
Vol. 28 - Num. 109
Original Papers
Assessment of parental knowledge about risk factors for sudden infant death syndrome after neonatal hospital discharge
Manuel Roa Prietoa, María López Marcosb, M.ª Paz García-Tenorio Balmasedac
aPediatra. CS Pinto. Madrid. España.
bPediatra. CS La Candelaria. Sevilla. España.
cFarmacéutica. Villafranca de los Caballeros. Toledo. España.
Correspondence: M Roa. E-mail: mroa610@gmail.com
Reference of this article: Roa Prieto M, López Marcos M, García-Tenorio Balmaseda MP. Assessment of parental knowledge about risk factors for sudden infant death syndrome after neonatal hospital discharge . Rev Pediatr Aten Primaria. 2026;28:31-8. https://doi.org/10.60147/68197667
Published in Internet: 25-02-2026 - Visits: 4022
Abstract
Objectives: sudden infant death syndrome (SIDS) is a leading cause of death in infants under one year. Despite known preventive measures, parental knowledge is often insufficient. This study assessed parental level of knowledge about SIDS prevention at the first newborn check-up at the primary care center and analyzed whether parental educational level influenced this knowledge.
Methods: we conducted a cross-sectional observational study in the Community of Madrid including 40 parents of newborns attending their first pediatric care appointment. A questionnaire was used to collect data on sociodemographic characteristics and knowledge about preventive measures against SIDS, completed on a voluntary basis. We analyzed differences based on educational attainment, number of children, type of hospital, and sex of the respondent.
Results: 97.5% correctly identified the supine sleeping position. There was confusion regarding other measures, such as bed-sharing or the use of anti-roll devices. We found significant differences based on educational attainment (p = 0.008), with university-educated parents scoring higher. Mothers demonstrated better knowledge than fathers (p = 0.027). There were no significant differences based on the number of children or type of hospital.
Conclusions: educational attainment is significantly associated with knowledge of preventive measures against SIDS. While most respondents recognized the correct sleeping position, there were still gaps in other areas, underscoring the need for tailored educational interventions in primary care, particularly aimed at less-educated parents.
Keywords
● Education status ● Sudden infant deathINTRODUCTION
Sudden infant death syndrome (SIDS) is one of the leading causes of death in infants under one year in developed countries. The definition of SIDS is sudden and unexplained death in an infant aged less than one year that remains unexplained after a thorough investigation, including the performance of a complete autopsy and review of the circumstances of death and the clinical history.1 In Spain, SIDS continues to be one of the leading causes of death in infants. In 2023, a total of 51 deaths due to SIDS (R95) were recorded, corresponding to a rate of 5.9 per 100 000 live births.2 Although the etiology of SIDS has yet to be fully elucidated, several risk factors have been identified, along with preventive strategies proven to significantly reduce its incidence.
One of the most relevant factors in the prevention of SIDS is the sleeping position of the infant. From the time educational campaigns recommending that babies sleep on their backs were first implemented, the incidence of SIDS has decreased significantly in many countries, with reductions of up to 81% in countries such as the United Kingdom.3-5 In contrast, sleeping in the prone or lateral position has been associated with an increased risk of SIDS.6
Despite the evidence, observational studies conducted in samples of families in Spain evince incomplete adherence to safe sleep recommendations, including the persistence of risky practices.7 Factors such as educational attainment, cultural beliefs, and the information provided by health care professionals affect the implementation of these preventive measures.8 In this regard, the primary care pediatrician plays a key role, as the first medical visits of the infant provide a crucial opportunity to educate parents about safer infant sleep practices. There is evidence suggesting that lower educational attainment may be a risk factor that increases the probability of SIDS,4 but there is insufficient evidence on whether a lack of information regarding the measures to prevent SIDS in these parents contributes to this association, and primary care pediatricians could affect the amount of information received by these families, thereby reducing risk.
The primary objective of the study was to assess parental knowledge about SIDS prevention strategies, particularly the importance of the supine sleeping position, during their first visit to the primary care pediatrician. A secondary objective was to assess whether parental educational attainment is associated with the level of knowledge about these recommendations. The primary hypothesis of the study was that a large percentage of parents would be aware of the most important preventive measures; as a secondary hypothesis, we expected that parents with lower educational attainment would be less informed about measures to prevent SIDS. The purpose of the study was to identify potential gaps in information and enable the improvement of educational strategies for prevention of SIDS implemented at the primary care level. To this end, we conducted an online survey through the Google Forms platform, collecting data on variables such as parental age, educational attainment, and number of previous children. The questionnaire also asked about the correct sleeping position for infants and eight more items regarding secondary measures for prevention of SIDS.
METHODS
Cross-sectional observational, descriptive and analytical study with the objective of describing and assessing parental knowledge of protective factors that reduce the risk of SIDS at the time of the first visit to the primary care pediatrician. In addition, we aimed to assess variables that could affect knowledge of preventive measures, such as educational attainment, previous children, or the type of hospital where the infant was born (public or private).
The study universe consisted of the parents of newborn infants attending the first visit to the pediatrician at one primary care center in the Community of Madrid. The sample included all parents who agreed to participate on a voluntary and anonymous basis by completing a custom questionnaire that has not been validated (Appendix 1). Participation was not restricted based on variables like age or sex, and the sole exclusion criteria were refusal to participate or the infant having required hospital admission due to prematurity, as parents in the latter case tend to receive more thorough information regarding the prevention of SIDS. The data were collected between January 5 and August 5, 2025, inviting all parents of neonates who attended the first visit to participate. The study was not approved by an ethics committee, as it did not involve collection of sensitive data and participation was both voluntary and anonymous.
The data were collected through a Google forms questionnaire specifically developed to assess parental knowledge about preventive measures against SIDS. The questionnaire included items on:
- Sociodemographic characteristics: age, educational attainment, parent who completed the questionnaire (mother or father).
- Previous history: number of children and place of birth of the infant (public or private hospital).
- Knowledge about SIDS: respondents were asked a direct question about the position in which infants should sleep; subsequently, a second question was included about secondary measures for preventing SIDS, which included four correct and four incorrect statements.
A correct answer in the item concerning the infant’s sleeping position was given a score of 4 points, while, in the second part of the questionnaire designed to assess more specific knowledge about SIDS prevention, one point was added to the score for each correct answer, and one point subtracted for each incorrect answer. This section assessed key aspects that affect the risk of sudden death, such as the use of soft mattresses, anti-roll devices, or pacifiers, exposure to tobacco smoke, co-sleeping, and breastfeeding. This scoring system was adopted to give more weight to the main preventive measure, which is having infants sleep in the supine position.
The collected data were exported to an Excel spreadsheet for analysis. We calculated the frequency of correct answers regarding SIDS preventive measures in the entire sample. We also compared these results according to the educational attainment of the respondents with the Student t-test, as the assumption of normality was met. We used the jamovi software package to perform all the analyses. To facilitate the analysis of the data, we divided participants in two groups according to educational attainment (parents who had a university degree and parents who did not), which allowed us to carry out the analysis without reducing the statistical power. Similarly, we grouped respondents according to whether or not they had other children, without taking into account the total number of children.
Finally, the Mann-Whitney U test was used to compare the scores obtained according to the parent who completed the questionnaire (father or mother) and the type of hospital where the child was born (public or private).
RESULTS
After collecting demographic data on the sample of respondents (Table 1), we found that the variables were distributed evenly in terms of whether the respondent was the father or mother, or whether the respondent had a university degree or not. However, they were not distributed based on whether the infant was born in a public or a private hospital. The descriptive analysis showed that, of the 40 respondents, 97.5% (n = 39) correctly identified the supine position as the appropriate sleeping position for an infant. Regarding the secondary measures that parents considered appropriate for reducing the risk of SIDS (Figure 1), most participants correctly identified avoiding exposure to tobacco smoke and promoting breastfeeding as protective factors.
| Table 1. Demographic characteristics of the respondents | |||||
|---|---|---|---|---|---|
| Type of hospital | Public | Private | |||
| 34 | 6 | ||||
| Responding parent | Mother | Father | |||
| 20 | 20 | ||||
| Number of previous children | 0 | 1 | 2 | 3 | >3 |
| 28 | 9 | 2 | 0 | 1 | |
| Educational attainment | Primary education | ESO | Bachillerato | Undergraduate degree | Doctorate |
| 1 | 6 | 8 | 23 | 2 | |
| Mean age | Fathers (SD) | Mothers (SD) | |||
| 36.18 (5.04) | 33.5 (4.72) | ||||
| Bachillerato: noncompulsory secondary education; ESO: compulsory secondary education. | |||||

| Figure 1. Knowledge of secondary preventive measures |
|---|
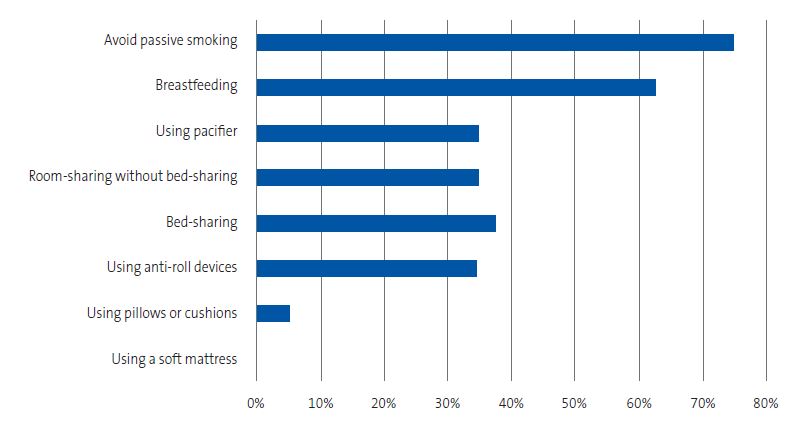 |

On the other hand, 37.5% and 35%, respectively, mistakenly believed that practices such as sharing the bed with parents or using anti-roll devices help reduce the risk of SIDS. Finally, as can be seen in Figure 1, 100% and 95%, respectively, correctly answered that the use of soft mattresses, pillows, or cushions is discouraged as a preventive measure against SIDS.
In the inferential analysis of the results, we compared the questionnaire scores according to educational attainment (respondents with a university degree versus respondents without a university education). We used the Shapiro-Wilk test to assess the distribution of the scores, which showed that the data were normally distributed and the Student t test could be applied. There was a statistically significant difference between the groups (p <0.05), with respondents with university degrees scoring better in the test assessing knowledge of the risk factors for SIDS. The mean score in university-educated respondents was 5.68 points out of a maximum possible 8 points, compared to 4.13 points in the group with lower educational attainment (Table 2).
| Table 2. Description of results according to educational attainment | ||||||
|---|---|---|---|---|---|---|
| Group | N | Mean | Median | SD | SE | 95 CI |
| University degree | 25 | 5.68 | 6.00 | 1.57 | 0.315 | 5.06-6.30 |
| No university degree | 15 | 4.13 | 4.00 | 1.85 | 0.477 | 3.20-5.06 |
| SD: standard deviation; SE: standard error; 95 CI: 95% confidence interval. | ||||||

Similarly, we compared the questionnaire scores in respondents who had previous children versus those who did not with the Mann-Whitney U test, given that the data did not fit a normal distribution. There were no significant differences between these two groups. We used the same test to compare scores according to the type of hospital where the infant had been born (public or private) and also found no significant differences.
In contrast, when we compared scores with the Mann-Whitney U test according to who had completed the questionnaire (father or mother), we did find statistically significant differences. Thus, the mean score of mothers was higher compared to parents (Table 3).
| Table 3. Description of results according to sex of respondent | ||||||
|---|---|---|---|---|---|---|
| Group | N | Mean | Media | SD | SE | 95 CI |
| Father | 20 | 4.40 | 5.00 | 1.85 | 0.413 | 3.59-5.21 |
| Mother | 20 | 5.80 | 6.00 | 1.54 | 0.345 | 5.13-6.47 |
| SD: standard deviation; SE: standard error; 95 CI: 95% confidence interval. | ||||||

DISCUSSION
In our study, during the first visit to the primary care pediatrician, most parents correctly identified the supine position as the safest sleeping position for infants. This finding is consistent with previous evidence and suggests that the key messages of safe sleep campaigns have been internalized by a large part of the population, probably thanks to their reinforcement in both hospital and primary care settings.4,5 Recent studies in the Spanish population have yielded similar results, with a good level of awareness of the recommendation to use the back sleeping position, although other risky practices persist.7
However, despite the adequate knowledge of the supine position, our results show significant gaps in the recognition of other preventive measures, such as the risk associated with bed-sharing or the use of anti-roll devices. This pattern, which has been described in previous studies, could be explained by the false sense of safety that may be associated with culturally accepted practices, such as co-sleeping, as well as by the lack of clear and consistent messages from health care professionals.7,9
In relation to the factors associated with the level of knowledge of preventive measures against SIDS, our study showed a statistically significant association with parental educational attainment. This finding is consistent with those of previous studies that identified educational attainment as a relevant social determinant in the acquisition of health-related knowledge and the adoption of preventive behaviors.8 This educational gradient may be explained by differences in health literacy, in the access to reliable sources of information and in the capacity to understand complex recommendations. However, our results suggest that educational attainment, rather than an independent risk factor, could act as a mediator involving the accessibility and comprehension of preventive information, which opens a window of opportunity for intervention at the primary care level.
One particularly interesting finding was that, in the comparison by parent, mothers exhibited a higher level of knowledge compared to fathers. This could be related to a greater involvement of mothers as primary caregivers and greater maternal exposure to health information during pregnancy and the postpartum period. This finding underscores the need to actively involve both parents in educational interventions, avoiding the exclusive delivery of preventive information to mothers.
The first checkup of the newborn in the primary care system is a strategic moment for the delivery of preventive intervention, as it occurs at a stage when parents are most receptive and allows the message to be adapted to their sociocultural context and health literacy level. Our results highlight that, while certain key messages have taken root in the population, there are still gaps in knowledge that require a more personalized educational approach. In this regard, primary care pediatricians not only act as vehicles for conveying information, but also as agents for identifying groups at risk of misinformation, as they can identify parents with lower comprehension and reinforce preventive messages in clear and simple language that is easy to understand, all of it tailored to the parents’ needs.
There are several limitations to this study that must be considered when interpreting its results. First of all, the small sample size may limit the generalization of the findings and the statistical power of the subgroup analyses. In addition, there is a risk of selection bias, as parents with greater awareness may have been more likely to participate, which would lead to overestimation of the actual level of knowledge in the study population. Finally, the variation based on the parent who completed the questionnaire, with significant differences between mothers and fathers, may have been a source of information bias.
In respect of future lines of research, it would be interesting to perform multicenter studies with larger and more representative samples allowing for a more in-depth exploration of sociocultural and geographical differences. Likewise, it would be useful to carry out longitudinal studies assessing not only self-reported knowledge, but also the actual implementation of preventive measures in the home and the temporal trends in their implementation, with the aim of designing more effective and equitable educational interventions.
CONCLUSIONS
Our study shows that most parents can correctly identify the supine decubitus position as the safest sleeping position for infants at the time of the first visit to the primary care pediatrician, which is indicative of an adequate dissemination of this preventive message. However, we identified relevant gaps in the knowledge of other preventive measures against SIDS, for instance, regarding the risks of co-sleeping or the inappropriate use of anti-roll devices, which highlights the need to reinforce health education strategies beyond the basic recommendations.
Furthermore, the findings corroborated that parental educational attainment is significantly associated with their level of knowledge about SIDS preventive measures, with parents with higher attainment demonstrating a more comprehensive understanding of these recommendations. This finding highlights the importance of considering health literacy and social determinants when designing preventive interventions, avoiding a one-size-fits-all approach and promoting the delivery of education tailored to the characteristics of each family.
Primary care (particularly in the context of the first routine check-up of the newborn) is a key setting for identifying information gaps and implementing personalized educational strategies. Proactive intervention by pediatricians is essential to ensure that preventive knowledge is transmitted effectively and equitably, helping to reduce health inequities and minimize the risk of SIDS in the pediatric population.
Lastly, we recommend expanding the scope of future research on the subject, performing studies in larger and more representative samples and assessing not only self-reported knowledge, but also the practical implementation of preventive measures in the family environment, with the ultimate goal of optimizing preventive strategies against SIDS with a holistic and family-centered perspective.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
AUTHORSHIP
All authors contributed equally to the writing of the published manuscript.
ABBREVIATIONS
SIDS: sudden infant death syndrome.
REFERENCES
- Fraile Martínez O, García Montero C, Castellanos Díez S, Bravo‑Blázquez C, Quintana Coronado MG, López González l, et al. Sudden Infant Death Syndrome (SIDS): State of the Art and Future Directions. Int J Med Sci. 2024;21(5):848. https://doi.org/10.7150/ijms.89490
- Ministerio de Sanidad. Patrones de mortalidad en España, 2023. Madrid: Ministerio de Sanidad; 2025 [online] [accessed 07/01/2026]. Available at www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/mortalidad/docs/Patrones_Mortalidad_2023.pdf
- Moon RY; Task Force on Sudden Infant Death Syndrome. SIDS and other sleep-related infant deaths: evidence base for 2016 updated recommendations for a safe infant sleeping environment. Pediatrics. 2016;138(5):e20162940. https://doi.org/10.1542/peds.2016-2940
- Centers for Disease Control and Prevention (CDC). Trends in SUID rates by cause of death, 1990-2022 (includes SIDS R95). Atlanta (GA): CDC [online] [accessed 07/01/2026]. Available at www.cdc.gov/sudden-infant-death/data-research/data/sids-deaths-by-cause.html
- The Lullaby Trust. Back to Sleep campaign anniversary statement. London: The Lullaby Trust; 2016 [online] [accessed 07/01/2026]. Available at www.lullabytrust.org.uk
- Task Force on Sudden Infant Death Syndrome. SIDS and other sleep-related infant deaths: Updated 2016 recommendations for a safe infant sleeping environment. Pediatrics. 2016;138(5):e20162938. https://doi.org/10.1542/peds.2016-2938
- Ruiz Botia I, Cassanello Peñarroya P, Díez Izquierdo A, Martínez Sánchez JM, Balaguer Santamaria A. Síndrome de muerte súbita del lactante: ¿siguen las familias las recomendaciones? An Pediatr (Barc). 2020;92(4):222-8. https://doi.org/10.1016/j.anpedi.2019.06.011
- Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol. 1991;11(5):677-84. https://doi.org/10.3109/15513819109065465
- Vennemann MM, Hans-Werner H, Bajanowski T, Blair PS, Complojer C, Moon RY, et al. Bed-sharing and the risk of sudden infant death syndrome: can we resolve the debate? BMJ Open. 2014;4:e004323. https://doi.org/10.1016/j.jpeds.2011.06.052