

Retrospective study of patients with a confirmed diagnosis of whooping cough treated in the emergency room of a tertiary hospital
Marta Marín Andrésa, Aída M.ª Gutiérrez Sánchezb, Carmelo Guerrero Laleonab, Matilde Bustillo Alonsoc, Virginia Gómez Barrenad, Carmen Campos Callejad
aMIR-Pediatría. Hospital Universitario Miguel Servet. Zaragoza. España.
bServicio de Pediatría. Hospital Infantil Universitario Miguel Servet. Zaragoza. España.
cUnidad de Infectología Pediátrica. Servicio de Pediatría. Hospital Universitario Miguel Servet. Zaragoza. España.
dUnidad de Urgencias de Pediatría. Hospital Universitario Miguel Servet. Zaragoza. España.
Correspondence: M Marín. E-mail: marta_marin91@hotmail.com
Reference of this article: Marín Andrés M, Gutiérrez Sánchez AM, Guerrero Laleona C, Bustillo Alonso M, Gómez Barrena V, Campos Calleja C. Retrospective study of patients with a confirmed diagnosis of whooping cough treated in the emergency room of a tertiary hospital. Rev Pediatr Aten Primaria. 2020;22:e197-e201.
Published in Internet: 16-11-2020 - Visits: 12842
Abstract
Introduction: the aim of the study was to analyse the clinical characteristics, diagnostic tests performed and treatment used in patients with pertussis evaluated in the paediatric emergency setting.
Material and methods: we conducted a retrospective descriptive study of patients with pertussis that sought care in the paediatric emergency department of a tertiary care hospital between March 2014 and October 2017.
Results: the sample included 89 patients with a mean age of 1.67 ± 2.9 years. Of the total, 98.9% presented with cough, 33% with inspiratory whoop and 34.8% with apnoea. Sixty-four percent of cases occurred in the context of an epidemic of cough or pertussis. The mean number of emergency visits made during a single episode of disease was 1.4. The most frequent diagnoses in the initial emergency visit were cough (36%), suspected pertussis (22.5%), upper respiratory tract infection (19.1%) and bronchiolitis (9%). Fifty-six patients were admitted to hospital (62.9%) with a mean age of 0.38 ± 1.2 years. Cultures for detection of Bordetella were performed in 88 cases (positive for B. pertussis in 38 and B. parapertussis in 3), and PCR tests in 73 (positive for B. pertussis in 70 and B. parapertussis in 3).
Conclusions: the diagnosis of pertussis is usually challenging, as its initial symptoms are nonspecific. Early diagnosis is essential for early initiation of treatment and adequate contact prophylaxis.
Keywords
● Whooping coughINTRODUCTION
Pertussis is an acute respiratory infection that manifests with characteristic coughing fits and is caused by Bordetella pertussis or parapertussis. The disease is transmitted through the airborne droplets emitted during coughing and is highly contagious.1,2
Since the manifestations of pertussis are frequently nonspecific, the diagnosis is usually delayed.3 Patients are often diagnosed after the 3-week window when antibiotics may be useful to shorten the course of disease and the duration of coughing.4 Consequently, pertussis generates a considerable number of paediatric emergency visits until the diagnosis is established.
Pertussis is most severe in newborns and young infants, potentially resulting in death. In December 2015, the autonomous community of Aragon in Spain introduced routine vaccination against pertussis during pregnancy with the aim of protecting infants until the primary vaccine series of the childhood immunisation schedule.
The aim of our study was to analyse the epidemiological and clinical characteristics of cases of pertussis, the diagnostic tests performed and the treatments given to patients with a confirmed diagnosis of pertussis that visited the paediatric emergency department of a tertiary care hospital.
MATERIAL AND METHODS
We conducted a retrospective and descriptive study of patients given a diagnosis of pertussis confirmed by detection of Bordetella in culture or by polymerase chain reaction (PCR) that sought care in the paediatric emergency department of a tertiary care hospital between March 2014 and October 2017.
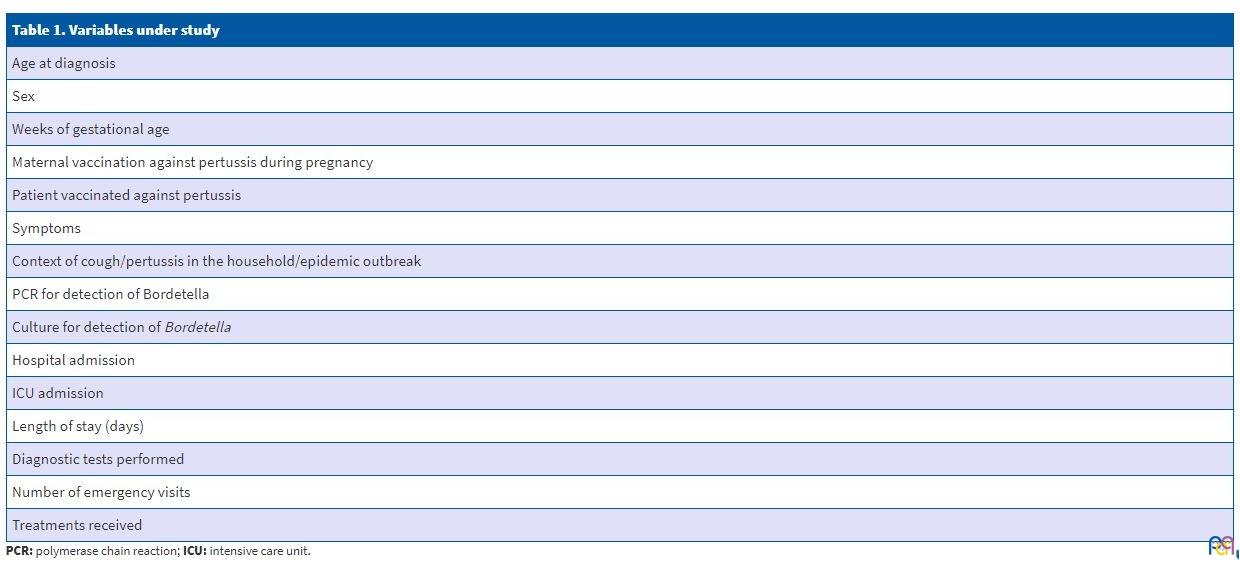
We searched the emergency department electronic health records database for patients with a discharge diagnosis of “pertussis-like syndrome” or “pertussis”. We excluded patients in who pertussis was suspected but with negative results of culture and PCR for detection of Bordetella.Table 1 details the variables under study.
| Table 1. Variables under study |
|---|
| Age at diagnosis |
| Sex |
| Weeks of gestational age |
| Maternal vaccination against pertussis during pregnancy |
| Patient vaccinated against pertussis |
| Symptoms |
| Context of cough/pertussis in the household/epidemic outbreak |
| PCR for detection of Bordetella |
| Culture for detection of Bordetella |
| Hospital admission |
| ICU admission |
| Length of stay (days) |
| Diagnostic tests performed |
| Number of emergency visits |
| Treatments received |
RESULTS
The sample included 89 patients with a confirmed diagnosis of pertussis. Fifty-five percent were female and 45% male. In addition, 13.4% were born preterm. The mean age at diagnosis was 1.67 ± 2.9 years and the range was 12 days to 12 years. Of all patients, 56.1% were aged less than 6 months and 29.2% less than 2 months.
When it came to the presenting complaints of the patients that visited the emergency department, 98.9% presented with cough (77.5% in coughing fits and 43.8% associated with vomiting), 33% with inspiratory whoop and 34.8% with apnoea. Fever was present in 14.6%. Sixty-four percent of cases occurred in the context of an outbreak of pertussis or cough. The mean number of emergency visits made during a single episode of disease was 1.48 ± 0.78 (range, 1-4); and 33.7% of patients visited the emergency room twice or more for a single episode.
The patients received the following diagnoses in the initial emergency visit: cough (36%), suspected pertussis (22.5%), upper respiratory tract infection (19.1%), bronchiolitis (9%), bronchitis (2.2%), laryngitis (3.4%), choking (2.2%), pneumonia (1.1%) and other (4.5%).
Fifty-six patients (62.9%) were admitted to hospital, of who 44 (78.5%) were aged less than 4 months. Four patients (4.5%), with a mean age of 1.3 months (range, 21 days-2 months) required transfer to the intensive care unit. There was 1 death, in a patient aged 1 ½ months with malignant pertussis. This patient developed severe myocardial dysfunction with pulmonary hypertension, acute respiratory distress and eventually sepsis caused by Klebsiella pneumoniae. The mean length of stay was 8.02 ± 5.51 days (range, 2-28). The mean age of the patients admitted to hospital was 0.38 ± 1.2 years.
Culture for identification of Bordetella was performed in 88 cases and was positive for B. pertussis in 38 and for B. parapertussis in 3. Also, PCR tests for detection of Bordetella were performed in 73 cases and were positive for B. pertussis in 70 cases and for B. parapertussis in 3.
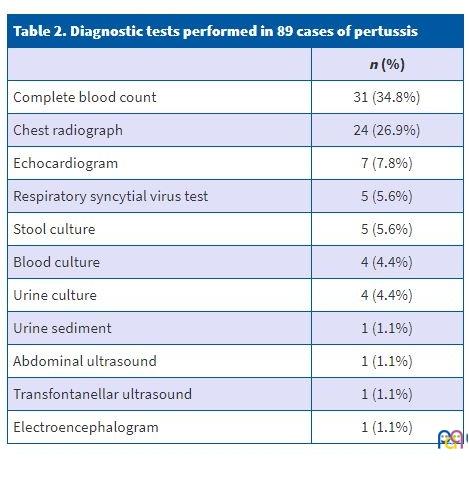
Blood tests were ordered in 34.8% of cases, with white blood cell (WBC) counts greater than 15 000/µl detected in 51.7% and WBC counts greater than 60 000/µl detected in 3.2%. Seven patients underwent an echocardiographic evaluation, which detected pulmonary hypertension in 2 (Table 2). Five (8.9%) of the 56 patients admitted to hospital, all of who were tested for detection of respiratory syncytial virus, were found to have this coinfection. Other microbiological tests included performance of stool culture for viral detection in 5 cases, with isolation of rotavirus in 1.
| Table 2. Diagnostic tests performed in 89 cases of pertussis | |
|---|---|
| n (%) | |
| Complete blood count | 31 (34.8%) |
| Chest radiograph | 24 (26.9%) |
| Echocardiogram | 7 (7.8%) |
| Respiratory syncytial virus test | 5 (5.6%) |
| Stool culture | 5 (5.6%) |
| Blood culture | 4 (4.4%) |
| Urine culture | 4 (4.4%) |
| Urine sediment | 1 (1.1%) |
| Abdominal ultrasound | 1 (1.1%) |
| Transfontanellar ultrasound | 1 (1.1%) |
| Electroencephalogram | 1 (1.1%) |
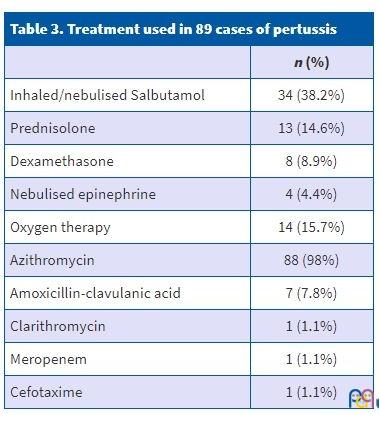
All patients received azithromycin for 5 days except 1, who was treated with clarithromycin for 7 days. Table 3 provides information on other treatments received in the emergency department or during the hospital stay. Two of the four patients that required admission to the intensive care unit required respiratory support with high-frequency oscillatory ventilation.
| Table 3. Treatment used in 89 cases of pertussis | |
|---|---|
| n (%) | |
| Inhaled/nebulised Salbutamol | 34 (38.2%) |
| Prednisolone | 13 (14.6%) |
| Dexamethasone | 8 (8.9%) |
| Nebulised epinephrine | 4 (4.4%) |
| Oxygen therapy | 14 (15.7%) |
| Azithromycin | 88 (98%) |
| Amoxicillin-clavulanic acid | 7 (7.8%) |
| Clarithromycin | 1 (1.1%) |
| Meropenem | 1 (1.1%) |
| Cefotaxime | 1 (1.1%) |
Seventy-six percent of patients aged more than 2 months had received at least 1 dose of a pertussis vaccine. Between March 2014 and December 2015 (before the introduction of routine vaccination of pregnant women), there were 65 cases (29 in infants aged ≤ 2 months). From December 2015 through October 2017, there were 24 cases (11 in infants aged ≤ 2 months). Out of these 24 cases, 65.5% occurred in children of mothers that had been vaccinated during pregnancy.
DISCUSSION
Pertussis is an acute bacterial infection caused by Bordetella pertussis or B. parapertussis, exclusively human pathogens that can infect individuals of all ages.5 Its incidence has decreased in developed countries thanks to the introduction of vaccination in infants. However, in recent years there has been an increase in cases, especially in adolescents and young adults, in Canada, the United States, Australia and some European countries.6 In Spain, despite a high vaccination coverage rate, there are still outbreaks of pertussis, with cyclical incidence peaks occurring every 3 to 5 years. Since 2010 there has been a progressive increase in the incidence of disease, the associated hospital admissions and mortality, especially in infants aged less than 1 year. In the region of Aragon, the increase was most pronounced in 2014 and 2015 and also affected infants the most. Some of the possible explanations for this phenomenon are advances in rapid diagnostic techniques, the waning immunity over time after vaccination and the lower effectiveness of the acellular vaccine compared to whole-cell vaccines.7
Adolescents and adults tend to develop mild forms of disease, but infants aged less than 4 months are the most vulnerable group, with a high incidence of complications and a high mortality.5 In the sample under study, 78.5% of patients admitted to hospital were aged less than 4 months and all patients that required admission to the intensive care unit were aged 2 months or younger. The mean length of stay was higher compared to other studies conducted in Spain.6,7
Most studies in the literature describe a mild predominance of the female sex, which was also observed in our sample.6
Sixty-four percent of cases were diagnosed in the context of an outbreak of cough or pertussis, a proportion that was higher compared to those reported by other Spanish studies, which range from 44% to 54%.6,8 The identification of a family member with prolonged cough allows a prompt diagnosis and prophylactic treatment of contacts in the family at risk of infection.5,6 However, early diagnosis may be challenging in some cases, as the clinical manifestations are nonspecific, previous vaccination alters the course of disease, mixed infections are frequent and physicians continue to have a low level of suspicion.5 Such delays in diagnosis result in patients making more visits for a single episode of disease. In our case series, 33.7% of the patients visited the emergency department at least twice in a single episode. We have not found references in the literature on the subject of repeated visits associated with this infection.
Pertussis was suspected in nearly 25% of patients in their first visit to the emergency department. The most frequent diagnosis given in the first emergency visit before confirmation of pertussis was upper respiratory tract infection, as its clinical manifestations overlap those of the catarrhal stage of pertussis.9 Consequently, in patients presenting with cough of unknown aetiology and duration greater than 15 days, the origin of the cough should be investigated and pertussis included in the differential diagnosis.10
The severity of the symptoms depends on several factors, including age, the strength of the immune response and the extent of systemic bacterial dissemination. In infants, bacteria descend to the lower respiratory tract and, via an unclear mechanism, produce necrotizing bronchitis and diffuse alveolar damage. In more severe cases, these pathological events can lead to pulmonary hypertension, respiratory failure, and even death. Pulmonary hypertension develops as an indirect effect of the toxin through induction of hyperleukocytosis.2 Leukocytosis is recognised as one of the characteristic laboratory findings in this disease, although it is not always present. In a study conducted in Spain that included 24 patients admitted to hospital with manifestations compatible with pertussis over a 5-year period, 25% had a WBC count greater than 15 000/µl. However, the diagnosis of pertussis was confirmed microbiologically in only 11 cases.7 In our case series, 51.7% of patients in who a complete blood count was performed had a WBC count greater than 15 000/µl, and all of them received a diagnosis of pertussis. In addition, one patient had a WBC count greater than 60 000/µl and was given a diagnosis of malignant pertussis.
After the introduction of routine vaccination of pregnant women against pertussis in Aragon in December 2015, there were 24 cases of pertussis over a period of 23 months compared to 65 cases in the 21 months preceding the introduction of this public health measure. We ought to highlight that despite the reduction in the incidence of pertussis, 65.5% of the cases that occurred after the enactment of this measure occurred in infants of vaccinated mothers.
The diagnosis of pertussis is usually challenging due to the nonspecificity of the initial symptoms. In our sample, the most frequent differential diagnosis was upper respiratory tract infection, followed by acute bronchiolitis. Nearly 80% of patients admitted to hospital were infants aged less than 4 months. The diagnostic tests performed most frequently were tests for detection of coinfection by respiratory syncytial virus and a complete blood count. Nearly all patients received azithromycin.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
PCR: polymerase chain reaction.
REFERENCES
- Guimarães LM, Carneiro EL, Carvalho-Costa FA. Increasing incidence of pertussis in Brazil: a retrospective study using surveillance data. BMC Infect Dis. 2015;15:442.
- Kilgore PE, Salim AM, Zervos MJ, Schmitt HJ. Pertussis: microbiology, disease, treatment, and prevention. Clin Microbiol Rev. 2016;29:449-86.
- World Health Organization (WHO). Pertussis vaccines: WHO position paper. Weekly Epidemiol Rec. 2010;85:385-400.
- Gopal DP, Barber J, Toeg D. Pertussis (whooping cough). BMJ. 2019;364:l401.
- Campins M, Moreno-Pérez D, Gil de Miguel A, González-Romo F, Moraga-Llop FA, Arístegui-Fernández J, et al. Tosferina en España. Situación epidemiológica y estrategias de prevención y control. Recomendaciones del Grupo de Trabajo de tosferina. Enferm Infecc Microbiol Clin. 2013;31:240-53.
- Villalobos-Pinto E, Martínez-Villanueva J, Cano-Fernández J, Flores-Pérez P, Sánchez-Bayle M. Factores de riesgo de complicaciones y duración del ingreso hospitalario en pacientes con tosferina. Rev Pediatr Aten Primaria. 2012;14:207-15.
- Red de Vigilancia Epidemiológica de Aragón. Secciones de Vigilancia Epidemiológica. Tosferina en Aragón. Años 2000-2015 [online] [accessed 13/11/2020]. Available at www.aragon.es/documents/20127/674325/20160829_tos_ferina_informe.pdf/791212ad-f0f3-0d18-781f-185fb254d751
- Rivero-Martín MJ, Díaz-Velázquez E, Grasa-Lozano C, P. Galán-del Río P, Zafra-Anta M, Navalón-Cebrián R. Tosferina: una enfermedad prevenible en aumento. Hospitalización en menores de 5 años en un centro de segundo nivel (periodo 2008-2012). Acta Pediatr Esp. 2015;73:10-3.
- Heininger U. Update on pertussis in children. Expert Rev Anti Infect Ther. 2010;8:163-73.
- Van Esso DL. Actualización en tosferina. Pediatr Integral. 2014;28:101-7.