
Vol. 24 - Num. 93
Original Papers
Prevalence of breastfeeding in the heatlh district of Purullena, Granada. Moving toward IHAN accreditation
Elena Conde Puertasa, Maribel Muñoz Blánquezb, Ángel Manuel de la Fuente Vílchezc
aPediatra. CS Purullena. Granada. España.
bMatrona. CS Purullena. Granada. España.
cEnfermero. CS Purullena. Granada. España.
Correspondence: E Conde. E-mail: elena.conde.puertas.sspa@juntadeandalucia.es
Reference of this article: Conde Puertas E, Muñoz Blánquez M, de la Fuente Vílchez AM. Prevalence of breastfeeding in the heatlh district of Purullena, Granada. Moving toward IHAN accreditation. Rev Pediatr Aten Primaria. 2022;24:13-21.
Published in Internet: 11-01-2022 - Visits: 12815
Abstract
Introduction: we conducted an observational and descriptive study with the aim of determining the prevalence, duration and characteristics of breastfeeding in our health district to establish a baseline for the implementation of improvements in perinatal care practices in adherence with the IHAN initiative, to monitor long-term results and to compare outcomes with other areas of Spain.
Material and methods: we carried out a survey of nutrition in a sample of 82 children aged 0 to 2 years to calculate the indicators of exclusive breastfeeding up to 6 months; continued breastfeeding at ages 1 and 2 years and the prevalence of complementary feeding at age 6-8 months. We also collected information on the nutrition received the previous day in 25 neonates that attended the primary care centre to calculate the indicator of exclusive breastfeeding in infants aged 0 to 15 days.
Results: we found a prevalence of exclusive breastfeeding of 68% in infants aged 0 to 15 days and 37% in infants aged 6 months, and a prevalence of continued BF of 24% at age 1 year and 21% at age 2 years. The proportion of infants that consumed other solid, semisolid or soft foods at ages 6 to 8 months was 100%.
Conclusions: the findings of our study were similar to those of other studies in Spain, but were still far from the targets recommended by the World Health Organization.
Keywords
● Breastfeeding ● Exclusive breastfeeding ● Primary health careINTRODUCTION
Breastfeeding (BF) is the optimal nutrition for neonates and infants not only from a physical standpoint, but also from a psychological standpoint, as it promotes adequate bonding and secure attachment. It also provides numerous health benefits not only to the child but also to the mother, as well as benefits to society and the environment.
There is evidence that BF is associated with a reduction in the risk of different diseases in children: acute otitis media, gastroenteritis, severe lower respiratory tract infections, atopic dermatitis, asthma, obesity, type 1 and 2 diabetes, childhood leukaemia, sudden infant death syndrome and necrotising enterocolitis in infants.1,2 There is also evidence of a beneficial impact on maternal health, with a decreased risk of type 2 diabetes, breast and ovarian cancer and post-partum depression.1
Consequently, all domestic and international scientific societies recommend initiation of BF within 1 hour of birth and maintenance of exclusive breastfeeding (EBF) the first 6 months of life followed by BF combined with complementary foods through age 2 years.3-5
Knowing the prevalence, duration and characteristics of BF in each country or region is essential to determine which BF support and promotion measures are required to achieve these objectives, and therefore it is recommended that data be collected at regular intervals.6
However, Spain does not have an adequate official system to survey and monitor BF practices. Most of the data currently available are from the National Health Survey of Spain (NHSS), which since 1995 has been collecting responses to items regarding BF, and sporadic studies conducted at the regional or local level with heterogeneous methodologies, which hinders comparison of results and long-term followup of BF. To allow comparisons between different countries and regions, it would be ideal for research to apply the BF indicators and methodology established by the World Health Organization (WHO).7
The most recent data from the NHSS (2017) show that BF was the most prevalent feeding modality for babies through 6 weeks post birth (73.9%), with the prevalence declining to 63.9% by 3 months and to 39% by 6 months post birth, which reflects a substantial improvement in recent decades and in the years that the survey has been conducted.8
Despite this improvement, BF outcomes continue to be suboptimal, which is an important public health problem. Thus, we need to continue striving to increase these rates, which would improve population health in the long term.
This is the reason that WHO and the UNICEF launched the Baby Friendly Hospital Initiative (BFHI) in 1992, which since 2006 has underscored that the ongoing support of mothers throughout the entire breastfeeding period is essential, thereby extending the strategy to all other maternal and child health care settings. In 2009, the initiative in Spain came to be known as Iniciativa de Humanización de la Atención al Nacimiento y la lactancia (IHAN, or Initiative for the Humanization of Childbirth and Lactation Care), with the launch of the IHAN Health Care Centres project, following the lead of other European countries.9
At present, since the length of stay in maternity wards after birth is very short for most women, BF support is mainly provided at the primary care level, and therefore it is essential that primary care providers and facilities implement evidence-based BF support practices and interventions.
Breastfeeding support interventions at the primary care level have a positive impact on the prevalence and duration of BF and the maintenance of EBF. However, there is significant variability in the interventions recommended by the different reviews and guidelines that provide the foundation for BF support practices. The Group for Child and Adolescent Health Prevention (PrevInfad) of the Asociación Española de Pediatría (Spanish Association of Paediatrics) recommends implementation of the American Academy of Paediatric guidelines or the seven-point plan of the BFHI/IHAN, which have the most overlap.10
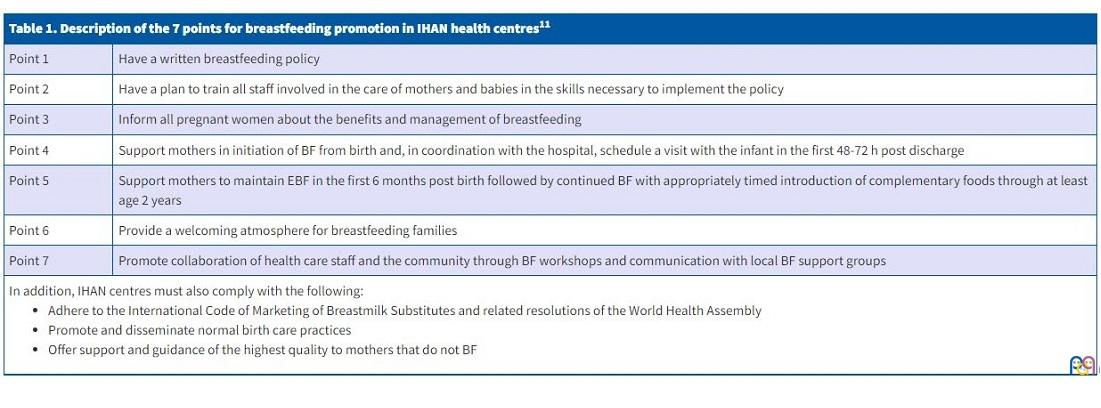
The goal of the IHAN health care centre initiative is for health care facilities to implement best practices for excellence in clinical care from childbirth through the end of breastfeeding and to promote best practices in child nutrition. Accreditation as an IHAN centre requires adherence to the 7-point plan of the BFHI/IHAN (Table 1) and the International Code of Marketing of Breastmilk Substitutes, and proven improvement in BF outcomes after implementation of the strategy.11 To date, very few centres have completed accreditation in Spain, but many have started the process and advancing through the required stages, including our hospital, reflecting the growing desire and commitment improve BF practices in our country.
| Table 1. Description of the 7 points for breastfeeding promotion in IHAN health centres11 | |
|---|---|
| Point 1 | Have a written breastfeeding policy |
| Point 2 | Have a plan to train all staff involved in the care of mothers and babies in the skills necessary to implement the policy |
| Point 3 | Inform all pregnant women about the benefits and management of breastfeeding |
| Point 4 | Support mothers in initiation of BF from birth and, in coordination with the hospital, schedule a visit with the infant in the first 48-72 h post discharge |
| Point 5 | Support mothers to maintain EBF in the first 6 months post birth followed by continued BF with appropriately timed introduction of complementary foods through at least age 2 years |
| Point 6 | Provide a welcoming atmosphere for breastfeeding families |
| Point 7 | Promote collaboration of health care staff and the community through BF workshops and communication with local BF support groups |
In addition, IHAN centres must also comply with the following:
|
|
MATERIAL AND METHODS
We conducted a cross-sectional observational and descriptive study to determine the prevalence and characteristics of BF in the health district of Purullena, in the North-East Granada Health Area, a mostly rural area encompassing multiple municipalities with an overall population of 11 930 inhabitants. We obtained data based on the list of children under 2 years born between February 1, 2017 and January 31, 2019, which corresponded to 228 children (1.19% of the total population) in the caseloads of the 2 paediatricians in our health district. We applied a randomised stratified sampling method, selecting children by means of their public health system cards and including 1 out of every 2 cards in consecutive order after the random selection of the first card. Both the sample size and the selection method adhered to the established methodology for the assessment of IHAN indicators, according to which, for centres managing fewer than 300 children under 2 years, as was the case, the sample should include a minimum of 75 infants adding an additional 10% to the calculated size to make up for possible losses.4
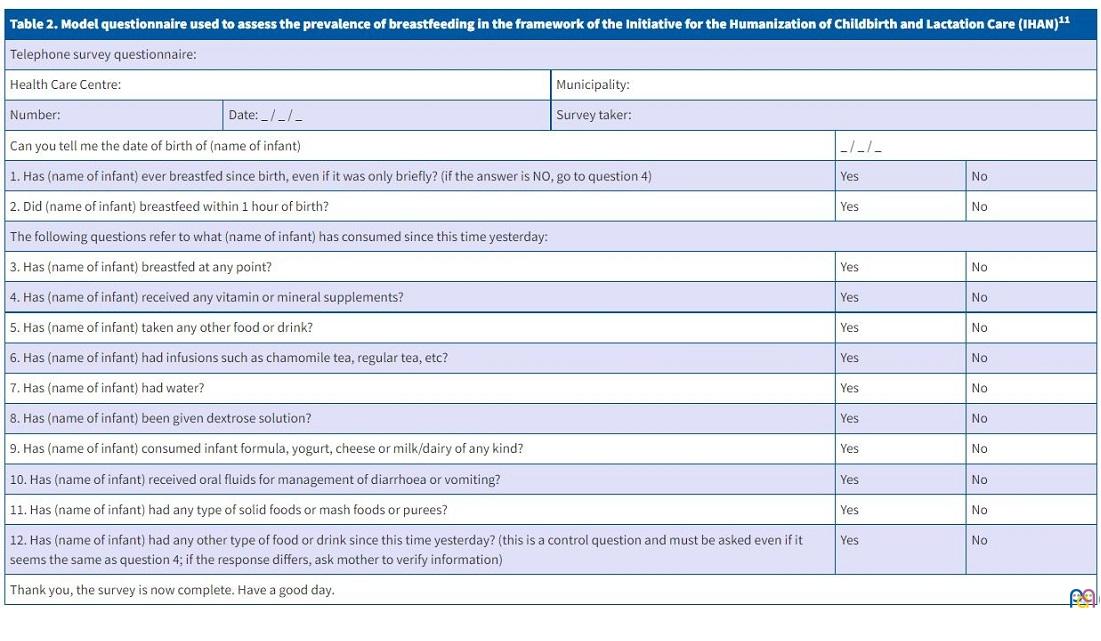
We interviewed the mothers or main caregivers of selected infants or toddlers aged 0 to 2 years on the phone using the IHAN model questionnaire (Table 2) to ask about their nutrition and obtain data on different BF indicators. The interviews were conducted by administrative and support staff that were not directly involved in care delivery to minimise bias.
| Table 2. Model questionnaire used to assess the prevalence of breastfeeding in the framework of the Initiative for the Humanization of Childbirth and Lactation Care (IHAN)11 | ||||||
|---|---|---|---|---|---|---|
| Telephone survey questionnaire: | ||||||
| Health Care Centre: | Municipality: | |||||
| Number: | Date: _ / _ / _ | Survey taker: | ||||
| Can you tell me the date of birth of (name of infant) | _ / _ / _ | |||||
| 1. Has (name of infant) ever breastfed since birth, even if it was only briefly? (if the answer is NO, go to question 4) | Yes | No | ||||
| 2. Did (name of infant) breastfeed within 1 hour of birth? | Yes | No | ||||
| The following questions refer to what (name of infant) has consumed since this time yesterday: | ||||||
| 3. Has (name of infant) breastfed at any point? | Yes | No | ||||
| 4. Has (name of infant) received any vitamin or mineral supplements? | Yes | No | ||||
| 5. Has (name of infant) taken any other food or drink? | Yes | No | ||||
| 6. Has (name of infant) had infusions such as chamomile tea, regular tea, etc? | Yes | No | ||||
| 7. Has (name of infant) had water? | Yes | No | ||||
| 8. Has (name of infant) been given dextrose solution? | Yes | No | ||||
| 9. Has (name of infant) consumed infant formula, yogurt, cheese or milk/dairy of any kind? | Yes | No | ||||
| 10. Has (name of infant) received oral fluids for management of diarrhoea or vomiting? | Yes | No | ||||
| 11. Has (name of infant) had any type of solid foods or mash foods or purees? | Yes | No | ||||
| 12. Has (name of infant) had any other type of food or drink since this time yesterday? (this is a control question and must be asked even if it seems the same as question 4; if the response differs, ask mother to verify information) | Yes | No | ||||
| Thank you, the survey is now complete. Have a good day. | ||||||
We also collected information on the intake of the infant or young child in the 24 hours preceding the interview for 25 neonates selected consecutively as patients attended the initial postpartum visit scheduled as part of the prenatal, labour and delivery and postpartum care protocol or the infant came for the first routine healthy child programme visit between December 2018 and March 2019, to obtain data on the EBF indicator in neonates aged 0 to 15 days. We excluded neonates that were assessed and surveyed for the first time after 15 days post birth.
Consent to participation in the study was obtained verbally from the mother or caregiver during the interview.
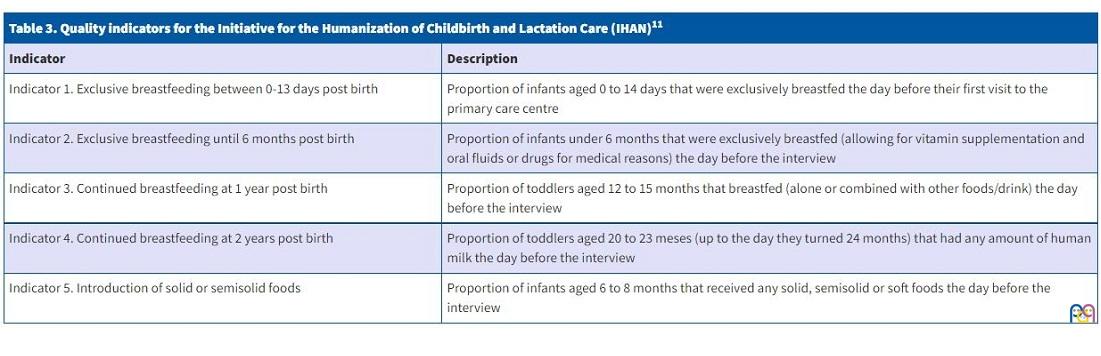
We applied the methodology recommended by the IHAN to calculate the proposed indicators, which also adhered to the indicator recommendations of the WHO, detailed in Table 3.
| Table 3. Quality indicators for the Initiative for the Humanization of Childbirth and Lactation Care (IHAN)11 | |
|---|---|
| Indicator | Description |
| Indicator 1. Exclusive breastfeeding between 0-13 days post birth | Proportion of infants aged 0 to 14 days that were exclusively breastfed the day before their first visit to the primary care centre |
| Indicator 2. Exclusive breastfeeding until 6 months post birth | Proportion of infants under 6 months that were exclusively breastfed (allowing for vitamin supplementation and oral fluids or drugs for medical reasons) the day before the interview |
| Indicator 3. Continued breastfeeding at 1 year post birth | Proportion of toddlers aged 12 to 15 months that breastfed (alone or combined with other foods/drink) the day before the interview |
| Indicator 4. Continued breastfeeding at 2 years post birth | Proportion of toddlers aged 20 to 23 meses (up to the day they turned 24 months) that had any amount of human milk the day before the interview |
| Indicator 5. Introduction of solid or semisolid foods | Proportion of infants aged 6 to 8 months that received any solid, semisolid or soft foods the day before the interview |
In addition to the indicators required by the IHAN methodology applied to the assessment of BF rates, we collected data on other BF indicators of interest to our study using the same questionnaire and in adherence with the WHO recommendations, such as the proportion of children ever breastfed, early initiation of BF within 1 hour of birth and the prevalence of the introduction of complementary foods before 6 months. We processed the data with the software SPSS 20.0.
RESULTS
The interviews were conducted between March and June of 2019.
We did not obtain responses for 29 of the selected children (32% non-response rate), so the final sample included 107 infants or toddlers under 2 years (25 neonates aged 0-15 days and 82 infants/toddlers aged less than 2 years).
Fifty-nine percent of respondents initiated BF within 1 hour of birth. In the group aged 0 to 15 days, 67% of neonates received EBF, and this prevalence that decreased to 37% in the group aged 0 to 6 months. The prevalence of continued BF was 24% at age 1 year and 21% at age 2 years.
In our area, it was exceptional for infants not to have started to receive foods other than milk from age 6 months, with a prevalence of complementary feeding of 100% in infants aged 6 to 8 months.
In the survey, we also collected information on variables that were not included in the IHAN model or indicators, such as the cumulative BF rate, and we found that 95.1% of children under 2 years had been breastfed at some point or some age, while 4.9% had never received maternal milk; we also calculated the percentage of infants that had started complementary feeding before 6 months post birth, which was 50%.
DISCUSSION
The proportion of infants that start breastfeeding in the first hour post birth is one of the main BF indicators, and initiation of BF in this time frame of the strongest predictors of BF efficacy and duration.12 It is also a key factor in the shaping of the intestinal microbiota, which in turn is associated with future disease and immune regulation.13 In our survey, 57% of mothers initiated BF in the first hour post birth. A study conducted in Andalusia in 200514 found a prevalence of BF in the first hour of life of 61.8%, and there is evidence of improvement in recent years, with percentages as high as 70% in Vigo15 and 88.4% in Jaen,16 for example, although the objectives set by the WHO have yet to be met, especially in our area.
In our survey, the prevalence of EBF in neonates aged 0-15 days was 68%. This prevalence was consistent with the findings of a recent study conducted in a cohort of 2066 children in different autonomous communities in Spain, in which the prevalence of EBF in neonates under 15 days was 67.2%,17 and was higher compared to the prevalence reported in other studies, for instance, in Vigo in 2017 (50%) or Zaragoza in 2015 (53%).15,18
When it came to indicator 2, EBF up to age 6 months, we found a proportion of 37% of EBF compared to 63% of infants that were not exclusively breastfed. According to data from the NHSS, in 2017 the mean duration of BF (EBF and mixed) was 6 months, and the prevalence of EBF at 6 months had increased from 28.5% in 2011 to 39% in 2017,8 findings that we cannot compare to ours on account of methodological differences. In the study published in 2005 conducted in 1087 children in Andalusia, the prevalence of EBF declined from 26.5% to 6.4% between ages 4 and 6 months, and only 13.5% of infants under 6 months were exclusively breastfed.14 Studies conducted in recent years in different regions in Spain reflected substantial variation in the prevalence of EBF at 6 months, ranging from 15.8% in Zaragoza in 201518 or 15.4% in the INMA cohort study of Gipuzkoa 19 to, for example, 25.4% in Madrid in 2017.20 The 2017 study conducted in Vigo,15 with used the same methods applied in our study, found better outcomes, with a prevalence of EBF in infants aged 0 to 6 months of 50%. Our health area has yet to achieve the 2025 target of 50% of EBF in infants up to 6 months of age established by the WHO for year 2025.
The benefits of BF are dose-dependent, and this indicator is essential as a predictor of BF duration. There is also evidence that EBF until 6 months compared to 3 to 4 months reduces morbidity secondary to gastrointestinal infections and prolongs postpartum amenorrhoea in the mother, and is not associated with an increased risk of nutrient deficiencies or abnormal growth or developmental outcomes.21
Early return to work (by 4 months post birth) and lack of BF support in the workplace continue to be probable barriers to the maintenance of EBF through 6 months. For this reason, a large part of the efforts made for BF promotion should be devoted to counselling and supporting mothers as they return to work.
When it comes to indicators 3 and 4 of continued BF at 1 and 2 years of age, our findings did not differ much from those of the 2017 study in Vigo (34.6 and 26.6%)15 or the CALINA study in Aragon, which find a prevalence of continued BF at 1 year of 27.8%,22 significantly better outcomes compared to the prevalence of continued BF at 2 years reported in cities like Zaragoza (14.2%)18 or Madrid (7.7%).20 Our health district is mostly a rural area, which was also the case of part of the sample included in the study conducted in Vigo, whose authors found that the proportions of continued BF at 2 years were higher in rural areas compared to urban areas (46 vs. 15%).15 This could explain some of the differences between studies conducted in large cities versus more rural areas, like our own, which could be attributed, among other reasons, by a lower percentage of women employed out of the home in rural areas, which could facilitate prolonged BF. In addition, there is not a significant decline in the prevalence of continued BF between 1 and 2 years post birth, probably because women that BF for a long time are more motivated, and having already overcome barriers in the past they are able to continue to maintain BF for a longer period.
In our sample, most infants (95.1%) had breastfed at some point. Although this percentage is high, we found a steep decline in the first days and months post birth. The recent study conducted in a cohort of 2066 children in different regions of Spain found a similar cumulative overall prevalence of BF (89.3%).17
Some of the main reasons for weaning or discontinuation of EBF in the study conducted in Castilla y Leon was hypogalactia, documented in up to 30% of mothers, and low infant weight gain in 20%, which may be due to early or inadequate initiation of complementary feeding. Another concerning finding is that in 20% of cases, mothers reported advice by a health professional as the reason for discontinuing BF.23 In our area, it is exceptional for infants aged 6 to 8 months to not be consuming complementary foods (100% of infants in our health district had initiated complementary feeding by that age). However, we ought to highlight the high proportion of infants with early introduction of complementary foods before age 6 months of 50%. In breastfed infants, it is recommended that EBF be maintained through age 6 months, to be followed by continued BF with gradual introduction of other foods. When it comes to formula-fed infants, there is no consensus regarding the optimal timing for initiation of complementary feeding.24 The culture surrounding formula feeding, combined with the lobbying of the food industry, may play a role in the early and inappropriate initiation of complementary feeding, resulting in weaning in many cases.
Some studies have found an association between the total duration of BF and maternal age (with greater durations in mothers aged more than 35 years) as well as attendance to childbirth and infant care classes,15 which leads us to believe that BF support measures like BF workshops and childbirth classes that are included in the IHAN guidelines could improve BF rates in our area.
Our study allowed us to assess the current situation in our area and to compare it to other regions and mean values in Spain, essentially establishing a baseline with which to evaluate the impact of measures for improvement of perinatal care and BF implemented as part of the process of accreditation as an IHAN centre that we are currently undergoing. Our centre has just received a favourable rating in phase 2D of the accreditation process after implementation of several improvement measures in staff training, education of women and mothers, BF and infant care classes and development of a BF policy. Studies like this one will allow us to compare these indicators to other facilities undergoing IHAN accreditation and monitor the evolution of every indicator over time.
CONCLUSION
For certain indicators, the results in our area are similar to those reported in other parts of Spain, although in some instances comparison was hindered by methodological differences, chiefly evincing a high cumulative prevalence of BF at any time and a relatively high prevalence of EBF in the first 15 days post birth that declines sharply in the first months of life, with acceptable proportions of continued BF at 1 and 2 years post birth.
Despite the awareness of the importance of BF and current recommendations, we are still far from reaching the targets set by the WHO. Measures need to be implemented to improve every indicator, but the most important objectives are to improve maintenance of EBF through age 6 months and continued BF in the long term, in which primary care professionals and the IHAN accreditation process play a key role.
The drive to improve perinatal care and BF practices stimulated by the IHAN project is spreading to an ever-growing number of primary care centres, and hopefully will be generalised in the future.
Spain needs a better system for BF monitoring and followup based on standardised and comparable indicators, and the IHAN study model could allow assessment of differences between geographical areas and monitoring improvement in the future.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
ABBREVIATIONS
BF: breastfeeding · BFHI: Baby-Friendly Hospital Initiative · EBF: exclusive breastfeeding · IHAN: I Initiative for the Humanization of Childbirth and Lactation Care · NHSS: National Health Survey of Spain · WHO: World Health Organization.
REFERENCES
- Aizpurua Galdeano P. Efectos de la lactancia materna sobre la salud de las madres y de los lactantes en países desarrollados. Evid Pediatr. 2008;4:45.
- Horta BL, Bahl R, Martines JC, Victoria CG. Evidence on the long-term effects of breastfeeding: a systematic review and meta-analysis. In: World Health Organization [online] [accessed 05/01/2021]. Available at https://apps.who.int/iris/bitstream/handle/10665/43623/9789241595230_eng.pdf?sequence=1
- Recomendaciones sobre lactancia materna del Comité de Lactancia materna de la Asociación Española de Pediatría. In: Asociación Española de Pediatría. [online] [accessed 05/01/2021]. Available at www.aeped.es/sites/default/files/201202-recomendaciones-lactancia-materna.pdf
- Infant and Young Child Nutrition. Global Strategy on Infant and Young Child Feeding. Report by the Secretariat. Fifty-fifth World Health Assembly, 16 April, 2003. In: World Health Organization [online] [accessed 05/01/2021]. Available at https://apps.who.int/gb/archive/pdf_files/WHA55/ea5515.pdf
- Innocenti Declaration 2005. Infant and Young Child Feeding. In: UNICEF [online] [accessed 05/01/2021]. Available at www.unicef-irc.org/publications/pdf/declaration_eng_p.pdf
- Lactancia materna en cifras, 2017: tasas de inicio y duración de la lactancia en España y en otros países. In: Comité de Lactancia Materna de la AEP [online] [accessed 05/01/2021]. Available at www.aeped.es/comite-nutricion-y-lactancia-materna/lactancia-materna/documentos/lactancia-materna-en-cifras-tasas-inicio-y
- Indicators for assessing infants and young child feeding practices. In: UNICEF [online] [accessed 05/01/2021]. Available at www.unicef.org/nutrition/files/IYCF_updated_indicators_2008_part_1_definitions.pdf
- Encuesta Nacional de Salud 2017. In: Ministerio de Sanidad, Consumo y Bienestar Social [online] [accessed 05/01/2021]. Available at www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_pres_web.pdf
- Hernández Aguilar MT, González Lombide E, Bustinduy Bascaran A, Argüelles Cañedo CA, Martínez-Herrera Merino A, Blanco del Val A, et al. Centros de Salud IHAN (Iniciativa de Humanización de la Atención al nacimiento y la Lactancia). Una garantía de calidad. Rev Pediatr Aten Primaria. 2009;11:513-29.
- Pallás Alonso CR, Soriano Faura J, Colomer Revuelta J, Cortés Rico O, Esparza Olcina MJ, Galbe Sánchez-Ventura J, et al. Apoyo a la lactancia materna en Atención Primaria. Rev Pediatr Aten Primaria. 2019;21:191-201.
- Estrategia centros de salud IHAN. Manual para la acreditación. Unicef/OMS. In: IHAN España [online] [accessed 05/01/2022]. Available at www.ihan.es/docs/documentacion-acreditacion/centros_salud/Manual_para_la_acreditacion_IHAN_en_AP_2018.pdf
- Moore ER, Bergman N, Anderson GC, Medley N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2016;11:CD003519.
- Victora CG, Bahl R, Barros AJ, Franca GV, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475-90.
- Aguayo Maldonado J, Posadas del Amo S, Ramírez Troyano A, Rello Yubero C, Martínez Rodríguez MT, Bonal Pitz P. Lactancia materna en Andalucía. Sevilla: Consejería de Salud; 2005.
- Rodríguez Pérez MJ, Álvarez Vázquez E, Medina Pomares J, Velicia Peñas C, Cal Conde A, Goicoechea Castaño A, et al. Prevalencia de lactancia materna en el Área Sanitaria de Vigo, Galicia. Rev Esp Salud Pública. 2017;91:e1-e9.
- Herrera Gómez A, Ramos Torrecillas J, Ruiz C, Ocaña Peinado FM, De Luna Bertos E, García Martínez Prevalencia del inicio precoz de la lactancia materna. Nutr Hosp. 2019;36:786-91.
- García Vera C, Viar Urieta M, Fernández León A, Surribas Murillo C, del Toro Calero C, Rodríguez- López Marquez GA, et al. Prevalencia global y por comunidades autónomas de los distintos tipos de lactancia durante el primer año de vida, a partir del seguimiento de una cohorte de 2066 niños. Rev Pediatr Aten Primaria Supl. 2020;(28):20-1.
- Giménez Pérez V, Jimeno Sierra B, Valles Pinto MD, Sanz de Miguel E, Prevalencia de la lactancia materna en un centro de salud de Zaragoza (España). Factores sociosanitarios que la condicionan. Rev Pediatr Aten Primaria. 2015;17:17-26.
- Oribe M, Lertxundi A, Basterrechea M, Begiristain H, Santa Marina l, Villar M, et al. Prevalencia y factores asociados con la duración de la lactancia materna exclusiva durante los primeros 6 meses en la cohorte INMA de Guipúzcoa. Gac Sanit. 2015;29:4-9.
- Ramiro González MD, Ortiz Marrón H, Arana Cañedo-Argüelles C, Esparzo Olcina MJ, Cortés Rico O, Terol Claramonte M, et al. Prevalencia de Lactancia materna y factores asociados con el inicio y duración de la lactancia materna exclusiva en la Comunidad de Madrid entre los participantes del estudio ELOIN. An Pediatr (Barc). 2018;89:32-43.
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. In: Cochrane Database of systematic review [online] [accessed 05/01/2022]. Available at www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003517.pub2/full
- Cuadrón Andrés l, Samper Villagrasa MP, Álvarez Sauras ML, Lasarte Velillas JJ, Rodríguez Martínez G; Grupo colaborativo CALINA. Prevalencia de la lactancia materna durante el primer año de vida en Aragón. Estudio CALINA. An Pediatr (Barc). 2013;79:312‐
- Sacristán Martín AM, Lozano Alonso JE, Gil Costa M, Vega Alonso AT Red Centinela Sanitaria de Castilla y León. Situación actual y factores que condicionan la lactancia materna en Castilla y León. Rev Pediatr Aten Primaria. 2011;13:33-46.
- Gómez Fernández-Vegue M; Comité de Lactancia materna y Comité de Nutrición de la Asociación Española de Pediatría. Recomendaciones de la Sociedad Española de Pediatría sobre la alimentación In: Asociación Española de Pediatría [online] [accessed 05/01/2022]. Available at www.aeped.es/sites/default/files/documentos/recomendaciones_aep_sobre_alimentacio_n_complementaria_nov2018_v3_final.pdf