
Vol. 14 - Num. 53
Originales
Prevalencia de hábitos orales infantiles y su influencia en la dentición temporal
Virginia Franco Varasa, B Gorritxo Gilb, F García Izquierdoc
aProfesora asociada. Departamento Estomatología. Universidad del País Vasco. España.
bProfesora Titular. Departamento Estomatología. Universidad del País Vasco. España.
cOdontóloga. CS Laviada. Gijón. Asturias. España.
Correspondencia: V Franco. Correo electrónico: virfranva@hotmail.com
Cómo citar este artículo: Franco Varas V, Gorritxo Gil B, García Izquierdo F. Prevalencia de hábitos orales infantiles y su influencia en la dentición temporal. Rev Pediatr Aten Primaria. 2012;14:13-20.
Publicado en Internet: 13-04-2012 - Número de visitas: 97243
Resumen
Objetivos: conocer en una muestra de niños preescolares la prevalencia de los hábitos orales anómalos y la influencia de los de succión no nutritiva (chupete y dedo) en la dentición temporal.
Material y métodos: diseño: estudio epidemiológico observacional descriptivo de tipo transversal; emplazamiento: tres colegios del País Vasco; participantes: 225 niños de edades comprendidas entre los dos y los seis años, con dentición temporal completamente erupcionada.
Mediciones principales: los datos se han obtenido mediante un cuestionario de hábitos dirigido a los padres y las exploraciones clínicas realizadas a los niños, registrando la presencia de alteraciones de la oclusión, como mordida abierta anterior, aumento del resalte y mordida cruzada posterior.
Resultados: la prevalencia de hábitos orales nocivos en el conjunto de niños estudiados ha sido muy alta (90,7%). Los hábitos de succión no nutritiva (chupete, dedo) han resultado ser los más frecuentes (85,3%). Hemos encontrado un aumento significativo de las maloclusiones estudiadas cuando el hábito de succión se mantenía.
Conclusiones: los hábitos de succión no nutritiva influyen en el desarrollo de la dentición, por lo que se recomienda un abandono temprano de los mismos (antes de los dos años) para prevenir la aparición de maloclusiones dentales.
Palabras clave
● Dentición temporal ● Hábitos de succión no nutritiva ● MaloclusiónINTRODUCCIÓN
La succión es un reflejo que se desarrolla desde la vida intrauterina, a partir del periodo fetal. La presencia de este reflejo en el neonato es un signo de normalidad y su progresiva desaparición posterior hacia los cuatro meses también es un signo de normalidad evolutiva; de manera que la succión pasará de reflejo innato a reflejo adquirido o voluntario hacia el cuarto mes después del nacimiento1.
Para el bebé, la succión es primordial, pues ayuda a satisfacer las necesidades nutricionales y psicológicas. Sin embargo, su persistencia más allá de lo razonable puede tener serios efectos nocivos en el desarrollo de las estructuras bucales y deberíamos intentar que desaparezca2.
Entre los hábitos orales de succión no nutritiva, los más perjudiciales son el uso prolongado del chupete y la succión digital.
El grado y tipo de alteración que la presencia de estos hábitos producirá en la oclusión del niño variará en función del tipo de hábito, de su duración, intensidad y frecuencia, así como de las características biotipológicas del paciente2-4.
Existe una controversia interdisciplinar sobre el papel de los hábitos de succión en el desarrollo del niño, lo que hace necesario conocer su repercusión a nivel bucodental, como profesionales implicados en la salud integral del niño.
El objetivo del presente trabajo es determinar en una muestra de niños preescolares la prevalencia de los hábitos orales anómalos y su papel en la génesis de maloclusiones dentales en la dentición temporal.
MATERIAL Y MÉTODOS
Hemos realizado un estudio epidemiológico observacional descriptivo de tipo transversal sobre la prevalencia de hábitos orales en la muestra a estudiar y las maloclusiones asociadas a los hábitos de succión no nutritiva (succión de chupete y succión digital).
La muestra empleada para este estudio ha estado compuesta por niños de edades comprendidas entre los dos y los seis años, que se ajustaban a los criterios de inclusión/exclusión establecidos. Hemos incluido a todos los niños matriculados en 1.º, 2.º y 3.º de Educación Infantil de tres centros escolares de Vizcaya (n = 260).
Nuestros criterios de inclusión para la selección de la muestra han sido:
- Disponer del consentimiento de los padres o tutores.
- Erupción de la dentición temporal completa y en oclusión.
- Mostrar una conducta adecuada para la exploración.
Consideramos como criterios de exclusión los siguientes:
- Erupción de algún diente permanente.
- Padecer alguna patología sistémica significativa.
- Haber recibido en el pasado o estar recibiendo en ese momento cualquier tratamiento ortopédico u ortodóncico, a excepción de la colocación de un mantenedor de espacio debido a la pérdida prematura de algún molar temporal.
- Faltar algún registro en la exploración clínica o en el cuestionario de hábitos.
Siguiendo estos criterios, el tamaño final de la muestra seleccionada ha sido de 225 sujetos (124 niños y 101 niñas).
Elaboramos una carta de presentación del estudio a los colegios con la finalidad de informar sobre sus contenidos y solicitar su autorización y colaboración. Los datos se han obtenido a partir de los cuestionarios sobre hábitos orales que se han dirigido a los padres o tutores de cada niño. Se preguntaba por la presencia de succión digital, succión de chupete, interposición labial, succión de objetos, mordisqueo de uñas y deglución lingual. Hemos diseñado la ficha clínica de exploración, recogiendo los datos de filiación del niño y las maloclusiones a estudiar (resalte aumentado, mordida abierta anterior y mordida cruzada posterior). Siempre que fue posible se ha utilizado material de exploración desechable, estando el resto del material empleado en kits individuales embolsados estériles.
Con la autorización de los directores de cada centro, y a través de ellos, hemos enviado una circular a los padres de los niños incluyendo el cuestionario sobre hábitos orales.
Antes de llevar a cabo el trabajo de campo, se realizó un estudio piloto con el fin de comprobar si el método era adecuado y para estimar el tiempo necesario para cada exploración.
El examen clínico de la totalidad de los niños se ha llevado a cabo en los colegios por la misma exploradora.
Las variables analizadas y los criterios de respuesta se definen a continuación:
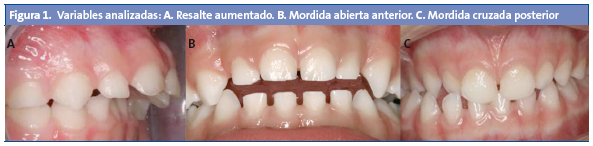
- Resalte incisivo aumentado (maloclusión en el plano sagital): cuando la distancia entre la cara palatina del incisivo central superior más protruido y la cara vestibular del inferior era mayor de 2 mm (Fig. 1A).
- Mordida abierta anterior (maloclusión en el plano vertical): cuando al ocluir los molares los incisivos no contactaban (Fig. 1B).
- Mordida cruzada posterior (maloclusión en el plano transversal): cuando las cúspides vestibulares de los molares superiores ocluyen en las fosas de los molares inferiores (Fig. 1C)5.
Hemos creados dos grupos teniendo en cuenta la edad (2-3 años/4-6 años), con el fin de analizar la presencia de hábitos al comienzo de la dentición temporal completa y en el momento cercano a su exfoliación.
Hemos dividido la muestra en tres grupos en función de la presencia de hábitos, para el estudio de las maloclusiones presentes en cada uno:
- GH1: niños que no tienen el hábito de succión de chupete ni succión digital en el momento de la exploración, ni han succionado en épocas anteriores.
- GH2: niños que han tenido hábito de succión, pero lo han abandonado anteriormente a la exploración.
- GH3: niños que mantenían el hábito de succión no nutritiva (chupete, dedo) en el momento de la exploración en dentición temporal.
Búsqueda bibliográfica
Se ha realizado una búsqueda bibliográfica presencial en la Biblioteca y Hemeroteca de la Universidad del País Vasco, en la Biblioteca y Hemeroteca de la Facultad de Odontología de la Universidad Complutense de Madrid y en el Centro de Información y Documentación Científica (CINDOC) del Consejo Superior de Investigaciones Científicas (CESIC). Posteriormente, y tras analizar los artículos encontrados, se elaboró una estrategia de búsqueda para consultar en las principales bases de datos bibliográficas, a través de los programas Medline, Índice Médico Español, Current Contents, Cochrane, Ebsco y Compludoc. La estrategia de búsqueda ha sido adaptada al thesaurus propio de cada base de datos.
Análisis informático y estadístico
Una vez recogidos los datos en fichas de trabajo, se diseñó una base de datos específica para su registro, y posteriormente se procedió al análisis estadístico, expresándose las variables cualitativas mediante el número y porcentaje, mientras que en las variables cuantitativas se ha utilizado la media como medida de posición central y la desviación estándar como medida de dispersión.
En el análisis inferencial de la comparación de medias se ha utilizado el análisis de la varianza, cuando la variable categorizada era de más de dos categorías, y la t de Student en el caso de variables con solo dos categorías. Previamente, se ha comprobado el seguimiento de la ley normal por parte de las variables mediante la prueba de Kolmogorov-Smirnov y la homogeneidad mediante la prueba de Levine.
En caso de no cumplirse las condiciones de aplicación de la prueba paramétrica, se ha aplicado la prueba no paramétrica de Kruskal-Wallis o la U-Mann-Withney, según sea la variable de categorización de más de dos o solo de dos categorías.
Para la comparación de dos variables cualitativas se ha utilizado la chi cuadrado, comprobando previamente que se cumplían las condiciones de aplicación; esto es, que la muestra fuera mayor de 30 y existiera un 25% o menos de celdas con valores esperados menores de 5. En el caso de no cumplirse las condiciones de aplicación y tratarse de tablas de 2 x 2, se ha aplicado la prueba exacta de Fischer.
Para el estudio y análisis de dos variables cuantitativas se ha utilizado la prueba de correlación de Pearson para estudiar la fuerza de asociación y la prueba de la regresión simple para valorar el modelo seguido.
RESULTADOS
La muestra inicial ha sido de 260 individuos, de los cuales 225 participaron en el estudio, lo que constituye el 86,5% del total de la muestra seleccionada. El 13,5% restante no se incluyó en el estudio por no cumplir los criterios de selección previamente fijados.
El nivel de respuesta a la encuesta de hábitos ha sido del 96,1%; de los 260 niños, 250 nos devolvieron la encuesta cumplimentada junto con la autorización correspondiente para realizar la exploración.
En la Tabla 1 hemos reflejado la prevalencia de hábitos orales, clasificando los resultados encontrados tanto para el total de la muestra como para los grupos de edad establecidos en la dentición temporal.
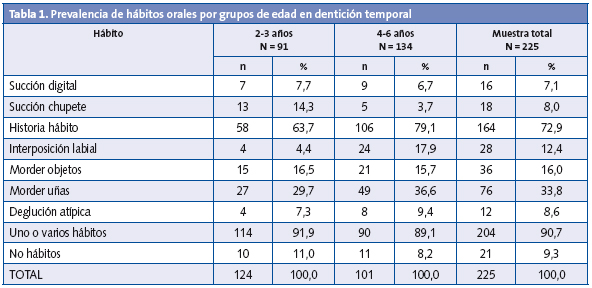
Hay que destacar la alta prevalencia de hábitos orales encontrada en la totalidad de la muestra (90,7%), frente al 9,3% que no presentaba ningún tipo de hábito ni historia de hábito.
Por grupos de edad, fueron más frecuentes los hábitos persistentes de succión en el grupo de los más pequeños (2-3 años).
Más del 80% del total de la muestra estudiada ha tenido relación con el hábito de succión de chupete (72,9% ha tenido historia de succión y el 8% mantiene el hábito).
Dada esta alta frecuencia, hemos considerado importante valorar aspectos sobre la duración de este hábito.
El intervalo de edad en el que fue más frecuente el abandono del hábito fue entre los 19 y los 24 meses (26,7%), seguido del abandono más temprano unos meses antes (7-12 meses, 14,2%), y del más tardío entre los dos años y medio y los tres (12,5%) (Tabla 2).

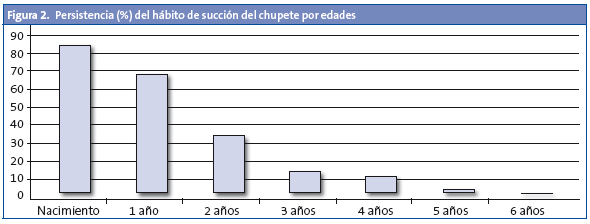
La Fig. 2 representa el abandono progresivo del hábito de succión del chupete, de manera que de ese 80,9% de niños que succionaban el chupete desde el nacimiento, el 31,1% mantuvo el hábito a los dos años, un 8,9% a los cuatro años y tan solo el 1,4% de los niños continuó con el hábito a los cinco años. A los seis años ninguno de los niños de nuestra muestra succionaba el chupete.
La Tabla 3 expresa la distribución de la muestra por grupos de hábitos establecidos tal y como se ha descrito en el apartado “Material y métodos”.

El 14,7% de los niños de nuestra muestra no presentaba ningún hábito de succión, ni había succionado el chupete en épocas anteriores (GH1), mientras que el 70,6% sí había succionado el chupete anteriormente (GH2).
El 14,7% restante de los niños de nuestra muestra mantenía alguno de los hábitos de succión no nutritiva en el momento de la exploración (GH3).
En la Tabla 4 reflejamos la presencia de las maloclusiones registradas en cada uno de los grupos considerados en el estudio.
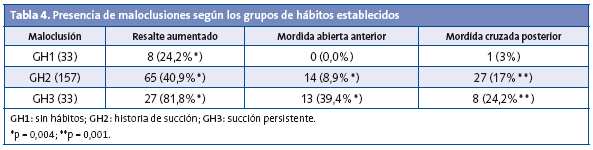
Hemos encontrado un aumento significativo de los resaltes aumentados, de las mordidas abiertas anteriores y de las mordidas cruzadas posteriores cuando el hábito de succión se mantenía (GH3), respecto a los niños que lo abandonaban tempranamente (GH2) y a los que no lo habían tenido (GH1).
DISCUSIÓN
El propósito de este trabajo ha sido analizar la repercusión que los hábitos de succión no nutritiva podían tener en el desarrollo de alteraciones dentales. Para ello, la muestra de inicio fue de 260 sujetos, correspondiente a los niños matriculados en los tres colegios seleccionados de las edades establecidas. Aplicando los criterios de selección, el tamaño final ha sido de 225, lo que consideramos un importante éxito de participación (86,5%) en el estudio. Este alto nivel de participación se justifica por la realización de las exploraciones en los centros escolares, evitando el desplazamiento de los menores, por la adecuada colaboración de padres y profesores, así como por la recaptación en las exploraciones cuando se registraba alguna ausencia.
La prevalencia de hábitos orales nocivos en el conjunto de niños estudiados en la fase de dentición temporal ha resultado ser muy alta, ya que el 90,7% presentaba al menos uno de los hábitos considerados. Los resultados ofrecidos por otros autores varían en relación a los hábitos considerados así como a las edades de los niños6-22.
Los hábitos de succión no nutritiva (chupete, dedo) han resultado ser los más frecuentes entre los niños de nuestra muestra (85,3%). En nuestro estudio hemos considerado la presencia de succión de chupete desde el nacimiento, lo que justificaría la alta prevalencia de estos hábitos, al igual que ofrecen otros autores8,14,19,23.
Como se podía esperar, hemos encontrado que los hábitos de succión son más frecuentes en el grupo de los niños más pequeños. La tendencia natural hacia su cese ha sido observada también por todos los autores que estudian la prevalencia de hábitos en las diferentes edades del niño8,14,19.
En nuestro estudio, los niños que mantenían el hábito de succión en dentición temporal mostraron mayor presencia de resaltes aumentados, de mordidas abiertas anteriores y de mordidas cruzadas posteriores, como han publicado otros autores (Infante11, 1976; Svedmyr24, 1979; Lindner y Modéer23, 1989; Ögaard6, 1994; Warren18, 2005; y Montaldo16, 2011).
Hemos observado que ciertas maloclusiones podían mejorar cuando se abandonaba tempranamente el hábito (resalte aumentado y mordida abierta anterior), dato que ya se había manifestado anteriormente, a excepción de la mordida cruzada posterior6,12,20,25-27. Por el contrario, cuando se producía un abandono tardío del hábito no era evidente la autocorrección de estas maloclusiones.
En la actualidad, no hay evidencia para apoyar la autocorrección de las mordidas cruzadas posteriores al abandonar el hábito11,13,15,28,29, por lo que se recomienda un abandono temprano de los hábitos de succión no nutritiva (antes de los dos años) para prevenir la aparición de maloclusiones dentales.
Ante la detección de una mordida cruzada posterior en dentición temporal, se aconseja el tratamiento temprano de la misma por un profesional especializado.
BIBLIOGRAFÍA
- Palacios J, Marchesi A, Coll C. Desarrollo psicológico y educación, 2.ª ed. Madrid: Alianza; 2008.
- Barbería E. Importancia de los hábitos nocivos. En: Barbería E. Atlas de Odontología infantil para Pediatras y Odontólogos. Madrid: Ripano; 2005. p. 105-25.
- Escobar F. El perfil sicológico del paciente infantil. Bases sicológicas de la Odontopediatría. En: Odontología Pediátrica. Santiago de Chile: Ed. Universitaria; 1991. p. 11-35.
- Solano-Reina E, Mendoza A. Hábitos orales: reeducación funcional. En: Boj JR, Catalá M, García-Ballesta C, Mendoza A, Planells P (eds.). Odontopediatría. La evolución del niño al adulto joven. Madrid: Ripano; 2011. p. 521-42.
- Foster TD, Hamilton MC. Occlusion in the primary dentition. Study of children at 2 ½ to 3 years of age. British Dent J. 1969;21:46-9.
- Ögaard B, Larsson E, Lindsten R. The effect of sucking habits, cohort, sex, intercanine arch widths, and breast or bottle feeding on posterior crossbite in Norwegian and Swedish 3-year-old children. Am J Orthod Dentofacial Orthop. 1994;106:161-6.
- Paredes-Gallardo V, Paredes-Cencillo C. Prevalencia de los hábitos bucales y alteraciones dentarias en escolares Valencianos. Anal Pediatr. 2005;62:261-5.
- Bishara SE, Warren JJ, Broffitt B, Levy SM. Changes in the prevalence of non nutritive sucking patterns in the first 8 years of life. Am J Orthod Dentofacial Orthop. 2006;130:31-6.
- Santos SA, Holanda AL, Sena MF, Gondim LA, Ferreira MA. Nonnutritive sucking habits among preschool-aged children. J Pediatr. 2009;85:408-14.
- Popovich F, Thompson GW. Thumb and finger-sucking, its relation to malocclusion. Am J Orthod. 1973;63:148-55.
- Infante PF. An epidemiologic study of finger habits in preschool children, as related to malocclusion, socioeconomic status, race, sex and size of community. J Dent Child. 1976;1:33-8.
- Larsson E. Sucking, chewing, and feeding habits and the development of crossbite: a longitudinal study of girls from birth to 3 years of age. Angle Orthod. 2001;71:116-9.
- Kutin G, Hawes RR. Posterior cross-bites in the deciduous and mixed dentitions. Am J Orthod. 1969;56:491-504.
- Sánchez-Molins M, Miravé FM, Ustrell JM. Hábito de succión del chupete. Estudio realizado a una población infantil de 3 a 5 años de edad. Arch Odontoestomatol. 1997;13:489-98.
- Karjalainen S, Rönning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediatr Dent. 1999;9:169-73.
- Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21:68-73.
- Aznar T, Galán-González AF, Marín IM, Domínguez-Reyes A. Dental arch diameters and relationships to oral habits. Angle Orthod. 2006;76:441-5.
- Warren JJ, Slayton RL, Bishara SE, Levy SM, Yonezu T, Kanellis MJ. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent. 2005;27:445-50.
- Duncan K, McNamara C, Ireland AJ, Sandy JR. Sucking habits in childhood and the effects on the primary dentition: findings of the Avon Longitudinal Study of Pregnancy and Chilhood. Int J Paediatr Dent. 2008;18:178-88.
- Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008;30:580-5.
- Oliveira EG, Ribeiro HC, Parreira MP, Martins Paiva S, Serra-Negra M. Influence of Nonnutritive sucking habits, breathing pattern and adenoid size on the development of malocclusion. Angle Orthod. 2008;78:647-54.
- Melink S, Vagner MV, Hocevar-Boltezar I, Ovsenik M. Posterior crossbite in the deciduous dentition period, its relation with sucking habits, irregular orofacial functions, and otolaryngological findings. Am J Orthod Dentofacial Orthop. 2010;138:32-40.
- Lindner A, Modéer T. Relation between sucking habits and dental characteristics in preschoolchildren with unilateral cross-bite. Scand J Dent Res. 1989;97:278-83.
- Svedmyr B. Dummy sucking. A study of its prevalence, duration and malocclusion consequences. Swedish Dent J. 1979;3:205-10.
- Katz CRT, Rosenblatt A. Nonnutritive sucking habits and anterior open bite in Brazilian children: a longitudinal study. Pediatr Dent. 2005;27:1-5.
- Burdi AR, Moyers RE. Desarrollo de la dentición y la oclusión. En: Moyers RE (ed.). Manual de Ortodoncia. Buenos Aires: Editorial Médica Panamericana; 1992. p. 102-150.
- Levine RS. Briefing paper: oral aspects of dummy and digit sucking: oral aspects of dummy and digit sucking. British Dent J. 1999;186:108.
- McNamara JA Jr. Early intervention in the transverse dimension: is it worth the effort? Am J Orthod Dentofacial Orthop. 2002;121:572-4.
- Kurol J, Berglund L. Longitudinal study and cost-benefit analysis of the effect of early treatment of posterior cross-bites in the primary dentition. Eur J Orthod. 1992;14:173-9.