

Vol. 14 - Num. 53
Original Papers
Prevalence of childhood oral habits and their influence in primary dentition
Virginia Franco Varasa, B Gorritxo Gilb, F García Izquierdoc
aProfesora asociada. Departamento Estomatología. Universidad del País Vasco. España.
bProfesora Titular. Departamento Estomatología. Universidad del País Vasco. España.
cOdontóloga. CS Laviada. Gijón. Asturias. España.
Correspondence: V Franco. E-mail: virfranva@hotmail.com
Reference of this article: Franco Varas V, Gorritxo Gil B, García Izquierdo F. Prevalence of childhood oral habits and their influence in primary dentition. Rev Pediatr Aten Primaria. 2012;14:13-20.
Published in Internet: 13-04-2012 - Visits: 87947
Abstract
Objectives: to assess the prevalence of anomalous oral habits and the influence of nonnutritive (pacifier and digit) sucking habits on primary dentition in a sample of preschool-age children.
Materials and methods: design: cross-sectional, descriptive, observational epidemiological study; location: three schools of the Basque Country; participants: 225 children of ages ranging from two to six years with fully erupted primary teeth.
Main measurements: the data were obtained through a habit questionnaire given to the parents, and clinical examinations performed on the children during which occlusal abnormalities such as anterior open bites, increased overjets and posterior crossbites were recorded.
Results: the prevalence of deleterious oral habits in the studied sample of children was very high (90.7%). Nonnutritive sucking habits (of pacifier, digits) were shown to be the most frequent among them (85.3%). We found a significant increase in the studied malocclusions when the sucking habit persisted.
Conclusions: nonnutritive sucking habits influence the development of teeth, and therefore we recommend that such habits be discontinued early (before two years of age) to prevent the development of dental malocclusions.
Keywords
● Malocclusion ● Nonnutritive sucking ● Primary dentitionINTRODUCTION
Sucking is a reflex that develops in intrauterine life, starting in the fetal period. The presence of this reflex in the neonate is a sign of normalcy and its gradual disappearance later on, toward four months of age, is also a sign of developmental normalcy. Thus, suction goes from being an innate reflex to being an acquired reflex or voluntary behavior around the fourth month following birth1.
For the baby, sucking is essential, since it helps satisfy his nutritional and psychological needs. However, its unwarranted persistence can have serious deleterious effects in the development of oral structures, and efforts should be made to eliminate it2.
Among all oral nonnutritive sucking habits, the most harmful are the prolonged use of pacifiers and digit sucking.
The type and extent of malocclusion caused in the child by the presence of these habits varies as a function of the type of habit, its duration, its intensity and frequency, and also depends on the biotypological characteristics of the patient2-4.
There is an interdisciplinary controversy around the role of sucking habits in the development of the child. Thus, as professionals involved in the integral health of children, we need to learn about the effects of these habits on the mouth and teeth.
The goal of the current work is to determine the prevalence of abnormal oral habits in a sample of preschool children and the contribution of these habits to the development of dental malocclusions in the primary dentition.
MATERIALS AND METHODS
We carried out a cross-sectional, descriptive, observational epidemiological study on the prevalence of oral habits in the sample under study and the malocclusions associated to nonnutritive sucking habits (pacifier suction and digit suction).
The sample used for the study consisted of children aged two to six years selected according to the established inclusion and exclusion criteria. We included all the children enrolled in years 1, 2, and 3 of early childhood education in three centers located in Vizcaya (n = 260).
The sample inclusion criteria were the following:
- The parents or tutors had given consent.
- Primary teeth had fully erupted and were in full occlusion.
- The behavior of the child was adequate for the purposes of examination.
The following were considered exclusion criteria:
- Eruption of at least one permanent tooth.
- Suffering from a significant systemic pathology.
- Having received or currently receiving any type of orthopedic or orthodontic treatment, with the exception of the placement of a space maintainer following the premature loss of a primary molar.
- Missing entries in the clinical examination form or the habit questionnaire.
Adhering to these criteria, the final sample size was of 225 subjects (124 boys and 101 girls).
We drafted a letter presenting the study to the schools, informing them of its contents and requesting their permission and collaboration. The data were collected through oral habit questionnaires given to the parents or tutors of each child. The surveys asked about the presence of digit sucking, pacifier sucking, lip interposition, object sucking, nail biting and tongue thrust. We designed the clinical examination form to gather the personal data of the child and data on the types of malocclusion under study (increased overjet, anterior open bite and posterior crossbite). Whenever possible, we used disposable examination materials, and the rest of the materials were kept in individually bagged sterile kits.
With the authorization of the directors of each center, and through them, we sent a circular to the children’s parents that included the oral habit questionnaire.
Before performing the fieldwork, we carried out a pilot study to ascertain that our methodology was satisfactory and to estimate the time needed for each examination.
The clinical examination of every child was performed by the same person in all three schools.
The analyzed variables and the response criteria were defined as follows:
- Increased incisor overjet (sagittal plane malocclusion): the distance between the palatal surface of the most protruded maxillary central incisor and the labial surface of the mandibular incisor was greater than 2 mm (Fig. 1A).
- Anterior open bite (vertical plane malocclusion): molars occluded but no contact between incisors (Fig. 1B).
- Posterior crossbite (transversal plane malocclusion): the vestibular cusps of the maxillary posterior teeth occluded on the fossae of the mandibular molars (Fig. 1C)5.

We have established two groups according to age (2-3 years & 4-6 years) in order to analyze the presence of habits soon after the full eruption of the primary teeth, and close to the time when they are expected to start exfoliating.
We divided the sample into three groups according to the presence of habits to study the prevalence of malocclusions for each of the groups:
- GH1: children who do not have a pacifier or digit suction habit at the time of examination, with no sucking habit history.
- GH2: children who used to have a nonnutritive sucking habit, but who had discontinued the habit prior to the examination.
- GH3: children whose nonnutritive (pacifier or digit) sucking habit persisted at the time of the primary teeth examination.
Literature Search
We performed literature searches by visiting the Library and Periodical Collection of the Universidad el País Vasco, the Library and Periodical Collection of the Odontology School of the Universidad Complutense de Madrid, and the Centro de Información y Documentación Científica (CINDOC) of the Consejo Superior de Investigaciones Científicas (CESIC). Later on, after analyzing the articles we found, we devised a strategy for consulting the main literature databases available through the engines of Medline, Índice Médico Español, Current Contents, Cochrane, Ebsco, and Compludoc. The search strategy was adapted to the thesaurus of each of the databases.
Computer and Statistical Analysis
Following collection of the data in forms, we designed a specific database for recording their contents. Then we proceeded to perform the statistical analysis, expressing the qualitative variables as numbers and percentages, and using the mean as the average measure and the standard deviation as the dispersion measure for quantitative variables.
The methods of inferential analysis used for comparing means were analysis of variance for polytomous variables, and Student’s t-test for dichotomous variables. We had previously verified that the variables followed a normal distribution using the Kolmogorov-Smirnov test, and the homogeneity of variances using Levene’s test.
Where criteria for the application of the parametric test were not met, we used the non-parametric Kruskal-Wallis test or the Mann-Whitney U test, depending on whether the variable was dichotomous or had more than two categories.
We used Pearson’s chi-square test to compare two qualitative variables after verifying that the assumptions for this test were met, that is, that the sample size was greater than 30 and that 25% or fewer of the cells had expected counts less than 5. Since we were working with 2 x 2 tables, if those assumptions were not met we applied Fischer’s exact test.
For the study and analysis of the two quantitative variables, we used Pearson’s correlation coefficient to assess the strength of the relationship, and simple linear regression to evaluate the model we had chosen.
RESULTS
The initial sample size consisted of 260 subjects, of which 225 participated in the study, which constitutes 86.5% of the full selected sample. The remaining 13.5% were not included in the study because they did not fit the pre-established criteria.
The response rate to the habit questionnaire was 96.1%; out of 260 children, 250 returned the completed questionnaire along with the corresponding consent to perform the examination.
In Table 1 we show the prevalence of oral habits, classifying the obtained results both for the total sample and for the age groups established in regards to primary dentition.
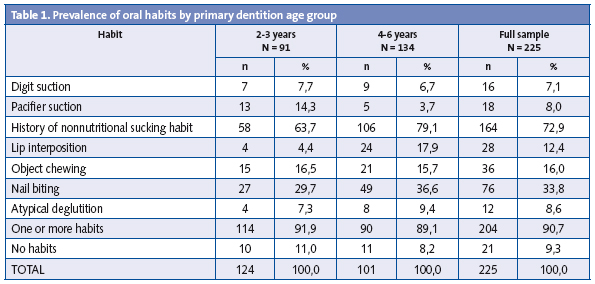
We must point out the high prevalence of oral habits found in the total sample (90.7%), compared to the 9.3% that did not present any type of habit or a habit history.
By age groups, sustained sucking habits were more frequent in the younger group (ages 2-3 years).
More than 80% of the total sample under study had an association to the pacifier suction habit (72.9% had a sucking history, and 8% still had the habit).
Given this high frequency, we felt that it was important for us to evaluate aspects relating to the duration of this habit.
The age interval when discontinuation of the habit was most frequent was between 19 and 24 months (26.7%), followed by the discontinuation of the habit a few months earlier (7-12 months, 14.2%), and then by the latest, between two and a half and three years (12.5%) (Table 2).

Figure 2 represents the progressive discontinuation of the pacifier suction habit, showing that out of the 80.9% children that started sucking on pacifiers soon after birth, 31.1% maintained the habit at two years, 8.9% at four years, and only 1.4% at 5 years of age. None of the children in our sample sucked on a pacifier at the age of six.
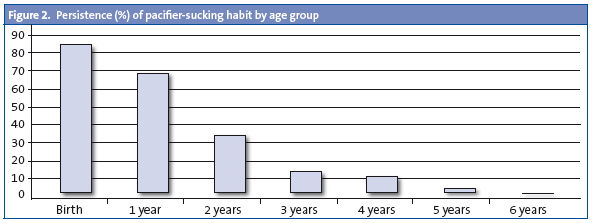
Table 3 shows the distribution of the sample into the habit groups established as described in the “Material and Methods” section.

14.7% of the children in our sample did not present any sucking habits, nor had sucked on a pacifier before (GH1), while 70.6% had a history of pacifier suction (GH2).
The remaining 14.7% of the children in the sample still had at least one of the nonnutritive sucking habits at the time of the examination (GH3).
In Table 4 we show the malocclusions recorded for each of the groups under study.
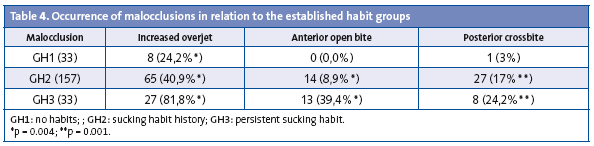
We found a significantly higher frequency of increased overjets, anterior open bites, and posterior crossbites when the sucking habit persisted (GH3), compared to children who discontinued it early (GH2) and children who had never had it (GH1).
DISCUSSION
The purpose of this work was to analyze the potential repercussions of nonnutritive sucking habits in the development of dental abnormalities. For this purpose, we had an initial sample size of 260 subjects, which corresponded to the children enrolled in the three selected schools who fell into the established age range. After applying the inclusion criteria, the final sample size was 225, which we consider a successful study participation rate (86.5%). This high participation rate can be explained by the fact that we did the examinations in the school facilities, so children did not have to travel, also by the satisfactory collaboration of parents and teachers, and by return visits for further explorations whenever a child was missing.
The prevalence of deleterious oral habits in the sample of children at the stage of primary dentition has turned out to be quite high, since 90.7% presented at least one of the habits under consideration. The results divulged by other authors vary in relation to the habits under consideration as well as to the ages of the children6-22.
Nonnutritive sucking habits (pacifier and digit sucking) turned out to be the most frequent habits in the children that formed our sample (85.3%). Our study considered the presence of the pacifier-sucking habit since birth, which would account for the high prevalence of these habits, as is also noted by other authors8,14,19,23.
As expected, we have found that sucking habits are more prevalent in the group of younger children. The natural tendency to discontinue them has also been noted by all the authors that research the prevalence of habits in children at different ages8,14,19.
In our study, children with primary teeth with a sustained sucking habit showed a higher prevalence of increased overjet, anterior open bite, and posterior crossbite, which has also been reported in previous publications by other authors (Infante11, 1976; Svedmyr24, 1979; Lindner and Modéer23, 1989; Ögaard6, 1994; Warren18, 2005; and Montaldo16, 2011).
We observed that some types of malocclusion could improve if the habit was eliminated early on (increased overjet and anterior open bite), a finding that had been observed before, which did not apply to posterior crossbites6,12,20,25-27. In contrast, when the habit stopped at a later age, there was no evidence of spontaneous correction of these types of malocclusion.
At present, there is no evidence supporting the spontaneous correction of posterior crossbites when the habit is discontinued,13,15,28,29, so we recommend the early discontinuation of nonnutritive sucking habits (before two years of age) to prevent the development of dental malocclusions.
If a posterior crossbite is detected on the primary teeth, it is recommended that treatment by a specialist be sought at an early stage.
BIBLIOGRAPHY
- Palacios J, Marchesi A, Coll C. Desarrollo psicológico y educación, 2nd ed. Madrid: Alianza; 2008.
- Barbería E. Importancia de los hábitos nocivos. In: Barbería E. Atlas de Odontología infantil para Pediatras y Odontólogos. Madrid: Ripano; 2005. p. 105-25.
- Escobar F. El perfil sicológico del paciente infantil. Bases sicológicas de la Odontopediatría. In: Odontología Pediátrica. Santiago de Chile: Ed. Universitaria; 1991. p. 11-35.
- Solano-Reina E, Mendoza A. Hábitos orales: reeducación funcional. In: Boj JR, Catalá M, García-Ballesta C, Mendoza A, Planells P (eds.). Odontopediatría. La evolución del niño al adulto joven. Madrid: Ripano; 2011. p. 521-42.
- Foster TD, Hamilton MC. Occlusion in the primary dentition. Study of children at 2 ½ to 3 years of age. British Dent J. 1969;21:46-9.
- Ögaard B, Larsson E, Lindsten R. The effect of sucking habits, cohort, sex, intercanine arch widths, and breast or bottle feeding on posterior crossbite in Norwegian and Swedish 3-year-old children. Am J Orthod Dentofacial Orthop. 1994;106:161-6.
- Paredes-Gallardo V, Paredes-Cencillo C. Prevalencia de los hábitos bucales y alteraciones dentarias en escolares Valencianos. Anal Pediatr. 2005;62:261-5.
- Bishara SE, Warren JJ, Broffitt B, Levy SM. Changes in the prevalence of nonnutritive sucking patterns in the first 8 years of life. Am J Orthod Dentofacial Orthop. 2006;130(1):31-6.
- Santos SA, Holanda AL, Sena MF, Gondim LA, Ferreira MA. Nonnutritive sucking habits among preschool-aged children. J Pediatr. 2009;85(5):408-14.
- Popovich F, Thompson GW. Thumb and finger-sucking, its relation to malocclusion. Am J Orthod. 1973;63:148-55.
- Infante PF. An epidemiologic study of finger habits in preschool children, as related to malocclusion, socioeconomic status, race, sex and size of community. J Dent Child. 1976;1:33-8.
- Larsson E. Sucking, chewing, and feeding habits and the development of crossbite: a longitudinal study of girls from birth to 3 years of age. Angle Orthod. 2001;71:116-9.
- Kutin G, Hawes RR. Posterior cross-bites in the deciduous and mixed dentitions. Am J Orthod. 1969;56(5):491-504.
- Sánchez-Molins M, Miravé FM, Ustrell JM. Hábito de succión del chupete. Estudio realizado a una población infantil de 3 a 5 años de edad. Arch Odontoestomatol. 1997;13(8):489-98.
- Karjalainen S, Rönning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediatr Dent. 1999;9(3):169-73.
- Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21(1):68-73.
- Aznar T, Galán-González AF, Marín IM, Domínguez-Reyes A. Dental arch diameters and relationships to oral habits. Angle Orthod. 2006;76(3):441-5.
- Warren JJ, Slayton RL, Bishara SE, Levy SM, Yonezu T, Kanellis MJ. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent. 2005;27:445-50.
- Duncan K, McNamara C, Ireland AJ, Sandy JR. Sucking habits in childhood and the effects on the primary dentition: findings of the Avon Longitudinal Study of Pregnancy and Chilhood. Int J Paediatr Dent. 2008;18(3):178-88.
- Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008;30(6):580-5.
- Oliveira EG, Ribeiro HC, Parreira MP, Martins Paiva S, Serra-Negra M. Influence of Nonnutritive sucking habits, breathing pattern and adenoid size on the development of malocclusion. Angle Orthod. 2008;78(4):647-54.
- Melink S, Vagner MV, Hocevar-Boltezar I, Ovsenik M. Posterior crossbite in the deciduous dentition period, its relation with sucking habits, irregular orofacial functions, and otolaryngological findings. Am J Orthod Dentofacial Orthop. 2010;138(1):32-40.
- Lindner A, Modéer T. Relation between sucking habits and dental characteristics in preschoolchildren with unilateral cross-bite. Scand J Dent Res. 1989;97(3):278-83.
- Svedmyr B. Dummy sucking. A study of its prevalence, duration and malocclusion consequences. Swedish Dent J. 1979;3:205-10.
- Katz CRT, Rosenblatt A. Nonnutritive sucking habits and anterior open bite in Brazilian children: a longitudinal study. Pediatr Dent. 2005;27:1-5.
- Burdi AR, Moyers RE. Desarrollo de la dentición y la oclusión. En: Moyers RE (ed.). Manual de Ortodoncia. Buenos Aires: Editorial Médica Panamericana; 1992. p. 102-150.
- Levine RS. Briefing paper: oral aspects of dummy and digit sucking: oral aspects of dummy and digit sucking. British Dent J. 1999;186(3):108.
- McNamara JA Jr. Early intervention in the transverse dimension: is it worth the effort? Am J Orthod Dentofacial Orthop. 2002;121(6):572-4.
- Kurol J, Berglund L. Longitudinal study and cost-benefit analysis of the effect of early treatment of posterior cross-bites in the primary dentition. Eur J Orthod. 1992;14(3):173-9.
Comments
This article has no comments yet.