

Nurse experience in performing spirometry in a pediatric team
Sarai Marsiñach Sáncheza, M.ª Carmen Santafé Méndeza, Isabel Gascón Casaredib
aEnfermera de Pediatría. CAP La Marina. Institut Català de la Salut. Barcelona. España.
bPediatra. Unidad de Neumología Pediátrica. Hospital Sant Joan de Déu. Barcelona. España.
Correspondence: S Marsiñach . E-mail: smarsinachsanchez@gmail.com
Reference of this article: Marsiñach Sánchez S, Santafé Méndez MC, Gascón Casaredi I. Nurse experience in performing spirometry in a pediatric team. Rev Pediatr Aten Primaria. 2021;23:e137-e145.
Published in Internet: 26-10-2021 - Visits: 14390
Abstract
Introduction: in Spain, asthma is the second leading cause of morbidity and chronic illness in the paediatric population, following obesity. Asthma is one of the most frequent presenting complaints at the primary care level, and its early diagnosis and treatment allow control of the disease, modifying its course and improving patient quality of life.
Objective: the aim of the study was to describe our experience in performing spirometry in the paediatric population and encourage other primary care centres to offer this test to their patients.
Material and methods: a total of 81 spirometry tests were performed in 67 patients aged 5 to 14 years between January 2019 and February 2020. Of the 81 tests, 16% were baseline tests, 32.1% were spirometry with bronchodilator responsiveness testing (BRT), and 51.9% spirometry with exercise challenge and BRT All tests were performed with a Sibelmed Datospir Touch 511-B00-MU1 spirometer.
Results: twenty-six spirometry tests included a BRT, with negative results of the BRT in 15 and positive results in 11. Another 32 tests included an exercise challenge, which was positive compared to baseline in 9, while in 23 there were no significant differences relative to baseline, although in 5 of them the BRT was positive.
Conclusion: it is possible to perform forced spirometry in paediatric patients with high-quality results at the primary care level if the necessary material resources and qualified personnel are available. Providing this service can reduce waiting lists and improve asthma control.
Keywords
● Asthma ● Children ● Nurse ● Pediatrics ● Primary care ● SpirometryINTRODUCTION
At present, asthma is the second leading cause of morbidity and chronic illness in the paediatric population of Spain, following obesity.1 The overall prevalence of asthma is of 10%, and is higher in coastal regions.2-4
Thus, this is a frequent disease in the paediatric age group, in which early diagnosis and treatment allow control of the disease, modifying its course and improving the quality of life of affected individuals.1 Adequate asthma control preserves lung function, improves quality of life, prevents mortality and reduces health care costs.1,3
Asthma is one of the most frequent presenting complaints at the primary care level and accounts for an approximate total expenditure of 535 million euro per year for the population of children under 16 years with asthma in Spain.1,3,5
Asthma is a clinical diagnosis based on compatible findings in the history-taking and physical examination signs such as wheezing, shortness of breath, cough and tightness in the chest.1,2 Still, these signs and symptoms are not specific to asthma, so clinical practice guidelines recommend performance of objective diagnostic tests, such as forced spirometry.2,4
Forced spirometry is used to confirm the diagnosis, rule out other diseases, assess severity, assess the response to treatment and monitor the course of disease.3,6,7 There are additional methods used to assess lung function in children, such as spirometry with bronchodilator responsiveness testing and spirometry with bronchial challenge tests.6
The bronchodilator responsiveness test (PRT) provides information on the reversibility of the airflow obstruction, and is therefore the most useful test for diagnosis and monitoring of asthma.6
Bronchial challenge tests can be performed with substances that act directly on bronchial smooth muscle or by inducing the release of endogenous mediators that cause airway narrowing through exercise, hyperventilation or administration of hypertonic saline.6
The exercise challenge test or free running test is indicated for assessment of symptoms suggestive of asthma associated with physical activity and for diagnosis of uncontrolled asthma and exercise-induced asthma.6,8
According to the most recent protocol of the Airway Group of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics), every child and adolescent with asthma should have results of some type of lung function testing documented in their health records. Ideally, lung function should be tested in the baseline evaluation, again at 3 to 6 months after initiation of maintenance therapy and at least once a year thereafter to keep the information up to date.8
In the past, spirometry was rarely used in the paediatric population at the primary care level because children were not able to perform voluntary respiratory manoeuvres as effectively as adults and adequate reference values had yet to be established. 7,9 However, in recent years several studies have demonstrated that it is possible to obtain high-quality spirometry data in children from age 3 years with the right methodology, properly trained health care staff and using reference values appropriate for age.2,7,9,10.
In the past few years, the use of functional assessment techniques has been increasing, as they facilitate the objective evaluation of asthma. It also reduces the number of patients with mild disease referred to hospitals.5,8,11
Different studies have found that the role and involvement of nursing staff in the performance of spirometry and the followup of the patient and the family is key in the management of children and adolescents with asthma. But delivery of high-quality care requires motivated health care professionals with appropriate and up-to-date training, software with settings adapted to children, the right organizational structure and adequate resources.9,12
Our primary care centre started to offer spirometry in 2016 because one of the paediatricians on staff had specialised training in paediatric pulmonology and allergy and created a care link clinic to bridge the gap between primary and hospital-based care with the aim of offering better care to patients in the centre and reduce waiting times for hospital referrals. In addition, one of the nurses had performed spirometry tests in adults for several years and had received specific training on spirometry in children, which encouraged us to start and continue offering these tests in our centre.
The aim of this article was to describe our experience with the performance of spirometry in the paediatric population and to encourage other primary care centres to offer this test.
MATERIAL AND METHODS
Participants
The children included in the study belonged to the catchment population of the paediatric care team of the Marina-Magória health district (Barcelona, Spain). We collected data between January 2019 and February 2020, taking into account that spirometry was not performed for a whole month due to staff vacations.
A total of 81 spirometry tests were performed during the period under study, of which 16% (n = 13) were baseline tests, 32.1% (n = 26) baseline spirometry with BRT, and 51.9% (n = 42) spirometry with exercise challenge test and BRT.
A total of 67 patients underwent lung function testing with spirometry, 58.2% of who were male (n = 39) and 41.8% female (n = 28). Patients were aged 5 to 14 years with a mean age of 9.5 years.
One patient underwent 7 follow-up spirometry tests and 9 patients 2 spirometry tests for different reasons.
The reasons to perform spirometry were making a definitive diagnosis of asthma, monitoring asthma, monitoring treatment or diagnosing exercise-induced asthma.
In most cases, patients already had diagnoses of asthma, dyspnoea, allergic rhinitis, acute obstructive bronchitis (AOB), cough or exercise-induced dyspnoea documented in the health record.
Procedure
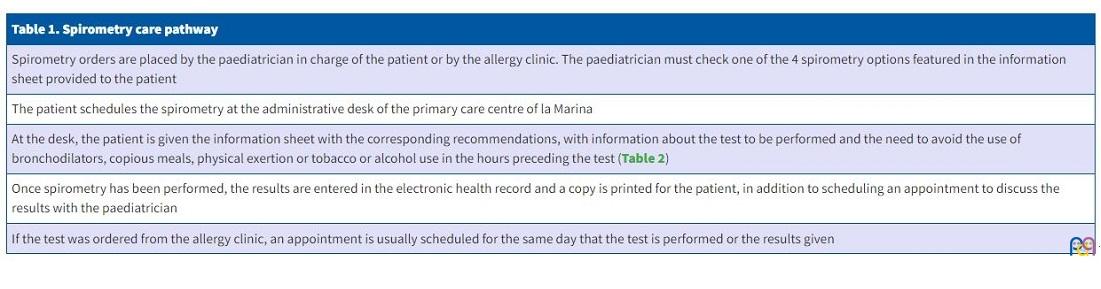
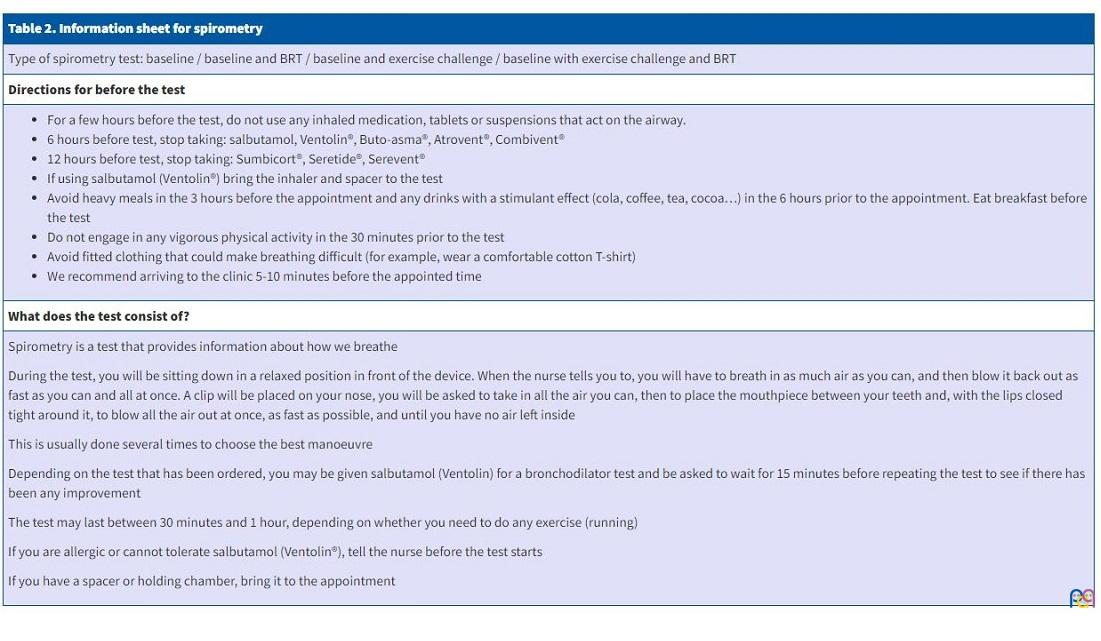
In our centre, spirometry tests are ordered by the paediatrician in charge of the patient or the paediatrician leading the allergy clinic, in adherence with the pathway established for the purpose (Table 1). Once spirometry has been requested, a date is scheduled for the test and the parents are given a printout with recommendations for the day of the appointment. This sheet gives directions to avoid use of bronchodilators, copious meals, physical activity or, in the case of adolescents, tobacco or alcohol use in the hours preceding the test (Table 2).
| Table 1. Spirometry care pathway |
|---|
| Spirometry orders are placed by the paediatrician in charge of the patient or by the allergy clinic. The paediatrician must check one of the 4 spirometry options featured in the information sheet provided to the patient |
| The patient schedules the spirometry at the administrative desk of the primary care centre of la Marina |
| At the desk, the patient is given the information sheet with the corresponding recommendations, with information about the test to be performed and the need to avoid the use of bronchodilators, copious meals, physical exertion or tobacco or alcohol use in the hours preceding the test (Table 2) |
| Once spirometry has been performed, the results are entered in the electronic health record and a copy is printed for the patient, in addition to scheduling an appointment to discuss the results with the paediatrician |
| If the test was ordered from the allergy clinic, an appointment is usually scheduled for the same day that the test is performed or the results given |
| Table 2. Information sheet for spirometry |
|---|
| Type of spirometry test: baseline / baseline and BRT / baseline and exercise challenge / baseline with exercise challenge and BRT |
| Directions for before the test |
|
| What does the test consist of? |
|
Spirometry is a test that provides information about how we breathe During the test, you will be sitting down in a relaxed position in front of the device. When the nurse tells you to, you will have to breath in as much air as you can, and then blow it back out as fast as you can and all at once. A clip will be placed on your nose, you will be asked to take in all the air you can, then to place the mouthpiece between your teeth and, with the lips closed tight around it, to blow all the air out at once, as fast as possible, and until you have no air left inside This is usually done several times to choose the best manoeuvre Depending on the test that has been ordered, you may be given salbutamol (Ventolin) for a bronchodilator test and be asked to wait for 15 minutes before repeating the test to see if there has been any improvement The test may last between 30 minutes and 1 hour, depending on whether you need to do any exercise (running) If you are allergic or cannot tolerate salbutamol (Ventolin®), tell the nurse before the test starts If you have a spacer or holding chamber, bring it to the appointment |
All the tests were performed in the spirometry clinic by a nurse experienced in performing spirometry in both adults and children. All tests were performed between 8:00 and 10:00 AM.
Spirometry was performed with a Sibelmed Datospir Touch 511-B00-MU1 spirometer, the W20S software version 511-BLA-1.06 and a disposable rigid mouthpiece. At the beginning of each session, the spirometer is calibrated with a Modelo S300 Volume 3000 calibration syringe accurate to ± 0.5%. Following the directions of the manufacturer, calibration involved performance of 1 to 5 air injection cycles aiming at obtaining a curve that fit within the boundaries established by the software.
Children were accompanied by an adult relative to help them feel at ease, and efforts made to create a pleasant environment. In our centre, spirometry is performed in one of the offices where paediatric visits are carried out regularly, a familiar setting with decoration appealing to children, to promote trust and ease anxiety.
We recorded the weight and height of the patient following the established protocol using a scale and stadiometer. We documented the age, sex and ethnicity of the patient and entered them in the electronic health records database used in our clinic (ECAP 10.0).
Before the test, we took the history of the patient, asking questions about general health and the use of medicines or other circumstances that could interfere with or contraindicate spirometry at that given time (lack of understanding or cooperation, recent haemoptysis, abdominal pain, nausea or vomiting, active respiratory infection, eye surgery or disease involving the ear, nose or throat).
In addition, before starting the manoeuvres, we explained and demonstrated the procedure to the patient.
In every case, spirometry was performed with the patient sitting down, and it was not necessary to use any other position. It is nevertheless important to remind the patient to keep a straight back, especially during the breathing manoeuvre, as there is a tendency to lean forward.
The nose clip could be used in most cases, which only needed to be removed in rare instances because the child did not tolerate it.
Children were given directions through words, gestures and body language, and the software also had an animation game in which the child had to push a rocket all the way to the moon by blowing out air.
To carry out the forced spirometry test, the child was instructed to first inhale quickly but without straining, trying to take in as much air as possible to reach the total lung capacity (TLC).
Then, the patient was asked to hold the mouthpiece in the mouth, holding it between the teeth and closing the lips around it. Then, after a pause lasting less than 2 seconds, the patient had to produce a vigorous exhalation (blowing fast and hard) in a sustained manner (to achieve maximum lung emptying) until reaching the residual volume (RV).
At the end of expiration, if recording of a flow volume loop is also needed, the test can be completed with the performance of a full inspiratory manoeuvre to TLC, asking the child to take as much air in as possible without letting go of the mouthpiece, although this manoeuvre was only performed once in our clinic at the request of the paediatrician.
Two types of criteria are applied to determine whether spirometry has been performed correctly. First, the acceptability criteria, which entail a subjective assessment by the technician performing the test. The technician has to consider whether the child has made a maximal effort, the start, middle and end of the tracings are satisfactory and the duration of expiration is less than 6 seconds (2-3 seconds in young children).
The other are the repeatability criteria. These are met when the 2 largest values of the forced vital capacity (FVC) and the 2 largest values of the forced expiratory volume in 1 second (FEV1) do not differ by more than 150 ml or more than 5%, respectively. If the FVC is equal or less than 1 l (children aged 2-6 years), the values should not differ by more than 100 ml.
Usually, spirometry requires a minimum of 2 acceptable manoeuvres in children and 3 in adolescents, and there is no recommended maximum, although in our centre we tried not to do more than 8 manoeuvres in a single appointment. On occasion, some child required more than 8 manoeuvres, so a longer resting time was allowed between manoeuvres to promote cooperation and attention in the child. If acceptable manoeuvres could still not be obtained, a new appointment was scheduled to repeat the test.
Although the spirometers used today automatically select the best manoeuvre, the nurse that performs the test verifies manually that the selection was appropriate.
Spirometry parameters are interpreted in comparison to reference values in the healthy population. In our case, the system allowed us to choose between several references, and we chose to use the values published by the Sociedad Española de Neumología y Cirugía Torácica (Spanish Society of Pulmonology and Thoracic Surgery, SEPAR).
We classified abnormal spirometry patterns (obstructive, restrictive or mixed) according to the spirometry protocol of the Airway Group of the Asociación Española de Pediatría de Atención Primaria.
Bronchodilator responsiveness testing (BRT)
The protocol for BRT in our centre consists in the performance of baseline spirometry followed by administration of 400 µg of salbutamol, or the equivalent to 4 puffs 30 seconds apart, which in paediatric patients were delivered through a holding chamber. To make the best use of the available time and be able to care for other patients, the child and accompanying adult were asked to wait for 10 to 15 minutes in the waiting area across the office. Once this time had elapsed, a second spirometry test was performed to assess for changes in the measured parameters.
We assessed the bronchodilator response by measuring the percent change relative to the predicted FEV1 value. We considered the BRT positive when the change in the FEV1 was equal or greater than 12% compared to the previous value, or 9% greater than the predicted value (≥12% or ≥200 ml) relative to the baseline in adolescents and adults.
Exercise challenge
The exercise bronchial provocation test seeks to evince the presence of an increased obstructive response in the context of physical exertion.
Prior to the test, the patient is provided with printed instructions to wear clothing appropriate for physical activity and refrain from using bronchodilators in the 12 hours prior (Table 2). The patient also must refrain from engaging in physical activity on the day of the appointment, which is why we usually schedule these tests first thing in the morning.
Before starting the test, the nurse asks questions to verify that the patient adhered to these instructions and is not experiencing any symptoms. The heart rate (HR) and oxygen saturation (SpO2) are recorded and the patient undergoes auscultation at rest.
A baseline spirometry is performed and considered valid if the FVC and FEV1 are above 80% of the respective reference values. Otherwise, a paediatrician assesses the state of the airway in the patient with a stethoscope, followed by performance of a BRT to assess the reversibility of airflow obstruction relative to baseline.
Since our primary care centre is not equipped with a treadmill or a stationary bike, the exercise consists in running in the park located behind the facility (Parque de los Derechos Humanos). Patients are asked to run continuously for 6 minutes vigorously enough to reach a heart rate greater than 85% of the maximum HR for their age (maximum HR = 210 – age in years).
The run must end abruptly and as soon as the patient is back in the clinic, without allowing time to rest, the SpO2 and HR are measured again, the patient undergoes auscultation, and the second spirometry is performed.
The second spirometry test must start within 2 minutes of discontinuing physical activity. Exercise challenge protocols call for performing serial spirometry tests at 5, 10 and 15 minutes with the option of performing additional tests at 20 and 30 minutes, unless the FEV1 decreases significantly in a shorter time span, in which case the test should be discontinued and a bronchodilator administered to the patient.
In our centre, given the type of spirometer used, the type of scheduled visits and the time available, the second spirometry test was performed 5 to 10 minutes after finishing the run, given that, based on a review of the current literature, the highest level of bronchial obstruction tends to occur 3 to 15 minutes after stopping physical activity.7 Thus, performance of spirometry at 5 and 10 minutes would be a reliable method to detect bronchial obstruction if it occurs.
We measured the HR and SpO2 and performed auscultation with both the second spirometry test (upon completing the run) and the third (10 minutes after exercising).
The spirometry parameter used to assess hyperresponsiveness is the FEV1, and the test is generally considered positive if there is a 12% or greater decrease in FEV1 compared to baseline (>10% in adolescents and adults). We ought to highlight that a negative result in the free running test does not rule out the diagnosis of exercise-induced asthma.
If there is a substantial decrease in the FEV1 or the paediatrician specifically requests it, a fourth spirometry with BRT is performed.
Any incidents during the performance of any of the tests are documented in the patient health records.
RESULTS
The spirometry clinic managed a total of 67 patients in the period under study. Although 104 appointments were scheduled, 18.3% (n = 19) of the children did not show, usually because they were ill or because they had to cancel due to field trips, camps or exams.
Four spirometry tests had to be rescheduled, in 3 cases because the acceptability and repeatability criteria were not met, either due to poor patient technique or because too many repetitions were required. In 1 case, the test had to be suspended due to technical problems with the spirometer.
Of the different tests performed (forced spirometry, spirometry with BRT and spirometry with free run challenge), what patients missed most frequently were scheduled appointments for the exercise challenge test, with 9.9% (n = 8) patients missing the appointment.
Thirteen baseline spirometry tests were conducted to assess asthma control and maintenance therapy. In the latter case, most tests evinced clinical improvement, with the exception of one patient that did not adhere to the prescribed treatment.
A total of 26 lung function tests with a BRT were performed in patients. They were ordered by by paediatricians in the centre to confirm the clinical diagnosis of asthma or to assess patients with recurrent acute obstructive bronchitis (AOB).
Out of these 26 tests with BRT, 15 were negative for bronchial hyperresponsiveness and 11 were positive.
We scheduled a total of 42 spirometry tests with a free run challenge, and the reasons for referral by paediatricians on staff were presence of cough, dyspnoea on exertion, intense fatigue after exercise and/or asthma.
Of these 42 scheduled tests, 10 could not be completed successfully: 2 had to be rescheduled due to inadequate technique and 8 due to abnormal results in the baseline spirometry (FVC and FEV1 < 80%). In these 8 patients, the decision was made to complete the assessment with a BRT, which was positive in 7 cases and negative in 1. In the patient with a negative BRT, there was no improvement in the spirometry parameters, but there was clinical improvement (improvement of wheezing detected on auscultation).
In 9 of the 32 spirometry tests with the exercise challenge, there was a decrease in FVC and FEV1 values immediately after exercise or 5 to 10 minutes after, and these patients received a diagnosis of exercise-induced asthma.
In 23 of the tests, there were no significant differences between the baseline spirometry and the spirometry following exercise. Although a significant decrease in FVC and FEV1 was not observed in association with exercise in these tests, in 5 of these patients the BRT was positive compared to baseline.
DISCUSSION
This article describes our experience with the performance of forced spirometry and the exercise challenge test in the paediatric catchment population of a primary care centre.
Today, the main goal of treatment in asthma is to control the disease. Asthma generates health care costs that amount to approximately 535 million euro a year in Spain. A large part of this expenditure is due to preventable causes, such as emergency care, either in ambulatory clinics or hospitals, and hospitalization. To reduce these costs, both preventive and disease-managing strategies should be implemented.
Primary care paediatricians are the first point of contact of paediatric patients with the health care system, and are responsible, along with paediatric nurses, for the followup of the healthy population in addition to the control and treatment of chronic diseases in children, such as asthma.
Therefore, it would be beneficial if the providers in closest contact with patients could carry out a closer and more exhaustive followup by performing tests to assess lung function for asthma diagnosis and control. We believe that bringing testing closer to the home of the patient could reduce patient absenteeism for these appointments, which would in turn improve asthma control. In our study, patients missed 23% of scheduled appointments, and 40% of missed appointments were appointments for the exercise challenge test. We wanted to compare the absenteeism observed for this test to the rate observed in specialty care clinics or other primary care centres, but we did not find current data on the subject.
In our centre, we succeeded in performing spirometry tests that met quality standards in 95.5% of the appointments at the primary care level and in the early childhood age range. It is still true that appropriate equipment is required, along with the use of age-appropriate techniques to engage the cooperation of the child and health care staff trained on spirometry and the management of the paediatric population. We believe that at present, training of health care professionals on the subject is deficient and that continuing education programmes should be developed to update knowledge and skills at regular intervals.
Furthermore, correct performance of spirometry requires time, patience and adequate organization to make the most of the time and space available.
We ought to highlight that most of our patients had not previously done spirometry tests, in spite of which we were able to obtain acceptable manoeuvres in a gratifyingly high percentage of cases.
The most frequent reason that some patients had to schedule new appointments for spirometry was that their tests did not meet the quality parameters to be considered acceptable.
As for the errors in spirometry, premature termination of the manoeuvre was the most frequent one, followed by an inadequate effort and peak flow.
Although children have fewer physical limitations compared to adults or even adolescents, their attention wanes quicker as the number of manoeuvres increases, so we consider that manoeuvres should be repeated only as long as the child continues to be engaged.
There are strengths and limitations to this descriptive study.
When it comes to its strengths, a salient aspect is that we did not find similar studies in the literature conducted in Spain and involving nursing staff, so, in sharing our experience, this article may encourage other centres to offer spirometry, as it is perceived very positively by both health care professionals and users.
Another strength of the study is that the same spirometry equipment was used for every test, in addition to their performance by appropriately trained staff.
We also have a park immediately adjacent to our centre, which makes it possible for children to engage in physical activity in a risk-free environment.
Yet another strength is that the tracings were interpreted by the same team that performed the tests, which therefore applied the same standards, in addition to also being reviewed by the paediatrician in charge of the patient.
As for the weaknesses and limitations, the main ones we can identify are that the study was conducted in a small sample, as patients were recruited exclusively from the caseload of our care team, and the study only included data from the last year. Therefore, it is possible that the number of tests performed is insufficient to draw valid conclusions.
In addition, since we were not able to find similar studies in the literature, we were not able to compare our results.
CONCLUSION
In conclusion, it is possible to perform lung function tests such as forced spirometry, spirometry with BRT and bronchial provocation tests with high-quality results in the paediatric population and at the primary care level, as long as they are performed by providers specialised in paediatric care.
Offering spirometry expands the services available to health care users, reducing the frequency of referral to speciality clinics and therefore waiting lists. It also allows us to follow up the population we serve more closely with the ultimate goal of improving disease control.
Lastly, with this article we sought to contribute to building the necessary foundations to develop measures to use available resources in primary care centres and establish similar care pathways managed by nurses.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
ABBREVIATIONS
AOB: acute obstructive bronchitis · BRT: bronchodilator responsiveness testing · HR: heart rate · FEV1: forced expiratory volume in 1 second · FVC: force vital capacity · RV: residual volume · SpO2: transcutaneous oxygen saturation · TLC: total lung capacity.
ACKNOWLEDGMENTS
We warmly thank all our colleagues in the paediatric care team of La Marina-Magoria and all medical residents and nurses for their support and their suggestions in the writing of the manuscript.
REFERENCES
- Sacristán Martín A, Arribas Santiago C, Camina Gutiérrez A, Machín Rodríguez E, Santos García J. Características del asma infantil en Atención Primaria. Mejora del seguimiento. Rev Pediatr Aten Primaria. 2008;19:593-601.
- GEMA. GEMA 5.0. Guía española para el manejo del asma. In: GEMA [online] [accessed 21/10/2021]. Available at: www.gemasma.com/
- Asensí Monzó MT, Duelo Marcos M, García Merino Á. Manejo integral del asma en Atención Primaria. AEPap (ed.). Curso Actualización Pediatría 2018. Madrid: Lúa Ediciones 3.0. 2018. pp. 489-506.
- Úbeda-Sansano MI, Cano-Garcinuño A, Rueda-Esteban S, Praena-Crespo M. Resources to handle childhood asthma in Spain: The role of plans and guides and the participation of nurses. Allergol Immunopathol (Madr). 2018;46:361-9.
- Blasco Bravo AJ, Pérez-Yarza EG, De Mercado PLY, Perales AB, Díaz Vázquez CA, Moreno Galdó A. Coste del asma en Pediatría en España: un modelo de evaluación de costes basado en la prevalencia. An Pediatr (Barc). 2011;74:145-53.
- Oliva Hernández A, Callejón Callejón A. Espirometría en el niño colaborador. Rev Esp Pediatr. 2012;68:104-13.
- Jat KR. Spirometry in children. Prim Care Respir J. 2013;22:221-9.
- Bercedo Sanz A, Úbeda Sansano I, Juliá Benito J, Praeno Crespo M, Grupo de Vías Respiratorias de la Asociación Española de Pediatría de Atención Primaria. Protocolo de Espirometría. El pediatra de Atención Primaria y la espirometría. In: Respirar.org [online] [accessed 21/10/2021]. Available at: www.respirar.org/images/pdf/grupovias/Protocolo_espirometria_GVR_2020-finalb.pdf
- Olaguíbel Rivera JM, Álvarez Puebla MJ, Vela Vizcaino C, Cambra Contín K, Uribe San Martín MP, De Esteban Chocarro B. Calidad de la espirometría en preeescolares. An Sist Sanit Navar. 2014;37:81-9.
- Comité de Enfermería de la SEICAP. Espirometría forzada en Pediatría. In: SEICAP [online] [accessed 21/10/2021]. Available at: www.seicap.es/espirometria-forzada-en-niños_38884.pdf
- García Merino Á, Carvajal Urueña I, Blanco González J. Espirometría básica en Pediatría de Atención Primaria. In: V Reunión anual de la Sociedad Asturiana de Pediatría de Atención Primaria [online] [accessed 21/10/2021]. Available at: https://cutt.ly/YRbQuXv
- Boqué Genovard M, Zamora Andreu B, Puigserver Sacares B. Estudio de la situación actual en el tratamiento del asma pediátrico en Atención Primaria de Mallorca. Rev Pediatr Aten Primaria. 2007;9:375-84.