
Vol. 15 - Num. 60
Original Papers
Management of pediatric dental injury in the Emergency Department of a tertiary hospital
Raquel Núñez Ramosa, J Díaz Díazb, S Mesa Garcíac, AI Romance Garcíad, M Marín Ferrerc
aSección de Gastroenterología, Hepatología y Nutrición Infantil. Servicio de Pediatría. Hospital Universitario 12 de Octubre. Madrid. España.
bMIR-Pediatría. Servicio de Urgencias de Pediatría, Hospital Universitario 12 de Octubre. Madrid. España.
cServicio de Urgencias de Pediatría, Hospital Universitario 12 de Octubre. Madrid. España.
dServicio de Cirugía Oral y Maxilofacial, Hospital Universitario 12 de Octubre. Madrid. España.
Correspondence: R Núñez . E-mail: nunezramos.raquel@gmail.com
Reference of this article: Núñez Ramos R, Díaz Díaz J, Mesa García S, Romance García AI, Marín Ferrer M. Management of pediatric dental injury in the Emergency Department of a tertiary hospital. Rev Pediatr Aten Primaria. 2013;15:307-13.
Published in Internet: 28-11-2013 - Visits: 30313
Abstract
Introduction: dental injury is very common in childhood and a frequent reason for consultation in pediatric emergency departments.
Objectives: to study the management of dental injury in a tertiary hospital.
Material and methods: retrospective descriptive study. All patients under 15 years old consulting for dental injury in the Pediatric Emergency Department of Hospital 12 de Octubre between September 2008 and August 2010 were included. During this period of time a specific management protocol of these patients was started.
Results: a total of 374 patients were treated, 63% being males, with a median age of 4.45 years. In 84% of cases the etiology was casual, followed by a 3% sports-related accident. Thirty-two percent of the patients were referred from other centers for Maxillofacial Surgery evaluation. In 60% of cases, children were treated exclusively by pediatricians. The most common reasons for maxillofacial surgery evaluation were: suture of gingival laceration (6.4%), dental extraction (3%) and ferulization (1.3%); 83.4% required only medical treatment.
Conclusions: dental injury is a common reason for consultation in the pediatric emergency department and referral to other centers. Most patients have mild lesions so they need neither complementary studies nor surgery treatment and should be managed by pediatricians following agreed protocols.
Keywords
● Dental injury ● Maxillofacial Surgery ● Paediatric emergencyINTRODUCTION
Dentoalveolar trauma is the second leading reason for seeking dental care in children following tooth decay and a frequent cause of emergency room visits and referral to reference hospitals. There is a broad range in type of injury and its consequences. While there are many minor injuries that can be treated at the outpatient level and leave no sequelae, those which result in the fracture or loss of a permanent tooth have long-lasting aesthetic, functional, economical and psychosocial effects1,2. The paediatrician is often the first specialist caring for these patients, and having a set protocol like the one used in Hospital Universitario 12 de Octubre3, designed by paediatricians and specialists in paediatric maxillofacial surgery, facilitates and standardises the safe management of these patients.
The purpose of this study was to describe the characteristics of dental injuries treated in our Emergency Care department over 23 months, and to describe the care provided following the implementation of this protocol.
MATERIALS AND METHODS
We did a retrospective descriptive study that included every patient younger than 15 years who presented with dental trauma in our emergency department between September 2008 and August 2010.
The patients were identified by means of the Paediatrics Emergency database of the Hospital Universitario 12 de Octubre, which uses de ICE-9 coding system. We collected data for the following variables: age, sex, healthcare area of origin, aetiology of the trauma, affected tooth, type of injury, type of specialist who treated the patient, and type of treatment received.
We created the database using Access® 2007, and processed the data for statistical analysis with the SPSS® software, version 15.0 for Windows® XP.
The study was approved by the Ethics Board of our centre, and patients were included in the study after signing the corresponding informed consent form.
RESULTS
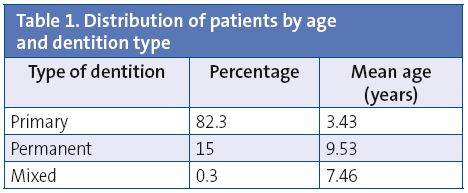
Between September 2008 and August 2010, 94,093 patients came to our hospital’s emergency room. The 374 patients younger than 15 years seeking care for dental trauma were included in the study, amounting to 0.4% of the emergency visits for that period. Out of these patients, 63% were male. The average age of the patients was 4.45 years. In 82.3% of the cases, patients came for primary teeth injuries (the average age for this group was 3.43 years), while permanent teeth were affected in 15% of the cases (average age of 7.46 years) (Table 1).
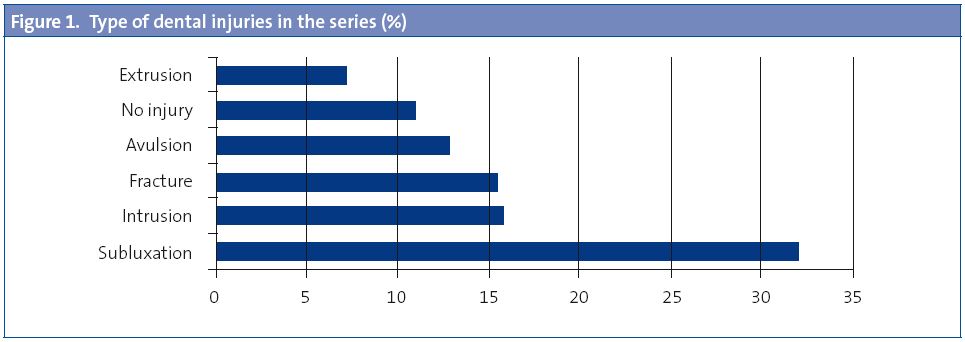
An accidental fall or collision was the aetiology found in 84.2% of the cases, with the second most frequent being sports-related accidents (2.7%) and then violence (0.3%). The aetiology of the trauma was not recorded in the chart in 12% of the cases. The most common presenting problem was loose teeth (32.4%), followed by intrusion (15.8%), uncomplicated fracture (15.5%) and avulsion (12.8%). In 11% of patients, no dental injury was found in the course of examination.
The most frequently injured teeth were the maxillary incisors (83.4%), followed by the mandibular incisors (3.5%).
Out of all patients, 44% belonged to the healthcare area served by our hospital, while 39.3% came from other areas; the area from which the patient came was not recorded in 16.6% of the cases. Of all patients, 32% were referred by an outpatient healthcare centre or another hospital to be evaluated by a maxillofacial surgeon. In the interval prior to the implementation of the protocol (August 2008-September 2009),the number of referral patients accounted for 39.6% of treated patients in that period, a percentage that decreased to 23% once the protocol was implemented and promoted.
Adhering to the protocol, 60% of the patients were managed exclusively by paediatricians. Care from the maxillofacial surgeon was most frequently sought for suturing gingival lacerations (6.4%), tooth extractions (3%) and dental splinting (1.3%). Of all patients, 83.4% required medical care alone. Supplemental tests were performed in 2.9% of the cases. None of the patients was admitted to the hospital.
DISCUSSION
Dentoalveolar trauma is defined as trauma in which there is injury to the teeth or supporting tissues, where the structural integrity of the teeth may or may not be affected, and the teeth may be partially or totally displaced from their usual position. Establishing the incidence and prevalence rates of dental trauma is challenging due to disparities between studies in the terminology used to define the trauma, the population under study, the age, and the geographical area4. Nevertheless, we know that the incidence of dental trauma is extremely high, and that it particularly affects children.
It is estimated that about one third of children suffer injuries to their primary dentition by five years of age, and that up to one fourth has sustained some sort of injury to the permanent dentition by 12 years of age5. When it came to distribution by sex, our series was in agreement with what has been previously described6,7, with a clear dominance of the male sex, which accounted for 63% of our patients. The male to female ratio has been estimated at around 2:1 in several studies8,9, although some authors note that this proportion more or less holds in trauma to the permanent dentition, while the distribution is similar in both sexes in trauma affecting the primary dentition10,11.
The distribution had two peaks of maximum incidence, probably related to the activity and characteristics of children at those ages. The first peak coincides with learning to walk, with the highest frequencies around 10-24 months of age, and the second corresponds to school ages, reaching the highest frequencies at ages between 9 and 11 years12,13.
The tooth affected most frequently in our series was the maxillary central incisor, followed by the maxillary lateral incisor and the mandibular central incisor. Previous reviews speak of similar results7-14, with the prominence of the incisors and the inability of the upper lip to protect them acting as important predisposing factors7-15.
Following the studies of Andreasen, and on the basis of the system used by the World Health Organization16, dentoalveolar trauma is classified into injuries affecting the tooth bone and the pulp, which include crown and root fractures, and injuries to the periodontium. Depending on degree of severity, trauma to periodontal tissues is classified into concussion (where there is no tooth mobility or displacement), subluxation (abnormal mobility without displacement), intrusion (displacement of the tooth into the alveolar socket bone, with fracture of the latter), extrusion (partial displacement of the tooth out of its socket), and avulsion (the tooth is completely displaced out of the socket). The most frequent trauma in primary dentition are subluxations and luxations, due to the greater resistance of alveolar bone at this age, and to the elasticity of the periodontal ligament17, among other factors. Crown fractures and avulsions occur more frequently in permanent teeth. The most frequent type of injury found in our sample was subluxation, followed by intrusion and crown fracture (Fig. 1).
As for the aetiology, accidental falls and collisions were the most frequent causes, accounting for 84.2% of cases in our sample. They were followed by sports accidents, especially in older boys, and traffic accidents, which are not referred to our hospital.
Dental trauma is also a red flag for child abuse, as it occurs in up to 50% of these cases18, so the paediatrician should be very alert, especially if the child presents with associated injuries, such as maxillary or mandibular fracture, facial burns, laceration of the lips or the lingual frenulum, or bite marks in the face or neck19. We did not suspect abuse in any of our patients. In three patients, the identified cause was aggression between children of the same age, for which we issued the corresponding injury report.
From the time the new protocol was implemented, dental trauma cases in our centre are always seen first by the paediatrician20. We get a large number of patients seeking treatment for these injuries, as this is one of three hospitals in Madrid that has an on-call maxillofacial surgery specialist, and it is the reference hospital for this pathology in the southeast area of Madrid. In addition to children from our healthcare area, who come of their own accord or are referred from Primary Care, the paediatric emergency department in our hospital sees children that come from healthcare areas corresponding to these other hospitals. Parents and patients often come full of anxiety and expect to be treated by a specialist, when in many cases the treatment falls into the scope of a paediatric dentist, disappointing the family’s expectations.
In 2009 a protocol validated by the Paediatrics and Maxillofacial Surgery departments, and coordinated by the Quality Unit, was implemented. Since then, injuries are managed more quickly and uniformly, and also more safely for the child, independent of the particular experience of the treating professional (Fig. 2). The implementation of the protocol has also affected the number of referrals, which used to account for 39.6% of treated patients, and went down to 23% after its establishment and promotion.
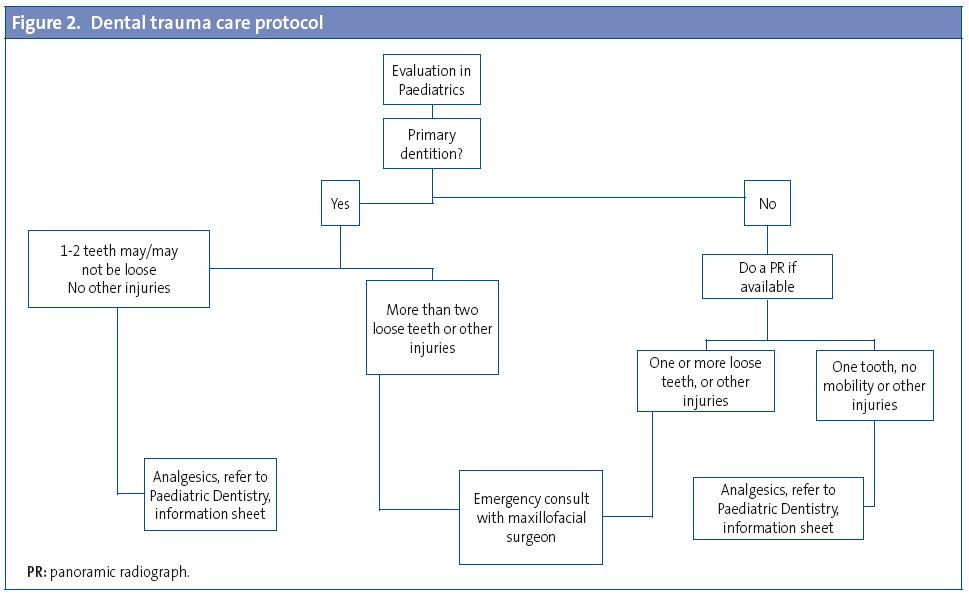
According to the action plan specified by the protocol, which has been applied in full for the past 12 months, patients with injuries in the primary teeth are assessed by the paediatrician in the emergency department, and always referred to the healthcare area paediatric dentist for evaluation within 24-48 hours. If more than two teeth are injured or displaced, or there are other wounds in the mouth, the child is treated in the paediatric emergency care department by the on-call maxillofacial surgeon, as happened in 40% of the cases in our series. In case of hard tissue or pulp injuries, a conservative treatment involving analgesics and a soft diet should be applied. Antibiotic prophylaxis is recommended when the pulp or tooth edges are damaged. Primary tooth concussions, luxations, and subluxations should also receive conservative treatment. In case of avulsion, the deciduous tooth should not be replanted, as this may affect the permanent successor teeth.
In case of injury in the permanent dentition, a panoramic radiograph or radiograph of the skull should be done, whenever possible, to be sent to the paediatric dentist. It is also recommended that the patient is put on a soft diet and given pain relief, with or without antibiotic therapy depending on the type of trauma. Whenever there is mobility in the teeth, even if it is in a single tooth, or other parts of the mouth are injured, the patient should be evaluated by the maxillofacial surgeon. While concussions and subluxations are managed in the same manner as they are in primary teeth, intrusive, extrusive, and lateral luxations require reduction and splinting. The most severe injury found in this group was undoubtedly avulsion of a permanent tooth. Its prognosis depends on the measures taken at the accident site, which are often insufficient21, and on receiving early and adequate treatment. The moment the injury occurs, the tooth should be held by the crown to avoid damage to the ligament and washed with saline solution or running water. Once rinsed, without brushing or drying it, we recommend inserting the tooth in the alveolar bone holding it by the crown, and for the patient to bite on gauze once the tooth has been placed. If this cannot be done, the tooth should be kept in milk or saline solution, or else carried in the patient’s mouth until it can be replanted. It is advisable that the tooth be replanted within one hour, so this type of injury constitutes a real emergency22.
Conclusion
Dental trauma is a frequent reason for seeking emergency care and for referral to reference hospitals. Most patients present with minor injuries that do not require the performance of supplemental tests nor require surgical treatment or transfer to other hospitals, and could be evaluated and treated by their paediatrician. We think that it is convenient to be acquainted with a protocol such as the one used in Hospital 12 de Octubre, designed by paediatricians and paediatric maxillofacial surgery specialists, to facilitate the standardised and safe management of these patients, and referral to the maxillofacial surgery specialists of patients who truly need it.
CONFLICT OF INTERESTS
The authors declare having no conflict of interests in relation to the preparation and publication of this paper.
BIBLIOGRAPHY
- Robertson A, Norén JG. Subjective aspects of patients with traumatized teeth. A 15-year follow-up study. Acta Odontol Scand. 1997;55:142-7.
- Cortes MI, Marcenes W, Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent Oral Epidemiol. 2002;30:193-8.
- Romance García AI, Álvarez Díaz AJ, Marín Ferrer M. Trauma dental. En: Marín Ferrer M, Ordóñez Sáez O, Palacios Cuesta A (ed.). Manual de Urgencias de Pediatría. Hospital 12 de Octubre. Madrid: Ergon; 2011. p. 202-6.
- García C, Pérez L, Castejón I. Prevalencia y etiología de los traumatismos dentales. Una revisión. RCOE. 2003;8:131-41.
- Andreasen JO, Andreasen FM. Classification, etiology and epidemiology of traumatic dental injuries. En: Andreasen JO, Andreasen FM (eds.). Textbook and color atlas of traumatic injuries to the teeth, 3rd ed. Copenhagen: Munksgaard; 1994. p. 151-77.
- Guedes OA, de Alencar AH, Lopes LG, Pécora JD, Estrela C. A retrospective study of traumatic dental injuries in a Brazilian dental urgency service. Braz Dent J. 2010;2:153-7.
- Livny A, Sgan-Cohen HD, Junadi S, Marcenes W. Traumatic dental injuries and related factors among sixth grade schoolchildren in four Palestinian towns. Dent Traumatol. 2010;26:422-6.
- Thelen DS, Bårdsen A. Traumatic dental injuries in an urban adolescent population in Tirana, Albania. Dent Traumatol. 2010;26:376-82.
- Forsberg CM, Tedestam G. Traumatic injuries to teeth in Swedish children living in an urban area. Swed Dent J. 1990;14:115-22.
- Andreasen JO, Ravn JJ. Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population. Int J Oral Surg. 1972;1:235-9.
- Coutinho TC, Cajazeira MR. Retrospective study on the occurrence of primary incisor trauma in preschool children of a low-income area in Brazil. Eur J Paediatr Dent. 2011;12:159-62.
- Andreasen JO, Andreasen FM. Textbook and color atlas of traumatic injuries to the teeth, 3rd ed. Copenhagen: Munksgaard; 1994.
- Celenk S, Sezgin B, Ayna B, Atakul F. Causes of dental fractures in the early permanent dentition: a retrospective study. J Endod. 2002;28:208-10.
- Kovacs M, Pacurar M, Petcu B, Bukhari C. Prevalence of traumatic dental injuries in children who attended two dental clinics in Targu Mures between 2003 and 2011. Oral Health Dent Manag. 2012;11:116-24.
- Tümen EC, Adigüzel O, Kaya S, Uysal E, Yavuz I, Ozdemir E, et al. Incisor trauma in a Turkish preschool population: prevalence and socio-economic risk factors. Community Dent Health. 2011;28:308-12.
- García-Godoy F. A classification for traumatic injuries to primary and permanent teeth. J Pedod. 1981;5:295-7.
- Fried I, Erickson P, Schwartz S, Keenan K. Subluxation injuries of maxillary primary anterior teeth: epidemiology and prognosis of 207 traumatized teeth. Pediatr Dent. 1996;18:145-51.
- Becker DB, Needleman HL, Kotelchuck M. Child abuse and dentistry: orofacial trauma and its recognition by dentists. J Am Dent Assoc. 1978;97:24-8.
- Jessee SA. Orofacial manifestations of child abuse and neglect. Am Fam Physician. 1995;52:1829-34.
- Romance García AI, Pérez Díaz AJ, Marín Ferrer M. Traumatismo dental. En: Marín Ferrer M, Ordóñez Sáez O, Palacios Cuesta A. Manual de Urgencias de Pediatría. Hospital 12 de Octubre. Madrid: Ergon; 2011. p. 202-7.
- Young C, Wong KY, Cheung LK. Emergency management of dental trauma: knowledge of Hong Kong primary and secondary school teachers. Hong Kong Med J. 2012;18:362-70.
- Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F, et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol. 2007;23:130-6.