
Vol. 26 - Num. 102
Originales
Valoración de la atención médico forense a víctimas de violencia sexual menores de edad en la provincia de Alicante (España)
Esperanza Navarro Escayolaa, Clara Vega Vegab, Rafael Bañón Gonzálezc, Mar Pastor Bravod
aSección de Laboratorio de Toxicología. Instituto de Medicina Legal y Ciencias Forenses de Alicante. Alicante. España.
bSección de Policlínica y Especialidades. Instituto de Medicina Legal y Ciencias Forenses de Alicante. Alicante. España.
cDirección General para el Servicio Público de Justicia. Ministerio de Justicia. Madrid. España.
dDirectora del Instituto de Medicina Legal y Ciencias Forenses de Alicante. Alicante. España.
Correspondencia: E Navarro. Correo electrónico: enavarroescayola@gmail.com
Cómo citar este artículo: Navarro Escayola E, Vega Vega C, Bañón González R, Pastor Bravo M. Valoración de la atención médico forense a víctimas de violencia sexual menores de edad en la provincia de Alicante (España) . Rev Pediatr Aten Primaria. 2024;26:155-64. https://doi.org/10.60147/c27181a1
Publicado en Internet: 24-06-2024 - Número de visitas: 17036
Resumen
Introducción: los abusos sexuales a menores constituyen un problema social complejo que requiere un abordaje multidisciplinario.
Material y métodos: estudio descriptivo retrospectivo de 256 víctimas de violencia sexual menores de 18 años, atendidas en el Instituto de Medicina Legal y Ciencias Forenses de Alicante, de 2016 a 2020. Agrupadas en dos intervalos de edad: de 0 a 12 años: (104 casos; 40,6%); y de 13 a 17 años: (152 casos; 59,4%).
Resultados: la mayoría de las víctimas eran mujeres (228 casos; 89,1%). Referían un único agresor (218 casos; 89%), conocido por la víctima (185 casos; 74,6%). En el grupo de menor edad, el tipo de violencia sexual más frecuente fueron los tocamientos (75 casos), y en el de mayor edad, la penetración vaginal (57 casos). En 51 casos (19,9% del total), los episodios de violencia sexual fueron reiterados, fundamentalmente en el ámbito familiar. La mayoría de las víctimas no presentaron lesiones (70,3% del total). En el grupo de mayor edad, se produjeron casi la mitad de las lesiones físicas (60 casos; 39,5%) y la totalidad de las lesiones psíquicas (3 casos; 1,5%). En 17 casos (6,7% del total) existía sospecha de sumisión química, fundamentalmente en el grupo de mayor edad, 15 casos (10,1%). Las tres sustancias más frecuentemente encontradas fueron: alcohol, seguido de cannabis y benzodiacepinas.
Conclusiones: nuestros datos muestran la importancia de los Institutos de Medicina Legal y Ciencias Forenses como fuente de información, aportando elementos que facilitan la detección y elaboración de estrategias de prevención en violencia sexual.
Palabras clave
● Examen médico forense ● Violencia sexual a menoresINTRODUCCIÓN
El abuso sexual a un menor consiste en la participación de un niño/a en una actividad sexual que no comprende plenamente, a la que no es capaz de dar su consentimiento, o para la que por su desarrollo no está preparado y no puede expresar su consentimiento, o bien que infringe las leyes o los tabúes sociales1.
Para que haya abuso sexual infantil deben concurrir dos criterios necesarios: una relación de desigualdad entre agresor y víctima (en cuanto a edad, madurez o poder) y la utilización del menor como objeto sexual2. En España la edad para otorgar el consentimiento sexual de forma autónoma se ha establecido a los 16 años3,4.
Los abusos sexuales a menores constituyen un problema social complejo de enormes dimensiones y que genera una gran alarma social. Constituyen una de las realidades menos conocidas, al ser considerado un tema tabú5. Por ello, requiere un abordaje multiprofesional de todas las instituciones implicadas (servicios sanitarios y educativos, órganos judiciales, Ministerio Fiscal, Fuerzas y Cuerpos de Seguridad del Estado, los Institutos de Medicina Legal y Ciencias Forenses [IMLCF] y el Instituto Nacional de Toxicología y Ciencias Forenses [INTCF])6.
En el año 2023 se creó en el IMLCF de Alicante una Unidad de Valoración Forense Integral de la Infancia y la Adolescencia, compuesta por un equipo multidisciplinar de profesionales de la medicina forense, la psicología y el trabajo social. Está dotada de un espacio físico adaptado a las necesidades de este tipo de procedimientos. Tiene como objetivo aglutinar a todos los agentes implicados en la respuesta institucional ante un niño, niña o adolescente (NNA) que sufre un acontecimiento traumático delictivo. Con esta unidad se intentan establecer pautas de actuación que garanticen la protección del menor, evitando la victimización secundaria, de acuerdo con las recomendaciones establecidas por diferentes instancias internacionales7,8.
El objetivo del presente trabajo es determinar la incidencia de la violencia sexual (VS) en NNA para visibilizar y conocer mejor este tipo de situaciones, y ayudar a poner los medios para prevenir este tipo de violencia.
MATERIAL Y MÉTODOS
Se realizó un estudio descriptivo retrospectivo de los menores de 18 años víctimas de VS atendidos por el IMLCF de Alicante, entre los años 2016 y 2020.
Las fuentes de información empleadas fueron la documentación de la historia clínica, el informe médico forense y el formulario normalizado de recogida de datos incluido en el protocolo de actuación médico forense en los casos de delitos contra la libertad sexual del IMLCF de Alicante9,10 y el protocolo del Consejo Médico Forense11.
Se han analizado los datos sociodemográficos, antecedentes médicos, circunstancias de los hechos y tipo de VS. Se tomaron muestras para estudios biológicos y químico-toxicológicos, que se realizaron en el INTCF (Departamento de Barcelona).
Los casos con sospecha de sumisión química (SSQ), han sido revisados por dos investigadores que han aplicado los criterios de inclusión de SSQ recogidos por Du Mont et al.12.
La información resultante fue analizada mediante el programa estadístico SPSS v.15.0 para Windows.
RESULTADOS
De los 702 casos de víctimas de VS recogidos en el IMLCF de Alicante en el periodo estudiado, 256 casos (36,5%) eran menores de 18 años. La edad media fue 11,8 años, (rango de 1 a 17 años, DE + 4,809). La moda de edad fue de 15 años.
Para mejorar el análisis discriminante de las variables, se han dividido los casos en 2 grupos de edad: grupo A, de 0 a 12 años (104 casos; 40,6%) y grupo B, de 13-17 años (152 casos; 59,4%) (Tabla 1).
| Tabla 1. Perfil de la víctima, del agresor y contexto espacio-temporal, en relación con los grupos de edad | ||||
|---|---|---|---|---|
| Variables | Total | Grupo A (0-12 años) | Grupo B (13-17 años) | P |
| N (%) | 256 (100) | 104 (40,6) | 152 (59,4) | |
| Perfil de la víctima | ||||
| Sexo | 256 (100) | 0,002 | ||
| Mujer | 85 (81,7) | 143 (94,1) | ||
| Varón | 19 (18,3) | 9 (5,9) | ||
| Antecedentes personales | 254 (99,2) | 0,007 | ||
| Enfermedad mental | 7 (6,7) | 30 (20) | ||
| Consumo voluntario | 252 (98,4) | 0,000 | ||
| Alcohol | 3 (2,9) | 62 (41,9) | ||
| Perfil del agresor | ||||
| N.º de agresores | 245 (95,7) | 0,001 | ||
| Uno | 99 (98) | 119 (82,6) | ||
| 2 o más | 2 (2) | 25 (17,3) | ||
| Relación con el agresor | 248 (96,9) | 0,000 | ||
| Conocido | 99 (97,1) | 86 (58,9) | ||
| Desconocido | 1 (1) | 32 (21,9) | ||
| Recién conocido | 2 (2) | 28 (19,2) | ||
| Relación de parentesco | 248 (96,9) | 0,000 | ||
| Padre/padrastro | 36 (34,6) | 11 (7,2) | ||
| Abuelo | 9 (8,8) | 1 (0,7) | ||
| Tío | 7 (6,9) | 3 | ||
| Contexto espacio temporal | ||||
| Lugar del hecho | 245 (95,7) | 0,000 | ||
| Domicilio agresor | 53 (53) | 54 (37,2) | ||
| Domicilio víctima | 28 (28) | 16 (11) | ||
| Vía pública | 6 (6) | 40 (27,6) | ||
| Local de ocio | 1 (1) | 15 (10,3) | ||
|
P: significación estadística (pruebas ji-cuadrado) |
||||

Perfil de la víctima (Tabla 1)
La mayoría de las víctimas eran mujeres (228 casos; 89,1%), mientras que solo 28 eran varones (10,9%). La proporción de varones fue mayor en el grupo A, con 19 casos (18,3%), respecto al grupo B, con 9 casos (5,9%) (p = 0,002).
El alcohol fue la sustancia consumida voluntariamente por la víctima con más frecuencia, fundamentalmente en el grupo B (62 casos; 41,9%), solo o en combinación con otras sustancias (p = 0,000).
Perfil del agresor (Tabla 1)
La mayoría de los casos de VS la produjo un único agresor (218 casos; 89%), conocido por la víctima (185 casos; 74,6%).
En aproximadamente la mitad de los casos del grupo B (60 casos; 41,1%) el agresor era desconocido o recién conocido por la víctima; mientras que en casi todos los casos del grupo A (97,1%) el agresor era conocido (p = 0,000).
En más de la mitad de los casos del grupo A, la VS la cometió un familiar: 62 casos (60,8%); mientras que el grupo B fueron 16 casos (11%) (p = 0,000).
Al analizar el grado de parentesco, el más frecuente fue el de padre/padrastro (47 casos; 18,2%). Por grupos, la mayor proporción fue en el grupo A (34,6%), respecto al obtenido en el grupo B (7,2%) (p = 0,000).
Contexto espacio-temporal
En nuestra muestra el número de casos de VS ha ido aumentando a lo largo de los años estudiados: en 2016 fueron 33 casos (12,9%); en 2017 fueron 56 casos (21,9%); y 2018 fue el año de mayor incidencia con 62 casos (24,2%). En el año 2019 descendió ligeramente el número (58 casos; 22,7%) y en el año 2020 el descenso fue mayor (47 casos; 18,4%), muy probablemente debido a la situación de pandemia por COVID-19 (Figura 1).
| Figura 1. Distribución de los casos de menores víctimas de violencia sexual a lo largo de los años, por intervalos de edad |
|---|
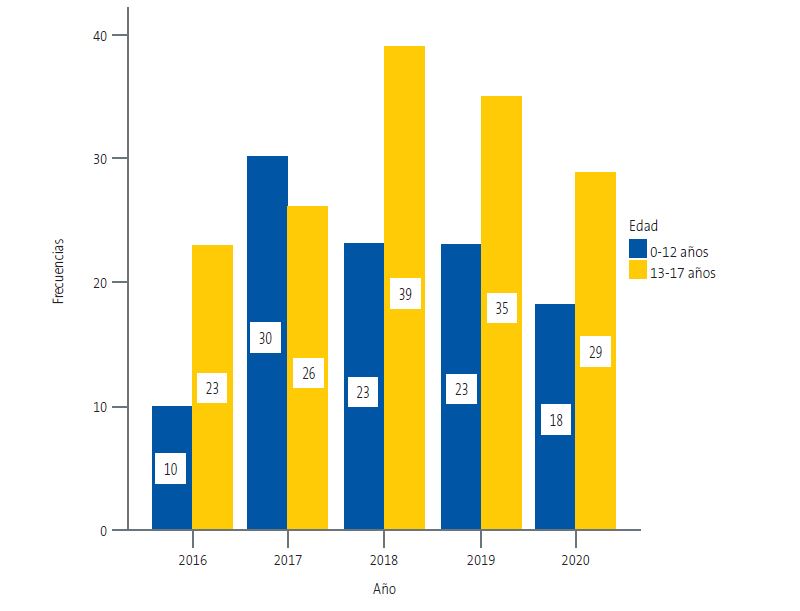 |

Los hechos se produjeron con mayor frecuencia durante los meses de mayo a agosto en casi la mitad de los casos (42,8%) y durante los fines de semana: sábado, 47 casos (19%), y domingo, 46 casos (18,6%).
En 132 casos (53,4%) se conocía la hora aproximada de los hechos. En el grupo B, los hechos se produjeron por la noche y en la madrugada (93 casos; 81,6%); mientras que en el grupo A, la VS se produjo predominantemente entre la mañana y la tarde (11 casos; 61,1%) (p = 0,000).
En el grupo A, los hechos se produjeron, por orden de frecuencia, en el domicilio del agresor, seguido del domicilio de la víctima. En el grupo B, en el domicilio del agresor, seguido de la vía pública, domicilio de la víctima y local de ocio (p = 0,000) (Tabla 1).
Circunstancias de la violencia sexual
En 51 casos (19,9%) se produjeron episodios reiterados de VS. Por grupos de edad, fue mucho menos frecuente en el grupo B (12 casos; 7,9%) (Tabla 2).
| Tabla 2. Circunstancias de la violencia sexual en relación con los grupos de edad | ||||
|---|---|---|---|---|
| Variables | Total | Grupo A (0-12 años) | Grupo B (13-17 años) | P |
| N (%) | 256 (100) | 104 (40,6) | 152 (59,4) | |
| Tipo de violencia sexual | 234 (91,4) | 0,000 | ||
| Tocamientos | 75 (73,5) | 22 (16,9) | ||
| Penetración vaginal | 7 (6,9) | 57 (43,8) | ||
| Penetración anal | 7 (6,9) | 7 (5,4) | ||
| Penetración más de 1 vía | 4 (3,9) | 26 (20) | ||
| Combinado (penetración, tocamientos, felación) | 8 (7,8) | 16 (12,3) | ||
| Número de episodios VS | 256 (100) | 0,000 | ||
| Único | 65 (62,5) | 140 (92,1) | ||
| Múltiples | 39 (37,5) | 12 (7,9) | ||
|
P: significación estadística (pruebas ji-cuadrado); VS: violencia sexual. |
||||

El tiempo transcurrido desde los hechos denunciados al reconocimiento y toma de muestras fue inferior a 24 horas en algo más de la mitad de los casos (140 casos; 56,7%).
El tipo de VS más frecuente fueron los tocamientos (101 casos; 43,2%), seguido de la penetración vaginal (65 casos; 27,8%).
En el grupo A predominan los tocamientos (75 casos), mientras que en el grupo B predomina la penetración vaginal (57 casos), seguido de penetración por más de una vía (26 casos), (p = 0,000) (Tabla 2).
La mayoría de las víctimas no presentaron lesiones (180 casos; 70,3%). En el grupo B se produjeron casi la mitad de las lesiones físicas (60 casos; 39,5%) y la totalidad de las lesiones psíquicas (3 casos; 1,5%) (p = 0,000).
En las víctimas con lesiones físicas (76 casos; 29,7%), las localizaciones más frecuentes fueron las extragenitales (54 casos; 21,1%), seguidas de las lesiones anogenitales (39 casos; 15,2%). Las lesiones psíquicas encontradas fueron: ansiedad, depresión, trastorno ansioso-depresivo.
La mayoría de las lesiones físicas curó en una semana o menos (65 casos; 95,7%) y ninguna víctima requirió ingreso hospitalario ni presentó secuelas. En tres casos pertenecientes al grupo B (2%) se produjeron secuelas psíquicas: un caso de agravación de depresión (0,7%) y dos casos de depresión (1,3%).
Se diagnosticaron dos casos de enfermedad de transmisión sexual (ETS): un varón de 5 años con sintomatología compatible con ETS; se obtuvieron anticuerpos positivos frente a Treponema pallidum (sífilis) y Chlamydia trachomatis. Y una niña de 6 años que acudió al hospital al presentar sintomatología y en el análisis se detectó Neisseria gonorrhoeae.
Estudios analíticos realizados (Tabla 3)
Se tomaron muestras biológicas con hisopos y/o ropa de la víctima en 192 casos (75%). En 72 casos (50,7%) se obtuvieron resultados positivos a semen y/o PSA, la mayoría de ellos en el grupo B (62 casos; 63,9%) (p = 0,000).
Se recogieron muestras de sangre, orina y cabello para estudios químico-toxicológicos en 62 casos (24,2%). Del total de 29 casos (11,3%), en los que se dispone de resultados, en 17 casos (6,7%) existía sospecha de probable sumisión química (SSQ). La mayor proporción de casos con SSQ fueron en el grupo B, con 15 casos (10,1%). En el grupo A se produjeron 2 casos (1,9%), eran dos hermanos de 10 y 11 años, a los que el padre administró benzodiacepinas para abusar de ellos de forma reiterada (Tabla 3).
| Tabla 3. Resultados biológicos, sospecha de sumisión química y resultados químico-toxicológicos, en relación con los grupos de edad | ||||
|---|---|---|---|---|
| Variables | Total | Grupo A (0-12 años) | Grupo B (13-17 años) | p |
| N (%) | 256 (100) | 104 (40,6) | 152 (59,4) | |
| Resultados biológicos | 142 (55,5) | 0,000 | ||
| Positivos | 10 (22,2) | 62 (63,9) | ||
| Negativos | 35 (77,8) | 35 (36,1) | ||
| SSQ | 256 (100) | 0,002 | ||
| Sumisión química probable | 2 (1,9) | 15 (10,1) | ||
| Resultados toxicológicos | 29 (11,3) | 0,036 | ||
| Alcohol | 0 | 6 (22,2) | ||
| Drogas | 0 | 2 (7,4) | ||
| Medicamentos | 2 (100) | 3 (11,1) | ||
| Combinación sustancias | 0 | 5 (18,5) | ||
|
SSQ: sospecha de sumisión química. |
||||

El alcohol fue la sustancia encontrada con mayor frecuencia (9 casos; 30,7%) solo o en combinación con drogas y/o medicamentos. Los medicamentos encontrados en orden de frecuencia fueron: benzodiacepinas (4 casos), antidepresivos (3 casos), antihistamínicos (2 casos) y antipsicóticos (1 caso). La droga de abuso encontrada con más frecuencia fue el cannabis, con 5 casos.
Nuestro trabajo tiene limitaciones, ya que la muestra estudiada se basa solo en los casos en que se ha formalizado denuncia y ha intervenido el IMLCF. No se recogen, por lo tanto, los casos no denunciados, posiblemente relacionados con niños de menor edad, en los que existe mayor dificultad para identificar indicios compatibles con VS, y que constituyen la parte sumergida del problema. Tampoco se incluyen los casos denunciados en los que no se ha solicitado reconocimiento e informe forense por la autoridad judicial.
DISCUSIÓN
El número de víctimas de VS menores de 18 años recogidos en el IMLCF de Alicante en el periodo estudiado fue de 256 casos; más de la mitad eran adolescentes de 13-17 años. Mc Cauley et al.13 describen la adolescencia como un periodo con alto riesgo de VS. Alrededor de 1/3 de violencia sexual en USA se produce en este periodo.
Al igual que lo descrito por otros autores, la mayoría de las víctimas eran mujeres13-16, siendo su proporción mayor en el grupo de mayor edad17; la de varones fue mayor en el grupo de 0-12 años (18,3%)18.
En nuestro estudio, en la mayoría de los casos la VS la ocasionó un único agresor, conocido por la víctima19. En el 20% de los casos se produjeron episodios de VS reiterada, semejante a lo descrito por Csorba et al. (20%)20, fundamentalmente en el entorno familiar13,19. En más de la mitad de los casos de víctimas menores de 13 años existía una relación de parentesco con el agresor19. La mayor vulnerabilidad del menor hace necesario extremar la vigilancia ante estas posibles situaciones y, ante el menor indicio o sospecha, realizar un seguimiento más estrecho del menor.
En algo más de la mitad de los casos, el reconocimiento médico se realizó dentro de las primeras 24 horas de los hechos denunciados. Estos resultados pueden deberse a que nuestro estudio incluye únicamente los casos en los que se ha producido denuncia e intervención del médico forense. También influye la elevada proporción de adolescentes en nuestra muestra. Como se describe en otros trabajos, los adolescentes tienden a revelar antes los hechos21. A edades más tempranas, el descubrimiento inmediatamente después de la VS es raro y es más frecuente el descubrimiento accidental tiempo después.
La mayoría de las víctimas no presentaron lesiones5. La presencia de lesiones físicas se dio con más frecuencia en el grupo de mayor edad19. Resulta lógico este resultado porque en el grupo de los niños de menor edad el tipo de violencia sexual más frecuente fueron los tocamientos, en los que apenas hay presencia de lesiones físicas, lo que hace que el hecho pase desapercibido. Ninguna de las lesiones físicas producidas dejó secuelas.
Llama la atención el escaso número de secuelas psíquicas que presentaron las víctimas, únicamente en tres casos, pertenecientes al grupo de 13-17 años. Nuestros resultados no están en consonancia con lo descrito por Mc Cauley et al.13, que asocian los delitos sexuales en adolescentes a un incremento de riesgo de síndrome de estrés postraumático, depresión y trastorno por abuso de sustancias. El escaso número de secuelas psíquicas que hemos encontrado puede estar relacionado, al igual que lo descrito por algunos autores22, con el tiempo transcurrido desde los hechos hasta la exploración, que en nuestro estudio fue generalmente breve en este grupo de mayor edad y a que no se suelen producir alteraciones psíquicas inmediatas. Para una correcta valoración es necesario un estudio clínico profundo de cada caso que pueda confirmar las relaciones causa-efecto en este tipo de patología23. También es necesario un seguimiento del menor, para poder establecer el alcance real de la VS. Aunque la literatura científica no reconoce un síndrome cognitivo-conductual específico de haber sufrido violencia sexual infantil, hay que destacar las consecuencias que este abuso produce en el menor y que afecta a todas las áreas de su vida5.
La mayoría de los casos que cumplían los criterios de probable sumisión química se encontraron en el grupo de 13-17 años. En orden decreciente, las tres sustancias más frecuentemente encontradas fueron el alcohol, seguido de cannabis y benzodiacepinas. En casi la mitad de los casos, el alcohol fue la sustancia más consumida voluntariamente por la víctima previamente a los hechos. Este hallazgo es semejante al de otros estudios, en los que el alcohol, solo o en combinación con otras sustancias, constituye un factor importante de vulnerabilidad24.
CONCLUSIONES
Los menores de edad presentan mayor vulnerabilidad y requieren de una mayor protección, por lo que es necesario extremar su vigilancia y así poder detectar este tipo de violencia lo antes posible. Así mismo, es importante realizar un seguimiento de menores víctimas de VS, tanto a nivel asistencial como por parte de personal médico forense, para poder establecer el alcance real de la violencia sexual sufrida.
Es necesario poner medios para ayudar a visibilizar este problema, planificando estrategias de formación para que los profesionales de la salud, educadores y familiares conozcan los indicadores de sospecha de VS, fundamentalmente en los menores de 13 años.
Es fundamental la intervención coordinada de todos los profesionales del sistema asistencial y jurídico que intervienen en los casos de denuncia de VS sobre el menor. La creación en Alicante de la Unidad de Valoración Forense Integral de la Infancia y Adolescencia ayudará a mejorar la calidad de la atención prestada a los menores tras un hecho de este tipo.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este trabajo no ha recibido ninguna subvención.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del manuscrito publicado.
AGRADECIMIENTOS
Nuestro agradecimiento al departamento de química del Instituto Nacional de Toxicología y Ciencias Forenses (departamento de Barcelona), por su trabajo y profesionalidad.
ABREVIATURAS
IMLCF: Instituto de Medicina Legal y Ciencias Forenses · INTCF: Instituto Nacional de Toxicología y Ciencias Forenses · NNA: niño, niña y adolescente · SSQ: sospecha de sumisión química · VS: violencia sexual.
BIBLIOGRAFÍA
- Report of the Consultation on Child Abuse and Neglect Prevention, 29-31, Document WHO/HSC/PVI. Ginebra, 1999. En: Iris VHO [en línea] [consultado el 22/08/2023]. Disponible en https://iris.who.int/handle/10665/65900
- Echuburúa E, Guerricaechevarría C. Abuso sexual en la infancia: víctimas y agresores, un enfoque clínico. 6.ª ed. Barcelona: Ariel; 2005.
- Orjuela López l, Rodríguez Bartolomé V. Violencia sexual contra los niños y las niñas. Abuso y explotación sexual infantil. Guía de material básico para la formación de profesionales. 2012. En: Save the Children [en línea] [consultado el 22/08/2023]. Disponible en www.savethechildren.es/sites/default/files/imce/docs/violencia_sexual_contra_losninosylasninas.pdf
- Ley Orgánica 1/2015, de 30 de marzo, por la que se modifica la LO 10/1995, de 23 de noviembre del Código Penal español de 2015. Título VIII, capítulo II bis, de los abusos y agresiones sexuales a menores de 16 años. En: BOE [en línea] [consultado el 22/08/2023]. Disponible en www.boe.es/buscar/doc.php?id=BOE-A-2015-3439
- Abuso sexual en la Infancia y la Adolescencia según los Afectados y su Evolución en España (2008-2019). 2020. En: ANAR [en línea] [consultado el 22/08/2023]. Disponible en www.anar.org/wp-content/uploads/2021/12/Estudio-ANAR-abuso-sexual-infancia-adolescencia-240221-1.pdf
- Actuación en la atención a menores víctimas en los Institutos de Medicina Legal y Ciencias Forenses. Consejo Médico-Forense. Ministerio de Justicia. Secretaría Técnica. Madrid, 2018. En: Ministerio de Justicia [en línea] [consultado el 22/08/2023]. Disponible en www.mjusticia.gob.es/es/AreaTematica/DocumentacionPublicaciones/InstListDownload/Actuacion_en_la_atencion_a_menores_victimas_en_los_institutos_de_medicina_legal_y_ciencias_forenses.PDF
- Portal estadístico de criminalidad. Ministerio de Interior. En: Estadisticas de criminalidad [en línea] [consultado el 22/08/2023]. Disponible en https://estadisticasdecriminalidad.ses.mir.es/publico/portalestadistico.html
- Comité de los Derechos del Niño (CRC). Observación general n.º 14 (2013) sobre el derecho del niño a que su interés superior sea una consideración primordial (artículo 3, párrafo 1) ONU, 2013. En: UNHCR/ACNUR [en línea] [consultado el 22/08/2023]. Disponible en www.refworld.org/es/ref/polilegal/crc/2013/es/95780
- Vega Vega C, Navarro Escayola E, Edo Gil JC. Protocolo de actuación médico forense en los delitos contra la libertad sexual. Rev Esp Med Legal. 2014;3:120-28. https://doi.org/1016/j.reml.2014.04.002
- Vega Vega C, Navarro Escayola E. Protocolo de Actuación Médico-Forense en los delitos contra la Libertad Sexual: Revisión y Actualización. Gac Int Cienc forense. 2021; 41:43-54.
- Protocolo de Actuación médico-forense ante la violencia sexual en los Institutos de Medicina Legal y Ciencias Forenses. Comité Científico-Técnico. Consejo Médico Forense, Secretaría General Técnica. Ministerio de Justicia. Madrid, 2021. En: Ministerio de Justicia [en línea] [consultado el 22/08/2023] Disponible en www.mjusticia.gob.es/es/ElMinisterio/OrganismosMinisterio/Documents/ProtocoloViolenciaSexual.pdf
- Du Mont J, Macdonald S, Rotbard N, Asllani E, Bainbridge D, Cohen MM. Factors associated with suspected drug-facilitated sexual assault. CMAJ. 2009;180(5):513-9. https://doi.org/10.1503/cmaj.080570
- McCauley Jl, Conoscenti M, Ruggiero KJ, Resnick HS, Saunders BE, Kilpatrick DG. Prevalence and correlates of Drug/Alcohol-facilitated and incapacitated sexual assault in a Nationally representative sample of adolescent girls. J Clin Chid Adolesc Psychol. 2009;38(2):295-300. https://doi.org/10.1080/15374410802698453
- Livano RM, Valdivia-Livano S, Mejía CR. Evaluaciones psicológicas forenses de abuso sexual en menores: proceso de revelación y cronicidad del evento en la serranía peruana. Rev Esp Med Legal. 2021;47:57-65.
- Finkelhor D, Hammer H, Sedlak AJ. Sexually assaulted children: national estimates and characteristics. US Government Printing Office. Washington, Juvenile Justice Bulletin-NCJ 214383, 2008. En: Office of Justice Program [en línea] [consultado el 22/08/2023]. Disponible en www.ojp.gov/pdffiles1/ojjdp/214383.pdf
- Pereda N. ¿Uno de cada cinco? Victimización sexual infantil en España. En: Papeles del psicólogo. 2016;37(2):126-33 [en línea] [consultado el 22/08/2023]. Disponible en www.papelesdelpsicologo.es/pdf/2697.pdf
- Snyder H.N. Sexual assault of young children as reported to law enforcement: Victim, incident, and offender characteristics. US Department of Justice, Annapolis. Bureau of Justice statistics. En: Office of Justice Program [en línea] [consultado el 22/08/2023]. Disponible en https://bjs.ojp.gov/library/publications/sexual-assault-young-children-reported-law-enforcement-victim-incident-and
- Gewirtz-Meydan A, Finkelhor D. Sexual abuse and assault in a large national sample of children and adolescents. Child Maltreat. 2020;23(2):203-14. https://doi.org/10.1177/1077559519873975
- Emmert C, Köhler U. Data about 154 children and adolescents reporting sexual assault. Arch Ginecol Obstet. 1998;261:61-70. https://doi.org/10.1007/s004040050200
- Csorba R, Aranyosi J, Borsos A, Balla l, Major T, Póka R. Characteristics of female child sexual abuse in Hungary between 1986 and 2001: a longitudinal, prospective study. Eur J Obstet Gynecol Reprod Biol. 2005;120:217-21. https://doi.org/10.1016/j.ejogrb.2004.08.018
- Leyton C, Quezada D, Molina T. Perfil epidemiológico de adolescentes mujeres con antecedentes de agresión sexual consultantes en el área de salud mental de un centro de salud sexual y reproductiva. Rev Chil Obstet Ginecol. 2013;78(1):26-31. http://dx.doi.org/10.4067/S0717-75262013000100005
- Suárez Solá M, González Delgado F. Importancia de la exploración médico forense en las agresiones sexuales a menores. Cuad Med Forense. 2003;31:37-45.
- Kaur S, Kaur S, Rawat B. Medico-legal evidence collection in child sexual assault cases: a forensic significance. Egypt J Forensic Sci. 2021;11(41):1-6.https://doi.org/10.1186/s41935-021-00258-y
- Gallo J, Padilla M. Abusos sexuales en niñas y adolescentes. Consideraciones médico legales. Clin Invest Gin Obst. 2006;33(6):222-9. https://doi.org/10.1016/S0210-573X(06)74121-1