
Vol. 23 - Num. 90
Original Papers
Breastfeeding and early childhood caries: are they associated?
Lorena García Blancoa, Nerea Martín Calvob, Edurne Ciriza Barea a, Maite Ruiz Goikoetxeac, Vanessa Fernández Iglesiad, Aitziber Barandiaran Urretabizkaiae
a, Maite Ruiz Goikoetxeac, Vanessa Fernández Iglesiad, Aitziber Barandiaran Urretabizkaiae
aPediatra. CS Ansoáin. Ansoáin. Navarra. España.
bDepartamento de Medicina Preventiva y Salud Pública. Universidad de Navarra. Pamplona. España.
cPediatra. CS de San Jorge. Pamplona. Navarra. España.
dPediatra. CS La Bañeza. León. España.
eOdontóloga. Clínica Dental Barandiaran. Pamplona. Navarra. España.
Correspondence: E Ciriza. E-mail: edurne.ciriza.barea@navarra.es
Reference of this article: García Blanco L, Martín Calvo N, Ciriza Barea E, Ruiz Goikoetxea M, Fernández Iglesia V, Barandiaran Urretabizkaia A. Breastfeeding and early childhood caries: are they associated? Rev Pediatr Aten Primaria. 2021;23:133-42.
Published in Internet: 17-06-2021 - Visits: 24860
Abstract
Introduction and objectives: there is debate whether prolonged breastfeeding is a risk factor for caries. Breastfeeding, recommended for at least two years, has been associated with several benefits, including in oral health. We reviewed the literature on the subject, and present the results observed in the cohort under study.
Methods: study conducted in a prospective, open-enrolment and multipurpose cohort of children aged 4-5 years, whose parents completed a self-administered questionnaire regarding diet and lifestyle habits. We performed a retrospective analysis of the prevalence of caries based on the duration of breastfeeding. We adjusted the analysis by age, sex, race, parental knowledge and attitudes, total energy and sugar intake and adherence to the Mediterranean diet.
Results: the sample included 370 children, of who 50 had developed caries. Breastfeeding up to 12 months was associated with a lower risk of caries, but breastfeeding longer than 12 months was associated with an increased risk (OR 2.75; 95 IC: 1.397 - 5.44; p = 0.003). The total energy and sugar intakes were not significant confounders in the association under study. Adherence to the Mediterranean diet may have a protective effect, but more research is needed to confirm it.
Conclusions: we found a significant direct association between breastfeeding for more than 12 months and the prevalence of caries. However, breastfeeding for less than 12 months had a protective effect. Our findings were consistent with the previous literature.
Keywords
● Breastfeeding ● Child ● Cohorts ● Dental caries ● PreschoolINTRODUCTION
Dental caries is currently the most frequent chronic disease in the paediatric age group, with a high prevalence in early childhood. In Spain, 31% of children aged less than 6 years have caries, which corresponds to decay in 7 million deciduous teeth.1 Dental caries is considered a sugar-dependent infectious disease. In fact, most dental associations continue to include on-demand or nocturnal bottle feeding or breastfeeding (BF) among the risk factors for dental caries.2
The association between BF and caries is a highly controversial subject. The World Health Organization (WHO) and the Asociación Española de Pediatría (Spanish Association of Pediatrics, AEP) recommend exclusive BF in the first 6 months of life, with continued BF combined with other foods through age 2 years or longer.3,4 However, some professionals recommend earlier BF cessation with the rationale that it increases the risk of tooth decay. For this reason, the Committee on Breastfeeding of the AEP issued a statement in 2015 that underscored the lack of scientific evidence supporting an association between BF and caries.5 Furthermore, there is robust evidence of the health benefits of BF, including in oral and dental health. 7-10 Other associations have stated the same position. According to the Sociedad Española de Ortodoncia (Spanish Society of Orthodontics), it is poor oral hygiene when the child already has teeth, and not BF, that may result in the development of caries. In addition, BF contributes to the development of the masticatory system, prevents oral habits that deform the mouth (such as thumb and finger sucking) and prevents dentomaxillofacial abnormalities and malocclusion.11-13 The La Leche League has also published a statement declaring that while BF is the best option for oral health, breastfed children may also develop caries, even if BF is not the cause, and therefore it is important to implement the available strategies to prevent or reduce tooth decay.14
The most recent scientific evidence demonstrates that BF has a clear protective effect against early childhood caries (ECC) when it is maintained through age 12 months. However, after age 1 year, BF does seem to be associated with an increased risk of caries.15 Specifically, we found evidence from 5 systematic reviews with meta-analyses. Ávila et al. (2015) concluded that BF may protect against caries in early childhood, but BF past age 12 months could be associated with an increased risk of ECC.16. Tham et al. (2017) found an increased risk of ECC when BF was maintained past age 12 months (odds ratio [OR], 1.99; 95% confidence interval [95 CI]: 1.35 to 2.95) compared to BF discontinued by age 12 months, and, in children BF past age 12 months, an increased risk in children BF at night or more frequently (OR: 7.14; 95 CI: 3.14 to 16.23).16 Angelika Kobyli et al. (2017) considered that the time when BF starts to be associated with an increased risk of ECC cannot be established with precision, but that once the maxillary incisors start to erupt, it would be prudent to recommend avoiding BF at night and before daytime naps and toothbrushing after feedings.18 Cui et al. (2017) found a decreased risk of caries in infants that had been breastfeed at all compared to infants that were never breastfed (OR: 0.77; 95 CI: 0.61 to 0.97; p = 0.026), although in the analysis by subgroups, children that had been breastfed for 12 months or longer the risk of caries increased significantly compared to children that have been breastfed less than 12 months (OR: 1.86; 95 CI: 1.37 to 2.52; p <0.001)19.
All these reviews highlight the substantial variability in the available evidence and conclude that further research is required to understand the increased risk of caries observed in children breastfed past age 12 months.16 Factors that need to be considered as potential confounders include socioeconomic status, exposure to fluoride and specific dietary and oral hygiene habits that may play a role in the observed association.20-22
Previous cohort studies have yielded similar results: Peres et al. (2017) concluded that children breastfed for 24 months or longer had a 2.4-fold risk of ECC compared to children breastfed for less than 12 months (relative risk [RR]: 2.4; 95 CI: 1.7 to 3.3) and that BF between ages 13 and 23 months did not have an effect on dental caries.23 The only randomised controlled trial identified in the literature search (Kramer et al., 2007) concluded that the intervention (promotion of BF) did not have an effect on the incidence of caries.24
The aim of our study was to analyse the current prevalence of dental caries in children aged 4 to 5 years and its association with the feeding modality during infancy: BF versus formula feeding (FF) and duration of BF. The most important confounders considered in the analysis were sugar intake and adherence to the Mediterranean diet, which we assessed with the KIDMED questionnaire.
MATERIAL AND METHODS
Sample
The SENDO project (Seguimiento de Escolares Navarros para un Desarrollo Óptimo [Longitudinal Study of Schoolchildren in Navarre for Optimal Development], www.proyectosendo.es) is a prospective, dynamic and multi-purpose paediatric cohort study initiated in Navarre in 2015 that uses self-reported data obtained through online questionnaires filled out by parents and children themselves. Recruitment was conducted through primary care paediatricians in health care centres or schools. The inclusion criteria were: 1) age greater than 4 and less than 6 years; 2) residence in Spain and 3) access to the Internet. There were no exclusion criteria.
The data used in this study were obtained from the baseline questionnaires completed by participants recruited from 2015 to June 2019 (n = 370).
Variables
The baseline questionnaire (Q0) collects information regarding breastfeeding (including duration), diagnosis of dental caries by a dental professional (including the number), sociodemographic variables (sex, date of birth and race), family and personal habits (parental tobacco use and age of enrolment in childcare centre/school), age at introduction of specific foods (cow’s milk, cereal and sugary drinks), food consumption frequency, and lifestyle habits (physical activity and screen time).
Statistical analysis
We conducted a retrospective analysis of the association of ECC and the duration of BF. We performed a logistic regression analysis to compare the presence or absence of caries based on the duration of BF: less than 3 months, 3 to 6 months, 6 to 9 months, 9 to 12 months, more than 12 months. We also considered the following categories: BF lasting less than 1 month, BF lasting 1 to 12 months, BF lasting more than 12 months.
The analysis was adjusted for age, sex, race, maternal age (continuous variable), adherence to the Mediterranean diet (low, moderate, high), body mass index (BMI, continuous variable), nutritional knowledge and dietary habits (low, moderate, high), total energy intake (tertiles) and sugar intake (tertiles).
We performed the statistical analysis with the software STATA 15.0. We considered p-values of less than 0.05 statistically significant.
Ethical considerations
Participation in the SENDO project is voluntary; most families are informed about the project by primary care paediatricians, and they sign an informed consent form.
The SENDO project has been approved by the Ethics Committee of Navarre under file no. 279 of 27/10/2015.
RESULTS
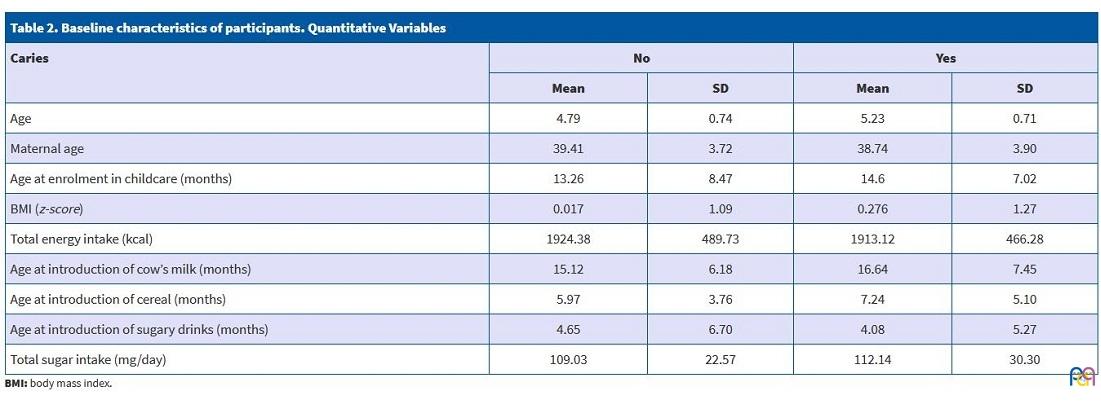
Of the 370 recruited participants, we excluded 35 that did not complete the questionnaire (9.46% loss to followup), resulting in a final sample size of 335. In this sample, 51 participants (15.22%) were fed artificial formula from birth and 284 (84.78%) were breastfed. Tables 1 and 2 summarise the baseline characteristics of participants based on whether or not they reported development of caries.
| Table 1. Baseline characteristics of participants. Qualitative variables | |||||
|---|---|---|---|---|---|
| Caries | No (%) | Yes (%) | |||
| Sex | Female | 118 | 41.4 | 28 | 56 |
| Male | 167 | 58.6 | 22 | 44 | |
| Race | Black | 2 | 0.7 | 0 | 0 |
| Asian | 1 | 0.35 | 0 | 0 | |
| White | 279 | 97.89 | 48 | 96 | |
| Hispanic/Latino | 1 | 0.35 | 1 | 2 | |
| Other | 2 | 0.7 | 1 | 2 | |
| Paternal educational attainment | No formal education | 0 | 0 | 0 | 0 |
| Compulsory primary and secondary education | 21 | 7.39 | 7 | 14 | |
| Vocational training or non-compulsory secondary education | 73 | 25.70 | 17 | 34 | |
| Undergraduate degree | 133 | 46.83 | 17 | 34 | |
| Graduate degree | 57 | 20.07 | 9 | 18 | |
| Maternal educational attainment | No formal education | 2 | 0.70 | 0 | 0 |
| Compulsory primary and secondary education | 5 | 1.75 | 3 | 6 | |
| Vocational training or non-compulsory secondary education | 40 | 14.04 | 12 | 24 | |
| Undergraduate degree | 158 | 55.44 | 22 | 44 | |
| Graduate degree | 80 | 28.07 | 13 | 26 | |
| Candies/sweets | Never or seldom | 46 | 16.67 | 7 | 14.58 |
| 2-3 times/month | 59 | 21.38 | 4 | 8.33 | |
| Once a week | 117 | 42.39 | 25 | 52.08 | |
| 2-4 times/week | 46 | 16.67 | 8 | 16.67 | |
| (nearly) every day | 8 | 2.90 | 4 | 8.34 | |
| Adherence to Mediterranean diet | Low (1) | 40 | 14.04 | 9 | 18 |
| Moderate (2) | 132 | 46.32 | 21 | 42 | |
| High (3) | 113 | 39.65 | 20 | 40 | |
| Introduction of sugary drinks <12 months | No | 23 | 8.07 | 3 | 6 |
| Yes | 262 | 91.93 | 47 | 94 | |
| Dietary knowledge of parents | <40% | 51 | 17.89 | 12 | 24 |
| 40-70% | 190 | 66.67 | 28 | 56 | |
| >70% | 44 | 15.44 | 10 | 20 | |
| Attitude of parents regarding food | <40% | 30 | 10.53 | 5 | 10 |
| 40-70% | 89 | 31.23 | 17 | 34 | |
| >70% | 166 | 58.25 | 28 | 56 | |
| Breastfeeding | No | 44 | 15.44 | 7 | 14 |
| Yes | 241 | 84.56 | 43 | 86 | |

| Table 2. Baseline characteristics of participants. Quantitative Variables | ||||
|---|---|---|---|---|
| Caries | No | Yes | ||
| Mean | SD | Mean | SD | |
| Age | 4.79 | 0.74 | 5.23 | 0.71 |
| Maternal age | 39.41 | 3.72 | 38.74 | 3.90 |
| Age at enrolment in childcare (months) | 13.26 | 8.47 | 14.6 | 7.02 |
| BMI (z-score) | 0.017 | 1.09 | 0.276 | 1.27 |
| Total energy intake (kcal) | 1924.38 | 489.73 | 1913.12 | 466.28 |
| Age at introduction of cow’s milk (months) | 15.12 | 6.18 | 16.64 | 7.45 |
| Age at introduction of cereal (months) | 5.97 | 3.76 | 7.24 | 5.10 |
| Age at introduction of sugary drinks (months) | 4.65 | 6.70 | 4.08 | 5.27 |
| Total sugar intake (mg/day) | 109.03 | 22.57 | 112.14 | 30.30 |
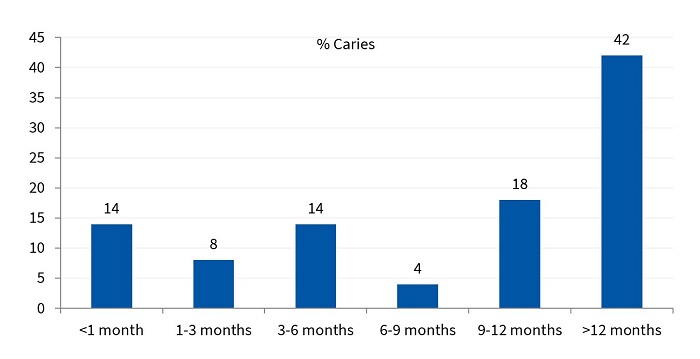
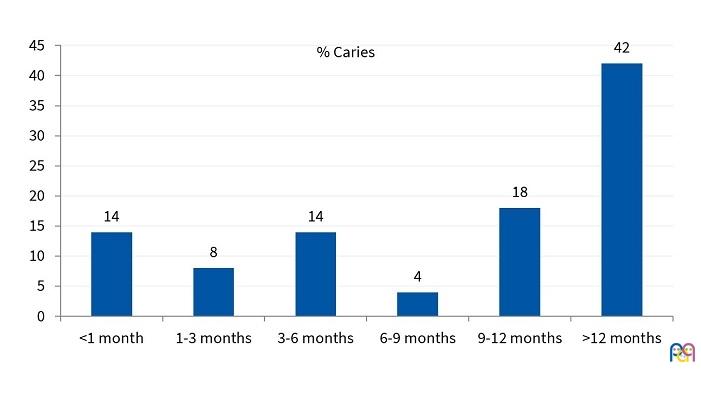
| Figure 1. Prevalence of caries in children aged 4 to 6 years in the cohort based on the duration of breastfeeding (% of total sample) |
|---|
 |
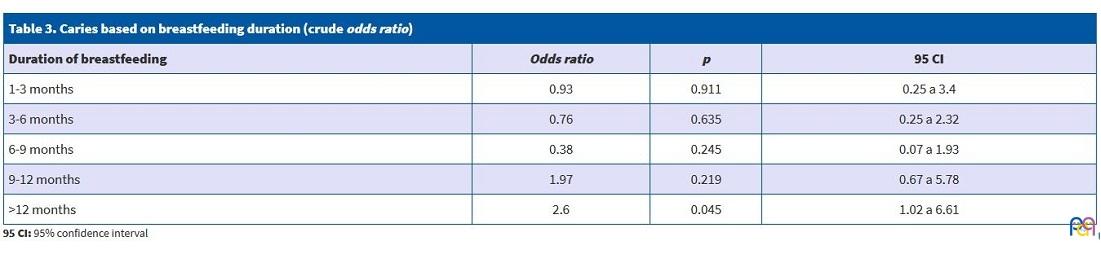
| Table 3. Caries based on breastfeeding duration (crude odds ratio) | |||
|---|---|---|---|
| Duration of breastfeeding | Odds ratio | p | 95 CI |
| 1-3 months | 0.93 | 0.911 | 0.25 a 3.4 |
| 3-6 months | 0.76 | 0.635 | 0.25 a 2.32 |
| 6-9 months | 0.38 | 0.245 | 0.07 a 1.93 |
| 9-12 months | 1.97 | 0.219 | 0.67 a 5.78 |
| >12 months | 2.6 | 0.045 | 1.02 a 6.61 |
After adjusting for age, sex, race, maternal age, total energy intake and adherence to the Mediterranean diet, we did not find statistically significant differences in the prevalence of caries based on whether participants had been breastfed or not (FF versus BF of any duration), with an OR for the total sample of 1.17 (95 CI: 0.45 to 3.03).
In the analysis by subgroups, we divided the sample into 3 groups: FF or BF lasting less than 1 month (n = 59), BF lasting 1 to 12 months (n = 195) or BF lasting more than 12 months (n = 81). Using the first group as reference, we found a lower risk of caries in the group with BF lasting less than 12 months and greater in the group with BF lasting more than 12 months, although the differences were not statistically significant.
When we compared only BF duration of more versus less than 12 months, we obtained an OR of 2.88 (95 CI: 1.41 to 5.89; p = 0.004) for BF longer than 12 months (Table 3). When we included children that were not breastfed (FF) in the reference group, the association was stronger, with an OR of 2.75 (95 CI: 1.39 to 5.44; p = 0.003) (Table 4).
| Table 4. Caries in “breastfeeding up to 12 months” group compared to “breastfeeding past 12 months” (adjusted odds ratio) | |||
|---|---|---|---|
| Breastfeeding | Odds ratio | p | 95 CI |
| Breastfeeding <12 months | 1.25 | 0.658 | 0.46 a 3.41 |
| Breastfeeding >12 months | 2.89 | 0.004 | 1.41 a 5.89 |

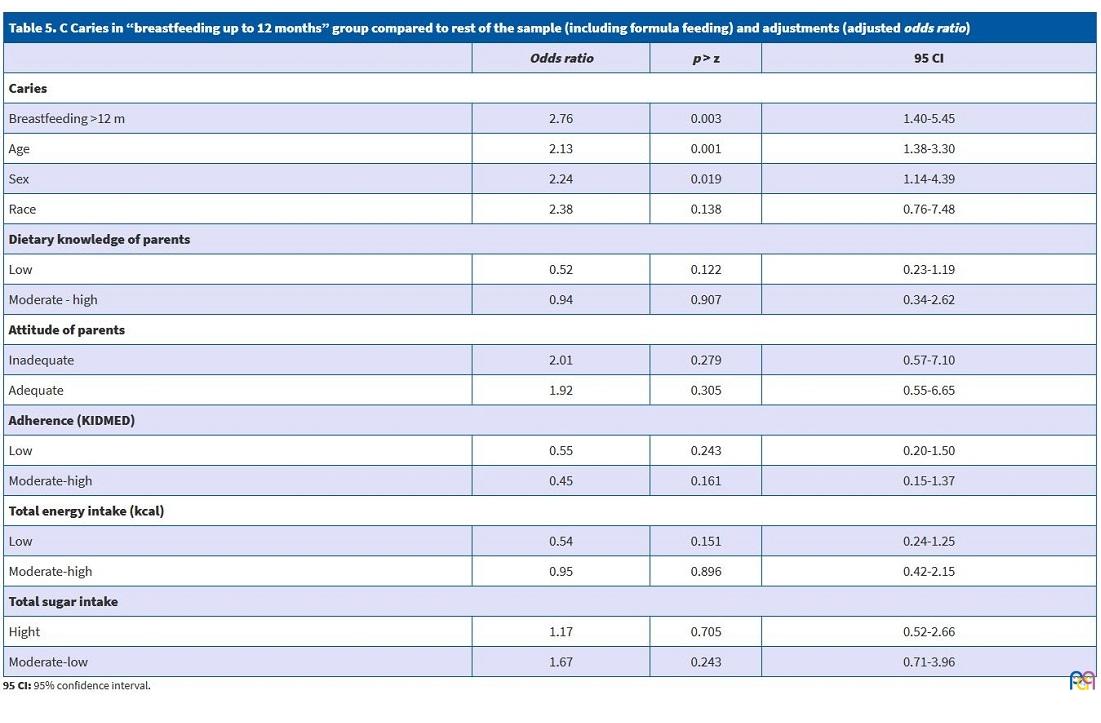
The adjusted analysis identified confounders that could contribute to an increased risk of caries, such as age (OR: 2.13; 95 CI: 1.38 to 3.30; p = 0.001) and female sex (OR: 2.23; 95 CI: 1.14 to 4.39; p = 0.019), which is probably not relevant, as this association has not been described in the previous literature. We did not find an association between the risk of caries and parental dietary knowledge and attitudes, total energy intake or total sugar intake (Table 5). Adherence to the Mediterranean diet showed a beneficial effect of marginal significance.
| Table 5. C Caries in “breastfeeding up to 12 months” group compared to rest of the sample (including formula feeding) and adjustments (adjusted odds ratio) | |||
|---|---|---|---|
| Odds ratio | p > z | 95 CI | |
| Caries | |||
| Breastfeeding >12 m | 2.76 | 0.003 | 1.40-5.45 |
| Age | 2.13 | 0.001 | 1.38-3.30 |
| Sex | 2.24 | 0.019 | 1.14-4.39 |
| Race | 2.38 | 0.138 | 0.76-7.48 |
| Dietary knowledge of parents | |||
| Low | 0.52 | 0.122 | 0.23-1.19 |
| Moderate - high | 0.94 | 0.907 | 0.34-2.62 |
| Attitude of parents | |||
| Inadequate | 2.01 | 0.279 | 0.57-7.10 |
| Adequate | 1.92 | 0.305 | 0.55-6.65 |
| Adherence (KIDMED) | |||
| Low | 0.55 | 0.243 | 0.20-1.50 |
| Moderate-high | 0.45 | 0.161 | 0.15-1.37 |
| Total energy intake (kcal) | |||
| Low | 0.54 | 0.151 | 0.24-1.25 |
| Moderate-high | 0.95 | 0.896 | 0.42-2.15 |
| Total sugar intake | |||
| Hight | 1.17 | 0.705 | 0.52-2.66 |
| Moderate-low | 1.67 | 0.243 | 0.71-3.96 |
DISCUSSION
In this study, we found BF lasting less than 12 months was associated with a decreased prevalence of caries, while BF longer than 12 months was associated with an increased prevalence.
A pathophysiological mechanism that could explain this association is the large number of feedings commonly observed in breastfed children, especially at night, when cleaning the teeth is more difficult and the production of saliva decreases. In fact, Tham found a greater increase in the risk of caries in children that continued to breastfeed frequently or to breastfeed at night from age 1 year.17 Other authors believe that the risk of tooth decay is associated with genetic or environmental factors unrelated to BF.26 Recent studies support the hypothesis that colonization by Streptococcus mutans is responsible for the development of dental caries.27,28 Another possible explanation is the potential cariogenicity of human milk (greater compared to cow’s milk but lower compared to artificial formula), as the high concentrations of lactose in contact with tooth surfaces may cause a pH reduction in dental plaque.29 While in vitro studies have demonstrated that human milk in contact with teeth does not produce a reduction in the pH, sucrose does have this effect.30
It is evident that caries is a multifactorial disease and that it is important to control the associated risk factors, or at least those that are most important. A recent systematic review and meta-analysis published in 2019 (Kirthiga et al.) analysed 123 factors associated with caries and concluded that enamel defects, the presence of other caries and colonization by Streptococcus mutans were the factors associated most strongly with tooth decay.31 There is also no evidence of an association between overweight/obesity and caries.32,33 Based on a recent systematic review,34 the recommendation of restricting consumption of foods and beverages with free sugars before bed, while founded on a solid physiological premise, is only supported by evidence of very low quality. Our results supported this view, as we did not find an association between the total sugar intake and the risk of caries.
Traditionally, it was recommended that deciduous teeth be cleaned exclusively with water or fluoride-free toothpaste due to the risk of fluorosis in young children. On the other hand, there is evidence that application of fluoride to the enamel may inhibit the demineralization of teeth produced by milk-based drinks35 and that only toothpastes with fluoride concentrations of 1000 ppm or greater have proven effective in reducing caries.36 The risk of fluorosis resulting from ingestion of toothpaste with fluoride at these concentrations and in the recommended amount is minimal.37 Our results could be explained by residual confounding, as we were not able to include the oral hygiene of participants in our analysis.
The population must educated on correct oral hygiene habits from an early age and be made aware of their importance. Current guidelines38-44 recommend that parents assist children in toothbrushing until age 6 years, and to use toothpaste with a fluoride concentration of 1000 ppm from age 0 to 3 years (using an amount the size of a rice grain). From age 3 years, the toothpaste must contain from 1000 to 1450 ppm (using a pea-sized amount) and 1450 ppm from age 6 years.
Encouraging discontinuation of BF for any reason detracts from the potential benefits of prolonged BF, blames mothers that wish to continue BF beyond 12 months and discourages other mothers from continuing to breastfeed, who then lose all the benefits of prolonged BF.5
Limitations and potential biases
Participants in cohort studies tend to be more aware of their health and take better care of it, which can give rise to nonrepresentative samples that limit the generalizability of results. However, the analysis of an association between two variables does not require a representative sample. In fact, some authors have suggested that nonrepresentative samples may be a strength in this type of studies, as the data provided by participants tend to be more valid.45
A possible explanation of the lack of significance in the association with certain variables, such as adherence to the Mediterranean diet, could be that the sample was too small.
Since the information was self-reported, there is a risk of information bias. However, in case information bias was at play, it would probably be nondifferential and move the distribution towards the null. Also, since the data were collected retrospectively, we must also consider the risk of recall bias. If participants that had breastfed longer happened to have a more accurate recall of the development of tooth decay, our analysis may have overestimated the association between BF and the prevalence of ECC.
Since the study had an observational design, there is a risk of confounding by variables that we may not have taken into account or adjusted for correctly.
CONCLUSIONS
We found a statistically significant positive correlation between BF duration greater than 12 months and the prevalence of ECC. However, BF up to 12 months was a protective factor against early childhood caries. Further research is required to investigate this association thoroughly and to account for the use of fluoride toothpaste in oral hygiene.
We did not find an association between total energy intake or total sugar intake and the prevalence of ECC. Our findings suggest an inverse association between adherence to the Mediterranean diet and the development of caries, although further research is required on this subject.
While we await the results of additional studies assessing the association of tooth decay with the combination of feeding modality in infancy, dietary habits, oral hygiene habits and other factors to establish specific risks with greater precision, we must insist on the importance of oral hygiene with fluoride toothpaste starting with the eruption of the first tooth. Given the above considerations and the multiple health benefits of BF on maternal and child health, we encourage families to prolong BF for as long as the mother and child wish.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article. The project was awarded the Nestlé-AEPap grant in 2018; neither the funding institution (Nestlé) nor the institution that awards the grant (AEPap) have been involved in the conception, design or development of the study or the writing of this article.
ABBREVIATIONS
AEP: Asociación Española de Pediatría · BF breastfeeding · BMI: body mass index · ECC: early childhood caries · FF: formula feeding · OR: odds ratio · ppm: parts per million · RR: relative risk · SD: standard deviation · WHO: World Health Organization.
REFERENCES
- La salud oral infantil, eje del Día Mundial de la salud bucodental, 2019. In: Sociedad Española de Odontopediatría [online] [accessed 09/06/2021]. Available at www.odontologiapediatrica.com/2019/03/26/la-salud-oral-infantil-eje-del-dia-mundial-de-la-salud-bucodental-2019/
- Prevención de la caries en la primera infancia. In: Sociedad Española de Odontopediatría [online] [accessed 09/06/2021]. Available at www.odontologiapediatrica.com/wp-content/uploads/2019/08/Prevenci%C3%B3n-de-la-caries-de-la-primera-infancia-rev-082019-marca-agua.pdf
- Lactancia materna. In: World Health Organization [online] [accessed 09/06/2021]. Available at www.who.int/topics/breastfeeding/es/
- Comité de Lactancia Materna de la AEP. Lactancia materna. In: Asociación Española de Pediatría [online] [accessed 09/06/2021]. Available at http://lactanciamaterna.aeped.es/
- Comité de Lactancia Materna de la AEP. Lactancia materna y caries. In: Asociación Española de Pediatría [online] [accessed 09/06/2021]. Available at www.aeped.es/sites/default/files/documentos/201502-lactancia-materna-caries.pdf
- Sankar MJ, Sinha B, Chowdhury R, Bhandari N, Taneja S, Martines J, et al. Optimal breastfeeding practices and infant and child mortality: a systematic review and meta-analysis. Acta Paediatr. 2015;104:3-13.
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012;(8):CD003517.
- Horta BL, Loret de Mola C, Victora CG. Breastfeeding and intelligence: a systematic review and meta-analysis. Acta Paediatr. 2015;104:14-9.
- Horta BL, Loret de Mola C, Victora CG. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: a systematic review and meta-analysis. Acta Paediatr. 2015;104:30-7.
- Peres KG, Cascaes AM, Nascimento GG, Victora CG. Effect of breastfeeding on malocclusions: a systematic review and meta-analysis. Acta Paediatr. 2015;104:54-61.
- La lactancia materna favorece el correcto desarrollo oral del bebé y evita la ortodoncia. In: Sociedad Española de Ortodoncia y Ortopedia Dentofacial [online] [accessed 09/06/2021]. Available at www.sedo.es/blog/185-la-lactancia-materna-favorece-el-correcto-desarrollo-oral-del-beb%C3%A9-y-evita-la-ortodoncia.html
- Boronat-Catalá M, Montiel-Company JM, Bellot-Arcís C, Almerich-Silla JM, Catalá-Pizarro M. Association between duration of breastfeeding and malocclusions in primary and mixed dentition: a systematic review and metaanalysis. Sci Rep. 2017;7:5048.
- Thomaz E, Alves C, Gomes E, Ribeiro de Almeida C, Soares de Britto E, Alves M, et al. Breastfeeding Versus Bottle Feeding on Malocclusion in Children: A Meta-Analysis Study. J Hum Lact. 2018;34:768-88.
- Salud bucodental y lactancia. In: La Liga de la Leche [online] [accessed 09/06/2021]. Available at www.laligadelaleche.es/lactancia_materna/salud_bucodental/Folleto-salud-bucodental-y-LM.pdf
- Banco de Preguntas Preevid. Asociación entre lactancia materna y caries infantil. In: Murciasalud [online] [accessed 09/06/2021]. Available at www.murciasalud.es/preevid/22833
- Avila WM, Pordeus IA, Paiva SM, Martins CC. Breast and bottle feeding as risk factors for dental caries: A systematic review and meta-analysis. PLoS ONE. 2015;10:e0142922.
- Tham R, Bowatte G, Dharmage S, Tan D, Lau M, Dai X, et al. Breastfeeding and the risk of dental caries: A systematic review and meta-analysis. Acta Paediatr Int J Paediatr. 2015;104:62-84.
- Kobylinska A, Rozniatowski P, Olczak-Kowalczyk D. Breastfeeding and early childhood caries - a systematic review. Pediatr Polska. 2017;92:417-26.
- Cui L, Li X, Tian Y, Bao J, Wang L, Xu D, et al. Breastfeeding and early childhood caries: a meta-analysis of observational studies. Asia Pac J Clin Nutr. 2017;26:867-80.
- Seow WK. Early Childhood Caries. Pediatr Clin North Am. Pediatr Clin North Am. 2018;65:941-54..
- Thitasomakul S, Piwat S, Thearmontree A, Chankanka O, Pithpornchaiyakul W, Madyusoh S. Risks for early childhood caries analyzed by negative binomial models. J Dent Res. 2009;88:137-41.
- Feldens CA, Giugliani ER, Vigo Á, Vítolo MR. Early feeding practices and severe early childhood caries in four-year-old children from southern Brazil: a birth cohort study. Caries Res. 2010;44:445-52.
- Peres KG, Nascimento GG, Peres MA, Mittinty MN, Demarco FF, Santos IS, et al. Impact of Prolonged Breastfeeding on Dental Caries: A Population-Based Birth Cohort Study. Pediatrics. 2017;140:e20162943.
- Kramer MS, Vanilovich I, Matush L, Bogdanovich N, Zhang X, Shishko G, et al. El efecto de la lactancia materna prolongada y exclusiva sobre la caries dental en niños en edad escolar temprana. Nueva evidencia de un gran ensayo aleatorizado. Caries Res. 2007;41:484-8.
- Peres K, Chaffee B, Feldens C, Flores-Mir C, Moynihan P, Rugg-Gunn A. Breastfeeding and Oral Health: Evidence and Methodological Challenges. J Dent Res. 2018;97:251-8.
- Wang X, Willing MC, Marazita ML, Wendell S, Warren JJ, Broffitt B, et al. Genetic and environmental factors associated with dental caries in children: the Iowa Fluoride Study. Caries Res. 2012;46:177-84.
- Yu LX, Tao Y, Qiu RM, Zhou Y, Zhi QH, Lin HC. Genetic polymorphisms of the sortase A gene and social-behavioural factors associated with caries in children: a case-control study. BMC Oral Health. 2015;15:54.
- Vachirarojpisan T, Shinada K, Kawaguchi Y, Laungwechakan P, Somkote T, Detsomboonrat P. Early childhood caries in children aged 6-19 months. Community Dent Oral Epidemiol. 2004;32:133-42.
- Prabhakar AR, Kurthukoti AJ, Gupta P. Cariogenicity and acidogenicity of human milk, plain and sweetened bovine milk: an in vitro study. J Clin Pediatr Dent. 2010;34:239-47.
- Neves P, Ribeiro C, Tenuta L, Leitão T, Monteiro-Neto V, Nunes A, et al. Breastfeeding, Dental Biofilm Acidogenicity, and Early Childhood Caries. Caries Res. 2016;50:319-24.
- Kirthiga M, Murugan M, Saikia A, Kirubakaran R. Factores de riesgo para la caries en la primera infancia: una revisión sistemática y metaanálisis de control de casos y estudios de cohortes. Odontología Pediatr. 2019;41:95-112.
- Sharma B, Indushekar KR, Saraf BG, Sardana D, Sheoran N, Mavi S. ¿Están relacionadas la caries dental y el sobrepeso/obesidad? Un estudio transversal en preescolares rurales y urbanos. J Indian Soc Pediatr Prev Dent. 2019;37:224-31.
- Karki S, Päkkilä J, Ryhänen T, Laitala ML, Humagain M, Ojaniemi M, et al. Body mass index and dental caries experience in Nepalese schoolchildren. Community Dent Oral Epidemiol. 2019;47:346-57.
- Baghlaf K, Muirhead V, Moynihan P, Weston-Price S, Pine C. Free Sugars Consumption around Bedtime and Dental Caries in Children: A Systematic Review. JDR Clin Trans Res. 2018;3:118-29.
- Xu Q, Zhang WR, Meng H, Wang L. Study of the effect of fluor protector on resistance to demineralization of milk beverages on enamel of primary teeth. Shanghai Kou Qiang Yi Xue. 2014;23:51-7.
- Walsh T, Worthington HV, Glenny AM, Appelbe P, Marinho VC, Shi X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2010;(1):CD007868.
- Flúor y fluoruros. In: Sociedad Española de Odontopediatría [online] [accessed 09/06/2021]. Available at www.odontologiapediatrica.com/protocolos/fluor/
- Innes NPT, Robertson MD. Recent advances in the management of childhood dental caries. Arch Dis Child. 2018;103:311-5.
- Protocolo de diagnóstico, pronóstico y prevención de la caries de la primera infancia. In: Sociedad Española de Odontopediatría [online] [accessed 04/11/2019]. Available at www.odontologiapediatrica.com/wp-content/uploads/2018/06/SEOP_-_Caries_precoz_de_la_infancia_fin4.pdf
- Vitoria Miñana I. Promoción de la salud bucodental. Recomendaciones PrevInfad/PAPPS. In: PrevInfad [online] [accessed 04/11/2019]. Available at http://previnfad.aepap.org/recomendacion/bucodental-rec
- Morata Alba J, Morata Alba L. Salud bucodental en los niños: ¿debemos mejorar su educación? Rev Ped Aten Primaria. 2019;21:e173-e178.
- Castro Reino O. Guía niño sano, boca sana. In: Consejo General Dentistas de España [online] [accessed 04/11/2019]. Available at www.consejodentistas.es/comunicacion/actualidad-del-consejo/publicaciones-del-consejo/libros-del-consejo/item/1247-guia-nino-sano-boca-sana.html
- Guidelines on Prevention of Early Childhood Caries: An EAPD Policy Document. In: European Academy of Paediatric Dentistry [online] [accessed 04/11/2019]. Available at www.eapd.eu/
- Parent Education Brochures. In: American Academy of Pediatric Dentistry [online] [accessed 04/11/2019]. Available at www.aapd.org/resources/parent/brochures/
- García Blanco L, Ciriza Barea E, Moreno-Galarraga L, Martín-Calvo N. ¿Por qué la representatividad de la muestra no siempre es importante? An Pediatr (Barc). 2018;88:361-2.