


Changing the narrative: a transformative gaze in the face of gender diversity
Filippo Fioritaa, Concepción Bonet de Lunab
aPediatra. CS Reina Victoria. Madrid. España.
bPediatra. CS Segre. Madrid. España.
Correspondence: F Fiorita. E-mail: fioritafilippo@gmail.com
Reference of this article: Fiorita F, Bonet de Luna C. Changing the narrative: a transformative gaze in the face of gender diversity. Rev Pediatr Aten Primaria. 2020;22:e121-132.
Published in Internet: 20-07-2020 - Visits: 11710
Abstract
Introduction: in recent years, there have been numerous scientific publications on gender diversity in children and adolescents along with establishment of medical and psychological services to serve this population. This increased visibility is the result of a more tolerant social and cultural context; however, there are still barriers and prejudices that these children and their families have to face in the process of self-acceptance and in their relationship with the different social settings of their lives.
Sample and methods: qualitative study through individual in-depth interviews with 6 parents of trans children of different ages in the Community of Madrid.
Results: we present the results organised in 3 main categories: the pathway of parents (the phases of understanding and accepting gender diversity in their children); the pathway of children (social transition and its emotional and psychological impact); the pathway of society (the relationships and dynamics between these families and their social environment). The latter category includes a specific section about the relationship with the health care system.
Conclusions: the narratives collected in the interviews evinced the presence of a virtuous circle that arose from the recognition of the gender diversity in these children and involving the love of parents and inclusion in society. This allows for the change in perspective required to become aware that the only disease that we need to fight is transphobia.
Keywords
● Gender identityINTRODUCTION
This project stems from the encounter in a primary care clinic in 2014 with a transgender girl aged 10 years. In the absence of knowledge on gender diversity in childhood, questions emerged such as, is it better to address this child as a boy or as a girl? Can it manifest at such an early age? What is our role as health care professionals? Is this OK? At the time, little attention was paid to the issue by the media and science, and after searching the available medical literature for information, we were most surprised to realize that our initial reaction had approached transphobia.
In recent years, there has been a growing interest in the medical community in gender diversity in childhood, manifesting in position statements by institutions such as the Asociación Española de Pediatría (Spanish Association of Pediatrics)1 and the institution of specialised clinics for transgender minors offering hormone therapy and psychological support.2
Despite this growing awareness, these minors and their families still face countless barriers and prejudices in the process of finding self-acceptance and searching acceptance in the different social settings in their lives. Understanding these experiences from the perspective of the individuals that live them may help overcome prejudices and improve health care delivery.
Few qualitative studies have made a phenomenological analysis of the personal experience of parenting transgender children. A study published in 2017 in the United States documented the experiences of 11 parents, which brought focus on 2 prevailing pathways: rescuing the child, from fear of stigma and hurt, or accepting gender variance and advocating for a more tolerant world.3
The evidence we found for Spain was very limited. The guideline for management of trans minors with gender variance published by the government of Madrid in 20154 presents a compilation of narratives of the experiences of trans youth (starting at age 16 years) and parents of trans minors from the initial manifestations of gender variance in early childhood to the challenges faced in changing the name and sex in official records. Also, a chapter in a book aimed at mental health professionals published in in 20185 documents the experiences of parents and social work, education and health care professionals working with transgender children and youth.
The aim of our study was to understand the experiences of the parents of transgender minors in the process of understanding and accepting gender variance in their children and in the context of difference social settings, such as the school and the health care system.
SAMPLE AND METHODS
We conducted a phenomenological qualitative study through the performance of in-depth interviews in April and May of 2018 in urban health care centres in the Community of Madrid.
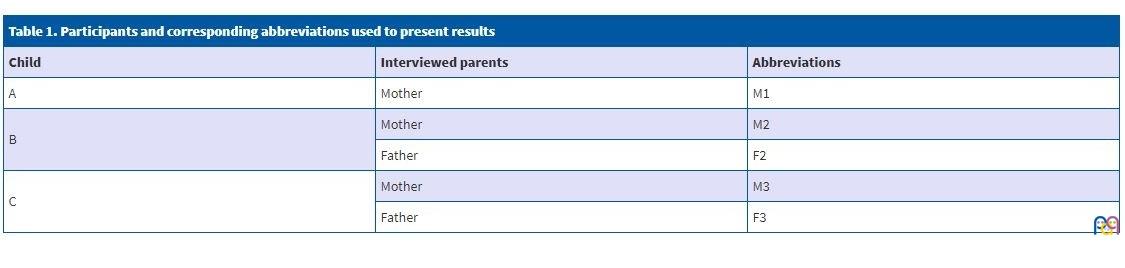
We carried out a total of 5 interviews:
- Mother (M1) of a child aged 5 years assigned male sex at birth exhibiting female gender expression and with a possible female gender identity (A). At the time of the interview, the child had not undergone social transition. We recruited this mother through a primary care clinic.
- Mother (M2) and father (F2) of a transgender girl aged 14 years (B) that had undergone social transition at age 6 years. At the time of the interview, the girl was in treatment with puberty blockers. These subjects were recruited through the website of an association of families of transgender children and youth.
- Mother (M3) and father (F3) of a transgender boy aged 7 years (C) that had undergone social transition a few months before the interview took place. Subjects recruited through the mother of case B.
We refer to each child using the gender used by the parents during the interviews, which was based on whether the child had undergone social transition.
Table 1 lists the participants in the study with the corresponding abbreviations used to refer to them in the results in the cited texts.
| Table 1. Participants and corresponding abbreviations used to present results | ||
|---|---|---|
| Child | Interviewed parents | Abbreviations |
| A | Mother | M1 |
| B | Mother | M2 |
| Father | F2 | |
| C | Mother | M3 |
| Father | F3 | |
Participation in the study was voluntary after consenting to participation, having informed parents about the study design, its objectives, the methods used and the possibility of future publication.
The interviewees selected the meeting place: M1 chose a bar and the other 2 couples chose to meet in their homes. We anticipated a maximum duration of 90 minutes, and the actual mean duration of the interview was 64 minutes.
The interview did not consist of a structured set of questions, but rather we asked participants to discuss their experiences in the process of understanding and accepting gender diversity in their children and in relation to the social environment (family, school, health care facilities).
We recorded the interviews, and the principal investigator later transcribed them verbatim into Word® documents.
Both researchers contributed to the analysis of the data. We conducted a thematic analysis with the grounded theory approach first described by Glaser and Strauss.6
This was followed by triangulation of the data, first involving both researchers and then involving the researchers and the interviewed participants.
We reached data saturation as regards the process of gender diversity acceptance and inclusion. However, we did not explore other potential attitudes that have been described in the literature, such as denial or repression. Gaining access to these perspectives could be challenging, as parents with these experiences are very unlikely to agree to participate in a study of these characteristics.
RESULTS AND DISCUSSION
Three main categories emerged in the data analysis, which we organised into 3 sections:
- The pathway of parents: stages in the process of understanding and accepting gender diversity in their child.
- The pathway of children: social transition and its emotional and psychological repercussions.
- The pathway of society: relationships and dynamics that form between these families and their social environment. This category includes a specific section on the health care system.
The pathway of parents
The moment when a child starts to consistently express a gender other than the assigned sex at birth usually comes as a surprise to parents. In their minds, they have always held the image of a “desired child” 7 that is the repository of fantasies and expectations:
[M3]: You have expectations, right? You have a daughter that’s a girl, right? And you want her to be a girl and you want her to become a woman and you want her to become a mother and you want her to… you don’t want her to suffer and you don’t want her to be something other than what you expect.
The mental representation of the “desired child” is in conflict with the “real child” 8 emerging before their eyes, and this triggers a psychological and emotional process that is different in each parent.
The narratives captured some of the classical stages of grief,9 such as denial, anger and sadness:
[F3]: You see? There are people that, like us, we’re not prepared for these things, psychologically. To face these situations… at the end of the day we just want to avoid problems: “Let’s see if it passes, let’s see if whatever…”
[M3]: Then I started to fight against… so to speak, fight against my daughter. “I said no! You’re a girl! And such…”. […] I cried a lot, I suffered a lot, and as I informed myself, I started to realise that my child was a transgender boy, not a girl at all: he was a transgender boy. And then I started to feel awful.
In addition, in the wake of such an unexpected and unfamiliar experience, different fears emerge. The most “primitive” fear of the different:
[M1]: Because at the end of the day any difference scares parents. None of us wants our child to be different.
The fear of suffering and social rejection:
[M3]: I keep thinking: “Will he suffer, not suffer… He could end up like those kids that committed suicide…”.
[M2]: And you also think: “They will attack her, they will do all sorts of things, they’ll beat her up…”. You know? It’s this thing that’s been in your mind all along.
The fear to make mistakes in managing such an important issue in the dark, despite the substantial amount of information at hand:
[M1]: For me, too, I’m a first-time mother with A [child]: you have every possible doubt in the world and more, endless insecurities, and you’ve read a ton of things and in the end you’ve become uninformed because… you’ve filled up with information and a lot of it is contradictory and at the end, you just go with your gut […]. I mean, I question myself, wondering if I’m consulting the internet too much and I’m creating something that does not exist, whether this is actually possible, how to do it right, or… oh, I don’t know.
In the search of an explanation for the unknown, it is also possible to develop feelings of guilt:
[M1]: In the end, I… at times you wonder whether it could be your fault that they’re different, right? Whether you’ve gone overboard and too “modern” and you’re the one that’s confusing the kid.
As they go through these stages, parents start to question their expectations (and, in doing so, the perspective of the prevailing social discourse), gradually changing their attitudes and how they view their children.
[M2]: Of course, you just have to change your mind some, and assume that… that things are not really as we think, and that there’s a lot more diversity than we realise.
This psychological journey allows them to bid farewell to the imaginary “desired child” and accept the “real child”. This is possible thanks to the main characteristic that defines adequate parenting7: love, which in this case translates to unconditional positive regard.
[M3]: Since I cared about my child more than I cared about my beliefs, I started to tell myself: “this won’t do, I have to change the way I think”.
Not all parents need to go through this transformation: the experience of one of the interviewed parents reflects a different attitude from those described this far.
[F2]: Well, for me it’s never been a problem at all … nor have I felt bad about it, nor… you know? […]. I’ve never thought: “We have to stop this right away, this…”, it has not even crossed my mind because I see it as a natural behaviour, you see? […]. You see such natural behaviour, so true, that you see that their happiness depends on it, and such, that you’re not harming anyone with it […], why should I go against it? To hurt my kid?
The pathway of children
“Transitioning” is the process that a transgender person may need to undergo to experience their gender identity in a fulfilling manner. It may include social changes (dress, hairstyle, name, documents…) and, starting in puberty, medical interventions2 (puberty blockers and gender-affirming hormone therapy) and surgical interventions. The nature and timing of these actions must be individualised to fit the needs of the individual and based on the safety of the environment.10
Social transition and medical interventions have beneficial effects: they alleviate psychosocial distress,11 improve anxiety and depression symptoms,12-18 behavioural problems and social functioning overall.19
In the interviews we made, too, social transition marked a turning point in the lives of these minors.
The first episodes of gender nonconformity that parents could remember occurred at early ages in the context of play and were perceived as natural.
[F2]: They have female cousins, and when we went to their house, the first thing she did was grab a dress… usually take one of the costumes she had, a princess costume or something like that, and she put it on first of all, and once she was wearing it, she would then go and play with the others.
As these children are redirected to fit a gender that they do not identify with, they progressively develop recurrent and exaggerated behaviours to reinforce and affirm their identity. This can lead to isolation and social rejection.
[M2]: I mean, she had to wear the dress, her pyjamas, everything, absolutely everything had to be extremely girlish. As extreme as possible, so there could be no doubt at any point that she was a girl.
[M1]: In fact, my son is more radical than any other girl. He does not play soccer. Why? Because soccer is for boys, he makes that separation! “I am not playing this”. “Why?” “Because I don’t want to”. He is starting to become isolated because he either plays princess with girls or he does not want to play.
The interviews uncovered numerous episodes of sadness and somatization due to not being recognised for who they were and being forced to be what they were not.
[M1]: He had asked for the dress from Frozen and instead got a Spiderman pencil case and, well, he looked at it, completely ignored it, and when we got home he told me: “I’ve been bad, right?” and I said: “Why are you saying that?” and he tells me: “Because Santa Claus has punished me” and I said: “How did Santa Claus punish you? Santa Claus would never punish you.” “So why did he bring me something I hate? Why did he bring me something I hate, Mum?”.
[F2]: When we went to the first psychiatrist, well, the very first one, when we went to Mental Health here, to see how it went, well: that “boys play with balls and girls with dolls…” Ahem, boing [gesture of bouncing off]. The next one, she was doing a drawing and started to cross it out and then came home, took a nap and wet the bed, which she’d never done in her life, you know? And then at night she wet the bed again.
[M3]: He did not want to wear knickers anymore, he wanted the earrings out, wanted his hair short, and it was frustrating, it was oppressive… “I mean, no, this itches! [while touching the ears] And, this hurts! [while touching the body]”.
On the other hand, there are many episodes of joy and happiness when their feelings are reaffirmed.
[F2]: And she would put on her dress […] and of course I could tell she changed. She played a lot more, she laughed more, she was happier… They took her for a girl, would say she was a girl, and she never said… she never corrected them, you know? She didn’t say anything… So I told myself “this is not just a thing…” told myself, “a whim, a thing…” No, no, it as something that affected her wellbeing, right? To be like this.
[M1]: [after he was given the costume of Elsa, from Frozen] Well, he run off and, well, he did not take it off in the three days at Disney, and he was happy… happy. And, then, I think for any parent to see their child so elated, happy and fulfilled, no amount of money in the world could buy something like that, right? And I think that that also helped us curb our fears and all that stuff…
The stage of transition is a time characterised by being recognised by the parents, and, as philosopher Axel Honneth claims,20 this is a necessary step for the construction of a stable identity. When the parents get to know their child anew through a loving and accepting gaze, the child in turn receives the projection of a positive image of themselves. This makes the child feel worthy and empowered and able to experience an identity that is no longer questioned more fully and harmoniously. It is only then that the child can express themselves without fear, freely and independently, and interact with others in a more authentic manner.
[M2]: It is true that when it came to B [daughter], she was quite exaggerated, she was very extreme, went for the most sparkly, the most pink, the gaudiest, until she transitioned and then she relaxed and started to do whatever she felt like, that is, to play with everything, play with boys, play…. Something she had not done until then.
[M3]: When we treated him as a girl and was C [female name given at birth], he didn’t make any friends. He had… they were his sister’s friends. […] Once he started to feel who he really was, that he was a boy, and transitioned, he made friends, had his own friends, his own things… He started to say “Damn, I am something too, not just part of what you are, but I have my own space, my own friends, etcetera.” And, and… he changed.
The pathway of society
Thanks to the considerable efforts of LGTBQI groups, in the past 2 decades laws and statements from international institutions have emerged depathologising gender diversity and seeking to fight discrimination and promote social equality. However, despite this growing openness, the prevailing social discourse continues to be highly prejudiced as regards gender diversity, especially in minors.
[M1]: Because of course, I’ll be walking with my son, and my son will be carrying a doll in his hand, and there’s always a mom or some woman as you go down the street that does not know you at all and tells him: “Young man, what are you doing with a doll? That’s a girl thing”.
[M2]: And then there’s the social pressure, see? People. “Ah, this is because you wanted a girl, right?”, do you know what I mean? It’s like, kind of … “Well, of course… it’s because you let him a bit… how do you let him wear this? And how…” And a bit like… “How did you let it go like this? Don’t you think? And she’s so young… ”, you know? This kind of comments.
The term phobia merges 2 different and parallel concepts: fear and hatred. A phobia is an irrational hatred rooted in the primitive human fear toward anything unknown that we cannot understand. It is a defence mechanism, a survival instinct by which we assert ourselves when facing difference. In this regard, phobia and ignorance (not knowing something) are deeply related.
For this reason, one of the first and possibly most important steps in fighting transphobia is visibility: to come into the open and be known to a civil society that is ignorant and transphobic.
[F2]: Well, we ourselves have raised them in our business, the kids I mean, and they’ve seen it; the thing with B [daughter] they’ve seen how it goes […]. People know, and know how it is, you know? I mean, in general, I mean about 95% […] 95% have taken it… you know. They’ve seen it from the very beginning, right? They’ve seen it, the evolution, what we have done […] because many of the problems around these issues have to do with ignorance, with a lack of data, with… it’s just not knowing… and it must come out and be seen, normalised, you see?
In addition, becoming visible in everyday life is key for families to meet one another, breaking a state of isolation that is difficult to endure. This leads to the establishment of a mutual support network, which allows the development of a group identity and the strength required to raise awareness in the public and advocate for trans rights. Just as in the previous section we saw that acknowledgment in parents developed through love, in this case social recognition of transgender individuals develops through the law.20
[M2]: One of the things you experience as a family at the beginning is isolation, right? I mean, this: “Is there nobody else out there that has a trans kid? Is it just us?”. And this feeling of isolation, when you tell the family: “No, you’re not alone, but it’s not just that, it’s not just that you’ve found me, it’s that you’re going to find hundreds… hundreds of families, because I’m going to get you in a group where there’s a ton of us [laughs]. [Speaking of the daughter] Because what she wanted was to get the blockers. That was her… her… and if getting the blockers took being visible, well that was it, then. And of course, then we thought “the louder we get…” you know? “the easier it will be to get things”. It’s obvious. And that’s how it was. […] So, we participated in the documentary, at that time we were 40 or so families… and… it just exploded. When the documentary came out, suddenly we were a hundred plus, just suddenly, I mean, in 2 or 3 days… I mean, it was… just incredible.
In addition to promoting rights, another outcome of social recognition is a progressive change in social discourse that questions the binary gender construct and proposes alternative solutions.
[M1]: We let the childcare centre and the school know that the kid likes pink and that we think it’s great, so that they won’t change his crayon or… “don’t draw with pink, draw with blue”. No, no, we think it’s great that he draws with whatever he pleases. […] “But they told me that I cannot colour it pink” “Who told you that?”. “So-and-so”. “Why?”. “Because it’s for girls”. “No, colours are not for boys or for girls, they are for anyone that feels like drawing”. […] And thus, well, I think one needs to be aware that… that it’s much richer to take away gender from games, and from colours, and… from everything, really, right?
Thanks to the change in the discourse promoted by these families, society also undergoes a transition. Phobia, once gender diversity is seen and recognised in these children, shifts to openness and inclusion.
[M3]: [After discussing her son’s social transition with the school]. They did a training for the entire teaching staff, they contacted me… everything was great. I’ve had no problems with the school. Even better, about 15 days after or so, maybe a month, one day C [child] came home very, very happy, telling me that all the bathrooms for… that all the bathrooms that he used were no longer labelled for “men”, but “unisex”. It’s wonderful, the school has been wonderful.
Relationship with health care system
[F2]: [Speaking of trans adults]. Because they have many problems, psychological problems, many things that are not caused by what they are, they are caused by other people. Health in trans people… I mean, in all people… 50% of health is social, right? It’s the part that nearly has most impact on health. So imagine what this means for trans people… right?
In 1946, the World Health Organization defined health as “state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. Therefore, although gender variance is not a disease, it is the duty of every physician to be informed and know how to manage the needs of transgender children, independently of their own political or religious beliefs.
In 2018, the Asociación Española de Pediatría (Spanish Association of Paediatrics) published a position statement regarding gender diversity in children and adolescents,1 offering recommendations for management at the primary care level.
When it came to these recommendations, the interviews revealed significant gaps, as the role of the paediatrician is often reduced to merely making referrals to specialists.
[M2]: The paediatrician… it was quite something. I mean, the paediatrician… I think he’s a fantastic paediatrician, as a professional, I mean. But… not to talk to. I mean, if the kid had, say, pneumonia, he’d detect it, you know? Cos he was a machine. But then, when it came to discussing anything, I would say something like: “So we heard this from the endocrinologist …”, “Ah OK, then …”, “No, I mean you need to send us here, and such …”, “Ah, sure” and he’d refer us. But he did not ask… he… he showed no interest. […] I think he was embarrassed. And I too felt embarrassed talking to him… you know, it was like I felt I could not… talking to him seemed hard. I don’t know if it was that it did not seem like he understood it very well, or that he did not support it, or… It did not seem as if he cared… you know?
[M3]: Well, at the doctor, for example, the paediatrician, when I went in November to ask for an appointment with *** [psychiatrist], I went to the paediatrician here at *** [city in the autonomous community of Madrid] and told him: “Look, I have to tell you something: C [son] is a transgender kid, we think he’s a transgender boy. So I need you to give me a referral for …”, “Don’t worry, no problem”. And blah, blah, blah … […]. “Where do I need to send you?”. “Here”. He did not know anything, he didn’t really understand much …
Support, acknowledgment and positive regard are an essential part of the help that families need.
[M2]: I wanted a professional to tell me what was going on, although I was quite certain that she was trans, I wanted to hear it from a… [laughs] a professional. […] Once I was told it, I could be at peace, because what I was seeing was real, right?
[M2]: And then we started to go [to psychiatric services] and, it’s true, only when they told us that it was going to be a… like a support thing, that it was not about doing an intervention at any point or anything, then… well, I thought it was great.
[M2]: Although in fact the psychologist kept telling us: “Well, you’re doing the right thing”, you know? I mean…, she could not tell us what we needed to do going forward or how to do everything, but what she was certain of is that we were doing a good job, and this affirmation was very good for me, because we worked with her nearly a year and I needed that support.
CONCLUSION
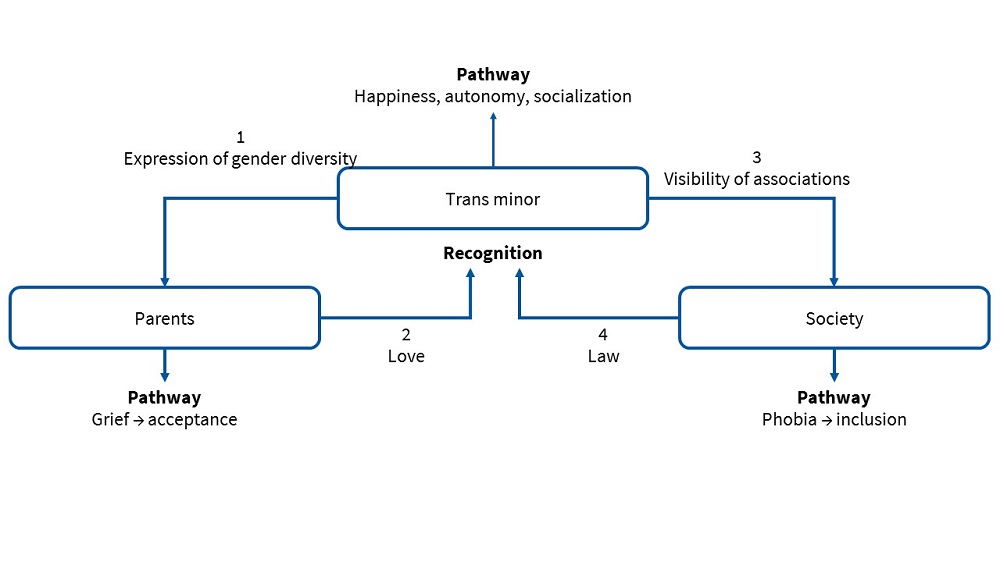
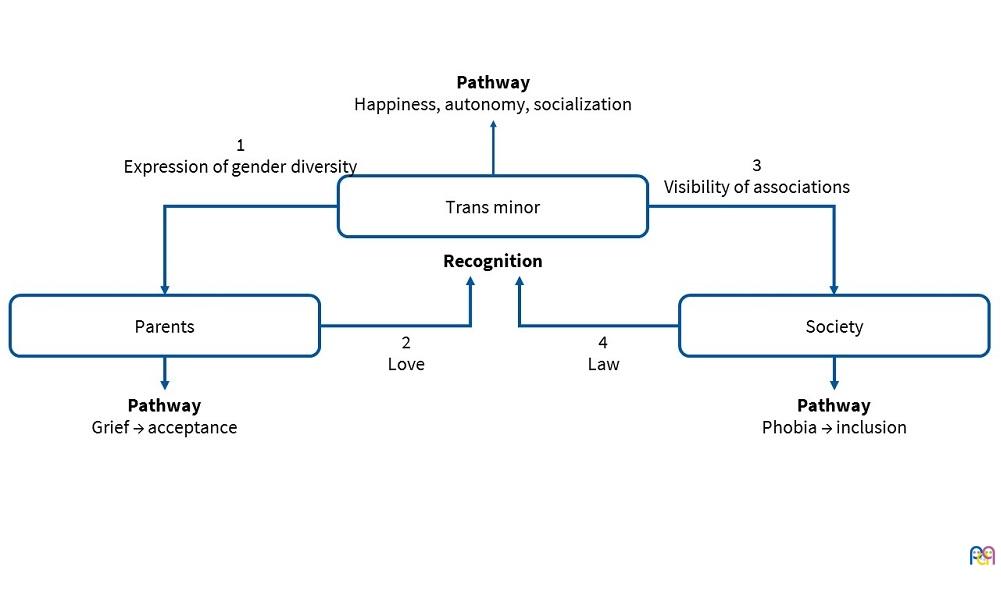
The narratives of the interviewed families demonstrate the virtuous cycle engendered by the recognition and acceptance of gender diversity in the offspring. These children persistently express and wish to be what they are, even when facing authority figures, such as the parents. This image often conflicts with the image of the “desired child”. The parents may go through different stages (denial, anger, sadness, fear, guilt), as their perception and appreciation of the “real child” changes. At first, they may feel like they are moving in the dark, unsure of what is the right thing to do. The love that characterises their relationship as parents manifests in the will to support their children and protect them from suffering. And when this love includes respect, parents gradually give children the necessary space to be who they are. This way, these children feel legitimised and empowered, and can experience their identity in a more authentic and fulfilling manner. When this happens, the image that parents receive and project back further affirms them in the process of acceptance, and thus the “circle” is completed. This is the source of the strength and the power needed to become visible to the rest of society. The fear-hatred of the unknown may give way to the recognition of diversity in increasingly wide social circles. Thus, minors acquire rights at the social level (administration, health care system…) and society is enriched, diversified and transformed, becoming more open and inclusive (Fig. 1).
| Figure 1. Summary of the relationships that emerged in interviews between trans minors, their parents and society |
|---|
 |
Going back to that encounter in 2014 that aroused our interest in the subject of this work, questions such as “is this right?” hinder the ability to see and interpret the reality of alternative ways. Rather than questioning the legitimacy of a diversity that simply exists (“so natural” and that “is not harming anyone”, as F2 said in the interview), perhaps we should question the model of society that we live in and ask ourselves: what kind of society do we wish to build? Does this rigid and exclusionary separation of 2 predefined genders make sense? Why condemn people that do not fit this system to suffering and fighting to be able to live the way they are?
The main source of suffering in these children is not their difference from others, but ignorance and the intolerance for the perceived “other”: a change in the colour of the markers in school, a careless remark at the doctor’s office… a change in perspective is necessary to understand that disease does not stem from gender diversity, but from the transphobia found in society. Perhaps the cure lies precisely in the diversity of these individuals, which challenges, enriches and broadens perceptions.
As paediatricians, we must be educated and know how to support families in this journey. It is our duty to do it, and to do it right.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ACKNOWLEDGMENTS
This project would not have been possible without the valuable testimony of the interviewed families and the priceless contribution of Dr Raquel González Rubio.
APPENDIX. GLOSSARY
These definitions (as all others) are necessary to make sense of the world and communicate with fewer misunderstandings. However, it is important that we always remain aware that any attempt to classify reality simplifies its complexity. We label diversity and in doing so it becomes crystallised in a social context that is actually constantly evolving.
Sex assigned at (or before) birth. The anatomy of the genitalia can already be established in prenatal ultrasound examinations, and a sex assigned based on these findings. Until recently, the sex was assigned by the midwife at the time of birth, but other than that the criteria have not changed. The anatomical sex positions the individual in a binary system (male vs female) and tends to be associated with other biological sex concepts (chromosomal sex, gonadal sex, hormonal sex). It is important to remember that none of these concepts in isolation is sufficient to provide an exhaustive definition of being female or male, as evinced by a number of conditions (history of hysterectomy or orchiectomy, Turner syndrome, androgen insensitivity syndrome, etc.) Furthermore, classifying persons based solely on biological criteria has limitations when it comes to the description of intersex conditions, which can be much more diverse and complex. Therefore, we need another concept to better understand what makes persons male or female.
Gender identity. According to the World Health Organization, gender is a set of social constructs that defines the roles, behaviours, activities, attributes and opportunities considered appropriate for all individuals in a given sociocultural context.21 Therefore, gender identity is defined as identifying as one of these 2 categories (male or female), or possibly not identifying with either or identifying with both. It corresponds to what many people outside academic circles refers to as “felt gender”.
There are studies in the scientific literature that describe the different phases in the development of gender awareness in children in relation to the prevailing gender norms in their environment and to their own gender identity. At age 2 years, children can already distinguish a male from a female face and differentiate male from female in speech (articles, pronouns, adjectives), and position themselves in one of the 2 genders. Furthermore, they explore both genders in play through different toys, costumes and colours.22,23 Children gradually exhibit interests and preferences that in most cases match the gender corresponding to the sex assigned at birth.24 Preschool-aged children assimilate gender stereotypes, preferentially playing with children of the same sex and socializing through roles and norms that reflect conventional gender constructs.12,25,26
All of these (preferred toys, social roles, pronouns), when occurring in a consistent, persistent and insistent fashion, constitute the initial manifestations of the gender identity. When this identity does not match the sex assigned at birth, it is referred to as gender incongruence.
Gender expression. Individuals can express themselves through characteristics that are culturally associated with either of the 2 genders (or combine characteristics of both): clothing, hairstyle, speech, etc. When gender expression does not fit established cultural norms or reflect the stereotypes of the sex assigned at birth, this is referred to as gender nonconformity.
Thus, it is important that we clarify: a minor with a gender identity that does not match the sex assigned at birth may express gender variance unconsciously in the early years of life, with an overlap of gender incongruence and nonconformity. With time, the individual may exhibit a gender expression that conforms more to the sex assigned at birth for a variety of reasons: the individual may truly become gender congruent, or may be afraid of hurting their family, may feel pressured to conform to dominant social norms and/or feel ashamed of their “difference”. But a lack of expression does not mean that gender incongruence does not persist. And vice versa: an individual assigned male sex at birth that behaves as a female does not necessarily identify as female. It may be that this individual simply wants to express himself this way while identifying as male.
Transgender (/trans). Umbrella term comprehending all individuals with gender incongruence or nonconformity (transsexual, transvestite, genderqueer etc). Cisgender is a neologism used to refer to individuals with a gender identity and expression matching the sex assigned at birth, which eliminates the discrimination implied in the comparison of “trans” versus “normal” gender identities.
Gender dysphoria. Distress and discomfort that transgender individuals may (or not) experience, mainly as a result of social perceptions and stigmatization or their own rejection. The resulting social isolation may promote the development of low self-esteem, school failure or employment difficulties and psychiatric disorders such as anxiety, depression and self-harm.
Transsexual. Often used interchangeably with transgender, although some sources qualify that this term exclusively refers to individuals with gender incongruence that feel uncomfortable with their bodies and resort to hormone therapy or surgery to have their bodies matched their gender identity. This process is known as gender affirmation. A trans man is a person assigned female sex at birth with a male gender identity, and a trans woman a person assigned male sex at birth with a female gender identity.
Transvestite. Individual with gender nonconformity that dresses in a manner that is culturally associated with the opposite sex. It is a form of gender expression: these individuals usually do not usually feel a mismatch with the sex assigned at birth.
Genderqueer. Individuals that identify as queer reject the binary male/female gender construct and position themselves in a dynamic and flexible spectrum that combines aspects of both genders without identifying with either.
Gender diversity. Term encompassing both gender incongruence and nonconformity.
Sexual orientation. Physical, emotional or affectual attraction towards individuals of a specific sex (opposite sex: heterosexuality, same sex: homosexuality) or both sexes (bisexuality). Another possibility is the absence of any such attraction (asexuality).
This is different from gender identity, so there are heterosexual, homosexual, bisexual and asexual trans men and trans women.
LGTBQI. Acronym encompassing sexual and gender diversity of (lesbian, gay, trans, bisexual, queer, intersex).
REFERENCES
- Riaño I, del Río I, Chueca M, Gabaldón S, de Montalvo F. Posicionamiento técnico de la Asociación Española de Pediatría en relación con la diversidad de género en la infancia y la adolescencia: mirada ética y jurídica desde una perspectiva multidisciplinar. An Pediatr (Barc). 2018;89:123.e1-6.
- Mora C, Guerrero J, Itza N, Ortiz A, González I. Cambios físicos y analíticos en menores transexuales bajo tratamiento médico. Rev Esp Endocrinol Pediatr. 2017;8:29-39.
- Gray S, Sweeney K, Randazzo R, Levitt H. “Am I doing the right thing?”: pathways to parenting a gender variant child. Fam Process. 2016;55:123-38.
- Dirección General de Servicios Sociales de la Consejería de Asuntos Sociales. Guía de Atención a Menores con Diversidad de género: programa LGTB de la Comunidad de Madrid. Consejería de Asuntos Sociales. In: comunidad.madrid/publicamadrid [online] [accessed 10/07/2020]. Available at www.madrid.org/bvirtual/BVCM013919.pdf
- Soler C. Acompañamiento a familias con hijas e hijos con identidades trans: un acercamiento desde la perspectiva familiar y profesional de la intervención social. In: Climent M, Carmona M (coords.). Transpsiquiatría. Abordajes queer en salud mental. Madrid: AEN Digital; 2018. p. 143-59.
- Glaser BG, Strauss AL. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine Transaction; 1967.
- Alizade M. La liberación de la parentalidad en el siglo XXI. In: Imago Agenda [online] [accessed 10/07/2020]. Available at www.imagoagenda.com/articulo.asp?idarticulo=1323
- Solis L. Acerca de las bases psicoanalíticas del estudio de la parentalidad. Grafo Working Papers. 2014;3:1-5.
- Kübler-Ross E. Sobre la muerte y los moribundos. 3.ª ed. Barcelona: Grijalbo; 1993.
- Olson-Kennedy J, Forcier M. Management of transgender and gender-diverse children and adolescents. In: UpToDate [online] [accessed 15/04/2020] Available at www.uptodate.com/contents/management-of-transgender-and-gender-diverse-children-and-adolescents
- Chew D, Anderson J, Williams K, May T, Pang K. Hormonal treatment in young people with gender dysphoria: a systematic review. Pediatrics. 2018;141:e20173742.
- Edwards-Leeper L, Spack NP. Psychological evaluation and medical treatment of transgender youth in an interdisciplinary “Gender Management Service” (GeMS) in a major pediatric center. J Homosex. 2012;59:321-36.
- Durwood L, McLaughlin KA, Olson KR. Mental health and self-worth in socially transitioned transgender youth. J Am Acad Child Adolesc Psychiatry. 2017;56:116-23.
- Olson KR, Durwood L, DeMeules M, McLaughlin KA. Mental health of transgender children who are supported in their identities. Pediatrics. 2016;137:e20153223.
- Zucker KJ. Gender identity disorder in children and adolescents. Annu Rev Clin Psychol. 2005;1:467-92.
- Yunger JL, Carver PR, Perry DG. Does gender identity influence children’s psychological well-being? Dev Psychol. 2004;40:572-82.
- Rosen AC, Rekers GA, Friar LR. Theoretical and diagnostic issues in child gender disturbances. J Sex Res. 1977;13:89-103.
- De Vries AL, McGuire JK, Steensma TD, Wagenaar EC, Doreleijers TA, Cohen-Kettenis PT. Young adult psychological outcome after puberty suppression and gender reassignement. Pediatrics. 2014;134:696-704.
- De Vries AL, Steensma TD, Doreleijers TA, Cohen-Kettenis PT. Puberty suppression in adolescents with gender identity disorder: a prospective follow-up study. J Sex Med. 2011;8:2276-83.
- Honneth A. La lucha por el reconocimiento: por una gramática moral de los conflictos sociales. Barcelona: Crítica; 1997.
- World Health Organization. Género y salud. 2018 [online] [accessed 15/04/2020] Available at www.who.int/es/news-room/fact-sheets/detail/gender
- Mallon GP, DeCrescenzo T. Transgender children and youth: a child welfare practice perspective. Child Welfare. 2006;85:215-41.
- Piper J, Mannino M. Identity formation for transsexual individuals in transition: a narrative famility therapy model. J GLBT Fam Stud. 2008;4:75-93.
- Zosuls KM, Ruble DN, Tamis-Lemonda CS, Shrout PE, Bornstein MH, Greulich FK. The acquisition of gender labels in infancy: implications for gender-typed play. Dev Psychol. 2009;45:688-701.
- Carver P, Yunger JL, Perry DG. Gender identity and adjustment in middle childhood. Sex Roles. 2003;49:95-109.
- MacCoby EE. The two sexes: growing up apart, coming together. Cambridge: Harvard University Press; 1999.
Comments
This article has no comments yet.