
Vol. 26 - Num. 103
Originales
Perfil del paciente con claudicación de la marcha
Verónica Gimeno-Hernández Garzaa, Álvaro García Atarésb, Marisol Camacho Lovilloc
aServicio de Pediatría. Hospital Ernest Lluch. Calatayud. Zaragoza. España
bPediatra. CS de Caspe. Zaragoza. España
cServicio de Pediatría. Hospital Virgen del Rocío. Sevilla. España.
Correspondencia: V Gimeno-Hernández . Correo electrónico: vgimenohernan@salud.aragon.es
Cómo citar este artículo: Gimeno-Hernández Garza V, García Atarés A, Camacho Lovillo M. Perfil del paciente con claudicación de la marcha. Rev Pediatr Aten Primaria. 2024;26:255-62. https://doi.org/10.60147/194309a5
Publicado en Internet: 16-09-2024 - Número de visitas: 11065
Resumen
Introducción: la cojera es un motivo de consulta frecuente en Atención Primaria y urgencias.
Material y métodos: estudio observacional, longitudinal, retrospectivo en pacientes que consultan por cojera en urgencias de un hospital terciario entre 2019-2022. Muestreo aleatorio sistematizado. Variables analizadas: edad, sexo, tiempo de evolución, síntomas, traumatismo previo, antecedentes, derivación o no, hallazgos en exploración, pruebas complementarias, tratamiento, diagnóstico en urgencias, diagnóstico final, grupo etiológico y destino.
Resultados: 321 pacientes, 65,1% varones, edad media 5,5 ± 3,4 años. El 60% consultaban con evolución inferior a 24 horas y el 81,6% sin derivación. Se solicitaron pruebas complementarias en un 87,5% (55,7% radiografía). La etiología más común fue inflamatoria 29% (sinovitis transitoria de cadera 24%). En un 2,49% hubo un diagnóstico final diferente al de urgencias, siendo el más frecuente la artritis idiopática juvenil (AIJ). Hubo asociación entre paciente derivado y triaje de mayor prioridad (p = 0,03), realización de ecografía (p = 0,009) y derivación a consultas(p = 0,003). La media de edad de los pacientes con ecografía patológica (5,65 años) fue superior a la de los de resultado normal (3,84 años). Hubo diferencias de medias en las edades de los grupos etiológicos (p = 0,000) y en los diferentes diagnósticos en urgencias (p = 0,002). Se encontró asociación entre síntomas previos y grupo etiológico (p = 0,000), tiempo de evolución y grupo etiológico (p = 0,002) e interconsulta a traumatología (p = 0,000) y destino final (p = 0,000).
Conclusiones: entre las causas de cojera, generalmente banales, es importante una alta sospecha clínica para el diagnóstico de otras menos comunes y con mayores implicaciones como la AIJ.
Palabras clave
● Cojera ● MarchaINTRODUCCIÓN
La cojera es una alteración del patrón de marcha normal de un niño que implica deambulación dificultosa, errática o desigual, de aparición aguda o subaguda debida al dolor, debilidad muscular o deformidad del esqueleto.
Debe diferenciarse de otras variantes fisiológicas de la marcha (genu varo o valgo, pie plano, metatarso aducto o marcha idiopática de puntillas). Cuando el niño es pequeño, puede presentarse en forma de rechazo al apoyo del miembro afecto. En función de la presencia o no de dolor puede clasificarse como antiálgica o no antiálgica.
Supone una de las causas más frecuentes de consulta en Atención Primaria y urgencias pediátricas, con una incidencia descrita de 1,8 casos por 1000 menores de 14 años, excluyendo las de causa traumática1. Por dicho motivo, la claudicación de la marcha precisa un abordaje ágil que logre el despistaje de causas que precisen un tratamiento urgente y aquellas potencialmente graves, y un seguimiento estrecho hasta su resolución2. El diagnóstico diferencial puede realizarse con una anamnesis y exploración física exhaustivas, constituyendo ambas el primer paso y el más importante en el proceso diagnóstico.
En la anamnesis debemos recabar información sobre:
- Edad y sexo.
- Inicio, tiempo de evolución y características de la cojera.
- Presencia o no de dolor, así como localización, ritmo mecánico (empeora con la actividad) o inflamatorio (empeora con el reposo) o mixto, factores que lo mejoran o empeoran, repercusión en la vida diaria o si interrumpe el sueño.
- Antecedente traumático: una caída puede deberse a la existencia previa de dolor y no ser necesariamente su causa. Hasta uno de cada tres pacientes con cojera asociada a infección osteoarticular presenta un antecedente traumático; por ello la historia de trauma debe valorarse cuidadosamente, sobre todo en menores de 3 años.
- Presencia o no de sintomatología acompañante: afectación del estado general, febrícula o fiebre en los días previos o en el momento de la consulta, infección respiratoria, lesiones cutáneas, presencia de vómitos, diarrea o estreñimiento, antecedentes personales (vacunación, infecciones, traumatismos…) y familiares (patología reumática/autoinmune, familiares con dolor agudo o crónico, problemas psicosociales, etc.)
Respecto a la exploración física, llevaremos a cabo una valoración del estado general del paciente, del aparato locomotor y de la marcha. Asimismo, deberíamos completar una exploración por aparatos, ya que la cojera puede ser un síntoma de una enfermedad sistémica prestando atención a la búsqueda de lesiones cutáneas, signos abdominales o afectación neurológica. En ocasiones esta exploración resulta dificultosa por la ausencia de colaboración del paciente, especialmente en los de menor edad, debiendo dedicar mayor tiempo para llevarla a cabo.
En algunos casos la información recabada de la anamnesis y exploración física no será suficiente para alcanzar un diagnóstico de sospecha definitivo y, en función de la situación clínica del paciente, del tiempo de evolución y de las posibilidades diagnósticas planteadas deberemos llevar a cabo pruebas de laboratorio3 (esencialmente reactantes de fase aguda como: proteína C reactiva (PCR), procalcitonina (PCT), velocidad de sedimentación globular (VSG), hemograma y creatinkinasa (CK) en caso de sospecha de miositis aguda) y/o pruebas de imagen (radiografía, ecografía, gammagrafía ósea con tecnecio o resonancia magnética nuclear)4.
Si clasificamos la claudicación de la marcha en función de la sospecha etiológica, los principales grupos son:
- Traumática, como fracturas de primeros pasos, esguinces, fracturas de estrés en deportistas, etc.
- Inflamatoria o inmunológica, como algunas artritis, la sinovitis transitoria de cadera (STC) y la miositis aguda benigna.
- Infecciosa, como artritis, osteomielitis y discitis. Pueden asociar febrícula/fiebre y/o afectación del estado general y/o elevación de reactantes de fase aguda (PCR y VSG).
- Otras causas osteoarticulares, como osteocondritis/osteocondrosis, Perthes, epifisiolisis de cabeza femoral, displasia evolutiva de cadera no diagnosticada en periodo neonatal.
- Neuromusculares, como una parálisis cerebral infantil leve que haya pasado desapercibida los primeros meses de vida.
- Oncohematológicas: la presencia de síntomas sistémicos como astenia, irritabilidad no justificada, anorexia, perdida ponderal, palidez, fiebre de origen desconocido… deben alertarnos ante una posible causa tumoral5.
- Causas facticias y simulación.
Podemos comprobar entonces que el abanico de posibilidades diagnósticas ante un paciente pediátrico con cojera es amplio, a lo que se suman las dificultades para llevar a cabo una exploración del aparato locomotor en niños no colaboradores. Todo ello conduce a que la cojera pueda suponer un reto para el profesional que atiende dicho motivo de consulta y a un posible infradiagnóstico inicial de entidades menos frecuentes como las reumatológicas. Su conocimiento y su sospecha precoz desde los servicios de Atención Primaria y urgencias permitiría una derivación adecuada, que evite retrasos diagnósticos y, consecuentemente, secuelas potencialmente graves6-8.
Hipótesis: en Pediatría existe un bajo índice de sospecha de la patología reumática como causa de cojera, especialmente en una primera asistencia, lo que conduce a un retraso diagnóstico en comparación con el resto de los grupos etiológicos.
El objetivo principal del presente estudio es realizar un análisis de los pacientes que acuden a urgencias pediátricas de un hospital terciario con cojera o claudicación de la marcha.
Los objetivos secundarios son:
- Describir las características de estos pacientes.
- Evaluar el perfil etiológico de dichos pacientes agrupados en causa traumática, inflamatoria, infecciosa, otras causas osteoarticulares, neuromuscular, oncohematológica, facticia o simulación.
- Analizar la presencia de qué síntomas y signos se asocian con cada uno de los perfiles etiológicos descritos.
- Analizar las pruebas complementarias que se les solicitan desde el servicio de urgencias.
- Conocer el diagnostico final de dichos pacientes.
- Comparar si el diagnóstico final concuerda con el diagnóstico de sospecha emitido en el servicio de urgencias.
- Conocer el periodo de tiempo que transcurre hasta alcanzar un diagnóstico correcto en este tipo de pacientes y si hay diferencias entre los distintos grupos etiológicos.
MATERIAL Y MÉTODOS
Se diseñó un estudio descriptivo y analítico, observacional y retrospectivo. La población a estudio está compuesta por pacientes que consultaron en urgencias de un hospital de tercer nivel entre el 1 de enero de 2019 y el 31 de diciembre de 2022.
Los criterios de inclusión fueron:
- Pacientes de 0 a 14 años que consultaron en urgencias del Hospital Infantil Miguel Servet con motivo de consulta “cojera o claudicación de la marcha” asignado en triaje.
- Fecha de la consulta en urgencias entre el 1 de enero de 2019 y el 31 de diciembre del 2022.
Por el contrario, los criterios de exclusión fueron:
- Pacientes de 15 años o más que son aceptados en urgencias del Hospital Infantil Miguel Servet por patología crónica/compleja en seguimiento en nuestro centro, ya que es un estudio sobre población pediátrica que en nuestra comunidad autónoma, salvo excepciones, abarca la atención hasta los 14 años y 12 meses.
- Pacientes fugados de urgencias previamente a la atención médica o tras la misma, pero antes de haber sido dados de alta por el personal médico.
- Pacientes que rechazan la realización de las pruebas complementarias indicadas por el personal médico tras su valoración inicial.
Del total de pacientes obtenidos, se seleccionó la muestra a través de un muestreo aleatorio sistematizado, seleccionando uno de cada tres casos.
Las dos variables principales del presente estudio fueron: diagnóstico al alta del servicio de urgencias hospitalarias y grupo etiológico en el que se encuadra dicho diagnóstico.
Las variables secundarias fueron: epidemiológicas (sexo, edad, centro de salud y sector sanitario al que pertenece), fecha de consulta en urgencias, datos de la anamnesis (paciente derivado desde atención primaria u otro centro hospitalario o no, antecedente personal o familiar de patología traumatológica, reumatológica y/o neurológica, antecedente personal de enfermedad crónica de otro tipo, antecedente de traumatismo o vacunación previa sobre dicha extremidad, síntomas acompañantes o previos, patrón de la cojera), de la exploración física (cojera o no en urgencias, tipo de marcha, extremidad y/o articulación afecta, presencia de dolor a la palpación/movilización, generalizado/localizado y donde, presencia de lesiones cutáneas y/o signos inflamatorios locorregionales y presencia o no de focalidad neurológica), de las pruebas complementarias (realización o no de radiografía, ecografía, analítica sanguínea, análisis de líquido articular y resultado normal/dudoso/patológico de las mismas, realización de pruebas en consultas de otro centro o en consultas previas en nuestras urgencias, presencia o ausencia de las mismas y cuáles, así como número total de pruebas complementarias realizadas), del manejo del paciente (control por su pediatra, derivación a consultas externas, control en urgencias en 5 días, ingreso hospitalario, tratamientos previos, tratamiento prescrito y número total de medidas terapéuticas prescritas), y datos relativos al diagnóstico (diagnóstico final del paciente y fecha de diagnóstico final).
El análisis estadístico de los datos se llevó a cabo a través del programa SPSS. Se realizó un estudio estadístico descriptivo de la muestra. Para comprobar la normalidad de cada variable cuantitativa se aplicó el test de Kolmogorov Smirnov o de Shapiro Wilk, en función del número de datos disponibles para cada variable. Para el análisis de la existencia de asociaciones estadísticamente significativas entre grupos en las variables categóricas tabuladas, se utilizó el test de ji-cuadrado. Para determinar asociación entre una variable cualitativa y una cuantitativa se empleó t de Student o análisis de la varianza (ANOVA) en el caso de variables con más de dos categorías. Para determinar la asociación de dos variables cuantitativas, el coeficiente de correlación de Pearson. Se consideraron como resultados estadísticamente significativos los valores de los contrastes con p <0,05.
Este proyecto ha sido aprobado por el Comité de Ética de la Investigación de nuestra comunidad autónoma.
RESULTADOS Y DISCUSIÓN
La cojera supuso el 0,53% de las consultas a urgencias en nuestro centro. En nuestro estudio se analizaron un total de 321 pacientes, siendo un 65,1% varones y la media de edad de 5,53 ± 3,46 años, características epidemiológicas similares a las descritas por otros autores9,10.
En torno a un 80% de los pacientes consultaron sin haber sido derivados y fueron catalogados con un nivel de prioridad 4 en triaje. Asimismo, un 59,92% consultaban en las primeras 24 horas de inicio de la cojera. Todo ello apunta a que, a pesar de que la mayor parte de las causas de cojera son benignas y se resuelven espontáneamente1, este es un motivo de consulta que angustia a los familiares, solicitando con frecuencia asistencia médica precoz y urgente.
Un 22,7% de los pacientes habían presentado cuadro catarral o gastrointestinal previo al inicio de la cojera, un 8,1% lo presentaban en el momento de consulta a urgencias y un 0,6% tenían fiebre aislada coincidiendo con el inicio de la cojera. Se detectó asociación estadísticamente significativa entre la presencia de síntomas previos o concomitantes a la cojera y el grupo etiológico de la misma (p = 0,000), lo que refuerza la importancia de una anamnesis detallada en la evaluación de este tipo de pacientes y del antecedente de proceso viral previo para el diagnóstico de sinovitis transitoria de cadera11. En la anamnesis es fundamental hacer hincapié en la presencia previa o en el momento de la cojera de fiebre-febrícula, astenia, mialgias, pérdida ponderal (que pueden orientar a una etiología reumatológica, infecciosa u oncohematológica), síntomas sugerentes de infección de vía respiratoria o gastrointestinal (más sugestivos de causa inflamatoria tipo STC o artritis reactiva). Asimismo, en la exploración física, además de detectar y describir el tipo de marcha o los signos locales inflamatorios en extremidades inferiores, rango de movilidad articular y dolor, se debería completar con una exploración física por aparatos que descarte megalias, lesiones en la piel o signos inflamatorios en otras articulaciones que puedan ser claves para el diagnóstico. Realizando una anamnesis y exploración física completas sería posible evitar pruebas complementarias innecesarias.
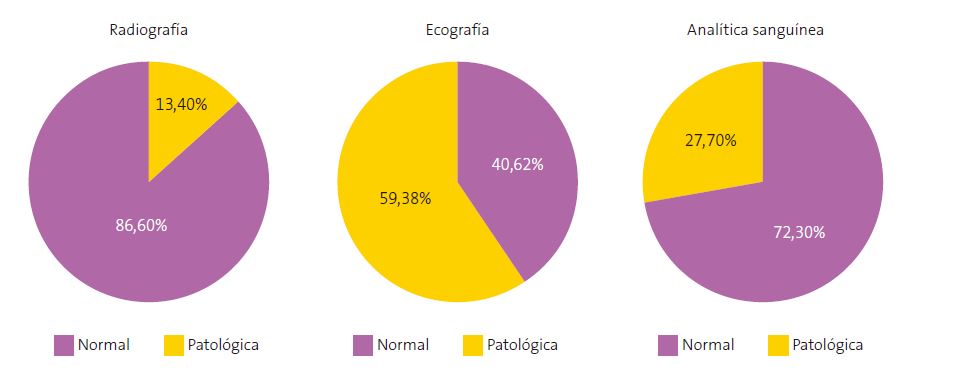
Se solicitaron pruebas complementarias a un elevado porcentaje de pacientes (87,5%), la más frecuente, la radiografía (55,76%), seguida de ecografía (19,93%), analítica sanguínea (11,21%) y artrocentesis (0,62%). La rentabilidad de la radiografía y la analítica (13,4% y 27,7% patológicas, respectivamente) fue menor que la de la ecografía y la artrocentesis (59,38% y 100% patológicas, respectivamente) (Figura 1). El porcentaje de pruebas complementarias solicitadas difiere al encontrado en otros estudios como el de Tu et al.10, en el que describen un 51% de solicitudes de pruebas de imagen en global y un 39% de analíticas sanguíneas; y el de Murias et al.12, con una solicitud de radiografías del 31,13%, de ecografía del 26,88% y de analítica sanguínea del 64%. Si bien estos resultados son difícilmente comparables al tratarse el trabajo de Tu et al.10 de un estudio retrospectivo de urgencias pediátricas en el que excluyen los pacientes con antecedente de traumatismo y el de Murias et al.12 un estudio que incluye a pacientes derivados a consulta de reumatología.
| Figura 1. Resultado normal vs. patológico de las pruebas complementarias solicitadas |
|---|
 |

Se detectó asociación estadísticamente significativa entre paciente derivado o no y la realización de ecografía (p = 0,009), lo que puede responder a una mayor adecuación en su solicitud, así como mayor media de edad en los pacientes con ecografía patológica que la de los pacientes con resultado normal de la misma (5,65 años, frente a 3,84). Esto último podría deberse a que en los niños mayores la ecografía es solicitada con una sospecha clínica más específica de sinovitis/artritis frente a los niños pequeños en los que lo inespecífico de los síntomas y complejidad de la exploración conduce a la solicitud de pruebas complementarias con el objetivo a veces más de descartar patología que de realizar un diagnóstico preciso.
No se encontró asociación entre paciente derivado o no y el número total de pruebas complementarias solicitadas, lo que podría deberse al pequeño porcentaje de pacientes derivados en nuestra muestra y al elevado porcentaje de solicitud de las mismas. Tampoco se detectó asociación entre antecedente traumático previo al inicio de la cojera y resultado patológico de la radiografía, lo que hace que nos planteemos que no es necesaria su solicitud ante traumatismos banales; ni entre antecedente de patología traumática e interconsulta a traumatología, lo que podría explicarse porque dicho antecedente no tenía implicación en el proceso actual (displasia de cadera o fractura previa correctamente tratadas).
Se obtuvo diferencia de medias en las edades de los distintos grupos etiológicos de la cojera, como entre causa inflamatoria y otra causa osteoarticular (p = 0,00) (Tabla 1), datos que concuerdan con la bibliografía, siendo la causa inflamatoria más frecuente en el lactante y niño pequeño, y otras causas osteoarticulares como la osteocondritis, más propias del niño mayor y adolescente13.
| Tabla 1. Diferencias de medias en la edad entre los diferentes grupos etiológicos | ||||
|---|---|---|---|---|
| Grupo etiológico | N | Media | DE | p |
|
Traumática Otra causa osteoarticular |
84 31 |
5,53 8,71 |
3,62 3,34 |
0,000 |
|
Inflamatoria Otra causa osteoarticular |
93 31 |
4,53 8,71 |
2,45 3,34 |
0,000 |
|
No causa encontrada Otra causa osteoarticular |
91 31 |
5,46 8,71 |
3,61 3,34 |
0,000 |
|
N: número de pacientes; DE: desviación estándar. |
||||

La etiología más frecuente de la cojera fue inflamatoria (29%), seguida de traumática (26,25%), otras causas osteoarticulares (9,7%), neuromuscular (2,2%), infecciosa (1,6%) y oncohematológica (0,6%). Hasta en un 28,3% no se encontró la causa de la cojera en su consulta a urgencias. Respecto al diagnóstico al alta, destaca como más frecuente la sinovitis de cadera (24%), seguido de cojera (23,1%), dolor de extremidad (15,3%) y contusión (9,03%). En un 2,49% (8) de los pacientes hubo un diagnóstico final diferente al primer diagnóstico en urgencias, siendo el más frecuente la AIJ. Así, un total de 5 pacientes tuvieron el diagnóstico final de artritis como causa de su cojera. Esto supone una incidencia en nuestra muestra de 0,015 casos por cada paciente que consulta por cojera en nuestro centro. En 2 de ellos (un caso de artritis séptica y otro de artritis reactiva) la sospecha diagnóstica se estableció en el servicio de urgencias, frente a 3 casos de AIJ que fueron diagnosticadas a posteriori en consultas de reumatología, siendo por tanto la sospecha de patología reumática baja en el primer momento de la atención sanitaria.
Entre las posibles líneas de trabajo futuras se encontraría la realización del presente estudio en pacientes que consultan en Atención Primaria y ver si existen diferencias con los resultados obtenidos. Así como su repetición tras una intervención consistente en formar a pediatras de urgencias, Atención Primaria y médicos internos residentes (por ser, generalmente, quienes atienden con mayor frecuencia dicho motivo de consulta en su evaluación inicial) en la exploración del aparato locomotor, comprobando si tras dicha intervención disminuye el número de pruebas complementarias solicitadas al mejorar la orientación diagnóstica inicial.
CONCLUSIONES
La cojera supone el 0,53% de las consultas a urgencias en nuestro centro. La media de edad de los pacientes fue de 5,53 ± 3,46 años. El 81,6% consultaron sin haber sido derivados y casi un 60% con un tiempo de evolución de la cojera inferior a 24 horas. Se solicitaron pruebas complementarias al 87,5% de los pacientes, la más frecuente la radiografía (55,76%), seguida de ecografía (19,93%). El 59,38% de las ecografías solicitadas fueron patológicas.
La etiología más frecuente de la cojera fue inflamatoria (29%) y el diagnóstico más común al alta de urgencias, STC (24%). En un 2,49% de los pacientes hubo un diagnóstico final diferente al primer diagnóstico en urgencias, siendo el más frecuente la AIJ.
Que el paciente fuese derivado se asoció de forma significativa a un nivel de triaje de mayor gravedad, mayor frecuencia de realización de ecografía y de derivación del paciente a consultas externas.
Se detectaron diferencias significativas entre las medias de edad de los distintos grupos etiológicos de la cojera de acorde a lo reportado en la bibliografía, y la media de edad de los pacientes con ecografía patológica fue mayor que la de los pacientes con ecografía normal.
Los pacientes con cojera de etiología inflamatoria son los que presentaban síntomas previos con más frecuencia, especialmente cuadro febril (57,1%), catarral (66,7%) o gastrointestinal previo (81%).
Conocer el perfil de pacientes atendidos por cojera en nuestras urgencias nos ayudará a detectar áreas de mejora.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: concepción y diseño del trabajo, elaboración de la base de datos, realización de análisis estadístico e interpretación del mismo, elaboración del manuscrito, aprobación de la versión final del manuscrito (VGHG, AGA), concepción y diseño del trabajo, revisión crítica del manuscrito con aportaciones intelectualmente relevantes, aprobación de la versión final del manuscrito (MCL).
ABREVIATURAS
AIJ: artritis idiopática juvenil · CK: hemograma y creatinkinasa · PCR: proteína C reactiva · PCT: procalcitonina · STC: sinovitis transitoria de cadera · VSG: velocidad de sedimentación globular.
BIBLIOGRAFÍA
- Fischer SU, Beattie TF. The limping child: epidemiology, assessment and outcome. J Bone Joint Surg Br. 1999;81(6):1029-34. https://doi.org/10.1302/0301-620x.81b6.9607
- Staheli LT. Fundamentals of Pediatric Orthopedics. 4th Ed. Philadelphia: Lippincott Williams and Wilkins; 2006.
- Abbassian A. The limping child: a clinical approach to diagnosis. Br J Hosp Med (Lond). 2007;68(5):246-50. https://doi.org/10.12968/hmed.2007.68.5.23330
- Jain N, Sah M, Chakraverty J, Evans A, Kamath S. Radiological approach to a child with hip pain. Clin Radiol. 2013;68(11):1167-78. https://doi.org/10.1016/j.crad.2013.06.016
- Jones OY, Spencer CH, Bowyer SL, Dent PB, Gottlieb BS, Rabinovich CE. A multicenter case-control study on predictive factors distinguishing childhood leukemia from juvenile rheumatoid arthritis. Pediatrics. 2006;117(5):e840-4. https://doi.org/10.1542/peds.2005-1515
- Antón J, Camacho Lovillo M, Núñez Cuadros E. Reumatología Pediátrica, de dónde venimos y a dónde vamos. An Pediatr (Barc). 2020;92(3):121-3. https://doi.org/10.1016/j.anpedi.2020.01.003
- De Inocencio J, Antón J. Reumatología pediátrica. Breve historia y situación de la especialidad en España. Acta Reumatológica. 2014;1(2):37-43.
- Spencer CH. Why should pediatric rheumatology be recognized as a separate subspecialty: an open letter to medical councils and government agencies. Pediatr Rheumatol Online J. 2007;21(5):21. https://doi.org/10.1186/1546-0096-5-21
- Sawyer JR, Kapoor M. The limping child: a systematic approach to diagnosis. Am Fam Physician. 2009;79(3):215-24.
- Tu J, Haines M, Gowdie P, Craig S. Paediatric acute non-traumatic limp presenting to the emergency department: a retrospective observational study. Emerg Med J. 2023;40(3):182-8. https://doi.org/10.1136/emermed-2022-212624
- Irfan A, Starr RJ, Foster S, Smith ID, Huntley JS. 'Irritable Hip': Diagnosis in the Emergency Department. A Descriptive Study Over One Year. Cureus. 2018;10(10):e3481. https://doi.org/10.7759/cureus.3481
- Murias S, Remesal A, Quiles MJ, Merino R. Características de los pacientes con cojera en Reumatología. An Pediatr (Barc). 2012;76(5):290-3. https://doi.org/10.1016/j.anpedi.2011.10.011
- Santili C, Lino Júnior W, De Oliveira Goiano E, Barreto Lins RA, Waisberg G, Dos Reis Braga S, et al. Limping in Children. Rev Bras Ortop. 2015;44(4):290-8. https://doi.org/10.1016/S2255-4971(15)30156-7