
Vol. 23 - Num. 89
Original Papers
Unintentional injuries in children: assessment of parental supervision of children by Primary Care paediatricians
Leyre Martí Martía, José M.ª Tenías Burillob, José Francisco Villaroya Lunac, Laura Uixera Marzald, Pilar Codoñer Franche
aPediatra. CS Carretera de Artés. Valencia. España.
bEpidemiólogo. Servicio de Medicina Preventiva, Hospital Padre Jofré. Valencia. España.
cPediatra. CS Fuente San Luis. Valencia. España.
dPediatra. CS de Benetusser. Valencia. España.
eServicio de Pediatra. Hospital Universitario Dr. Peset. Departamento de Pediatría, Ginecología y Obstetricia. Universitat de València. Valencia. España.
Correspondence: L Martí . E-mail: leyre.marti@gmail.com
Reference of this article: Martí Martí L, Tenías Burillo JM, Villaroya Luna JF, Uixera Marzal L, Codoñer Franch P. Unintentional injuries in children: assessment of parental supervision of children by Primary Care paediatricians. Rev Pediatr Aten Primaria. 2021;23:25-31.
Published in Internet: 17-03-2021 - Visits: 14287
Abstract
Introduction: unintentional injuries are one of the leading causes of morbidity and mortality in the paediatric population and can be prevented if the risk factors that make them more likely are identified and addressed. The degree of parental supervision is one of the factors that may affect the occurrence of unintentional injuries. The aim of our study was to compare the degree of parental supervision estimated subjectively by health care professionals and the degree measured objectively using a questionnaire validated for this purpose. The ultimate objective was to determine the need to use questionnaires to act more efficiently to address risk factors.
Material and methods: we conducted an observational, cross-sectional and analytic study to assess the agreement between the degree of parental supervision perceived by paediatricians and the degree measured using the Parental Supervision Attributes Profile Questionnaire (PSAPQ), which has been adapted and validated for use in Spanish translation.
Results: we found no correlation between the agreement between the degree of parental supervision perceived by paediatricians and the degree measured using the PSAPQ.
Conclusions: validated methods need to be used to objectively measure the risk factors involved in unintentional injuries in children, including the degree of parental supervision, in order to avoid perception biases and address these factors as efficiently as possible.
Keywords
● Parental supervision ● Prevention ● Unintentional child injuryINTRODUCTION
Unintentional child injuries are considered a public health problem on account of the sudden morbidity and mortality they cause in previously healthy children and of the social and psychological impact on affected children and their families.
In Spain, unintentional injury is the second leading cause of death in the paediatric population following cancers,1 and therefore the leading cause of death in previously healthy children. In addition, they are preventable and to some extent predictable when appropriate measures are taken.
Due to the impact and frequency of these accidents, it is very important to study the risk factors that promote them. This would allow more efficient interventions and therefore reducing the incidence of this problem. Of the many risk factors that may give rise to an unintentional injury, the medical literature has repeatedly emphasised the degree of parental supervision.2-6 Thus, most unintentional injuries in the paediatric population could be preventable with proper supervision from the caregivers, especially in young children.
One of the objectives of primary care (PC) paediatricians is the primary and secondary prevention of unintentional injuries, which can be pursued in practice through counselling, educational campaigns and other means. Good prevention requires knowing the attitude of parents in regard to their child’s risk of unintentional injury, and it is very important that this can be assessed objectively.
There is evidence that questionnaires are a valid and reliable tool to study parental behaviour.7 In 2006, Morrongiello and Corbett developed and validated the Parental Supervision Attributes Profile Questionnaire (PSAPQ),5 a questionnaire in English comprised by 29 items that assesses the degree of parental supervision of children using a 5-point Likert scale and structured in 4 subscales: protectiveness (items 1-9), supervision (items 10-18), risk tolerance (items 19-26), and belief in fate (items 27-29). This scale is validated for children aged 2 to 5 years.
This questionnaire was adapted and validated for the Portuguese language in 20138 and for the Spanish language in 20199 to be applied in children aged 2 to 5 years.
For these reasons, we sought to analyse the concordance between the estimated degree of parental supervision perceived by PC paediatricians and the degree of supervision measured objectively through the use of the transcultural adaptation and translation to Spanish of the PSAPQ. Thus, our objective was to assess the usefulness of an objective instrument for use in PC clinics that would facilitate more efficient intervention.
MATERIAL AND METHODS
Before starting the study, we asked for permission from the author of the original PSAPQ in English (Barbara A. Morrongiello) and obtained approval by the Clinical Research Ethics Committee of the Hospital Universitario Dr. Peset of Valencia, Spain.
We conducted an observational, cross-sectional and analytical study to assess the agreement between the degree of parental supervision estimated by PC paediatricians and the degree of supervision measured objectively with the adapted and validated Spanish version of the PSAPQ,10 and the identification of other potential risk factors that may influence the degree of parental supervision. To do so, the Spanish version of the PSAPQ was administered to 149 parents or legal guardians of children aged 2 to 5 years selected at random from those that attended the routine Healthy Child Programme visits at the participating primary care centres between August 4, 2015 and May 2, 2017. These centres were located in the Valencia metropolitan area, mainly in the city of Valencia.
After informing the parents or legal guardians about the study and ensuring that no exclusion criterion applied (history of intentional injury, language barrier, refusal to participate), we asked them to sign an informed consent form to participate in the study.
Once enrolled, parents were given a booklet in which were asked to fill out the validated version of the PSAPQ adapted and translated to Spanish and several questions on demographic and socioeconomic characteristics (occupation, educational attainment and nationality of the parents, number of siblings and sibling position of the patient).
The booklet also contained a section to be filled out by the paediatrician or paediatric nurse to collect data on the following: relevant medical history of the patient, history of unintentional injury in the past 6 months, degree of supervision of the included child by the parents based on the perception of the health provider answering the questions, with the latter item scored on a 5-point Likert scale ranging from very low to very high. These items had to be filled out after the parents had submitted the completed questionnaire to avoid potential biases, as providers would not be inhibited in responding since the parents would not see their answers to these questions.
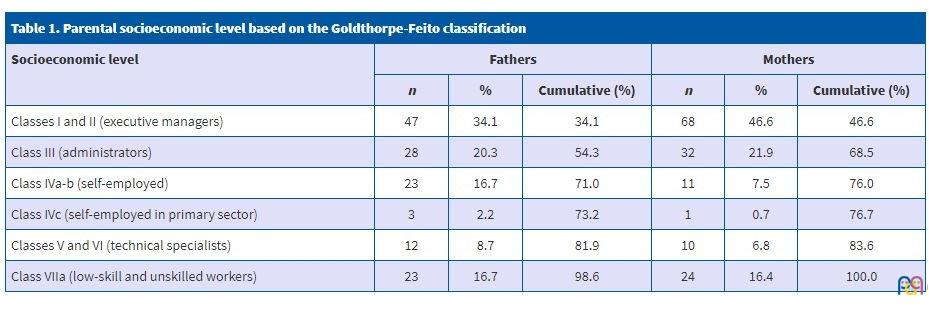
To assess the socioeconomic level of the household we used Goldthorpe-Feito classification, as proposed by the Sociedad Española de Epidemiología (Spanish Society of Epidemiology).10
We conducted an inferential analysis using the software SPSS version 22.0 to assess the agreement between the degree of parental supervision attributed by health care professionals and the degree measured objectively in each of the 4 subscales of the PSAPQ.
RESULTS
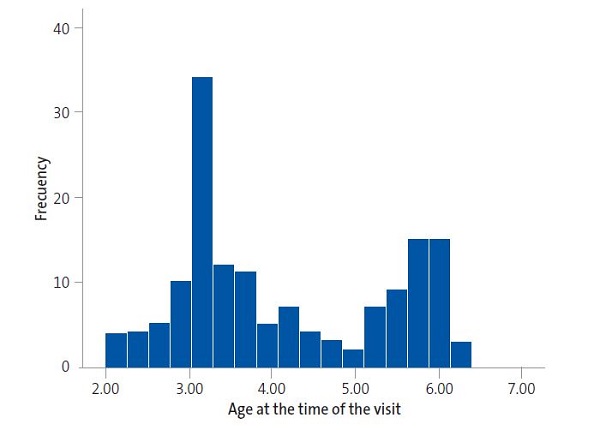
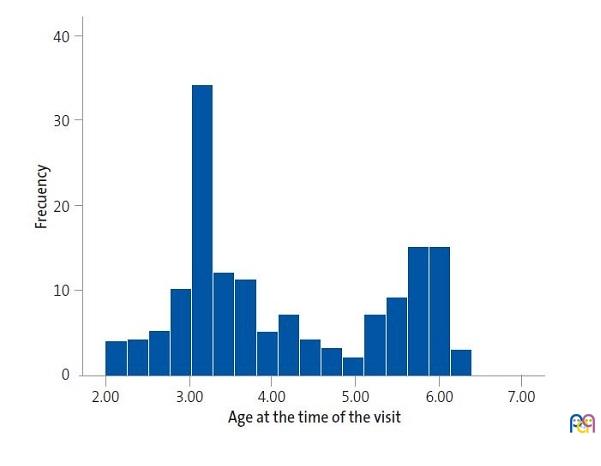
We recruited a total of 149 participants, parents of 77 girls and 72 boys. Figure 1 shows the age distribution of included children.Table 1 presents the socioeconomic characteristics of participating families.
| Figure 1. Age distribution of included children |
|---|
 |
| Table 1. Parental socioeconomic level based on the Goldthorpe-Feito classification | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Socioeconomic level | Fathers | Mothers | |||||||
| n | % | Cumulative (%) | n | % | Cumulative (%) | ||||
| Classes I and II (executive managers) | 47 | 34.1 | 34.1 | 68 | 46.6 | 46.6 | |||
| Class III (administrators) | 28 | 20.3 | 54.3 | 32 | 21.9 | 68.5 | |||
| Class IVa-b (self-employed) | 23 | 16.7 | 71.0 | 11 | 7.5 | 76.0 | |||
| Class IVc (self-employed in primary sector) | 3 | 2.2 | 73.2 | 1 | 0.7 | 76.7 | |||
| Classes V and VI (technical specialists) | 12 | 8.7 | 81.9 | 10 | 6.8 | 83.6 | |||
| Class VIIa (low-skill and unskilled workers) | 23 | 16.7 | 98.6 | 24 | 16.4 | 100.0 | |||
When it came to parental supervision, the classification of parents based on the degree of supervision perceived by health care professionals shows that more than half of couples were considered to supervise their children to a normal (46.7%) or high (31.3%) degree (Table 2).
| Table 2. Degree of parental supervision perceived by the health provider | |||
|---|---|---|---|
| Degree of supervision | n | % | Cumulative (%) |
| Low | 4 | 2.7 | 2.7 |
| Normal | 70 | 46.7 | 49.7 |
| High | 47 | 31.3 | 81.2 |
| Very high | 28 | 18.7 | 100.0 |

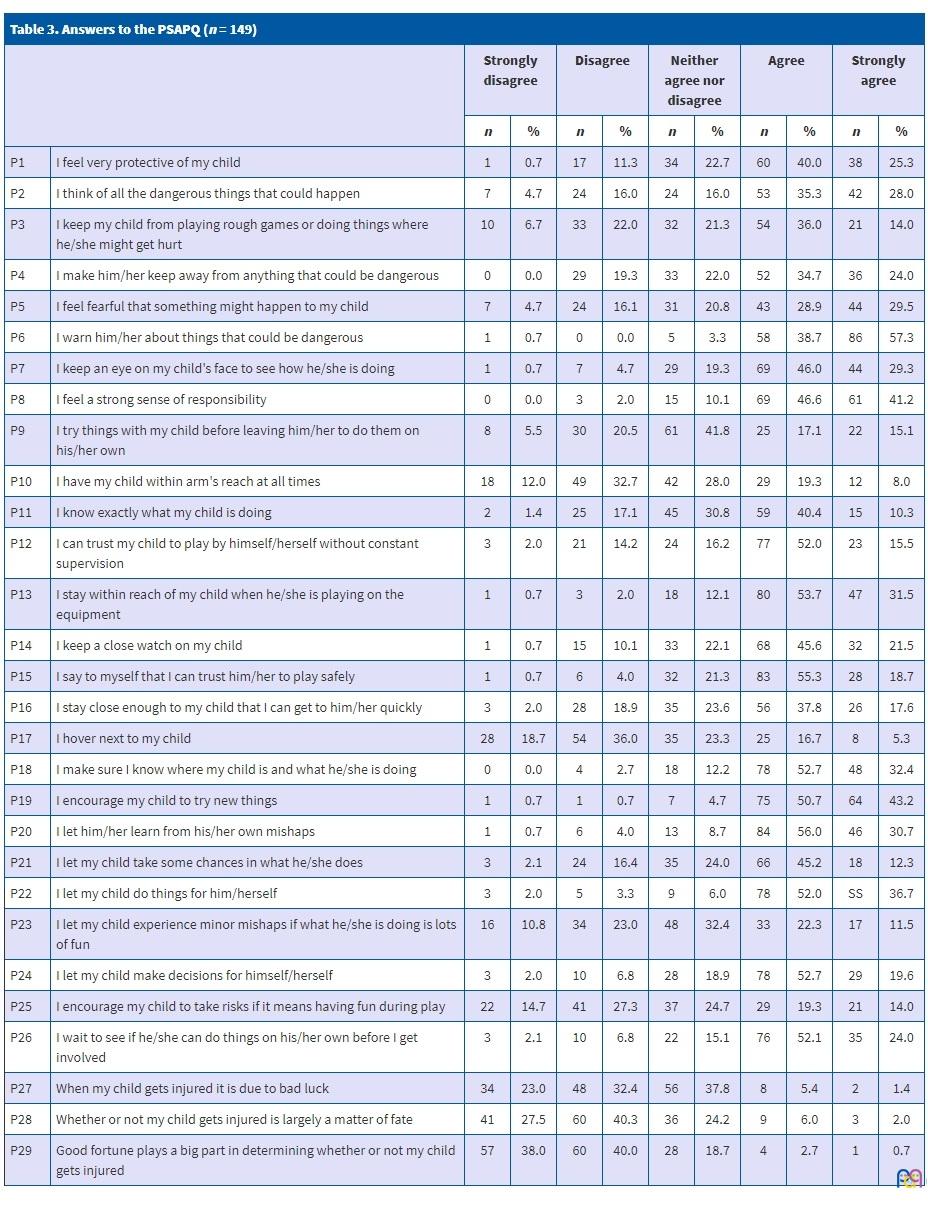
Table 3 summarizes the responses obtained through the objective PSAPQ adapted and validated for the Spanish language for each item of the questionnaire. We found that the most frequently answer choice was “agree”, both for items associated with a higher degree of parental supervision (supervision and protectiveness) and for items associated with a lower degree (tolerance of children taking risks and belief in fate).
| Table 3. Answers to the PSAPQ (n = 149) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Strongly disagree | Disagree | Neither agree nor disagree | Agree | Strongly agree | |||||||
| n | % | n | % | n | % | n | % | n | % | ||
| P1 | I feel very protective of my child | 1 | 0.7 | 17 | 11.3 | 34 | 22.7 | 60 | 40.0 | 38 | 25.3 |
| P2 | I think of all the dangerous things that could happen | 7 | 4.7 | 24 | 16.0 | 24 | 16.0 | 53 | 35.3 | 42 | 28.0 |
| P3 | I keep my child from playing rough games or doing things where he/she might get hurt | 10 | 6.7 | 33 | 22.0 | 32 | 21.3 | 54 | 36.0 | 21 | 14.0 |
| P4 | I make him/her keep away from anything that could be dangerous | 0 | 0.0 | 29 | 19.3 | 33 | 22.0 | 52 | 34.7 | 36 | 24.0 |
| P5 | I feel fearful that something might happen to my child | 7 | 4.7 | 24 | 16.1 | 31 | 20.8 | 43 | 28.9 | 44 | 29.5 |
| P6 | I warn him/her about things that could be dangerous | 1 | 0.7 | 0 | 0.0 | 5 | 3.3 | 58 | 38.7 | 86 | 57.3 |
| P7 | I keep an eye on my child's face to see how he/she is doing | 1 | 0.7 | 7 | 4.7 | 29 | 19.3 | 69 | 46.0 | 44 | 29.3 |
| P8 | I feel a strong sense of responsibility | 0 | 0.0 | 3 | 2.0 | 15 | 10.1 | 69 | 46.6 | 61 | 41.2 |
| P9 | I try things with my child before leaving him/her to do them on his/her own | 8 | 5.5 | 30 | 20.5 | 61 | 41.8 | 25 | 17.1 | 22 | 15.1 |
| P10 | I have my child within arm's reach at all times | 18 | 12.0 | 49 | 32.7 | 42 | 28.0 | 29 | 19.3 | 12 | 8.0 |
| P11 | I know exactly what my child is doing | 2 | 1.4 | 25 | 17.1 | 45 | 30.8 | 59 | 40.4 | 15 | 10.3 |
| P12 | I can trust my child to play by himself/herself without constant supervision | 3 | 2.0 | 21 | 14.2 | 24 | 16.2 | 77 | 52.0 | 23 | 15.5 |
| P13 | I stay within reach of my child when he/she is playing on the equipment | 1 | 0.7 | 3 | 2.0 | 18 | 12.1 | 80 | 53.7 | 47 | 31.5 |
| P14 | I keep a close watch on my child | 1 | 0.7 | 15 | 10.1 | 33 | 22.1 | 68 | 45.6 | 32 | 21.5 |
| P15 | I say to myself that I can trust him/her to play safely | 1 | 0.7 | 6 | 4.0 | 32 | 21.3 | 83 | 55.3 | 28 | 18.7 |
| P16 | I stay close enough to my child that I can get to him/her quickly | 3 | 2.0 | 28 | 18.9 | 35 | 23.6 | 56 | 37.8 | 26 | 17.6 |
| P17 | I hover next to my child | 28 | 18.7 | 54 | 36.0 | 35 | 23.3 | 25 | 16.7 | 8 | 5.3 |
| P18 | I make sure I know where my child is and what he/she is doing | 0 | 0.0 | 4 | 2.7 | 18 | 12.2 | 78 | 52.7 | 48 | 32.4 |
| P19 | I encourage my child to try new things | 1 | 0.7 | 1 | 0.7 | 7 | 4.7 | 75 | 50.7 | 64 | 43.2 |
| P20 | I let him/her learn from his/her own mishaps | 1 | 0.7 | 6 | 4.0 | 13 | 8.7 | 84 | 56.0 | 46 | 30.7 |
| P21 | I let my child take some chances in what he/she does | 3 | 2.1 | 24 | 16.4 | 35 | 24.0 | 66 | 45.2 | 18 | 12.3 |
| P22 | I let my child do things for him/herself | 3 | 2.0 | 5 | 3.3 | 9 | 6.0 | 78 | 52.0 | SS | 36.7 |
| P23 | I let my child experience minor mishaps if what he/she is doing is lots of fun | 16 | 10.8 | 34 | 23.0 | 48 | 32.4 | 33 | 22.3 | 17 | 11.5 |
| P24 | I let my child make decisions for himself/herself | 3 | 2.0 | 10 | 6.8 | 28 | 18.9 | 78 | 52.7 | 29 | 19.6 |
| P25 | I encourage my child to take risks if it means having fun during play | 22 | 14.7 | 41 | 27.3 | 37 | 24.7 | 29 | 19.3 | 21 | 14.0 |
| P26 | I wait to see if he/she can do things on his/her own before I get involved | 3 | 2.1 | 10 | 6.8 | 22 | 15.1 | 76 | 52.1 | 35 | 24.0 |
| P27 | When my child gets injured it is due to bad luck | 34 | 23.0 | 48 | 32.4 | 56 | 37.8 | 8 | 5.4 | 2 | 1.4 |
| P28 | Whether or not my child gets injured is largely a matter of fate | 41 | 27.5 | 60 | 40.3 | 36 | 24.2 | 9 | 6.0 | 3 | 2.0 |
| P29 | Good fortune plays a big part in determining whether or not my child gets injured | 57 | 38.0 | 60 | 40.0 | 28 | 18.7 | 4 | 2.7 | 1 | 0.7 |
Later on, we performed an inferential analysis that yielded the results shown in Figure 2.
| Figure 2. Degree of parental supervision based on the PSAPQ and the perception of the health care provider |
|---|
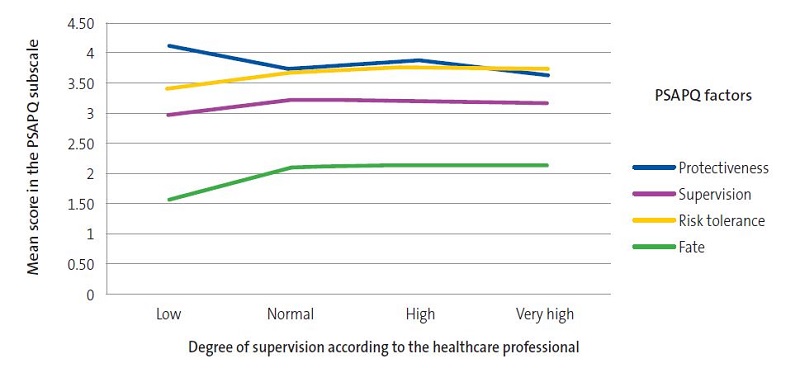 |
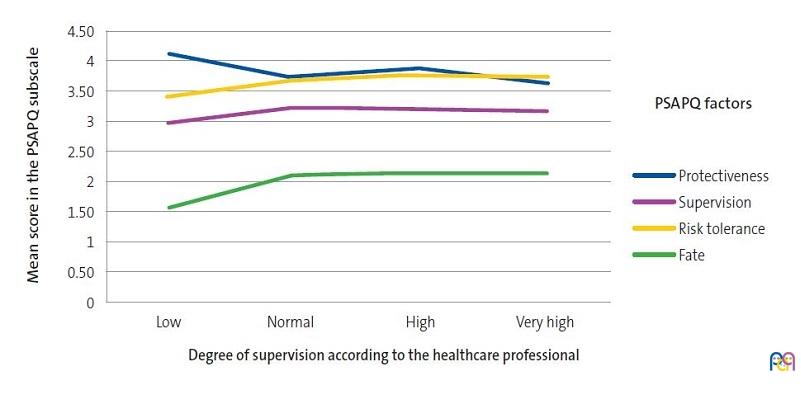
When we analysed the subscales associated with a greater degree of parental supervision (protectiveness and supervision), we found that when professionals reported perceiving low parental supervision, the objective measurement obtained through the PSAPQ showed this was not the case. However, we did find agreement when the subjective estimates were high, with a tendency to overestimate very high degrees of supervision. However, the analysis of the subscales associated with a low degree of supervision showed that when health professionals perceived low tolerance of risk-taking by the child or a belief in fate or inevitability, objective measures of these factors were actually medium to high (the actual degree of parental supervision was lower compared to the level estimated by the provider).
Based on these findings, it is reasonable to state that there is no agreement between the subjective estimation of parental supervision by health professionals and the degree of parental supervision measured objectively through the administration of the PSAPQ. In addition, since, as we noted above, most health care providers responded that the degree of supervision of children by caregivers was normal to high, the data suggest that there is a tendency to overestimate by providers compared to the objective measure.
DISCUSSION
There is no isolated risk factor that promotes the occurrence of unintentional injuries in children, but it is rather a combination of several of these factors along with various intrapersonal and interpersonal characteristics that account for increases in the probability of accidents.11,12 Knowledge of these factors is very important for the purpose of prevention and reducing the mortality associated with these injuries.
Keeping these associations in mind is important at the PC level, as most primary prevention of unintentional injuries in children take place in this care setting, and preventing these injuries is one of the stated goals of the Child Health Programme of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics).13 There are also studies that show that the PC paediatrician is the professional best suited to carry out these activities.14
Thus, articles on this subject have been published in the past few years. For instance, one published in 200415 that reviewed the Spanish and international literature on the potential risk factors involved in unintentional child injuries described to and provided strategies or advice on how to address each of them. The authors underscored the importance of PC in changing attitudes and knowledge through health education. In 2009, the PrevInfad/PAPPS published another review16 of the literature on these risk factors (social and family factors, household characteristics, walkers, etc) and proposed interventions to be delivered at the PC level to address each of them. However, none of these studies mention the degree of parental supervision as a factor associated with the risk of unintentional injury in children. We also found no articles assessing the association between the subjective perception of PC paediatricians of these factors and objective reality.
On account to the above, the aim of our study was to assess this association and the need to use an objective questionnaire in PC paediatrics practice to adequately assess and address parental supervision, which is considered a factor related to the risk of unintentional injury in children.2-6
Our study did not find a correlation between the degree of parental supervision measured with the PSAPQ and the degree perceived by paediatric providers, which evinces the need of using a specific test at the PC level to accurately establish the degree of parental supervision of children in order to provide guidance and develop strategies specific for each family based on the results, which would increase the efficiency of interventions.
CONCLUSIONS
Unintentional child injuries are one of the leading causes of morbidity and mortality in the paediatric population in addition to having psychological and economic repercussions in the affected child, the family and society overall.
An awareness of the risk factors that promote these accidents and interventions to address them are key to reduce the incidence of unintentional child injuries. This is also one of the objectives of the practice of PC paediatrics.
Our study found disagreement between the degree of parental supervision perceived by health care professionals and the degree measured objectively by the transcultural adaptation to Spanish of a validated test, which evinces the need to use this tool in PC clinics in order to be more efficient in preventing this risk factor through the use of campaigns and messages adapted to each situation.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
PC: primary care · PSAPQ: Parental Supervision Attributes Profile Questionnaire.
REFERENCES
- Instituto Nacional de Estadística (INE). Mortalidad por causas 2017. In: Instituto Nacional de Estadística [online] [accessed 03/03/2021]. Available at: www.ine.es/jaxi/tabla.do?type=pcaxis&path=/t00/mujeres_hombres/tablas_1/l0/&file=d09003.px
- Morrongiello B, Ondejko L, Littlejohn A. Understanding toddlers’ in home injuries: II. Examining parental strategies, and their efficacy, for managing child risk injury. J Pediatr Psychol. 2004;29:433-6.
- Morrongiello B, Ondejko L, Littlejohn A. Understanding toddlers’ in home injuries: I.context, correlates and determinants. J Pediatr Psychol. 2004;29:415-31.
- Morrongiello B, House K. Measuring parent attributes and supervision behaviors relevant to child injury risk: examining the usefulness of questionnaire measures. Inj Prev. 2004;10:114-8.
- Morrongiello BA, Corbett M. The Parent Supervision Attributes Profile Questionnaire: A measure of supervision relevant to children’s risk of unintentional injury. Inj Prev. 2006;12:19-23.
- Schnitzer PG, Dowd MD, Kruse RL, Morrongiello BA. Supervision and risk of unintentional injury in young children. Inj Prev. 2015;21:e63-e70.
- Watson M, Benford P, Coupland C, Clacy R, Hindmarch P, Majsak-Newman G, et al. Validation of a home safety questionnaire used in a series of case-control studies. Inj Prev. 2014;20:336-42.
- Andrade C, Carita AI, Cordovil R, Barreiros J. Cross-cultural adaptation and validation of the Portuguese version of the Parental Supervision Attributes Profile Questionnaire. Inj Prev. 2013;19:421-7.
- Martí Martí L, Tenías Burillo JM, Graullera Millás M, Fernández Castaño MT, Barona Zamora P, Codoñer-Franch P. Validación y adaptación transcultural al español del Parental Supervision Attributes Profile Questionnaire: método de medición de la supervisión parental. Rev Esp Salud Publica. 2019;93:e201908053.
- Regidor E. La clasificación de clase social de Goldthorpe: marco de referencia para la propuesta de medición de la clase social del grupo de trabajo de la Sociedad. Rev Esp Salud Publica. 2001;1:13-22.
- Jiménez de Domingo A, Rubio García E, Marañon Pardillo R, Arias Constanti V, Frontado Haiek LA, Soriano Arola M, et al. Epidemiología y factores de riesgo de las lesiones por caídas en niños menores de un año. An Pediatr (Barc). 2017;86:337-43.
- Schwebel DC, Bounds ML. The role of parents and temperament on children’s estimation of physical ability: links to unintentional injury prevention. J Pediatr Psychol. 2003;2 8:505-16.
- Asociación Española Pediatría Atención Primaria. Programa de salud infantil. 1.ª edición. Madrid: Exlibris Ediciones SL; 2009.
- Buñuel Álvarez JC, García Vera C, González Rodríguez P, Aparicio Rodrigo M, Barroso Espadero D, Cortés Marina RB, et al. ¿Qué profesional médico es el más adecuado para impartir cuidados en salud a niños en Atención Primaria en países desarrollados? Revisión sistemática. Rev Pediatr Aten Primaria. 2010;12:s9-s72.
- Casaní Martínez C. Accidentes en la infancia: su prevención, tarea de todos. Rev Pediatr Aten Primaria. 2004;6:583-95.
- Esparza Olcina MJ, Grupo PrevInfad/PAPPS Infancia y Adolescencia. Prevención de lesiones infantiles por accidentes. Rev Pediatr Aten Primaria. 2009;11:657-66.