
Vol. 26 - Num. 102
Originales
Valoración de la eficacia de la educación en el manejo de autoinyectores de adrenalina
María Villarreal Calvoa, Juan Carlos Juliá Benitob
aPediatra de Atención Primaria. Servicio Navarro de Salud. España.
bPediatra de Atención Primaria. Servicio Valenciano de Salud. España.
Cómo citar este artículo: Villarreal Calvo M, Juliá Benito JC. Valoración de la eficacia de la educación en el manejo de autoinyectores de adrenalina . Rev Pediatr Aten Primaria. 2024;26:165-71. https://doi.org/10.60147/279dc09a
Publicado en Internet: 14-06-2024 - Número de visitas: 11301
Resumen
Introducción: la anafilaxia es una emergencia médica y la administración temprana de adrenalina es esencial para disminuir su morbimortalidad. Los pacientes ya diagnosticados de anafilaxia disponen de autoinyectores de adrenalina para que instauren el tratamiento sin esperar a ser atendidos por los servicios médicos. El objetivo de nuestro estudio es valorar los conocimientos de los padres acerca de la anafilaxia y el uso de los autoinyectores, y si mejoran tras una breve formación especializada.
Material y métodos: estudio comparativo antes-después. Se revisaron 6 cupos de Atención Primaria seleccionando aquellos pacientes que tenían diagnóstico de anafilaxia y prescripción de adrenalina. Se enviaron dos correos electrónicos: el primero con una encuesta acerca de la enfermedad y los autoinyectores de adrenalina; el segundo contenía videos y hojas informativas y una segunda encuesta. De esta manera, se han comparado los conocimientos pre y posintervención.
Resultados: los alimentos fueron la principal causa de reacción anafiláctica. El 56,3% admitía llevar siempre el dispositivo. Comparando los conocimientos pre y posintervención (test exacto de Fisher) destaca una mejoría en casi todos los pasos a seguir al administrar la adrenalina. Mejoraron de forma significativa la identificación del tapón de seguridad (p 0,018) y conocer que se puede repetir una segunda dosis (p 0,006). Respecto a la necesidad de masajear la zona, la mejoría fue clara pero sin llegar a ser estadísticamente significativa (p 0,066).
Conclusiones: la formación periódica a padres de niños con prescripción de adrenalina autoinyectable es fundamental para disminuir la morbimortalidad de estos pacientes.
Palabras clave
● Adrenalina ● Anafilaxia ● Autoinyector de adrenalina ● Educación ● Reacción alérgicaINTRODUCCIÓN
La anafilaxia es la reacción alérgica más grave que existe, de instauración rápida y potencialmente mortal1,2.
Según las recomendaciones de las guías clínicas2, el diagnóstico se basa en criterios clínicos y el tratamiento de elección es la adrenalina intramuscular. Para ello es fundamental que padres y demás personas a cargo de niños con esta enfermedad (otros familiares, profesores, etc.) conozcan el alérgeno que causa la reacción, los síntomas característicos y el manejo de la medicación para poder administrar el tratamiento de forma correcta y eficaz.
Se trata de una emergencia médica y el retraso en la administración de adrenalina aumenta el riesgo de hospitalización y de muerte por anafilaxia2. Por ello, los pacientes ya diagnosticados de anafilaxia disponen de los autoinyectores de adrenalina, para que puedan instaurar el tratamiento sin esperar a ser atendidos por los servicios médicos.
El objetivo de este estudio es valorar los conocimientos de padres de niños con anafilaxia: conceptos generales sobre la enfermedad y sobre el funcionamiento de los autoinyectores de adrenalina y constatar si tras recibir una breve formación específica en la materia mejoran dichos conocimientos. Todo ello con el objetivo final de mejorar la formación de los responsables de estos niños para disminuir la morbimortalidad asociada a esta enfermedad.
MATERIAL Y MÉTODOS
Diseño del estudio y selección de la muestra
Estudio analítico comparativo antes-después en pacientes diagnosticados de anafilaxia y con prescripción médica de adrenalina intramuscular autoinyectable.
Criterios de inclusión: se incluyó en el estudio a todos los niños que tenían en historia clínica el diagnóstico de “anafilaxia” y además tenían prescripción médica de adrenalina autoinyectable. Se reclutaron pacientes durante aproximadamente 5 meses.
Criterios de exclusión: pacientes que no habían sido diagnosticados en el momento del estudio de anafilaxia y todos aquellos en los que se había sospechado inicialmente este diagnóstico, pero que tras el estudio alergológico se había descartado dicha enfermedad y no tenían como consecuencia prescrito el autoinyector de adrenalina.
Selección de la muestra: se analizaron 6 cupos de pacientes de Atención Primaria, de aproximadamente 1000-1100 niños cada uno. Mediante la extracción de datos de historia clínica informatizada se objetivó que en cada cupo había entre 3 y 6 niños que cumplían los criterios de inclusión. Se contactó con dichas familias vía telefónica para ver si querían participar en el estudio, explicándoles las características del estudio y la finalidad. Solo aquellas que querían participar, y dando su consentimiento, recibían dos emails a su correo electrónico.
Pasos del estudio
Variables iniciales de estudio (preintervención): en un primer email se enviaba una encuesta en la que se consultaba sobre los siguientes datos.
- Datos sociodemográficos: edad al diagnóstico y sexo. Lugar habitual de residencia (urbano/rural) y distancia en coche a un centro médico (minutos).
- Antecedentes alérgicos: antecedentes familiares. Antecedentes personales de enfermedades relacionadas con la marcha alérgica (dermatitis atópica/rinitis alérgica/asma).
- Preguntas sobre su alergia: a qué tiene alergia (alimentos/picadura de himenópteros/fármacos/inhalantes). Posteriormente, debían describir en concreto a qué tenían alergia (ejemplo: avellana, veneno de abeja o amoxicilina).
- Preguntas sobre anafilaxia: tratamiento de elección (debiendo elegir entre: antihistamínico oral/corticoide oral/oxígeno/adrenalina intramuscular), existencia de contraindicaciones para el uso de adrenalina (sí algunos fármacos/sí muchas enfermedades/no, no hay contraindicaciones).
- Preguntas sobre autoinyectores de adrenalina: qué marca de autoinyector tiene (Altellus/Jext/Anapen/Emerade), cuántos autoinyectores tiene, si suele revisar la fecha de caducidad, si el niño lo lleva siempre consigo.
- Preguntas prácticas sobre cómo se usan los autoinyectores: identificar en una imagen el tapón de seguridad, cómo sujetar correctamente el autoinyector, necesidad de retirar la ropa antes de administrar la medicación (verdadero/falso), lugar de administración del fármaco, tiempo de espera antes de retirar la aguja, necesidad de masajear la zona tras administrar la medicación, posibilidad de repetir la dosis si el niño no se encuentra bien. Miedo a usar el autoinyector (sí/no), antecedente de haber entrenado con algún autoinyector de prueba o con uno caducado sobre una naranja (sí/no).
Intervención: tras contestar a esa primera encuesta recibían un segundo email con la intervención, que consistía en la visualización de vídeos formativos y hojas con gráficos sobre el uso de los autoinyectores de adrenalina. Toda esta información era de fuentes oficiales y validadas (Anexo 1):
- Sociedad Española de Alergología e Inmunología clínica (SEAIC): www.youtube.com/watch?v=g_l7ECDN-W8
- Agencia Española de Medicamentos y Productos Sanitarios (AEMPS): Autoinyector Altellus (www.youtube.com/watch?v=co0v_S-Dbjw) y autoinyector Yext.
- Sociedad Española de Inmunología Clínica, Alergología y Asma Pediátrica (SEICAP) (Anexo 1).
Estudio posintervención: para valorar la repercusión en los conocimientos sobre el uso de los autoinyectores tras una breve formación específica en la materia. Junto con el segundo email se enviaba la segunda encuesta en la que se preguntaba de nuevo (mismas preguntas con mismo formato) sobre el uso de los autoinyectores. Finalmente, se consultaba sobre su percepción acerca de la utilidad de realizar actividades de formación continuada como esta (sí/no).
Tras cumplimentar la segunda encuesta, el programa corregía al participante simultáneamente a la realización del propio test. De esta forma, el usuario no tenía forma de modificar la respuesta, pero era consciente de si había contestado de manera correcta o si se había equivocado, aprendiendo así de su error.
Para la realización del estudio se siguieron las consideraciones éticas sin vulnerar los derechos de los participantes. Solo participaron aquellos que voluntariamente quisieron dar su dirección de correo electrónico para recibir la información. Todas las respuestas de las encuestas eran anónimas.
Dada la situación en la cual se realizó el estudio, en contexto de pandemia mundial por COVID-19, se decidió plantear todo el estudio y la formación vía online.
Análisis
El análisis estadístico se realizó con el programa IBM SPSS Statistics (SPSS Statistics for Windows, Version 22.0; IBM Corp. Armonk, NY).
Los resultados de las variables cualitativas se han expresado con porcentajes. Los resultados de las variables cuantitativas se han descrito con medianas y rangos intercuartílicos. Las diferencias entre grupos en variables categóricas se han analizado mediante el test exacto de Fisher (teniendo en cuenta el tamaño muestral). Se ha considerado un nivel de significación estadística del 5% (p < 0,05).
RESULTADOS
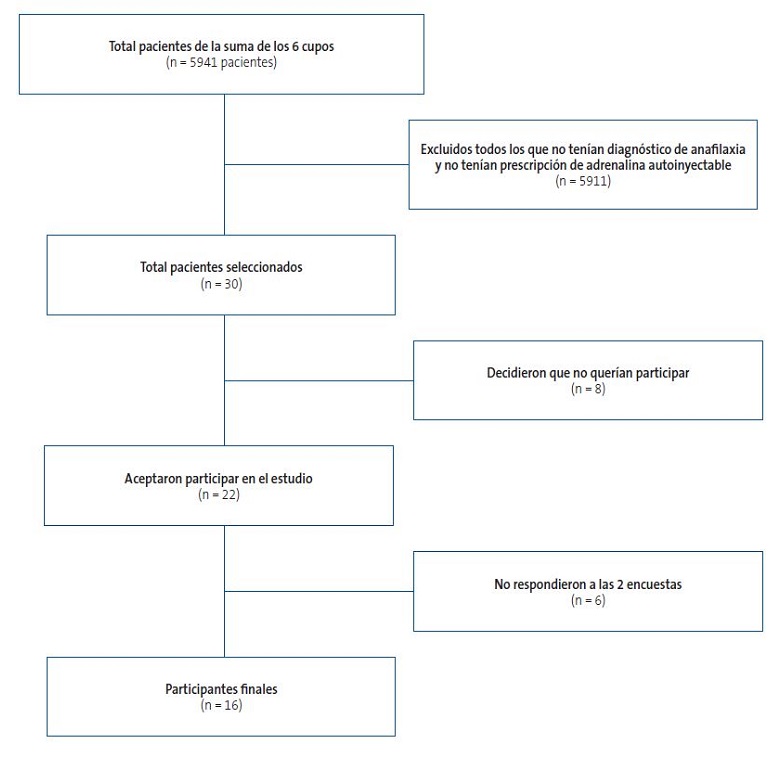
La Figura 1 muestra la selección de pacientes.
| Figura 1. Esquema de selección de pacientes |
|---|
 |

La mayor parte de los pacientes reclutados vivían en zona urbana 81,3% vs. 18,8% en zona rural. A pesar de esta diferencia, la mediana de tiempo en coche a un centro médico fue de 5 minutos (5-7).
Consultando sobre los antecedentes familiares, el 50% no tenía antecedentes alérgicos. De los que sí tenían antecedentes, en el 18,75% de los casos era la madre la que tenía alergia. En dos casos (12,5%) el antecedente era paterno. También en dos casos eran ambos progenitores alérgicos y, por último, un paciente (que representa el 6,25% de la muestra) tenía ambos progenitores y algún hermano con este antecedente.
El 75% de los pacientes participantes en el estudio eran varones. Más del 50% de los participantes tenían entre 1 y 4 años al diagnóstico, mediana de edad 3,5 años (1-4,75).
Todos los pacientes de la muestra habían sido diagnosticados de alguna enfermedad de la llamada marcha alérgica: 43,75% dermatitis atópica, 43,75% rinitis alérgica, 25% asma.
Los alimentos representaban el alérgeno más frecuente, en esta serie de pacientes, el 100% de los casos. Solamente un paciente tenía también alergia a fármacos, pero se encontraba en estudio en el momento de responder la encuesta y no supo especificar en concreto a qué medicamento. Ningún paciente tenía alergia provocada por picaduras de himenópteros.
Consultando en concreto a qué alimentos presentaban alergia, destaca que casi el 50% tenía alergia a varios alimentos y que a pesar de la corta edad de los pacientes la gran mayoría presentaba alergia a frutos secos (56,25%). En segundo lugar se encontraban las frutas con hueso (31,25%), seguido de kiwi y legumbres (en ambos casos 18,75%), marisco, pescado y huevo (12,5%) y, por último, proteínas de leche de vaca (6,25%).
Profundizando acerca de la medicación en caso de anafilaxia llama la atención que el 100% de los participantes tenía claro que el tratamiento de elección es la adrenalina intramuscular. Además en todos los casos salvo en uno tenían también claro que no hay contraindicaciones para la administración de la adrenalina.
Preguntando sobre qué autoinyector tenían prescrito, el 56,3% tenían Altellus y el 43,8% Jext. Ningún paciente tenía Anapen ni Emerade. Cinco pacientes (31,3%) tenían 2 autoinyectores y dos pacientes (12,5%) tenían 3 o más. El 56,25% restante tenía solo uno.
A pesar de la importancia de tener siempre accesible la medicación para poderla administrar cuanto antes, llama la atención que poco más de la mitad la llevan siempre consigo (56,3%).
Un dato muy positivo fue que la mayoría (87,5%) revisaba con frecuencia la fecha de caducidad del autoinyector para tenerlo siempre en buen estado en caso de necesitarlo.
Las siguientes preguntas trataban sobre el uso de los autoinyectores, preguntas prácticas sobre los pasos a seguir. La hipótesis de este trabajo trataba de demostrar la mejoría de los resultados tras un poco de formación (Tabla 1).
| Tabla 1. Resultados al cuestionario preintervención y posintervención. Análisis realizado mediante test exacto de Fisher | |||
|---|---|---|---|
| Pregunta | Número aciertos preintervención (%) | Número aciertos posintervención (%) | P |
| Reconocimiento tapón de seguridad | 10 (62,5%) | 16 (100%) | 0,018 |
| Cómo sujetar el autoinyector | 13 (81,3%) | 12 (75%) | 1 |
| Necesidad de retirar la ropa | 14 (87,5%) | 15 (93,8%) | 1 |
| Dónde inyectar la adrenalina | 16 (100%) | 16 (100%) | |
| Necesidad de esperar antes de retirar el dispositivo | 13 (81,3%) | 16 (100%) | 0,226 |
| Necesidad de masajear la zona | 7 (43,8%) | 13 (81,3%) | 0,066 |
| Posibilidad de administrar una segunda dosis | 6 (37,5%) | 14 (87,5%) | 0,006 |

Comparando los conocimientos pre y posintervención mediante el test exacto de Fisher destaca una mejoría en los resultados tras la intervención en casi todos los pasos (Tabla 1). El lugar de administración de la medicación (en la cara externa del muslo) no suscitó dudas en ningún momento, lo tenían claro antes de la intervención. Los conocimientos que mejoraron de forma significativa fueron la identificación del tapón de seguridad (p 0,018) y conocer que se puede repetir una segunda dosis a los 5-15 minutos si el niño no se encuentra bien (p 0,006). Respecto a la necesidad de masajear la zona tras la administración de la medicación, la mejoría en los conocimientos fue clara, pero sin llegar a ser estadísticamente significativa (p 0,066).
Otro dato llamativo fue que el 68,8% de los participantes admitía tener miedo a utilizar el autoinyector de adrenalina, el mismo porcentaje que afirmaba no haber entrenado nunca cómo utilizarlo, ya fuese con un autoinyector de prueba o con uno caducado, por ejemplo, en una naranja.
Casi el 100% de los participantes consideraron que esta actividad fue de su interés y tras la formación se sentían más preparados para actuar si fuese necesario. Los participantes consideraban que esta información debería llegar a profesores, responsables de comedores y cuidadores de campamentos para tranquilidad de todos y por el bien de los menores.
DISCUSIÓN
El incremento en la prevalencia de alergias2, especialmente las causadas por alimentos, provoca un aumento en la prescripción de autoinyectores de adrenalina. El Registro Europeo de Anafilaxia describe la causa alimentaria como la principal causa de anafilaxia en niños (88% en niños <6 años, 57% en niños de 6-12 años)3. Las cifras de nuestro estudio son superiores a las descritas en la bibliografía, siendo la causa alimentaria la causa de la prescripción en el 100% de los casos. Probablemente el pequeño tamaño muestral esté influyendo en este resultado. El principal alérgeno de los pacientes de nuestra muestra fueron los frutos secos, lo cual, teniendo en cuenta la mediana de edad (3,5 años), concuerda con la bibliografía consultada2 que describe los frutos secos (como la avellana y el anacardo) como la principal causa en preescolares. En los países europeos2, las frutas con hueso (como el melocotón) son una causa también frecuente de alergia alimentaria (en nuestra serie se trata de la segunda causa).
Se ha visto asociación entre los casos de anafilaxia fatal y la ausencia de adrenalina o la administración incorrecta de dicha medicación4. El error de administración más frecuentemente registrado en el uso del autoinyector es la inyección accidental de la medicación en el dedo/pulgar5,6. En nuestro estudio analizamos los errores en la administración de la medicación, destacando como los más frecuentes no saber que se puede repetir una segunda dosis si el paciente no mejora (62,5% de error), la necesidad de masajear la zona de punción (56,2% fallaron esta pregunta) y el error en la identificación del tapón de seguridad (37,5% se equivocaron).
La hipótesis de nuestro estudio era valorar si esos errores se solventaban con formación objetivando una mejoría generalizada en el uso del autoinyector y de forma significativa en aspectos tan básicos como la identificación del tapón de seguridad (p 0,018) o conocer que se puede repetir una segunda dosis a los 5-15 minutos si el niño no se encuentra bien (p 0,006).
De todas formas, de nada sirve la formación si finalmente los pacientes deciden no llevar consigo el dispositivo. En nuestra serie, poco más de la mitad (56,3%) de los pacientes lo llevaban siempre. En un estudio realizado en 20197 los pacientes afirmaban que no lo llevaban principalmente porque no se sentían preparados para utilizarlo. Llegaron a la conclusión de que informando a los pacientes de la importancia del tratamiento precoz y prescribiendo dispositivos sencillos y con instrucciones claras era más probable que lo llevaran. Algunos estudios8 sugieren que hay que tener en cuenta otros factores para que los pacientes no lleven siempre el dispositivo, como el elevado coste, la corta fecha de caducidad, la baja probabilidad de uso final y el miedo a utilizarlo9 (dato que se objetiva en nuestro estudio, donde casi el 70% admite tener miedo). Algunos de estos factores se pueden solventar o mitigar con la formación y el entrenamiento.
Las guías de la Agencia Europea del Medicamento recomiendan la prescripción de dos autoinyectores, ya que aproximadamente el 10% de los pacientes requieren de una segunda dosis10. En la guía de actuación de anafilaxia (GALAXIA 2016)1, recomiendan prescribir un segundo dispositivo en unas situaciones concretas. En nuestra serie, más de la mitad (56,25%) tenían solo uno, probablemente siguiendo las recomendaciones españolas. Hay que tener en cuenta que muchos pacientes llevan solo uno consigo, pero quizás tienen otro en casa, en el colegio o en otra localización, como han postulado en estudios previos11.
CONCLUSIONES
La formación continuada y la realización de actividades dirigidas al correcto uso de la medicación (ya sea presencial u online) son clave en la educación sanitaria de los pacientes. Es muy importante informar a los padres con lenguaje inteligible sobre los aspectos fundamentales de la enfermedad y explicarles cómo evitar posibles desencadenantes de una reacción anafiláctica.
Este estudio demuestra que hay conceptos muy básicos sobre el uso de los autoinyectores que los padres no tienen claros y que tras un proceso de formación esos conocimientos pueden mejorar de forma significativa y aportar confianza a los padres y seguridad a sus hijos.
MATERIAL SUPLEMENTARIO
Anexo 1. Uso de adrenalina autoinyectable
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo. Este trabajo no ha contado con financiación.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: idea original, supervisión y corrección (JCJB), diseño de encuestas, reclutamiento pacientes, análisis resultados y redacción (MVC). Los autores han remitido un formulario de autorización para usar la imagen del Anexo 1 (Material suplementario).
BIBLIOGRAFÍA
- Cardona V, Cabañes N, Chivato T, De la Hoz B, Fernandez M, Gangoiti I, et al. Grupo GALAXIA. Guía de Actuación en Anafilaxia. 2016. https://doi.org/10.18176/944681-8-6
- Juliá JC, Sanchez CA, Alvarado MI, Álvarez F, Arroabarren E, Capataz M, et al. Manual de anafilaxia pediátrica. SEICAP. Mayo 2017 [en línea] [consultado el 10/06/2024]. Disponible en https://seicap.es/wp-content/uploads/2022/05/MAP2017-Version-2-1.pdf
- Grabenhenrich LB, Dolle S, Moneret-Vautrin A, Kohli A, Lange l, Spindler T, et al. Anaphylaxis in children and adolescents: the European anaphylaxis registry. J Allergy Clin Immunol. 2016;137(4):1128-37.e1. https://doi.org/10.1016/j.jaci.2015.11.015
- Esenboga S, Ocak M, Cetinkaya PG, Sahiner UM, Soyer O, Buyuktiryaki B, et al. Physicians prescribe adrenaline autoinjectors, do parents use them when needed? Allergol Immunopathol (Madr). 2020;48(1):3-7. https://doi.org/10.1016/j.aller.2019.07.009
- Simons FE, Lieberman PL, Read EJ Jr, Edwards ES. Hazards of unintentional injection of epinephrine from autoinjectors: a systematic review. Ann Allergy Asthma Immunol. 2009;102(4):282-7. https://doi.org/10.1016/s1081-1206(10)60332-8
- Simons FE, Edwards ES, Read EJ Jr, Clark S, Liebelt EL. Voluntarily reported unintentional injections from epinephrine auto-injectors. J Allergy Clin Immunol. 2010;125(2):419-23.e4. https://doi.org/10.1016/j.jaci.2009.10.056
- Portnoy J, Wade RL, Kessler C. Patient Carrying Time, Confidence, and Training with Epinephrine Autoinjectors: The RACE Survey. J Allergy Clin Immune Pract. 2019;7(7):2252-61. https://doi.org/10.1016/j.jaip.2019.03.021
- Murata MA, Yamamoto LG. Patient/parent administered epinephrine in acute anaphylaxis. Am J Emerg Med. 2021;46:499-502. https://doi.org/10.1016/j.ajem.2020.10.060
- Bilò MB, Martini M, Tontini C, Corsi A, Antonicelli l. Anaphylaxis Eur Ann. Allergy Clin Immunol. 2021;53(1):4-17. https://doi.org/10.23822/eurannaci.1764-1489.158
- Muraro A, Worm M, Alviani C, Cardona V, et al; European Academy of Allergy and Clinical Immunology, Food Allergy, Anaphylaxis Guidelines Group. EAACI guidelines: Anaphylaxis Allergy. 2022;77(2):357-377. https://doi.org/10.1111/all.15032
- Song TT, Brown D, Karjalainen M, Lehnigk U, Lieberman P. Value of a second dose of epinephrine during anaphylaxis: a patient/caregiver survey. J Allergy Clin Immunol Pract. 2018;6(5):1559-67. https://doi.org/10.1016/j.jaip.2018.01.019