
Vol. 25 - Num. 100
Original Papers
Reading promotion and its association with professional vocations and care settings
Ana Garach Gómeza, Iván Gutiérrez Garcíab, Antonio Molina Carballoc, Jesús L. Megíasd
aPediatra. CS Zaidín Sur. Granada. España.
bPediatra. Hospital Universitario Nuestra Señora de la Candelaria. Santa Cruz de Tenerife. España
cPediatra. Departamento de Pediatría. Facultad de Medicina. Universidad de Granada. Granada. España.
dPsicólogo. Departamento de Psicología Experimental. Facultad de Psicología. Universidad de Granada. Granada. España.
Correspondence: A Garach. E-mail: anagarach@hotmail.com
Reference of this article: Garach Gómez A, Gutiérrez García I, Molina Carballo A, Megías JL. Reading promotion and its association with professional vocations and care settings . Rev Pediatr Aten Primaria. 2023;25:377-87. https://doi.org/10.60147/76a271c6
Published in Internet: 21-11-2023 - Visits: 10771
Abstract
Introduction: healthy lifestyle promotion is a common practice among paediatricians. Reading promotion is included in that practice. It has numerous benefits for children: it stimulates brain activity and cognitive reserve, improves concentration and language development and helps develop emotional skills.
The aim of our study was to assess the implementation of reading promotion activities in real-world paediatric care practice, as well as its association with the underlying vocation for paediatrics (clinical, preventive or social) and the care setting (residency programme, hospital and primary care).
Material and methods: cross-sectional, descriptive study of national scope through an online survey of paediatrics residents and hospital-based and primary care paediatricians carried out in March 2022.
Results: 326 paediatricians participated, of who 16.8% worked in hospitals, 69.8% in primary care and were 13.4% paediatrics residents. Of this total, 18.8% reported a vocation for preventive care, 60.8% for clinical work and 20.5% for social paediatrics. In addition to carrying a detailed descriptive analysis of the type of reading promotion activities carried out in Spain, we found, firstly, that the vocation for medical practice was associated to the frequency of reading promotion (χ2(2)=13.11; p<0.001), with a higher proportion of paediatricians with a social vocation reporting performance of these activities. Secondly, the care setting also seemed to be a determining factor for the performance of these activities (χ2(2)=19.0; p<0.001), which were conducted more frequently in the primary care setting.
Conclusion: activities to promote reading are carried out mainly by primary care professionals within the framework of other health promotion work, and their performance was mainly associated with the greater proportion of primary care professionals with a vocation for social paediatrics.
Keywords
● Child development ● Health promotion ● Medical vocation ● Reading promotionINTRODUCTION
Although there are different definitions of the specialty of Paediatrics, the order of the Ministry of Health that approved the paediatrics curriculum in Spain (BOE-A-2006-17999) described it as the “comprehensive care of the individual during the period of human development ranging from conception to the end of adolescence”.
The functions of paediatrics are diverse and of a broad scope, as they include everything that concerns:
- Healthy child and adolescent care (preventive paediatrics).
- The comprehensive and holistic management and followup of children and adolescents with disease (clinical paediatrics).
- Interpersonal relationships and relationships with the community of healthy and ill children and adolescents within the physical and human environment in which their development unfolds continuously and with its particular characteristics (social paediatrics).1
Paediatric practice can take place in hospital or out-of-hospital settings, depending on the subspeciality. Of the 17 subspecialities recognised in the White Book of Paediatric Specialities endorsed by the Asociación Española de Pediatría (Spanish Association of Paediatrics),2 most are practiced in the hospital setting, while primary care paediatrics is the speciality practiced in dedicated outpatient health centres. According to data of the Ministry of Health for 2021, Spain has just over 4750 paediatricians working in hospitals, more than 1800 in training as medical residents3 and about 6600 working in out-of-hospital settings.4
The choice of the subspecialty and the area of work in which the paediatric professional carries out his or her practice depends to a large extent on his or her vocational interests. The medical vocation can be defined in several ways, but the one that may be most widely agreed on is that it is a strong calling to serve the patient and society that is motivated by personal experience and the surrounding environment.5 Based on the different functions of paediatrics, we can differentiate between paediatricians whose vocation leans more toward prevention, others with a more clinical vocation and others with a social vocation. Although all paediatric subspecialties concern themselves with disease in children and adolescents, the practice of paediatrics at the primary care level emphasises the importance of preventive care and a biopsychosocial approach. Its main goals are: on one hand, to provide and coordinate ongoing, comprehensive, child- and family-centred medical care in the environment in which the child grows and develops, from birth until physical growth and psychosocial development are completed; and, on the other hand, to provide individualized care, considering the social and community context of the patient with a population-based approach, avoiding an exclusive focus on risk groups.6
Thus, one of the defining features of primary care paediatrics is the promotion of healthy habits. Guidance on healthy habits must be age-appropriate, should start from the first medical visit and is in large part delivered in the framework of the child health prevention and promotion programme (routine “healthy child” visits). In this regard, primary care paediatricians are in a privileged position in relation to children and their families, as they are able to carry out a longitudinal followup of the child’s growth and development through age 14 years. The field of paediatrics encompasses the entire span of human neurodevelopment, so perhaps it would be preferable not to set the limit of paediatric age at 14 years, but at 18 years or even later, as is done in other countries. Positive health behaviours can have a very favourable impact on the development and the overall health of the child, as conceived from a biopsychosocial perspective.7
Among the recommendations offered in healthy child visits, there is one, the promotion of reading, that is becoming increasingly important given the evidence on its positive impact.8 Reading aloud in the first few years of life offers numerous benefits. Therefore, it is one of the activities that pediatricians could promote from the earliest check-ups. The following are some of its main benefits9:
- Reading aloud stimulates the activity of brain areas that have to do with narrative comprehension and the creation of mental images, which has an impact on oral and written language learning.
- It has an impact on the cognitive development of the child, by providing an opportunity to listen, think, feel, ask, answer, associate...
- It has a significant impact on language development, increasing language skills through the exposure to new words and more complex expressions than those heard in everyday conversation.
- It promotes familiarity with the language of books, which is more complex than spoken language.
- It allows working on the sphere of emotion: it creates intimacy between reader and listener in the moment, contributing to the formation and strengthening of affectional bonds, and helping express and share emotions.
Since the benefits of promoting reading from the paediatric care setting are so relevant and backed by evidence, it was necessary to determine the current situation of this practice in Spain and assess some of the factors that could have an impact on the degree to which it is pursued. To this end, the objectives of our study were, first, to explore the care settings where paediatricians work in Spain and their association with their original vocation in pursuing the profession and, second, to identify how many of the implemented reading promotion activities are carried out in the greater framework of health prevention, the types of activities performed and the barriers experienced in their implementation.
MATERIAL AND METHODS
Participants: A total of 326 pediatricians (273 female and 53 male) participated, with a mean age ± standard deviation (SD) of 47 ± 12.77 years (female: 46.8 ± 12.1; male: 51 ± 15.1). Of this total, 54 (16.8%) worked in hospital settings, 224 (69.8%) in primary care and 43 (13.4%) were doing their medical residency. All participants signed an informed consent form to participate in the survey and were contacted through mass mailings through the distribution lists of paediatric groups. The project was approved by the ethics committee of the University of Granada.
Study design: cross-sectional, descriptive and nationwide study, carried out through an online survey in March 2022. The inclusion criterion was that participants be actively practicing paediatrics at the time of the survey. The survey was performed through the platform Qualtrics version XM (2020).
Variables: we collected data for the following variables.
- Related to the participant: age, sex, number of children, setting where they carried out most of their professional activity (primary care, hospital or residency training), perceived workload (rated on a scale from 1 to 5, with 1 indicating a low load and 5 a very high load) and the number of years of experience as paediatricians.
- Concerning the population served, we asked participants to estimate the socioeconomic status and educational attainment (SES/EA) of the population they served through the MacArthur Scale of Subjective Social Status-adult version developed by Adler et al. (2000).10 This scale is a standardised instrument for assessing subjective social status. To administer this instrument, the respondent is presented with the drawing of a ladder with 10 rungs that correspond to different social class positions, ranging from 1 (lowest rung, lowest social class) to 10 (highest rung, highest social class). Participants were asked to choose the rung that best represented their catchment population, making a subjective estimate considering income, educational attainment and employment.
- The Official Programme of the Specialty of Paediatrics and its Subspecialities describes the scope of practice of paediatrics as the care of the healthy child and adolescent (preventive paediatrics), the comprehensive and holistic medical management and followup of the ill child and adolescent (clinical paediatrics) and the relationship and interactions of the healthy or ill child or adolescent with the community and immediate environment (social paediatrics).1 In relation to this, we asked participants which of these functions best represented their main vocation in their practice of medicine.
- Lastly, we asked respondents to estimate the time they devoted to health promotion activities. In addition, we asked about their performance of reading promotion activities, and, if they performed any, their frequency and type.
Statistical analysis: we conducted a descriptive analysis of the study variables calculating measures of central tendency and relative frque4ncies. We used one-way ANOVA to compare data regarding the participants themselves, conducted paired post hoc tests (Tukey test) and compared proportions with the χ2 test. We considered results with a p-value of less than 0.05 statistically significant. The data were analysed with the Jamovi statistical software, version 2.3.21.
RESULTS
Table 1 presents basic data about the participants (age, number of children, perceived workload and estimated SES/EA of the population they served) by care setting (hospital or primary care), creating a separate group for medical residents in training. The age of residents, as expected, was significantly younger compared to paediatricians working in hospitals and in primary care, and paediatricians in primary care were significantly older than those in hospitals. When it came to the number of children, there were no differences between hospital and primary care paediatricians. As for the perceived workload, residents were the group that reported the highest workloads. There were no significant differences in the estimated SES/EA of the catchment population based on the care setting.
| Table 1. Characteristics of the sample by care setting (mean ± SD) | |||||
|---|---|---|---|---|---|
| Hospital (n = 54) | Primary care (n = 224) | Residency (n = 43) | Fs (gl = 2) | p value | |
| Age | 43.3a ± 9.7 | 51.6b ± 9.9 | 28.1c ± 2.6 | 481 | p <0.001 |
| Number of children | 1.9a ± 1.1 | 1.9a ± 1.1 | 0.1b ± 0.4 | 212 | p <0.001 |
| Perceived workload | 3.7a ± 0.9 | 3.6a ± 0.9 | 4b ± 0.6 | 5.5 | p <0.05 |
| SES/EA of served population | 5.1 ± 1.50 | 5.3 ± 1.79 | 5.1 ± 1.38 | 0.62 | p = 0.54 |
|
Note: The different letters indicate statistically significant differences in each row of the 2 × 2 post hoc comparison (Tukey test). The absence of letters indicates that the value was not significantly different from any of the other values in the same row. SD: standard deviation; SES/EA: socioeconomic status and educational attainment. |
|||||
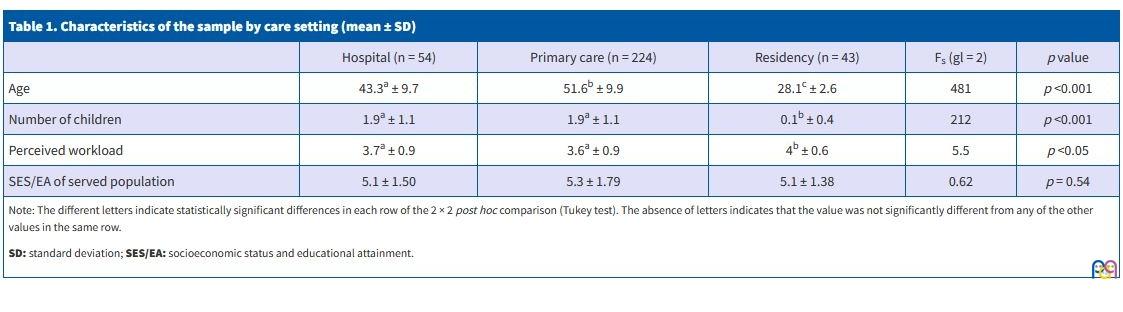
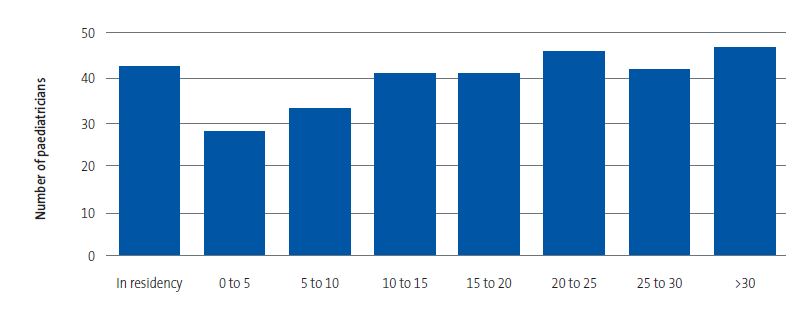
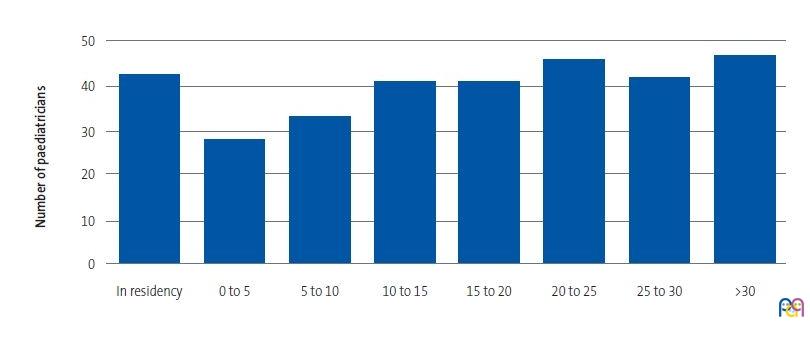
Figure 1 shows the distribution of participants by the number of years of professional experience. The first bar represents medical residents, and all other bars represent the rest of the participants (combining primary care and hospital-based paediatricians).
| Figure 1. Years of experience in paediatric care |
|---|
 |
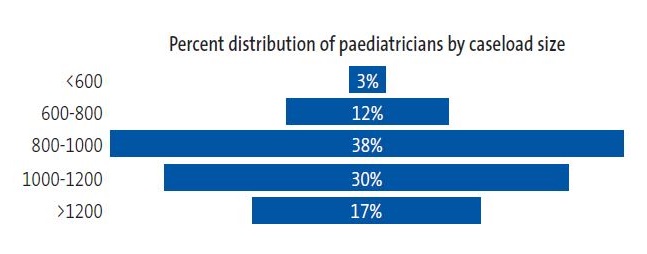
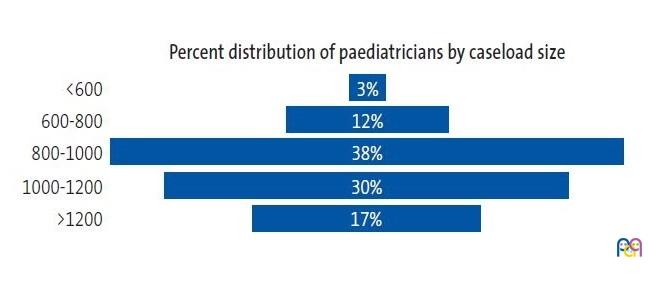
When it came to the caseloads of primary care paediatricians, they varied widely between participants. As can be seen in Figure 2 , these practitioners most frequently had caseloads of 800-1000 children (38%), followed by 1000-1200 children (30%) and caseloads greater than 1200 children (17%).
| Figure 2. Caseloads of primary care paediatricians |
|---|
 |
As regards the vocation reported by participants (preventive, clinical, or social paediatrics), Table 2 shows the distribution of the participants by vocation and care setting. The clinical vocation predominated in every care setting, although it was more prevalent among hospital-based providers and residents. On the other hand, primary care paediatricians reported a vocation for social paediatrics or for preventive paediatrics in greater proportions compared to the other two groups.
| Table 2. Vocation of respondents by care setting | |||||
|---|---|---|---|---|---|
| Vocation | Care setting | ||||
| Hospital | Primary care | Residency | Total | χ2 (4) = 14.4 | |
| Preventive paediatrics | 3 (6.3%) | 45 (22%) | 7 (17.5%) | 55 (18.8%) | |
| Clinical paediatrics | 39 (81.3%) | 111 (54.1%) | 28 (70%) | 178(60.8%) | |
| Social paediatrics | 6 (12.5%) | 49 (23.9%) | 5 (12.5%) | 60 (20.5%) | |
| Total | 48 (100%) | 205 (100%) | 40 (100%) | 293 (100%) | |
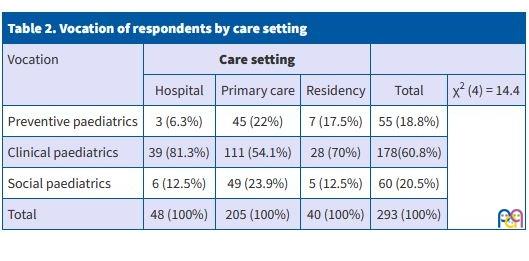
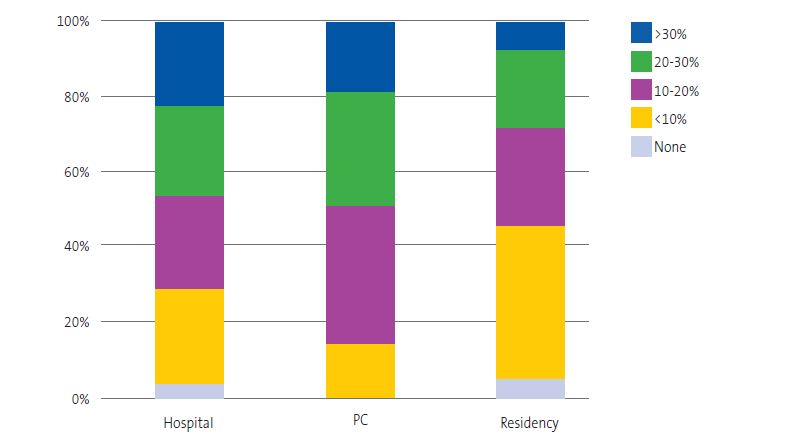
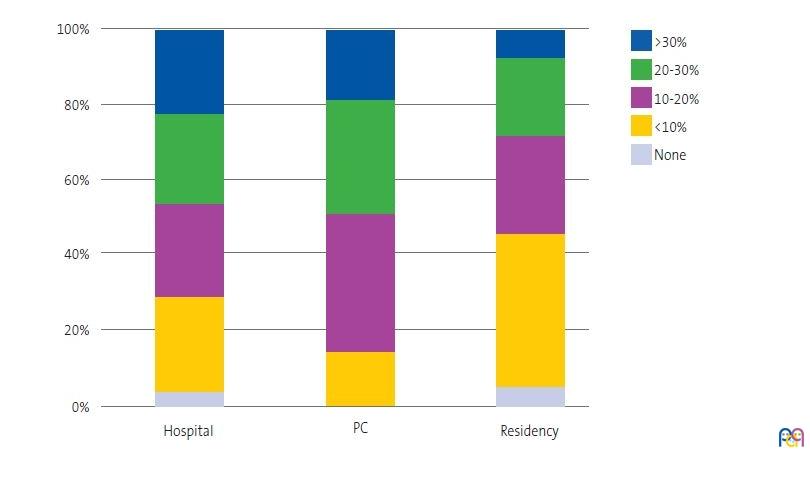
Figure 3 presents the time spent by participants on health promotion activities, evincing differences between care settings (χ2(8) = 26.1; p <0.001). Most paediatricians reported engaging in health promotion activities, but those who worked at the primary care level spent the most time on them, especially compared to residents.
| Figure 3. Time devoted to health promotion activities |
|---|
 |
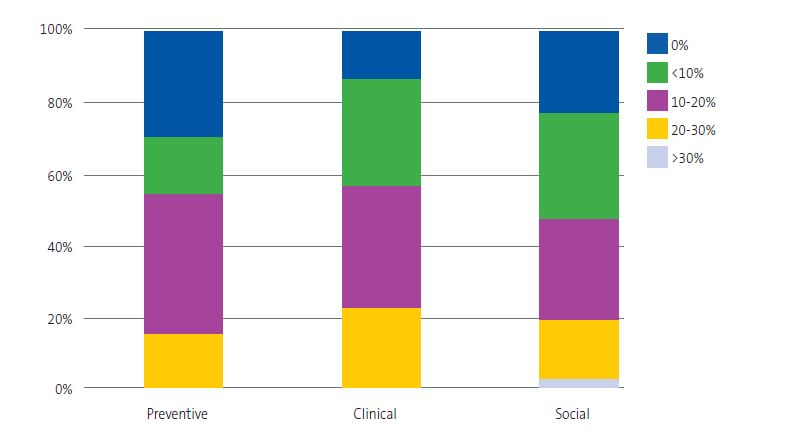
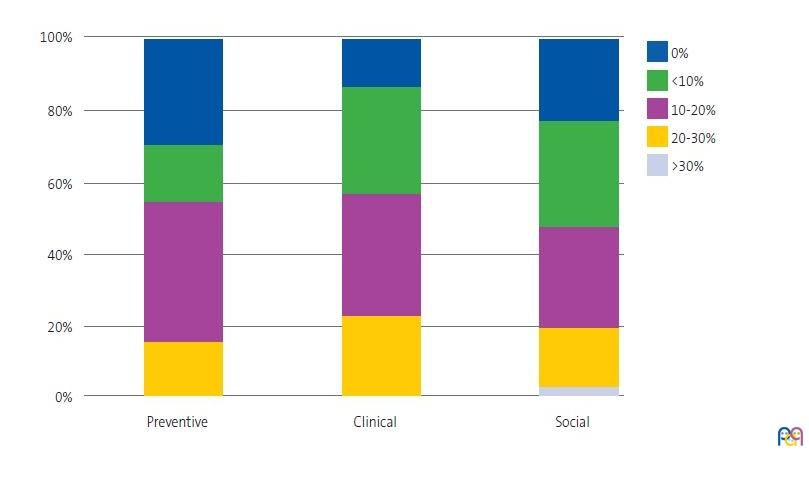
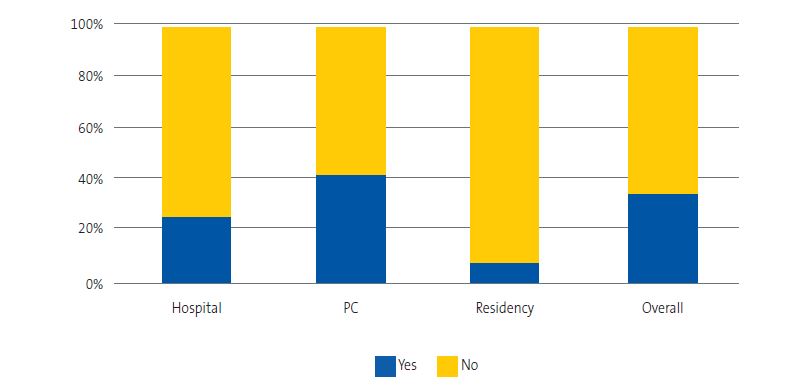
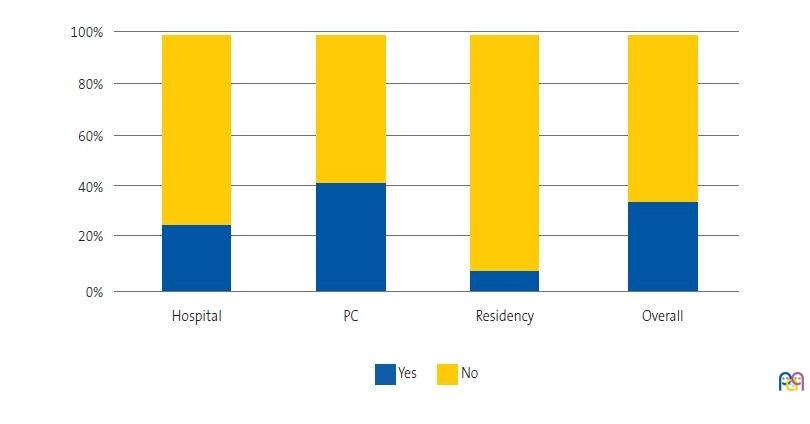
The reported vocation was also associated with the frequency of engagement in health promotion activities, as can be seen in Figure 4, and participants with a vocation for preventive care were the group that devoted the most time to it; however, this difference was not statistically significant (χ2(8) = 13.8; p <0.09). When it came to reading promotion activities, which are a particular form of health promotion, we also found significant differences based on the care setting (χ2(2) = 19.0; p <0.001), with a greater proportion of primary care paediatricians reporting this type of activity (41.7% compared to 25% of hospitalists and 7.7% of residents) (Figure 5).
| Figure 4. Performance of health promotion activities by vocation |
|---|
 |
| Figure 5. Performance of health promotion activities by care setting and in the overall sample |
|---|
 |
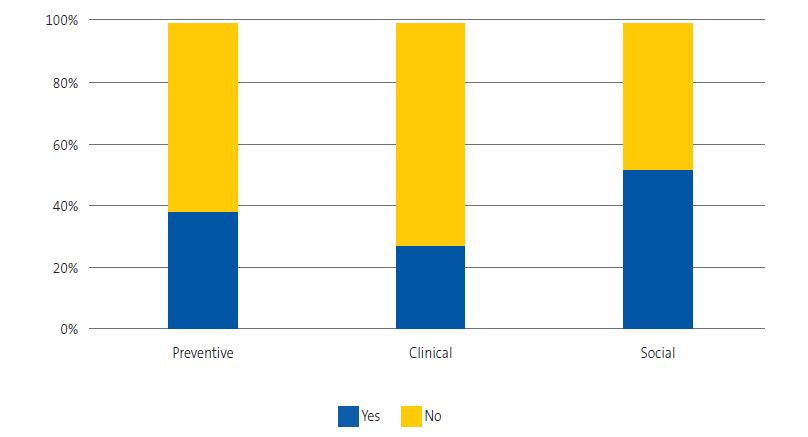
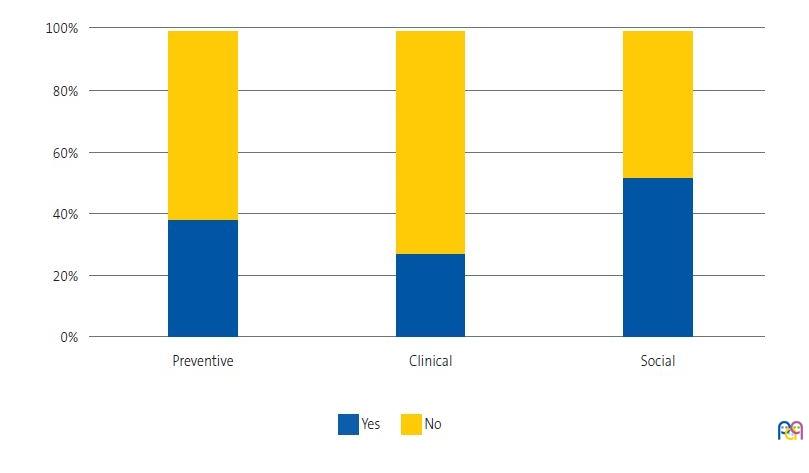
To assess whether there was any form of association between the reported vocation and the implementation of reading promotion activities, we carried out a new analysis that showed that the proportion who carried these activities was greatest in the subset that reported a social paediatrics vocation (52.7% compared to 38.2% of those who reported a preventive vocation and 27.3% among those who reported a clinical vocation), (χ2(2) = 13.11, p <0.001) (Figure 6).
| Figure 6. Performance of reading promotion by vocation |
|---|
 |
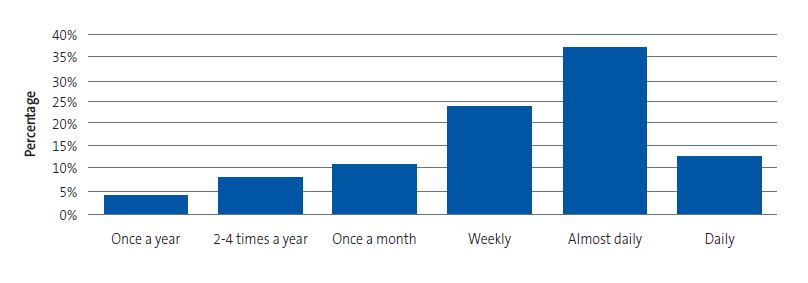
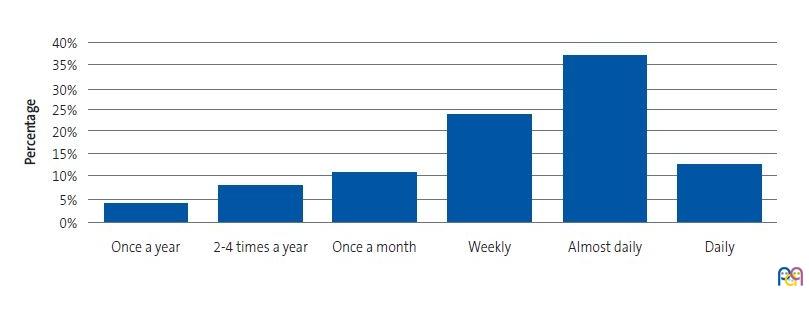
In the subset of paediatricians who reported performing reading promotion activities, there were substantial differences in how frequently they carried them out (Figure 7), with half of them reporting a daily or almost daily frequency.
| Figure 7. Frequency of performance of reading promotion activities (percentage of professionals) |
|---|
 |
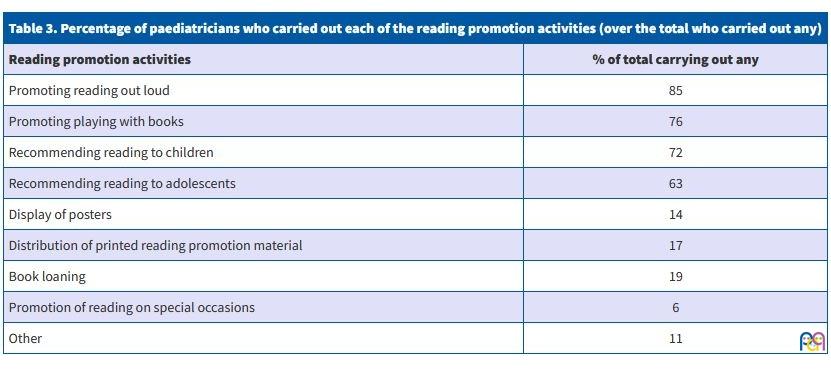
The type of activities for reading promotion were also very varied and are detailed in Table 3. Most paediatricians who engaged in reading promotion carried out more than one type of intervention. The most frequent one was recommending reading aloud (85%). This was followed by recommending devoting time to reading to children (76%) and to adolescents (63%). Seventy-two percent promoted the use of books as a tool for parents to play and interact with their children, helping them learn to turn pages, identify images in books, etc, as appropriate for the age of the child. Fourteen percent had posters promoting reading in their office or waiting room, and 17% provided printed handouts (leaflets, trifolds…). Nineteen percent reported loaning books and 6% supporting reading promotion activities on special occasions (yearly book fair, National Reading Month …).
| Table 3. Percentage of paediatricians who carried out each of the reading promotion activities (over the total who carried out any) | |
|---|---|
| Reading promotion activities | % of total carrying out any |
| Promoting reading out loud | 85 |
| Promoting playing with books | 76 |
| Recommending reading to children | 72 |
| Recommending reading to adolescents | 63 |
| Display of posters | 14 |
| Distribution of printed reading promotion material | 17 |
| Book loaning | 19 |
| Promotion of reading on special occasions | 6 |
| Other | 11 |
On the other hand, participants who reported not engaging in any reading promotion activities (65.6% of the total) were asked to explain the reason. Their responses were also varied, and the most frequent one was lack of time (66 paediatricians; 43.2%), followed by lack of space (27 paediatricians; 16.4%) and lack of support (13 paediatricians; 8.5%).
DISCUSSION
A substantial number of paediatricians participated in the survey, with strong representation not only of the two key care settings for paediatric practice (hospital and primary care) but also of residents training in the speciality. Their ages covered the full age range of the collective of paediatricians, with participants from different generations and levels of experience ranging from the start of the residency to the time of retirement. As expected, there was a higher proportion of female than male participants, with a greater proportion working in primary care, a group in which the reported caseloads were within the usual range. In other words, although the sample was not selected at random, its final composition was large and diverse enough to assume that their views offered an adequate representation of the perspective of the profession as a whole.
As regards the vocation for paediatric practice, our study found that a vocation for clinical work predominated among the surveyed paediatricians, and was reported by a greater proportion of residents and hospital-based paediatricians compared to primary care paediatricians. On the other hand, a vocation for preventive work was the least reported overall, although it was expressed with greater frequency in the group of primary care paediatricians compared to the other groups. Lastly, a vocation for social paediatrics was also reported by a minority of respondents, although it was also most frequently reported by primary care paediatricians.
Regarding health promotion activities, most participants reported devoting more than 10% of their time to them, in adherence to the recommendations of the World Health Organization, which consistently highlights the importance of this type of activity. The 9th Global conference on health promotion11 reaffirmed health as a universal right, an essential resource for everyday living and a shared social goal, noting that health care systems must pursue health prevention and promotion.12 The responsibility for this task is shared by primary care and hospital based paediatricians, although a larger percentage of the former devote more time to this type of activities. There is a growing awareness of the need to approach the care of children from a holistic perspective, putting families at the centre, eliciting and responds to family needs and supporting families throughout the development of the child.13
Our survey also revealed that paediatric residents devoted the least amount of time to health promotion activities. This finding was consistent with other studies that found that only 1 in 4 residents in paediatrics expresses a desire to work at the primary care level after completing their training.14 At present, we suffer from a deficit of primary care paediatricians that is expected to get worse. Given this situation, the health care authorities should invest resources on the medical residency training programme and making primary care paediatrician vacancies more appealing to beginning paediatricians.15
Focusing on the primary outcome of our study, reading promotion activities were carried out by approximately one third of the surveyed paediatricians, although the proportion was higher in those who worked at the primary care level. At the international level, there are many associations that encourage the performance of these activities. The American Academy of Pediatrics (AAP) considers literacy promotion an essential element of primary care,16 and the Asociación Española de Pediatras de Atención Primaria (AEPap, Spanish Association of Primary Care Paediatricians), along with other societies in Spain, has also underscored the importance of promoting reading, arguing that reading aloud should be a widespread habit in households, for, while it does not in itself make up for social or cultural disadvantages, it makes it easier for any child to learn how to read and write and can promote a stronger affectional bond between adults and children.17
In the characterization of the practices of reading promotion within paediatric care in Spain, our study found a wide range, among which the promotion of reading aloud was most frequent, followed by the recommendation of reading to children and of play involving books. It is worth noting that adolescents were encouraged to somewhat less frequently than younger children. Some of the least common practices were the loaning of books in the clinic, the display of posters in the office or waiting room or the provision of printed information at the clinic to promote reading, as was the recommendation to read provided by the paediatrician on special occasions, such as the World Book Day or the National Reading Month. The findings of our study regarding specific interventions were consistent with widespread recommendations regarding the range of activities that can be performed in paediatric care practice. For instance, the AAP proposes the following: (1) advising parents that reading aloud with young children can enhance parent-child relationships and prepare young minds for learning; (2) counselling parents about developmentally appropriate shared-reading activities that are enjoyable for all involved and offer exposure to language-rich books, pictures and the written word; (3) providing developmentally appropriate books, which could be handed out at routine child health visits, especially to children of lower socioeconomic status/from low-income families; (4) partnering with other child advocates to influence national messaging and policies that support and promote these key early shared-reading experiences.18 With the exception of the fourth one, the rest are implemented to a varying degree by a large number of paediatricians in Spain, as found in our study.
Limitations: the extrapolation of the results of our study may be limited by our having accessed the sample through mailing lists, which does not guarantee that the sample was representative of the population under study. However, the final distribution of the sample of participants, which included a large number of professionals employed in different care settings and with a wide range of ages and years of experience, was remarkably similar to that of the population of paediatricians in Spain.
CONCLUSION
Based on the collected data, we can conclude that reading promotion activities are carried out predominantly by primary care paediatricians in the context of other health promotion activities, which in turn were chiefly associated with a vocation for social paediatrics.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
AUTHORSHIP
Author contributions: study design, development of instrument, analysis of results (AGG, IGG, JLM), participant recruitment, data collection (AGG, IGG), writing of first draft (AGG), manuscript revision and writing of the definitive version (all).
ABBREVIATIONS
AAP: American Academy of Pediatrics · AEPap: Asociación Española de Pediatría de Atención Primaria · EA: educational attainment · MIR: medical intern-resident · SD: standard deviation · SES: socioeconomic status.
REFERENCES
- Orden SCO/3148/2006, de 20 de septiembre, por la que se aprueba y publica el programa formativo de la especialidad de Pediatría y sus Áreas Específicas. In: BOE no. 246. Year 2006 [online] [accessed 10/10/2023]. Available at www.boe.es/buscar/doc.php?id=BOE-A-2006-17999
- Asociación Española de Pediatría. Libro blanco de las ACES Pediátricas. Año 2021 [online] [accessed 10/10/2023]. Available at https://luaediciones.com/aep/aces2021/
- Portal Estadístico Ministerio de Sanidad, Área de Inteligencia y Gestión, Sistema de Información de Atención Especializada, Área de profesionales y Especialidades. In: Portal Estadístico, Área de Inteligencia de Gestión. Año 2021 [online] [accessed 10/10/2023]. Available at https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/C/siae/siae/hospitales/personal-y-formacion/areas-profesionales-y-especialidades
- Portal Estadístico Ministerio de Sanidad, Área de Inteligencia y Gestión, Sistema de Información de Atención Primaria, Área de profesionales y Modalidades Asistenciales. In: Portal Estadístico, Área de Inteligencia de Gestión. Año 2021 [online] [accessed 10/10/2023]. Available at https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/C/sistema-de-informacion-de-atencion-primaria-siap/profesionales/modalidades-asistenciales
- Hidalgo Cantabrana C, González García M, González Rodríguez S, Hidalgo A, Hidalgo Cantabrana C, González García M, et al. Sobre la vocación médica a través de opiniones tomadas de la literatura médica y de ficción. Rev Med Cine. 2020;16(4):319-30. https://dx.doi.org/10.14201/rmc2020164319330
- Asociación Española de Pediatría de Atención Primaria. Competencias específicas pediatría de atención primaria. In: AEPap [online] [accessed 10/10/2023]. Available at www.aepap.org/sites/default/files/documento/archivos-adjuntos/competencias_especificas_pediatria_de_ap_aepap.pdf
- Council on Early Childhood, Council on School Health. The Pediatrician’s Role in Optimizing School Readiness. 2016;138:e20162293. https://doi.org/10.1542/peds.2016-2293
- Duursma E, Augustyn M, Zuckerman B. Reading aloud to children: the evidence. Arch Dis Child. 2008;93:554-7. https://doi.org/10.1136/adc.2006.106336
- Garach Gómez A, Alperi García S, Gutiérrez García I. La lectura como herramienta de promoción de la salud. Form Act Pediatr Aten Prim. 2021;14:133-6.
- Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol Off J Div Health Psychol Am Psychol Assoc. 2000;19:586-92. https://doi.org/1037//0278-6133.19.6.586
- 9.a Conferencia Mundial de Promoción de la Salud. Acuerdo de dirigentes mundiales para promover la salud en pro de los Objetivos de Desarrollo Sostenible. In: Organización Mundial de la Salud. Año 2016 [online] [accessed 10/10/2023]. Available at www.who.int/es/news/item/21-11-2016-9th-global-conference-on-health-promotion-global-leaders-agree-to-promote-health-in-order-to-achieve-sustainable-development-goals
- Camarelles Guillem F. Los retos de la prevención y promoción de la salud, y los del PAPPS. Aten Primaria. 2018;50(Suppl 1):1-2. https://doi.org/10.1016/S0212-6567(18)30358-5
- Inkelas M, Oberklaid F. Improving preventive and health promotion care for children. Isr J Health Policy Res. 2018;7:62. https://doi.org/10.1186/s13584-018-0259-3
- Álvarez Casaño M, Gorrotxategi Gorrotxategi PJ, Castillo Campos l, Cámara Otegui A, Martín Moya R, Fuentes Redondo T, et al. Salidas laborales de los residentes de Pediatría. Datos del periodo 2014-2017. Rev Pediatr Aten Primaria. 2019;21:247-53.
- Gorrotxategi Gorrotxategi P, García Vera C, Graffigna Lojendio A, Sánchez Pina C, Palomino Urda N, Rodríguez Fernández-Oliva CR, et al. Situación de la Pediatría de Atención Primaria en España en 2018. Rev Pediatr Aten Primaria. 2018;20:e89-e104.
- Zuckerman B, Needlman R. 30 Years of Reach Out and Read: Need for a Developmental Perspective. 2020;145:e20191958. https://doi.org/10.1542/peds.2019-1958
- Manifiesto de la voz a las letras. In: Asociación Entrelibros [online] [accessed 10/10/2023]. Available at www.asociacionentrelibros.es/wp-content/uploads/2016/12/de-la-voz-a-las-letras.pdf
- Council on Early Childhood, High PC, Klass P. Literacy promotion: an essential component of primary care pediatric practice. 2014;134:404-9. https://doi.org/10.1542/peds.2014-1384