
Vol. 14 - Num. 54
Original Papers
Care of infants born in 2009 and their mothers in an urban healthcare centre of Zaragoza. Opportunities for improvement
José Galbe Sánchez-Venturaa, Lorena Gracia Torralbab, J Metola Lozac, Ana M.ª Mateo Ferrandod, M Sánchez Ercee, P Traver Cabreraf
aPediatra. CS Torrero La Paz. Zaragoza. España.
bPediatra. CS Torre Ramona. Zaragoza. España.
cMatrona. Zaragoza. España.
dPediatra. CS Canal Imperial. Zaragoza. España.
eMIR-Pediatría. Hospital Miguel Servet. Zaragoza. España.
fPediatra. CS Sector II. Zaragoza. España.
Correspondence: J Galbe. E-mail: galbester@gmail.com
Reference of this article: Galbe Sánchez-Ventura J, Gracia Torralba L, Metola Loza J, Mateo Ferrando AM, Sánchez Erce M, Traver Cabrera P. Care of infants born in 2009 and their mothers in an urban healthcare centre of Zaragoza. Opportunities for improvement. Rev Pediatr Aten Primaria. 2012;14:101-6.
Published in Internet: 05-07-2012 - Visits: 20415
Abstract
Introduction: in the past few years, the composition and origin of the population served by the Torrero La Paz Healthcare Centre (HCC) in Zaragoza has changed considerably. This project intends to analyse the demographic and healthcare data for newborns and their mothers corresponding to the health district of Torrero La Paz throughout 2009. The authors are particularly interested in analysing the breastfeeding (BF) prevalence rates and their evolution through time, as well as their relationship with other variables. Another objective is to identify opportunities for improvement following the data analysis, and to propose fitting corrective measures. Finally, if possible, we wanted to establish an easily measurable criterion that could serve as an indicator of the quality of the provided care.
Materials and methods: we analysed the data corresponding to the care received by the 105 infants born throughout 2009 and their mothers in a HCC of the city of Zaragoza (Spain). We studied the rates of BF. We identified opportunities for improvement and proposed corrective measures to address them.
Results: the first visit of the newborn to the HCC took place at an average of ten days of age. The rate of exclusive or mixed BF when the babies were discharged was of 85%, and it was 51.9% at six months of age. For this population we observed a caesarean birth rate of 19.65%, and the percentage of mothers that smoked during the pregnancy was 20.95%. Younger mothers and mothers from developing countries tend to have higher rates of BF. The BF rates of children with the lowest birth weights and lowest gestational age were comparatively lower.
Conclusions: we propose corrective measures that would fit in the context of what we call “child-friendly HCC” measures.
Keywords
● Breastfeeding ● Primary careINTRODUCTION
In the past few years, the composition and origin of the population served by the Torrero La Paz Healthcare Centre (HCC) of Zaragoza have changed considerably. These shifts have happened quickly, and have involved changes in the origins of newborns (NB) and their mothers, too, along with the prevalence of health habits that differ from those of the population served only a few years ago. All of this requires that Primary Care (PC) teams adapt to the changing reality of the community that they care for. One of the objectives of this work is to become acquainted with the socio-medical reality of the NB in our healthcare district, as well as that of their mothers and family at large, analysing the presence of potential risk factors. On the other hand, this population is the target of specific preventative and health-promoting programmes, and it is important that we identify areas that could be improved so the appropriate corrective measures can be implemented. This project takes advantage of the development of a multi-centre collaborative study at the autonomous community level, and with broad participation of healthcare professionals and centres throughout Aragón called “Growth and diet during infancy and early childhood in children from Aragón” (CALINA; Project FIS PI080559 2009-2011). The Torrero La Paz HCC of Zaragoza participates in this project, which is referred to as “CALINA”. The parents of every NB were asked to sign an informed consent form. The CALINA project has been approved, as required, by the Committee for Ethics and Research of Aragón (CEICA). We will analyse only the data corresponding to the Torrero La Paz HCC.
The objectives established for this study are: a) analysing the demographic and healthcare data of NBs and their mothers corresponding to the Torrero La Paz healthcare district throughout 2009 (within this data, it is of particular interest to analyse the breastfeeding [BF] prevalence rates as well as their evolution across time and their relationship to other variables); b) analysing the opportunities for improvement that are identified through the analysis of these data; c) proposing appropriate corrective measures, and d) defining, if possible, some easily measurable quality criterion that could serve as an indicator of the quality of the provided care.
MATERIAL AND METHODS
Study design type: descriptive study. Sample: cohort of NBs in the district, born between February 2009 and February 2010. Setting: PC, urban HCC in the city of Zaragoza.
The data were obtained by means of a survey addressed to the parents that included questions about the health of the parents, their employment status, their country of origin, ethnicity, dietary habits following discharge from the hospital, date of discharge, date of first visit at the HCC, smoking habits of the mother, gestational age, Apgar test, prenatal and perinatal health problems, gestational weight gain, as well as the basic anthropometric data at birth. These data were obtained from the implementation of the CALINA Project, in which the Torrero La Paz HCC participates.
At the time of this study, the BF prevalence data for 2, 4, and 6 months of age were not part of the data collected by the CALINA study protocol, so we gathered these data directly from the electronic medical histories (OMI®) of each of the children.
RESULTS
In the period ranging from February 2009 to February 2010, 105 NB and their mothers were included in the CALINA study. 235 NB were born in the Torrero La Paz health district in 2009, and 258 in 2008. The distribution by sex was 49.53% female and 50.47% male.
The age at discharge was 3.29 days (standard deviation [SD]: 2.06; range: 2-13 days). The age at the first post-natal visit, excluding neonatal hospital admissions, was 10.35 days (SD: 6.28; range: 4-56 days).
The place of birth corresponded to the Hospital Miguel Servet (reference centre) in 92.45% of the births, 3.77% to the Hospital Clínico Universitario, and the rest was divided among the various private clinics of the city of Zaragoza. As for the ethnicity of the NB, 73% were Caucasian, with the rest belonging to other ethnicities. When it came to gestational management, 98.13% of mothers reported that it had been appropriate. There was a 19.63% caesarean birth rate. 8.41% of the NB were delivered by forceps, and 71.96% of the deliveries were normal.
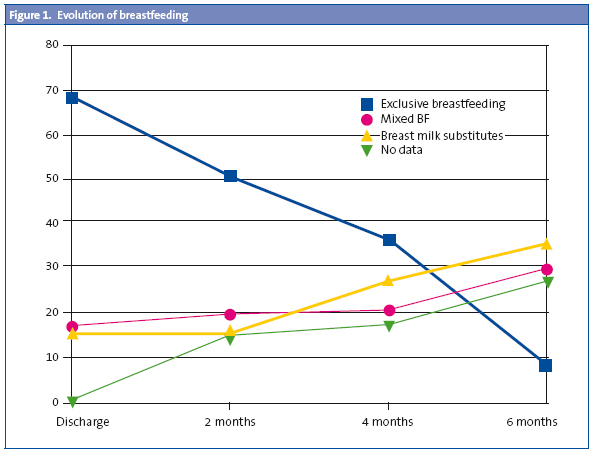
The data pertaining to diet, as well as the evolution of the rates of exclusive BF, mixed BF or breast milk substitute feeding, respectively, are those shown in Fig 1.
Out of the admissions to the neonatal ward, 12.04% were due to a variety of reasons, 34.91% were due to gestational problems and 17.92% to perinatal problems. The average gestational age at birth was 38.75 weeks (SD: 1.85; range: 29-41weeks). 18% of the NB were born before the 37th week of gestation, and 6.6% weighed less than 2500 g at birth. The average score for the Apgar test done at five minutes after birth was 9.66 (SD: 0.82; range: 5-10). Multiple pregnancies represented 7.55% of the total. The average age of mothers was 31.95 years (SD: 5.3; range: 19-46 years). 20.95% of the mothers smoked during the pregnancy.
When it comes to the origin of the mothers, 28.97% came from developing countries; in the case of fathers, this percentage was 24.3%. 69.05% of the mothers reported working outside the home.
Hypothesis testing
The weight of babies born to mothers from developing countries was higher than that of NB of mothers from developed countries (t = –3.03; p = 0.003). The same was seen in weight in relation to the father’s origin (t = –2.84; p = 0.054).
The weights of NB of smoking mothers was slightly lower, but the differences were not statistically significant (t = 1.49; p = 0.138).
There were no significant differences in the Apgar test scores between mothers who smoked and mothers who did not (t = 0.70; p = 0.40).
The birth weight of NB who were breastfed exclusively or in combination with other food had been higher than that of NB who were fed with breast milk substitutes: 3.2 kg in contrast to 2.92 (t = –2.56; p = 0.01). Likewise, children who were BF exclusively or in combination with other food have reached a higher average gestational age: 39.1 weeks in contrast to 37.6 (t = 2.85; p = 0.0052). The youngest mothers were the ones who most frequently breastfed their NB exclusively or in combination with other foods: 31.28 years old in contrast to 35.5 (t = 2.86; p = 0.0053). This effect was maintained when the target population consisted exclusively of Caucasian mothers. The average age of mothers that engaged in exclusive or mixed BF was 30 years, as opposed to the 35.7 year olds who provided breast milk substitutes (t = –2.37; p = 0.02). Mothers that were from poor or developing countries breastfed their NB exclusively or in combination with other food with greater frequency than mothers from developed countries (χ2 = 5.88; p = 0.0153). The same happened in relation to the country of origin of the father (χ2 = 4.21; p = 0.04).
There were no significant differences in the weight of the NB in relation to the mother’s occupation, whether she stayed home or worked outside the house (t = 0.31; p = 0.75), nor in relation to the type of occupation and the Apgar test score at five minutes after birth (t = –0,66; p = 0,51). The relationship between the Apgar test at five minutes after birth and the mother’s origins (t = 2.15; p = 0.003) showed significant differences between groups, but this did not occur in relation to the origin of the father.
Mothers who had past histories of disease showed lower rates of exclusive or mixed BF (χ2 = 9.66; p < 0.0019). The study did not show significant differences in NB birth weights as a function of the mother’s occupation outside the home.
The mean body mass index (BMI) of our sample was 23.98 kg/m2 (SD: 4.45; interval of confidence 95% [IC 95%]: 23.11-24.85; range: 15.62-38.29). The BMI was not correlated to the type of BF at any age, but it was significantly higher in mothers with a history of disease (t = –2.79; p = 0.0063). The BMI was also correlated to perinatal problems, which were more frequent the higher the BMI.
There were no significant differences in the initial BF rates and the rates at 2, 4, and 6 months and the type of delivery (normal or caesarean).
DISCUSSION
From our data analysis, we can conclude that:
- For this cohort of NB, the first visit to the HCC took place after 10 days of life.
- There is a considerable percentage, about 25%, of babies born to mothers and fathers of different ethnicities and from developing countries.
- The latter NB tend to show greater birth weights, but do not differ comparatively in the remaining variables analysed in relation to Spanish Caucasian children.
- Children with lower birth weights and gestational ages, and those whose mothers were older, seem to have a lower prevalence of exclusive and mixed BF.
- Children whose fathers or mothers come from developing countries and those whose mothers have no history of medical conditions have higher breastfeeding rates.
- There is a considerable percentage of mothers who smoke, around 20%.
- Mothers with higher BMI have a higher incidence of perinatal pathological histories, as well as of gestational health problems.
From the data presented we can deduce interesting aspects of how children born in our healthcare district are raised. A first aspect involves BF rates, which could still improve, but are nevertheless above the published BF rates for our autonomous community1.
We also think that the caesarean delivery rate is worth noting, reaching 19.63% in our cohort. It is known that a higher caesarean delivery rate is associated with lower BF rates2,3, so it would be desirable to lower the number of these deliveries to the absolute minimum necessary. The WHO has set the optimal caesarean section rate at 15%, and the same guideline is included in the document for the “Normal delivery care in the National Health System”4.
In our cohort, the first visit to the HCC took place somewhat late, and we think that this visit should not be delayed beyond 7 days from birth. Still, we think that the ideal time for the first visit would be at 48 hours post-birth, especially if there are any risk factors. Early neonatal visits are associated with better BF rates and better outcomes in children with hypernatremic dehydration resulting from lactation failure5.
Our data reflect a significant percentage of foreign natives in our health district. After analysing the data, we observed that the BF rates in the younger immigrant mothers were higher than those among the Spanish participants, and that the size and weight of their NB were also higher, with no other differences recorded in relation to national participants.
We found a percentage of 20% of mothers who smoked in our cohort. The side effects of tobacco on the health of mothers and their newborns are well known6,7 and we must make every possible effort from PC to lower this percentage. The efficacy of brief smoking cessation counselling in PC has been demonstrated.
The BMI of mothers is statistically correlated to gestational health problems, diabetes, etc, but this is not the case with BF rates.
It is important that we also mention the lower BF rates for lower birth weights and gestational ages, even though there were not many pre-term babies in our cohort. It is known that these children have higher morbidity and mortality rates, and that the benefits of BF are even greater for them, which is why extra efforts should be made to ensure higher BF rates in these children8,9.
Opportunities for improvement
- Providing information about BF to mothers and families, and to women planning on becoming pregnant, during any kind of PC visit. The aim of providing this information is to help make an informed decision unbiased by marketing pressures.
- To promote exclusive BF in the first six months of life, and BF until two years of age after the correct introduction of complementary feeding starting at six months.
- Promoting BF by taking advantage of PC visits and of childbirth education. We propose the establishment of a BF support group as a proven efficacious means to promote BF.
- Having a clear strategy to train the centre’s staff about BF.
- Having a written document with updated information about lactation and nutrition available to the entire staff of the centre. Promoting awareness and use of this document by the entire staff of the HCC.
- Scheduling the first appointment for the NB at the HCC for a time within the first 72 hours after discharge from the maternity ward, regardless of any pending bureaucratic transactions.
- Strictly adhering to the normative regarding the advertisement of breastmilk substitutes.
- Promoting the use of simultaneous BF during painful procedures such as heel puncture, ear piercings, etc.
- Promoting the use of the World Health Organization growth charts to monitor babies in general and breastfed babies in particular.
- Promoting the use of online electronic resources to get information about medications and BF (for example, www.e-lactancia.org/).
- Taking advantage of PC visits and childbirth education to evaluate tobacco use and advise against it throughout the pregnancy.
- Referral to mother’s PC physician or nurse to start smoking cessation programme whenever it is considered indicated.
- Advising the mother on healthy dietary habits throughout the entire process: pregnancy, peripartum and lactation.
- Proposed quality indicators: a) age of the NB at the first PC visit; b) percentage of NB with exclusive BF at the first PC visit; c) percentage of NB with mixed BF at the first PC visit; d) percentage of children with exclusive BF at 2, 4, and 6 months of age; e) percentage of mothers that smoke at the first PC visit, and f) percentage of mothers that attend or have attended a BF support group linked to the PC team during the first month of life of a NB (to be recorded during the first-month visit).
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interest in regard to the preparation and publication of this paper.
ACRONYMS: PC: Primary Care • CALINA: Growth and Diet during the infancy and early childhood of children in Aragón • CEICA: Ethics and Research Committee of Aragón • HCC: healthcare centre • SD: standard deviation • CI 95%: 95% confidence interval• BMI: body mass index • BF: breastfeeding • NB: newborn.
BIBLIOGRAPHY
- Grupo de Trabajo CS-IHAN, Hernández Aguilar MT, González Lombide E, Bustinduy Bascarán A, Arana Argüelles-Cañedo C, Martínez-Herrera Merino B, et al. Centros de Salud IHAN (Iniciativa de Humanización de la Atención al Nacimiento y la Lactancia). Una garantía de calidad. Rev Pediatr Aten Primaria. 2009;11:513-29.
- Montañés Cuestas A, Aparicio Sánchez JL. Los niños nacidos por cesárea toman menos lactancia materna. Evid Pediatr. 2011;7:15.
- Aguayo Maldonado J, Romero Escós D, Hernández Aguilar MT; Comité de Lactancia Materna de la AEP. Influencia de la Atención al parto y al nacimiento sobre la lactancia, con especial atención a las cesáreas. Evid Pediatr. 2011;7:2.
- Observatorio de la Salud de la Mujer y del Sistema Nacional de Salud y Dirección General de la Agencia de Calidad del Sistema Nacional de Salud. Estrategia de Atención al Parto Normal. Madrid: Ministerio de Sanidad y Consumo; 2007.
- Grupo NIDCAP y Grupo Previnfad. Cuidados desde el Nacimiento. Recomendaciones basadas en pruebas y en buenas prácticas. Madrid: Ministerio de Sanidad y Política Social; 2010.
- Lumley J, Chamberlain C, Dowswell T, Oliver S, Oakley L, Watson L. Interventions for promoting smoking cessation during pregnancy. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD001055. DOI: 10.1002/14651858.CD001055.pub3.
- Galbe Sánchez-Ventura J, Córdoba García R, García Sánchez N. Prevención del tabaquismo activo y pasivo en la infancia. Rev Pediatr Aten Primaria. 2009;11 (Supl 17):s359-s369.
- Pallás Alonso C; Grupo Previnfad. Promoción de la lactancia materna. En: Recomendaciones PrevInfad/PAPPS [en línea] [actualizado marzo de 2010] [consultado el 28/07/2011]. Disponible en www.aepap.org/previnfad/Lactancia.htm
- Pallás Alonso C. Programa de Actividades Preventivas y de Promoción de la Salud para niños prematuros con una edad gestacional menor de 32 semanas o un peso inferior a 1500 gramos. Del alta hospitalaria a los 7 años. En: Recomendaciones PrevInfad/PAPPS [en línea] [actualizado marzo de 2010] [consultado el 28/07/2011]. Disponible en www.aepap.org/previnfad/menor32-1500.htm