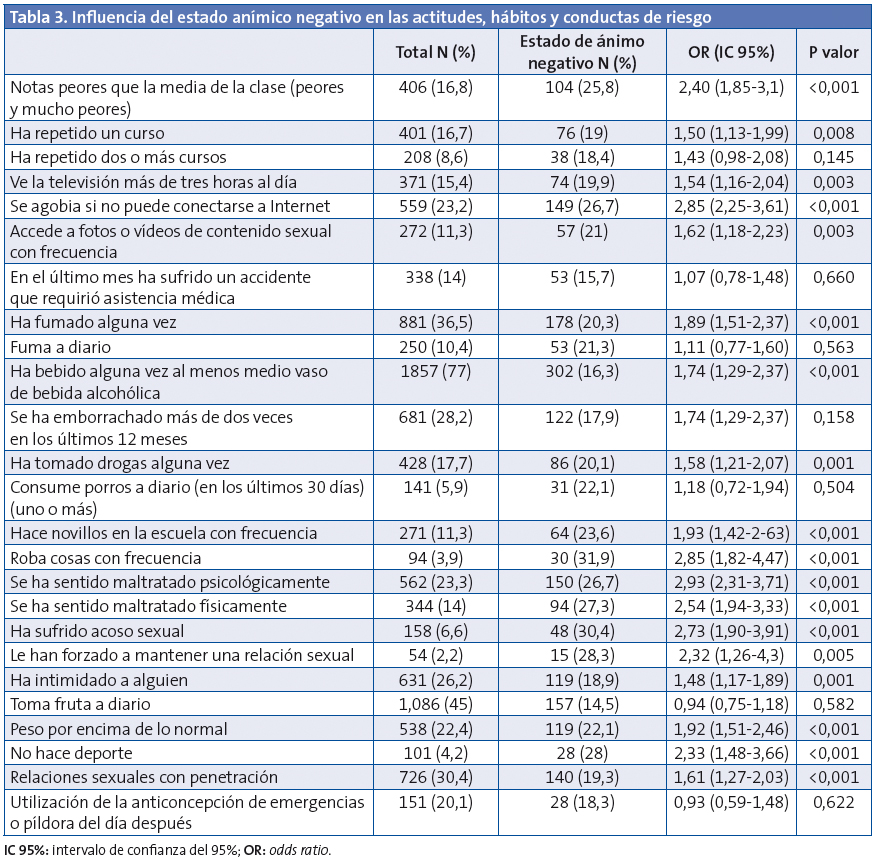
La Tabla 3 resume la frecuencia de los hábitos, conductas y actitudes de riesgo de los adolescentes encuestados, así como el análisis bivariante de estos con el estado de ánimo negativo. De esta manera encontramos asociación estadísticamente significativa y una OR por encima de 1, con la mayoría de las variables de riesgo. Sin embargo, no se encuentra asociación con repetir dos o más cursos, haber sufrido un accidente, fumar a diario, emborracharse con frecuencia, consumir porros a diario, tomar fruta diariamente y la utilización de la píldora del día después.
En el modelo de regresión logística multivariante (Tabla 4), en los resultados para la OR ajustada vemos que presentan mayor riesgo de estado de ánimo negativo las chicas, en segundo de Bachillerato, con situaciones familiares distintas a convivir con el padre, la madre y/o los hermanos, con la situaciones laborales en las que no trabajan el padre y la madre, con tener notas peores que la media, con dependencia de Internet y acceso con frecuencia a fotos o vídeos de contenido sexual, con robar cosas con frecuencia, sentirse maltratado física o psicológicamente, haber sufrido acoso sexual o tener un peso por encima de lo normal.
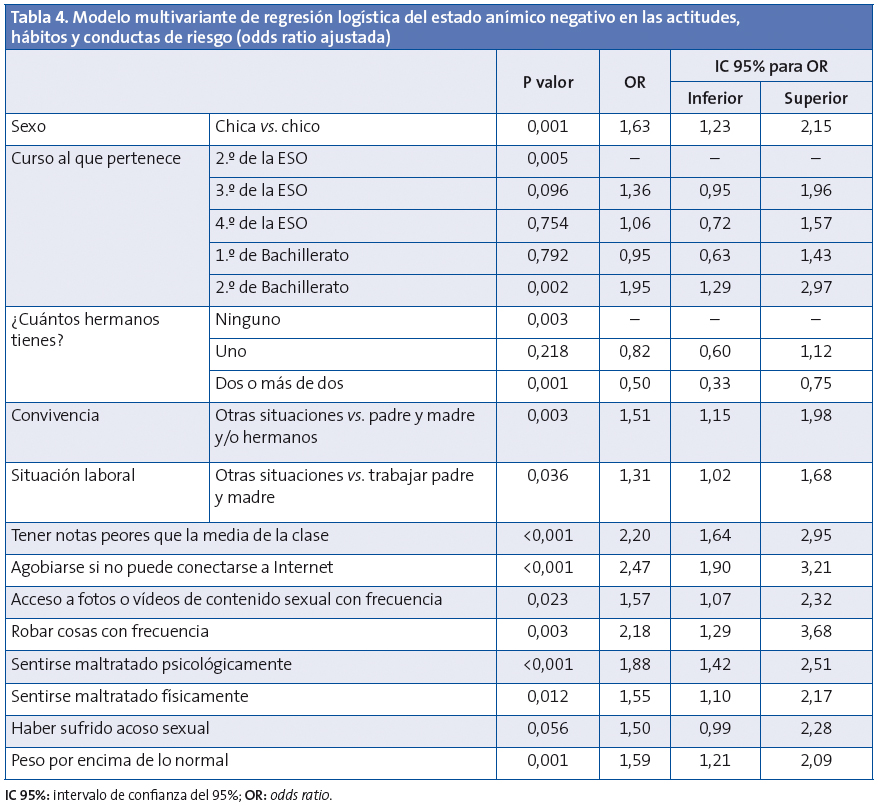
Como factores de protección estaría tener hermanos, siendo estadísticamente significativa la categoría de dos o más.
DISCUSIÓN
Aunque la salud mental no es sinónimo del estado de ánimo, la literatura se refiere con frecuencia a enfermedades como la ansiedad y la depresión6 como desencadenantes de conductas de riesgo. Este tipo de cuestionarios sobre el estado de ánimo de los adolescentes ya se ha aplicado con éxito en otros trabajos7,8. Nuestro estudio es un intento de complementar y corroborar los resultados obtenidos por otros autores.
Como limitaciones, destacamos que se trata de un estudio trasversal en el que determinamos como positivo o negativo el estado de ánimo en un momento determinado. Es muy probable que las personas experimenten variaciones del estado de ánimo a lo largo del tiempo, máxime los adolescentes, que experimentan cambios emocionales bruscos y extremos1. Pese a ello, la escala Lickert donde se incluyen los ítems “nunca”, “casi nunca”, “a veces”, “a menudo” y “siempre”, intenta diferenciar el estado ocasional de la experiencia más duradera.
Se estima que la prevalencia de trastornos mentales en los jóvenes europeos de 15-24 años está en torno al 20%. Entre el 10 y el 20% de los jóvenes españoles podría presentar problemas de salud mental19. Nuestro trabajo demuestra una frecuencia similar del estado de ánimo negativo (14,9%) entre los adolescentes de 13 a 18 años.
El sexo femenino y el aumento de edad durante la adolescencia han sido asociados al estado de ánimo negativo en diversos estudios8. Ahonen et al. refieren valores para las chicas del 21%, más altos que en nuestro estudio (16,9%), y similares para los chicos (en torno al 13%). Estos factores también se asocian a estados de ansiedad y depresión6 y a estados de “mala salud mental”12.
Respecto a los factores socioeconómicos, las investigaciones previas han mostrado que el bajo estatus se asocia con enfermedad mental. Sin embargo, no está claro cuáles son los más influyentes en la salud mental20. Además, conocer con exactitud la capacidad adquisitiva de los chicos y chicas es un proceso complicado, ya que es frecuente que desconozcan los estudios y la categoría laboral de los padres. En este estudio hemos encontrado asociación de estados mentales negativos con el colegio privado, el hábitat urbano, los modelos de convivencia no habituales o tradicionales (madre sola, padre solo, pareja del padre, pareja de la madre, abuelos u otros familiares, solo, en centro educativo, en institución o en pareja), las situaciones en las que uno o ambos padres están sin trabajo remunerado y, en menor medida, ser hijo único. Como factor de protección, asociado a estados anímicos positivos, estaría el tener dos o más hermanos. Aunque en el estudio de McLaughlin el nivel educativo de los padres se asocia con menor riesgo de trastornos de ansiedad20, en el nuestro este factor no parece influir en los problemas del estado de ánimo, de la misma manera que tampoco existe asociación con la nacionalidad de los padres y el alumno.
La conducta de riesgo de los adolescentes es un proceso muy complejo y multifactorial donde intervienen factores diversos. A mayor número de factores, mayor riesgo21, estudios previos han demostrado asociación entre determinadas prácticas sexuales22, alimentación y ejercicio físico23, la violencia24 y el acoso escolar9, con determinados estados de salud mental. Algunos han establecido relación entre la depresión y el consumo de tabaco25 y de drogas26.
Hemos seleccionado las conductas de mayor riesgo y analizado la probabilidad de que el estado anímico se asocie o las propicie. La mayoría de hábitos y conductas de riesgo se asocian al estado negativo. Pero destacamos que los adolescentes con experiencias y hábitos como repetir curso más de dos veces, fumar a diario, emborracharse con frecuencia y consumir cannabis a diario no presentan demasiada asociación con estados anímicos negativos. Parece que las conductas de riesgo más establecidas y peligrosas se asocian a adolescentes con estados anímicos más positivos, mientras que las conductas intermedias o de prueba, como repetir un solo curso, fumar y beber alguna vez, se dan más en estados negativos, pudiendo ser estos el inicio de esos hábitos. No es el caso de las situaciones de tener peores notas que la media, la dependencia de Internet con acceso a contenidos sexuales, las conductas antisociales como robar y hacer novillos en la escuela, tener un peso por encima de lo normal y sentirse maltratado (física, psíquica y sexualmente) donde se observa una clara relación con los problemas del ánimo.
Conclusiones
- Hemos encontrado frecuencias similares a otros trabajos de estado anímico negativo en la población adolescente masculina y algo más bajo en la femenina.
- La prevalencia del estado de ánimo negativo aumenta con la edad.
- Los problemas mentales se asocian a diversas variables sociodemográficas y económicas.
- Determinados hábitos y conductas de riesgo se relacionan con estados de ánimo negativos.
- El profesional debe sospechar y reconocer los problemas de salud mental. La valoración en la consulta mediante una adecuada historia clínica en un ambiente de confianza y confidencialidad puede ser útil para la detección de adolescentes en riesgo de adoptar, o incluso que se hayan iniciado, estilos de vida no saludables, con el fin de dirigirlos a programas preventivos específicos.
AGRADECIMIENTOS
A los centros educativos (directores, profesores, orientadores y alumnos), por la colaboración que han prestado para llevar a cabo la encuesta. Al grupo Educación para la Salud de la Asociación Española de Pediatría de Atención Primaria (AEPap) por su interés y ayuda en la consecución del proyecto. A la Directiva de la AEPap, por la confianza mostrada y la ayuda económica que ha permitido su realización.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
FUENTE DE FINANCIACIÓN
Este trabajo ha sido financiado por la AEPap.
ABREVIATURAS: AEPap: Asociación Española de Pediatría de Atención Primaria • ESO: Enseñanza Secundaria Obligatoria• IC 95%: intervalo de confianza del 95% • OR: odds ratio.
BIBLIOGRAFÍA
- Ruiz Lázaro PJ. Promoviendo la adaptación saludable de nuestros adolescentes. Proyecto de promoción de la salud mental para adolescentes y padres de adolescentes. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad; 2004 [en línea] [consultado el 09/11/2012]. Disponible en http://bit.ly/VXRRr2
- Hidalgo Vicario MI, Júdez Gutiérrez J. Adolescencia de alto riesgo. Consumo de drogas y conductas delictivas. Pediatr Integral. 2007;11:895-910.
- Centers for Disease Control and Prevention. Methodology of the Youth Risk Behaviours Surveillence System; 2004 [en línea]. Disponible en www.cdc.gov/mmwr/preview/mmwrhtml/rr5312a1.htm
- Terry PC, Lane AM, Lane HJ, Keohane L. Development and validation of a mood measure for adolescents. J Sports Sci. 1999:17(11):861-72.
- Ras Vidal E, Briones Carcedo O. Los trastornos de ánimo en los adolescentes de un centro de atención primaria. Aten Primaria. 2004;34:565.
- Saluja G, Iachan R, Scheidt PC, Overpeck MD, Sun W, Giedd JN. Prevalence of and risk factors for depressive symptoms among young adolescents. Arch Pediatr Adolesc Med. 2004;158:760-5.
- Monteagudo M, Rodriguez-Blanco T, Pueyo MA, Zabaleta-Del-Olmo E, Mercader M, García J, et al. Gender differences in negative mood states in secondary school students: health survey in Catalonia (Spain). Gac Sanit. 2012;28. [Epub ahead of print].
- Ahonen E, Nebot M, Giménez E. Estados de ánimo negativos y los factores relacionados en una muestra de adolescentes de enseñanza secundaria de Barcelona (España). Gac Sanit. 2007;21:43-52.
- García Continente X, Pérez Giménez A, Nebot Adell M. Factores relacionados con el acoso escolar (bullying) en los adolescentes de Barcelona (Spain). Gac Sanit. 2010;24:103-8.
- Brooks F, Van der Sluijs W, Klemera E, Morgan A, Magnusson J, Gabhainn SC, et al. Young People’s Health in Great Britain and Ireland. Findings from the Health Behaviour in School-Aged Children Study. HBSC International Coordinating Centre. University of Edinburgh; 2006.
- University of California. Adolescent Questionnaire. California Health Interview Survey. CHIS 2010 [en línea]. Disponible en www.chis.ucla.edu
- Encuesta nacional de salud de España. Madrid: Ministerio de Sanidad, Política Social e Igualdad; 2006 [en línea]. Disponible en www.msps.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm
- Moreno-Rodríguez C, Muñoz Tinoco V, Pérez Moreno PJ, Sánchez Queija I, Granado Alcon MC, Ramos Valverde P, et al. Desarrollo adolescente y salud. Resultados del estudio HBSC 2006 con chicos y chicas españoles de 11-17 años. Madrid: Ministerio de Sanidad y Consumo; 2008 [en línea]. Disponible en www.hbsc.es/castellano/inicio.html
- Nebot M, Pérez A, García-Continente X, Ariza C, Espelt A, Pasarín M, et al. Informe FRESC 2008. Resultats principals. Barcelona: Agència de Salut Pública de Barcelona; 2010.
- Encuesta de Salud Infantil en Asturias. Dirección General de Salud Pública y Participación de la Consejería de Salud y Servicios Sanitarios del Principado de Asturias. Observatorio de la Infancia y la Adolescencia del Principado de Asturias; 2009 [en línea]. Disponible en www.observatoriodelainfanciadeasturias.es
- Schiaffino A, Moncada A, Martín A. Estudi EMCSAT 2008. Conductes de salut de la població adolescent de Terrassa, 1993-2008. Terrassa: Ajuntament de Terrassa; 2009 [en línea] [consultado el 09/11/2012]. Disponible en www.terrassa.cat/files/319-5110-fitxer/informe_definitiu-salut.pdf?download=1
- Encuesta de Salud del País Vasco, 2007. Vitoria: Gobierno Vasco; 2008 [en línea] [consultado el 09/11/2012]. Disponible en http://bit.ly/VXRAo0
- Servicio de Epidemiología. Hábitos de salud en la población juvenil de la Comunidad de Madrid. Año 2008. Bol Epidemiol Comunidad Madrid. 2009;15(2):3-48 [en línea] [consultado el 09/11/2012]. Disponible en http://bit.ly/VXRfSm
- Hernán M, Fernández A, Ramos M. La salud en los jóvenes. Gac Sanit. 2004;18(Supl 1).
- McLaughlin KA, Costello EJ, Leblanc W, Sampson NA, Kessler RC. Socioeconomic Status and Adolescent Mental Disorders. Am J Public Health. 2012;102:1742-50.
- Igra V, Irwin Jr CE. Theories of adolescent risk-taking behavior. En: Diclemente RJ, Hansen WB, Ponton LE (eds.). Handbook of adolescent health risk behavior. New York: Plenum Press; 1996.
- Brooks TL, Harris SK, Trall JS, Woods ER. Association of adolescent risk behaviours with mental health symptoms in high school students. J Adolescent Health. 2002;14:280-5.
- Hassmen P, Koivulu N, Uutela A. Physical exercise and psychological well-being: a population study in Finland. Prev Med. 2000;30:17-25.
- Karnik NS, McMullin MA, Steiner H. Disruptive behaviors: conduct and oppositional disorders in adolescents. Adolesc Med. 2006;17:97-114.
- Brown RA, Lewinsohn PM, Seeley JR, Wargner EF. Cigarrette smoking, major depression, and other psychiatric disorders among adolescents. J Am Acad Child Adolesc Psychiatry. 1996;35:1602-10.
- Ceballos Rivera JJ, Ochoa Muñoz J, Cortez Pérez E. Depression in the adolescent. Its relationship with sports activities and drug consumption. Rev Med. 2000;38:371-9.