
Vol. 28 - Num. 110
Original Papers
Contribution of primary care to the approach to mental health
Miguel Antoñón Rodríguez a, María Aldana Villamañánb, Cristina Rosillo Martínb, Hemir David Escobar Pirelaa
a, María Aldana Villamañánb, Cristina Rosillo Martínb, Hemir David Escobar Pirelaa
aServicio de Pediatría. Hospital Universitario de Torrejón. Torrejón de Ardoz. Madrid. España.
bMIR-Pediatría. Hospital Universitario de Torrejón. Torrejón de Ardoz. Madrid. España.
Correspondence: M Antoñón. E-mail: miguelantrod@hotmail.es
Reference of this article: Antoñón Rodríguez M, Aldana Villamañán M, Rosillo Martín C, Escobar Pirela HD. Contribution of primary care to the approach to mental health . Rev Pediatr Aten Primaria. 2026;28:187-93. https://doi.org/10.60147/3958bece
Published in Internet: 13-04-2026 - Visits: 2815
Abstract
Introduction: child and adolescent mental health is a growing public health challenge, with an overall prevalence of pediatric psychiatric disorders of 25% in Spain. In recent years, their incidence has increased alarmingly, as has the incidence of self-injurious thoughts and behaviors (SITBs), which is as high as 16% in the pediatric population.
Material and methods: retrospective observational study in a sample of 198 pediatric patients treated at a secondary hospital between 2019 and 2024 aimed at evaluating SITBs and the role of primary care in their management.
Results: in our sample, which was predominantly female (71.3%), the prevalence of SITBs was 33.3%. Significant risk factors identified included bullying (OR: 2.24) and psychiatric comorbidities (OR: 3.32). Mixed anxiety and depressive mood was associated with a ten-fold risk of SITBs compared to isolated anxiety. The value of primary care was reflected in the early diagnosis of cases that eventually reach greater clinical severity. The analysis identified early referral to specialized mental health services as a critical protective factor, significantly reducing the risk of SITBs (OR: 0.24).
Conclusions: our results underscore the role of primary care services in effectively screening for mental health disorders and detecting severe cases. It is imperative to reinforce this level of care with specific training and sufficient resources (in terms of both education and allocated time) to guarantee a preventive, comprehensive, and coordinated approach to pediatric psychosocial health.
Keywords
● Adolescent ● Childhood ● Mental health ● Self-Injurious Thoughts and Behaviors ● SuicideINTRODUCTION
Child and adolescent mental health is one of the greatest public health challenges today. In Spain, the prevalence of psychiatric disorders in children and adolescents is approximately 15% to 25%, reflecting a substantial increase in recent years.1,2 This sustained increase is placing a significant burden on health care systems and requires greater involvement from both primary care (PC) centers and pediatric emergency departments.
Within the spectrum of pediatric psychiatric disorders, most patients present features of anxiety or depression.3 A considerable proportion of this subset of patients (of up to 16%) exhibit non-suicidal self-injury or suicidal ideation or attempts.4 There is evidence of an increasing trend in the incidence of these behaviors, with a significantly higher frequency in the female population. They can serve multiple purposes, including relieving overwhelming emotions, restoring the integrity of the self during dissociative episodes, or social signalling.5 The current figures highlight the critical magnitude of this problem and evince the need to develop and implement effective management strategies to address it.
The objective of the study was to analyze the characteristics of pediatric patients with psychiatric disorders and to describe the associations between the implemented interventions and patient outcomes.
MATERIAL AND METHODS
We conducted a retrospective observational study in the pediatric emergency department of a secondary hospital, including all children aged less than 16 years treated for a psychiatric diagnosis (based on International Classification of Diseases, 10th Revision [ICD-10] codes,6 detailed in Table 1) between January 1, 2019 and December 31, 2024. We excluded patients whose health records contained only that single care episode to ensure a follow-up period of at least 12 months. For each patient, we reviewed both the previous history and the course and outcomes of the mental health disorder documented in the health records through June 1, 2025. The primary outcome was the presence of self-injurious thoughts and behaviors (SITBs), a composite variable that includes both non-suicidal self-injury and suicidal ideation or attempts.
| Table 1. ICD-10 codes by diagnostic category | ||
|---|---|---|
| ICD 10 | Diagnosis | |
| Anxiety | F06.4 | Anxiety disorder due to known physiological condition |
| F41.1 | Generalized anxiety disorder | |
| F41.8 | Other specified anxiety disorders | |
| F41.9 | Anxiety disorder, unspecified | |
| F43.20 | Adjustment disorder, unspecified | |
| F43.22 | Adjustment disorder with anxiety | |
| F43.23 | Adjustment disorder with mixed anxiety and depressed mood | |
| F93.0 | Separation anxiety disorder of childhood | |
| F93.8 | Other childhood emotional disorders | |
| Depression | F32.0 | Major depressive disorder, single episode, mild |
| F32.1 | Major depressive disorder, single episode, moderate | |
| F32.2 | Major depressive disorder, single episode, severe without psychotic features | |
| F32.3 | Major depressive disorder, single episode, severe with psychotic features | |
| F32.4 | Major depressive disorder, single episode, in partial remission | |
| F32.5 | Major depressive disorder, single episode, in full remission | |
| F32.9 | Major depressive disorder, single episode, unspecified | |
| F33.0 | Major depressive disorder, recurrent, mild | |
| F33.1 | Major depressive disorder, recurrent, moderate | |
| F33.2 | Major depressive disorder, recurrent severe without psychotic features | |
| F33.3 | Major depressive disorder, recurrent, severe with psychotic symptoms | |
| F33.41 | Major depressive disorder, recurrent, in partial remission | |
| F33.42 | Major depressive disorder, recurrent, in full remission | |
| F33.9 | Major depressive disorder, recurrent, unspecified | |
| Bipolar and mood disorders | F31.30 | Bipolar disorder, current episode depressed, mild or moderate severity, unspecified |
| F31.31 | Bipolar disorder, current episode depressed, mild | |
| F31.32 | Bipolar disorder, current episode depressed, moderate | |
| F31.4 | Bipolar disorder, current episode depressed, severe, without psychotic features | |
| F31.5 | Bipolar disorder, current episode depressed, severe, with psychotic features | |
| F31.75 | Bipolar disorder, in partial remission, most recent episode depressed | |
| F31.76 | Bipolar disorder, in full remission, most recent episode depressed | |
| F31.81 | Bipolar II disorder | |
| F31.9 | Bipolar disorder, unspecified | |
| F34 | Dysthymia, cyclothymia, persistent mood [affective] disorders | |
| Other | F23 | Acute and transient psychotic disorders |
| F23.8 | Other acute and transient psychotic disorders | |
| F43.23 | Adjustment disorder with mixed anxiety and depressed mood | |
| R45.851 | Suicidal ideations | |

The rest of the variables included in the multivariate model were selected based on their clinical relevance, based on the previous literature,7,8 and the quality of the data available in the health records. We prioritized variables related to risk factors and the care delivery process, particularly the role of primary care, in line with the objectives of our study.
Thus, we included sociodemographic variables such as date of birth, age (in years), sex, family type (nuclear, single-parent, separated, foster care, other), and year of onset; risk factors such as school bullying or psychiatric comorbidities (family history, substance use) and/or medical comorbidities (chronic diseases such as diabetes, cancer, or rheumatic diseases); and clinical variables such as the primary diagnosis established by a psychiatrist, classified into general categories (anxiety, depression, adjustment disorder with mixed anxiety with depressed mood, other). Owing to its high prevalence, we considered diagnostic code F43.23 separately. We collected data on the year of onset and the setting of diagnosis (emergency department, primary care, other).
In addition, we recorded primary care data: year of the first visit for a mental health complaint, total number of visits, initiation of treatment, referral to specialized mental health (MH) services, and adherence to follow-up at the primary care center, defined as attending at least three scheduled follow-up visits with the pediatrician following the initial diagnosis, along with documented adherence to the treatment plan and scheduled follow-up appointments.
The statistical analysis was performed with the software IBM SPSS Statistics, version 25. We compared categorical data with the χ2 test. Statistical significance was defined as p < 0.05. For data that did not follow a normal distribution, we used the Mann-Whitney U test. The probability of SITBs in relation to independent factors was determined by means of binary logistic regression. The study was approved by the Ethics Committee of our hospital (CEImHUV, code 2025.032).
RESULTS
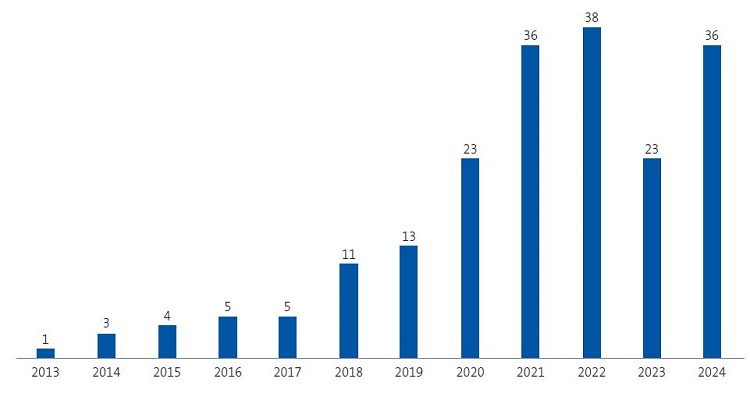
The study included a total of 198 patients (71.3% female) whose characteristics are summarized in Table 2. Self-injurious thoughts and behaviors were documented in 33.3% of cases. Figure 1 shows the annual incidence of pediatric psychiatric disorders in the sample, with a peak in year 2022.
| Table 2. Characteristics and psychosocial history of the patients with and without SITBs | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variable | SITBs | No SITBs | Χ2 | Fisher | p | OR | 95 CI | |
| Sex (n, %) | Female | 55 (39) | 86 (61) | 7.1 | <0.01 | 2.02 | 1.14-3.57 | |
| Male | 11 (19.3) | 46 (80.7) | ||||||
| Age in years (mean, SD) | 11.4 (2.6) | 11 (2.9) | ||||||
| Family structure (n, %) | Nuclear | 35 (34.7) | 66 (65.3) | 5.2 | 0.22 | |||
| Single-parent | 0 (0) | 4 (100) | ||||||
| Separated/divorced parents | 11 (55) | 9 (45) | ||||||
| Foster care | 20 (43.5) | 26 (56.5) | ||||||
| Other | 0 (0) | 1 (100) | ||||||
| Bullying (n, %) | 30 (53.6) | 26 (46.4) | 5.8 | <0.05 | 2.24 | 1.15-4.35 | ||
| Comorbidities (n, %) | Medical | 4 (20) | 16 (80) | 1.8 | 0.22 | |||
| Psychiatric | 28 (53.8) | 24 (46.2) | 13.4 | <0.01 | 3.32 | 1.72-6.41 | ||
| Primary diagnosis (n, %) | Anxiety | 23 (18.0) | 105 (82.0) | 39.8 | <0.01 | |||
| Depression | 2 (66.7) | 1 (33.3) | ||||||
| Mixed | 24(68.6) | 11 (31.4) | ||||||
| Other | 17 (23.1) | 15 (46.9) | ||||||
|
CI: confidence interval; OR: odds ratio; SITBs: self-injurious thoughts and behaviors. |
||||||||

| Figure 1. Annual incidence of psychiatric disorders |
|---|
 |

Self-injurious thoughts and behaviors were more frequent in patients with depression and mixed anxiety and depressed mood (p <0.01). Compared to anxiety alone, the risk of SITBs was tenfold in patients with a diagnosis of adjustment disorder with mixed anxiety and depressed mood (code F43.23) (OR: 10.0; 95% confidence interval [95 CI]: 4.3-23.1; p <0.01). We found no differences in the risk of SITBs between patients with a diagnosis of depression (OR: 9.1; 95% CI: 0.80-105.0; p = 0.08) and those with a diagnosis of anxiety.
We found a higher proportion of SITBs in patients in whom the psychiatric disorder was initially diagnosed at the primary care level (p < 0.01). Table 3 presents the data on the use of PC resources.
| Table 3. Use of primary care resources by patients with and without SITBs | |||||||
|---|---|---|---|---|---|---|---|
| Variable | SITBs | No SITBs | Χ2 | p | OR | 95 CI | |
| Visit (n, %) | Yes | 55 (33.3) | 110 (66.7) | 0.1 | 0.91 | 1.05 | 0.46-2.38 |
| No | 10 (32.3) | 21 (67.7) | |||||
| Treatment initiation (n, %) | Yes | 2 (12.5) | 14 (87.5) | 2.9 | 0.06 | 0.26 | 0.06-1.21 |
| No | 53 (35.1) | 98 (64.9) | |||||
| Referral to MH services (n, %) | Yes | 4 (10.0) | 36 (90.0) | 3.7 | <0.05 | 0.24 | 0.07-0.82 |
| No | 46 (35.9) | 82 (64.1) | |||||
| Adherence (n, %) | Yes | 25 (43.1) | 33 (56.9) | 3.4 | 0.08 | 0.69 | 0.45-1.05 |
| No | 29 (29.6) | 69 (70.4) | |||||
|
CI: confidence interval; MH: mental health; OR: odds ratio; SITBs: self-injurious thoughts and behaviors. |
|||||||

As regards the distribution of resources (Table 4), we found statistically significant differences in the number of both PC and specialized MH visits. The average number of PC visits was significantly greater in patients with SITBs compared to patients without these behaviors, with a similar trend in in MH visits.
| Table 4. Distribution of resources | ||||||
|---|---|---|---|---|---|---|
| Variable | With SITBs | Without SITBs | Average (SITB group) | Average (no SITB group) | Mann-Whitney | p |
| PC visits | 55 | 111 | 108.3 | 71.2 | 1689 | <0.01 |
| Specialized MH visits | 64 | 132 | 140.2 | 78.3 | 1555.5 | <0.01 |
|
MH: mental health; PC: primary care; SITBs: self-injurious thoughts and behaviors. |
||||||

DISCUSSION
Our results show a higher incidence of SITBs compared to the international literature. In 2022, Liu et al. reported a prevalence of SITBs of 21.3%, with approximately 17% of patients with suicidal ideation transitioning to attempting suicide. This underscores the magnitude of the problem and the need for strategies allowing early identification. In Spain, the number of pediatric emergency department visits related to SITBs has increased in recent years,1,9 mainly on account of girls and female adolescents.1,3
Our findings highlight the protective role of PC services. Paradoxically, the proportion of patients engaging in SITBs was higher among patients with psychiatric disorders first identified at the PC level, which probably reflects a greater likelihood of detection of potentially severe cases and adequate screening at this care level. This suggests that PC pediatricians are effective at screening for psychiatric disorders, with greater accuracy in the detection of more severe cases. In this regard, the American Academy of Pediatrics recommends universal screening for suicide risk at age 12 years to enable early identification and intervention. 10 Primary care is frequently the first point of contact with the health care system in Spain. However, although the foundations for a nationwide strategic plan have already been set, routine screening of children and adolescents has not yet been officially introduced.11
Although it was not statistically significant, we observed that both initiation of treatment and adherence to follow-up at the PC level tended to exhibit a protective effect. This suggests that seeking care at the PC level does not provide any benefit unless it is accompanied by prompt and appropriate management.10 In general, health care professionals in the field of pediatrics consider that they receive insufficient training to competently address issues related to mental health overall and suicidal ideation and behavior in particular.12 Adequate training13 and being allowed sufficient time to address these issues in the office14 both contribute to improving the quality of care.
There is already evidence that integrating mental health in primary care improves outcomes in the pediatric population.9,15 Our findings demonstrate that referral to specialized MH services is associated with a clear improvement in outcomes in these patients.
With regard to resource utilization, our results indicate that patients who develop SITBs make greater use of both primary care and specialty care resources. Compared to the international literature, although most at-risk adolescents seek care at the PC level within 6 months of onset, only a minority access specialized mental health services.16 This suggests that primary care serves as a critical point of contact for the identification of mental health disorders and appropriate referral, although there is a significant gap in access to specialized services.
The strengths of our study include the large size of its sample, which therefore provides a realistic reflection of real-world clinical practice. The use of electronic health records as a source of data ensured the systematic collection of information and reduced the risk of recall bias. The analysis included multiple variables, providing a comprehensive view of the study population and care pathways, with particularly emphasis on the role of primary care. In addition, it focused on a clinically relevant issue whose impact is increasingly growing, providing useful information for improving detection, coordinating care, and designing preventive strategies.
As for the limitations of our study, we should highlight that we did not distinguish between different forms of SITBs or the intent behind them. In addition, selection bias may have resulted in the overestimation of the severity of the cases. There is also a risk of observer bias, as the selection of patients based on the health records may have limited the collected data, which could be incomplete or unavailable if part of the follow-up took place in the private health care system or in the health care systems of other regions in Spain.
CONCLUSIONS
Our findings confirm that early identification and management of psychiatric disorders at the PC level significantly improve outcomes in these patients. Primary care plays a key role as the entry point to health care services and the primary resource for the long-term follow-up of children and adolescents. Our study found that close follow-up and, in particular, effective referral to specialized MH services from the PC center are directly associated with a reduced risk of SITBs.
We must also emphasize the urgent need to reinforce PC services by allocating specific resources, allowing adequate time for the visits, and providing ongoing training for health care professionals. Establishing standardized screening protocols at the PC level would not only enable more efficient detection of severe cases, but would also help optimize the use of health care resources, allowing for more sustainable management of the growing demand for child and adolescent mental health services.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the presentation and publication of this article.
AUTHORSHIP
All authors contributed equally to the published manuscript.
An earlier version of this paper was presented at the annual conference of the Spanish Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria in Seville, Spain, in October 2025.
ABBREVIATIONS
CI: confidence interval · ICD: International Classification of Diseases · MH: mental health · OR: odds ratio · PC: Primary Care · SH: self-harm.
REFERENCES
- Kieling C, Buchweitz C, Caye A. Worldwide Prevalence and Disability From Mental Disorders Across Childhood and Adolescence: Evidence From the Global Burden of Disease Study. JAMA Psychiatry. 2024;81(4):347-56. https://doi.org/10.1001/jamapsychiatry.2023.5051
- Thapar A, Eyre O, Patel V, Brent D. Depression in Young People. Lancet. 2022;400(10352):617-31. https://doi.org/10.1016/S0140-6736(22)01012-1
- Mojtabai R, Olfson M. Trends in Mental Disorders in Children and Adolescents Receiving Treatment in the State Mental Health System. J Am Acad Child Adolesc Psychiatry. 2024;S0890-8567(24)01357-1. https://doi.org/10.1016/j.jaac.2024.08.008
- Liu RT, Walsh RFL, Sheehan AE, Cheek SM, Sanzari CM. Prevalence and Correlates of Suicide and Nonsuicidal Self-injury in Children: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2022;79(7):718-26. https://doi.org/10.1001/jamapsychiatry.2022.1256
- Suárez AD, Espina CC. Principales patologías psiquiátricas en Urgencias Pediátricas. Pediatr Integral. 2024; XXVIII(2):103-08.
- World Health Organization. CIE-10: Clasificación internacional de enfermedades y problemas relacionados con la salud. 10.ª Rev. In: WHO [online] [accessed 17/02/2026]. Available at platform.who.int/docs/default-source/mca-documents/policy-documents/guideline/NIC-CC-55-01-GUIDELINE-2018-esp-CIE-10-Volume2.pdf
- Gertner A, Easterly CW, DeSilva S, Shafer PR, Lombardi B, Hunt-Harrison T, et al. Changes in the Proportion of Office-Based Child and Adolescent Physician Visits Addressing Mental Health, 2005-2019. Psychiatr Serv. 2026;77(1):49-57. https://doi.org/10.1176/appi.ps.20240553
- Yonek J, Lee C, Harrison A, Mangurian C, Tolou-Shams M. Key Components of Effective Pediatric Integrated Mental Health Care Models: A Systematic Review. JAMA Pediatr. 2020;174(5):487-98. https://doi.org/10.1001/jamapediatrics.2020.0023
- Vázquez López P, Armero Pedreira P, Martínez-Sánchez l, García Cruz JM, Bonet de Luna C, Notario Herrero F, et al. Autolesiones y conducta suicida en niños y adolescentes. Lo que la pandemia nos ha desvelado. An Pediatr. 2023;98:204-12. https://doi.org/10.1016/j.anpedi.2022.11.006
- Hua LL, Lee J, Rahmandar MH, Sigel EJ. Suicide and Suicide Risk in Adolescents. Pediatrics. 2024;153(1):e2023064800. https://doi.org/10.1542/peds.2023-064800
- Ministerio de Sanidad. Plan de acción para la prevención del suicidio 2025-2027. Madrid: Ministerio de Sanidad; 2024 [online] [accessed 17/02/2026]. Available at https://www.sanidad.gob.es/areas/calidadAsistencial/estrategias/saludMental/docs/Plan_de_accion_para_la_prevencion_del_suicidio_2025_2027.pdf
- Díez Suárez A, Carballo JJ, Sánchez-Pina C. Acerca de la salud mental y el suicidio en niños y adolescentes. An Pediatr. 2023;98:401-92. https://doi.org/10.1016/j.anpedi.2023.04.003
- McMillan JA, Land M Jr, Leslie LK. Educación en residencia pediátrica y la crisis conductual y de salud mental: un llamado a la acción. Pediatrics. 2017;139(1):e20162141. https://doi.org/10.1542/peds.2016-2141
- Cooper S, Valleley RJ, Polaha J, Begeny J, Evans JH. Running out of time: physician management of behavioral health concerns in rural pediatric primary care. Pediatrics. 2006;118(1):e132-8. https://doi.org/10.1542/peds.2005-2612
- Glenn CR, Esposito EC, Porter AC, Robinson DJ. Evidence Base Update of Psychosocial Treatments for Self-Injurious Thoughts and Behaviors in Youth. J Clin Child Adolesc Psychol. 2019;48(3):357-92. https://doi.org/10.1080/15374416.2019.1591281
- Sayal K, Yates N, Spears M, Stallard P. Service use in adolescents at risk of depression and self-harm: prospective longitudinal study. Soc Psychiatry Psychiatr Epidemiol. 2014;49(8):1231-40. https://doi.org/10.1007/s00127-014-0843-y