
Vol. 25 - Num. 100
Originales
Intervención interdisciplinaria para la prevención primaria de la caries en lactantes de 0 a 18 meses
Rosa Juanola Mercadera, M.ª Lluïsa Ribas Casalsb, Anna Fàbrega Rierac, Laura Company Ardilad, M.ª Mercè Fina Rodejae, Silvia Pons Salvadore, Ruth Martí Lluchf, Jordi Blanchg
aEnfermera. ABS Vilafant. Gerona. España.
bEnfermera. ABS Bàscara. Gerona. España.
cPediatra. ABS Bàscara. Gerona. España.
dPediatra. ABS Figueres. Gerona. España.
eOdontóloga. ABS Figueres. Gerona. España.
fBióloga. Institut Universitari per a la Recerca en Atenció Primària Jordi Gol I Gurina (IDIAPJGol). Barcelona. España.
gMatemático. Institut Universitari per a la Recerca en Atenció Primària Jordi Gol I Gurina (IDIAPJGol). Barcelona. España.
Correspondencia: R Juanola. Correo electrónico: rjuanola.girona.ics@gencat.cat
Cómo citar este artículo: Juanola Mercader R, Ribas Casals ML, Fàbrega Riera A, Company Ardila L, Fina Rodeja MM, Pons Salvador S, et al. Intervención interdisciplinaria para la prevención primaria de la caries en lactantes de 0 a 18 meses . Rev Pediatr Aten Primaria. 2023;25:367-76. https://doi.org/10.60147/5898493f
Publicado en Internet: 14-11-2023 - Número de visitas: 14069
Resumen
Introducción: la caries es la enfermedad crónica más frecuente en la infancia. La presencia de caries en la dentición temporal es el principal factor de riesgo para desarrollar caries en la dentición definitiva. La mayoría de los factores de riesgo de la caries son modificables y pueden convertirse en elementos para la prevención y control de la enfermedad. Con el objetivo de reducir la incidencia de caries a la edad de 18 meses se diseña una intervención interdisciplinaria de prevención primaria dirigida a familias con niños que se visitan siguiendo el Protocol d’activitats preventives i de promoció de la salut a l’edat pediátrica (PAPPS).
Material y métodos: ensayo clínico no aleatorizado, realizado en dos centros de asistencia primaria de Catalunya desde enero de 2019 hasta junio de 2022. En uno de los centros se diseñó e implementó una intervención educativa de prevención primaria de la caries con consejos y habilidades para las familias. En el otro centro se mantuvo el protocolo habitual de recomendaciones. Se evaluó y comparó la incidencia de caries en ambos grupos a la edad de 18 meses con un modelo de regresión logística estimado con el programa R.
Resultados: la incidencia de caries a los 18 meses fue superior en los niños del grupo control (OR = 6,0; IC 95% 1,8-20,2), a pesar de que la valoración del riesgo de caries basada en el sistema llamado Caries Management by Risk Assessment (CAMBRA) indicó mayor riesgo de desarrollo de caries en los lactantes del grupo intervención.
Conclusión: la intervención interdisciplinaria de prevención primaria de la caries incorporada en los programas de salud infantil reduce la incidencia de caries en los primeros años de vida.
Palabras clave
● Atención Primaria ● Caries dental ● Educación en salud dental ● Flúor ● Prevención primariaINTRODUCCIÓN
La caries es la enfermedad crónica infantil más frecuente. Estudios epidemiológicos recientes realizados en preescolares españoles muestran una prevalencia de caries del 17,4% en los niños de 3 años, y de hasta un 36,7% a la edad de 5 años1,2. En el área geográfica de influencia de nuestro centro de salud, la prevalencia de caries observada en el año 2021 fue del 54% en los escolares de 6 años.
La etiología de la aparición de caries es multifactorial, si bien hay tres factores esenciales que deben coincidir y mantenerse en el tiempo: características del huésped (dientes y saliva), presencia de microorganismos y dieta rica en azúcares1. Otros factores de riesgo asociados a la formación de caries en la primera infancia son: insuficiente higiene oral, poca exposición al flúor, colonización oral bacteriana precoz, antecedentes familiares de caries o bajo nivel socioeconómico3. La mayoría de estos factores son modificables, por lo que pueden convertirse en elementos susceptibles de intervención para la prevención de la enfermedad1,3,4.
La presencia de caries en la dentición temporal es el principal factor de riesgo para desarrollar caries en la dentición definitiva5,6, además de conllevar morbilidad asociada como infecciones periodontales, odontalgias, pérdida de dientes e incluso anorexia con repercusión ponderal5.
Las intervenciones interdisciplinarias educativas, dirigidas a los cuidadores de los niños de 0 a 3 años, que tienen por objetivo mejorar los hábitos alimentarios y la higiene oral han demostrado ser efectivos y eficientes en la reducción de la prevalencia de caries1,3,5,7,8. Estas intervenciones se pueden integrar en el ámbito de atención primaria (AP), en las visitas de seguimiento del Protocol d’activitats preventives i de promoció de la salut a l’edat pediátrica (PAPPS), tal y como recomienda la Organización Mundial de la Salud (OMS)2,5. Actualmente, la educación sanitaria realizada en dicho programa de salud no incluye algunas de las últimas recomendaciones que se han demostrado eficaces, como son el uso de la pasta con 1000-1450 partes por millón (ppm) de flúor desde la erupción del primer diente, el inicio de las revisiones odontológicas al año de vida o consejos sobre prevención de transmisión de microorganismos de la flora oral a los bebés1,2,4,7,9,10.
El Programa de salud bucodental vigente en Cataluña inicia el cribado de la caries en la visita odontológica durante el embarazo, y posteriormente no incluye ninguna visita odontológica pediátrica hasta la edad preescolar (4-6 años), a pesar de la evidencia existente de que un inicio precoz del cribado de caries permite hacer un tratamiento más efectivo.
Por todo ello, el objetivo principal de este trabajo es reducir la incidencia de caries infantil a la edad de 18 meses, mediante una intervención interdisciplinaria de prevención primaria dirigida a las familias con niños recién nacidos atendidos en las visitas del PAPPS.
MATERIAL Y MÉTODOS
Diseño: ensayo clínico no aleatorizado, realizado en las áreas básicas de salud (ABS) de Figueres (grupo intervención) y Roses (grupo control), desde enero de 2019 hasta junio de 2022.
Criterios de inclusión: recién nacidos que inicien el seguimiento del PAPPS en uno de los dos centros de atención primaria del estudio.
Criterios de exclusión:
- Diagnóstico de patologías relacionadas con alteraciones en la erupción dental, agenesias o alteraciones en la morfología dental: síndrome de Down, disostosis cleidocraneal, acondroplastia, displasia ectodérmica, síndrome de Gardner.
- Diagnóstico de síndromes asociados a hipoplasias del esmalte o de alteraciones genéticas de la estructura dental, como la amilogénesis imperfecta o la dentinogénesis imperfecta.
Tamaño de la muestra y procedimiento de muestreo: el tamaño de la muestra se calculó con el programa GRAMO11, aceptando un riesgo alfa de 0,05 y un riesgo beta inferior al 0,2 en un contraste bilateral y asumiendo una tasa de pérdida de seguimiento estimada del 20%, se estimó necesario 183 sujetos en cada grupo para detectar diferencias estadísticamente significativas en la proporción de incidencia de caries, que para el grupo control se estimó del 0,16 (a partir de datos objetivos de los propios centros de salud) y en el grupo intervención del 0,06 (utilizando la aproximación del ARCSINUS). El procedimiento de muestreo que se llevó a término fue no probabilístico consecutivo.
Intervención: el grupo intervención (ABS Figueres) implementó la intervención diseñada para este estudio, integrada en las visitas del PAPPS. El grupo control (ABS Roses) mantuvo la práctica clínica habitual según las recomendaciones del PAPPS (Tabla 1).
| Tabla 1. Actividades realizadas por el equipo de Pediatría del grupo intervención (ABS Figueres), por los equipos de Pediatría de ambos grupos y por los equipos de Odontología de las ABS de Figueres y Roses |
|---|
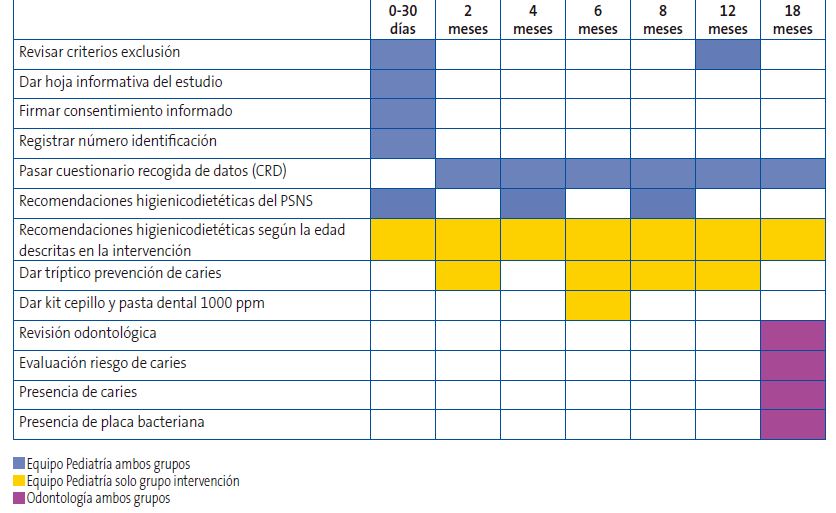 |
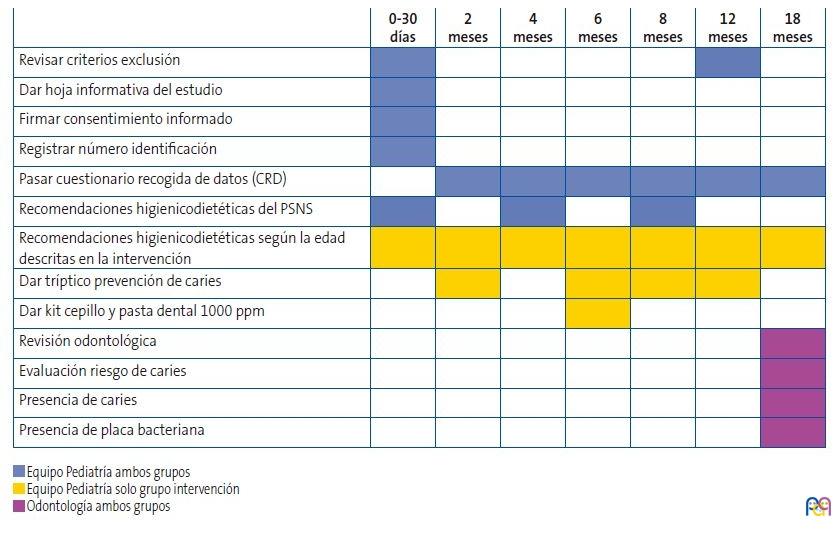
La intervención de prevención primaria interdisciplinaria diseñada en el estudio se llevó a cabo en el siguiente orden:
- El equipo de Odontología impartió una sesión de actualización de conocimientos sobre la caries al equipo de Pediatría: factores de riesgo prevenibles de la caries del lactante, técnicas y utensilios de higiene oral más adecuados, uso de flúor, maniobra de levantar el labio para detección de manchas blancas en los dientes.
- El equipo de Pediatría realizó las intervenciones de prevención primaria integradas dentro del PAPPS a las familias que entraban en el estudio.
- Formación desde la primera visita, capacitándolas para identificar y prevenir factores de riesgo cariogénico. Se les dio información oral durante la visita y se les entregó un tríptico explicativo elaborado por los equipos de Pediatría y Odontología, con recomendaciones sobre alimentación saludable, como evitar la transmisión de gérmenes vía oral entre los cuidadores y los lactantes, así como consejos y habilidades para realizar una adecuada higiene dental en función de la edad del lactante.
- Recomendaciones sobre el uso adecuado de pasta dental fluorada (1000-1450 ppm de flúor) desde la erupción del primer diente, con una demostración práctica de la cantidad de pasta necesaria y técnica para obtener la colaboración del niño durante la higiene oral. En la visita de control de los 6 meses se entregaba de forma gratuita un kit de higiene dental, compuesto por cepillos dentales y dedal para higiene oral/dental junto con un tubo de pasta dental fluorada de 1000 ppm de flúor. Todos los participantes de ambos grupos realizaron una visita con el odontólogo a los 18 meses de vida para detectar caries y valorar el riesgo de presentar caries precozmente (Tabla 1). La valoración del riesgo de caries precoz se realizó mediante el Protocolo de actuación en niños de alto riesgo de caries en diferentes edades y situaciones, elaborado por la Sociedad Española de Epidemiología y Salud Pública en el año 2013, basado en el sistema llamado CAMBRA12,13.
Variables: la variable dependiente del estudio fue la incidencia de caries a los 18 meses de edad, registrada por las profesionales de Odontología. Se consideró caries: observar una mancha blanca en el diente (lesión incipiente) o bien la presencia de cavitación. Como variable dependiente secundaria se estudió la valoración del riesgo de caries precoz realizado por los odontólogos según el sistema CAMBRA. Las variables independientes estudiadas fueron: uso de pasta dental de 1000-1450 ppm de flúor desde la erupción del primer diente (sí/no); alimentación nocturna a demanda sin higiene posterior (n.º veces/noche), los padres prueban los alimentos antes de dárselos al bebé (sí/no), los padres soplan los alimentos antes de dárselos al bebé (sí/no), los cuidadores dan besos en la boca al niño/a (sí/no), los padres limpian el chupete del bebé con la boca (sí/no).
Covariables: se registró la fecha de nacimiento y el sexo de los lactantes participantes en el estudio. Se recogió información de los padres y madres de otras covariables como: lugar de nacimiento, nivel de estudios, situación laboral y si la madre había realizado la visita del cribado odontológico durante el embarazo (sí/no). También se recolectó información en relación con el bebé sobre el tipo de lactancia (materna/artificial), la ingesta de azúcares refinados (sí/no), los hábitos de succión para dormir, los hábitos y métodos de higiene oral en las diferentes visitas de seguimiento.
Análisis de datos: se realizó un análisis descriptivo de la población estudiada para comparar los dos grupos. Las variables cuantitativas continuas normales se describen con la media y desviación estándar, las no normales con estadísticos de posición (percentiles) y las cualitativas con porcentajes. Se utilizó el test T-Student o el test U-Mann-Whitney para contrastes de variables continuas y el test exacto de Fisher para las categóricas.
Para conocer la efectividad de la intervención en la reducción de la incidencia de caries se ha seguido la estrategia de intención de tratar. Para analizar las diferencias dentro del mismo grupo antes y después de la intervención se han utilizado los test para datos aparejados. Para estimar la efectividad de la intervención en la aparición de caries se ha aplicado un modelo de regresión logística ajustado por las variables significativas en los análisis bivariantes. Se ha aplicado la corrección de Firth a la regresión logística para no tener un sesgo en la estimación de la verosimilitud cuando se estudian eventos raros.
Para comparar, la valoración del riesgo de caries con el sistema CAMBRA se ha calculado la proporción de “alto riesgo” y su intervalo de confianza (según el intervalo de puntuación de Wilson) para cada grupo.
El nivel de significación se fijó en el 0,05. El análisis de los datos se realizó mediante el programa R versión 4.2.1.
Consideraciones éticas: la investigación ha contado con el dictamen favorable del comité ético de investigación clínica de IDAP Jordi Gol con código P18/204. La invitación de las familias a participar en el estudio se realizó dentro de la visita del PAPPS del primer mes de vida del bebé. Se incluyeron todos los niños/as que no cumplían ningún criterio de exclusión, previa firma del documento de consentimiento informado.
RESULTADOS
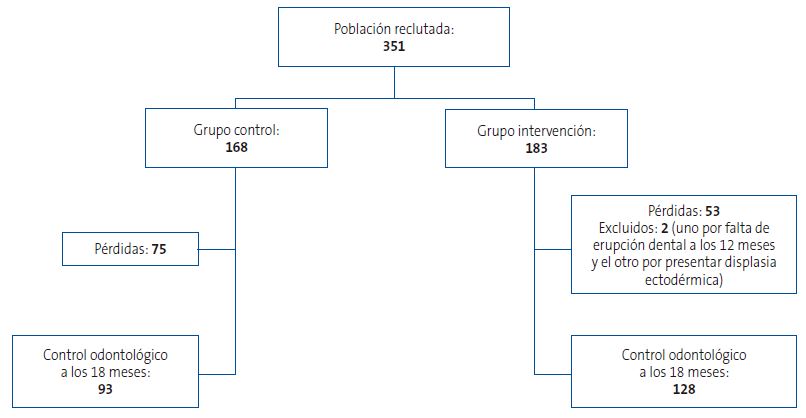
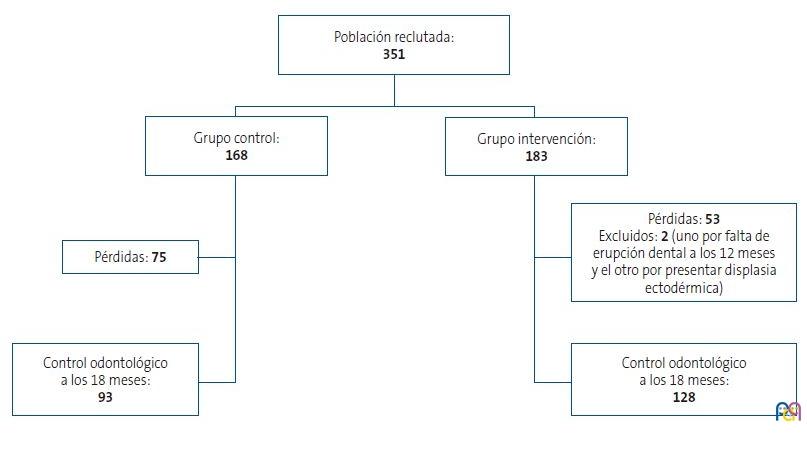
Cumplieron criterios de inclusión 351 familias, de las cuales 183 formaron parte del grupo intervención y 168 del grupo control. A la visita final odontológica de los 18 meses acudieron 128 familias del grupo intervención (69,9%,) y 93 familias del grupo control (55,4%). En la Figura 1 se muestra el flujo de participación.
| Figura 1. Población de estudio |
|---|
 |
La visita de cribado odontológico durante el embarazo fue realizada por 110 madres del grupo intervención (61,8%) y por 112 (72,3%) del grupo control (p = 0,109).
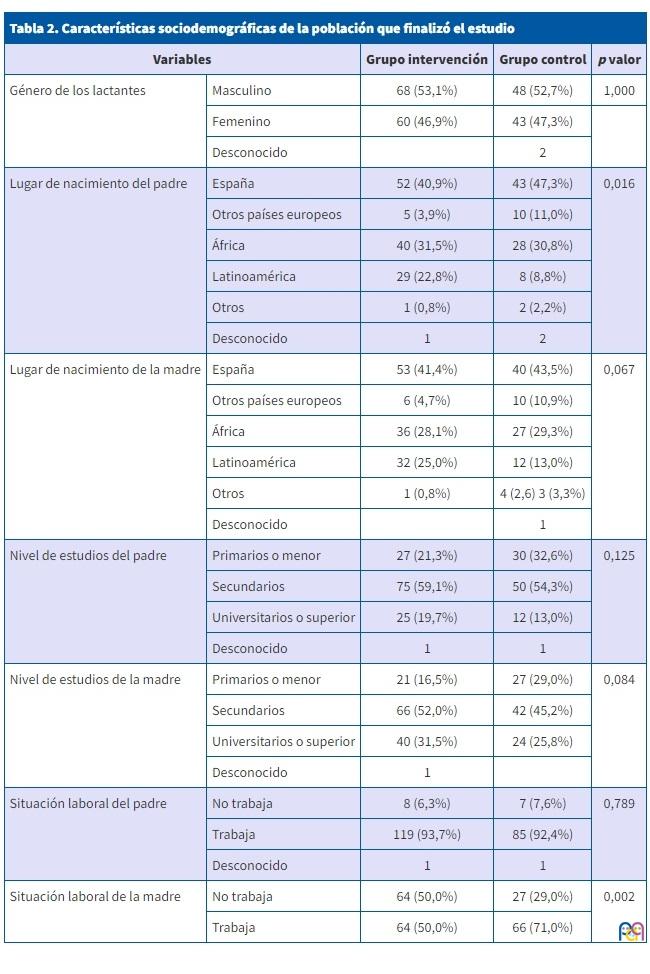
En la Tabla 2 se recogen las características sociodemográficas de las familias participantes. En ambos grupos el nivel de estudios medios era el más frecuente para ambos progenitores. Solamente se detectaron diferencias significativas entre el grupo control e intervención en dos variables, la situación laboral de las madres y el lugar de nacimiento de los padres. En el grupo control había mayor proporción de madres trabajadoras y un porcentaje mayor de progenitores nacido en España.
| Tabla 2. Características sociodemográficas de la población que finalizó el estudio | ||||
|---|---|---|---|---|
| Variables | Grupo intervención | Grupo control | p valor | |
| Género de los lactantes | Masculino | 68 (53,1%) | 48 (52,7%) | 1,000 |
| Femenino | 60 (46,9%) | 43 (47,3%) | ||
| Desconocido | 2 | |||
| Lugar de nacimiento del padre | España | 52 (40,9%) | 43 (47,3%) | 0,016 |
| Otros países europeos | 5 (3,9%) | 10 (11,0%) | ||
| África | 40 (31,5%) | 28 (30,8%) | ||
| Latinoamérica | 29 (22,8%) | 8 (8,8%) | ||
| Otros | 1 (0,8%) | 2 (2,2%) | ||
| Desconocido | 1 | 2 | ||
| Lugar de nacimiento de la madre | España | 53 (41,4%) | 40 (43,5%) | 0,067 |
| Otros países europeos | 6 (4,7%) | 10 (10,9%) | ||
| África | 36 (28,1%) | 27 (29,3%) | ||
| Latinoamérica | 32 (25,0%) | 12 (13,0%) | ||
| Otros | 1 (0,8%) | 4 (2,6) 3 (3,3%) | ||
| Desconocido | 1 | |||
| Nivel de estudios del padre | Primarios o menor | 27 (21,3%) | 30 (32,6%) | 0,125 |
| Secundarios | 75 (59,1%) | 50 (54,3%) | ||
| Universitarios o superior | 25 (19,7%) | 12 (13,0%) | ||
| Desconocido | 1 | 1 | ||
| Nivel de estudios de la madre | Primarios o menor | 21 (16,5%) | 27 (29,0%) | 0,084 |
| Secundarios | 66 (52,0%) | 42 (45,2%) | ||
| Universitarios o superior | 40 (31,5%) | 24 (25,8%) | ||
| Desconocido | 1 | |||
| Situación laboral del padre | No trabaja | 8 (6,3%) | 7 (7,6%) | 0,789 |
| Trabaja | 119 (93,7%) | 85 (92,4%) | ||
| Desconocido | 1 | 1 | ||
| Situación laboral de la madre | No trabaja | 64 (50,0%) | 27 (29,0%) | 0,002 |
| Trabaja | 64 (50,0%) | 66 (71,0%) | ||
La incidencia acumulada de caries en el grupo intervención fue significativamente menor que en el grupo control. Se detectaron 3 casos en el grupo intervención (2,3%; IC 95%: 0,8-6,7%) y 13 casos en el grupo control (14,0%; IC 95%: 8,4-22,5%). Los resultados de la regresión logística mostraron que el riesgo de presentar caries en los pacientes del grupo control fue 6 veces superior al del grupo intervención (odds ratio 6,0; IC 95%: 1,8-20,2). Ninguna de las variables de ajuste de las incluidas en la Tabla 2 fue significativa.
La valoración del riesgo de caries precoz realizado a los 18 meses por Odontología según el sistema CAMBRA indicó una mayor proporción de “alto riesgo” de desarrollo de caries en el grupo intervención. Se asignó “alto riesgo” a 69 participantes del grupo intervención (55,2%; IC 95%: 46,5-63,6%) y 21 participantes del grupo control (31,3%; IC 95%: 21,5-43,2%).
Se analizó si existían diferencias en la incidencia de caries en relación con la información recogida al bebé sobre el tipo de lactancia (materna/artificial), la ingesta de azúcares refinados (sí/no) y los hábitos de succión para dormir (chupete/pecho/biberón) (Tabla 3).
| Tabla 3. Incidencia de caries en relación con el tipo de lactancia materna, ingesta de azúcares refinados y hábitos de succión al dormir. Se indica la incidencia y el intervalo de confianza del 95% | ||||||
|---|---|---|---|---|---|---|
| Intervención | Control | |||||
| N | Incidencia | N | Incidencia | p valor | ||
| Tipo de lactancia materna | ||||||
| Lactancia materna durante 12 m | 0 | 3 | 11,5% (71,0-96,0) | 0,089 | ||
| Lactancia artificial o mixta a los 8 m | 2 | 2,1% (0,6-7,3) | 7 | 12,7% (6,3-24,0) | 0,012 | |
| Ingesta de azúcares refinados durante el primer año de vida | ||||||
| No ingesta | 1 | 2,1% (0,4-11,1) | 3 | 10,7% (3,7-27,2) | 0,144 | |
| Ingesta | 1 | 1,4% (0,2-7,4) | 5 | 11,9% (5,2-25,0) | 0,024 | |
| Hábitos de succión al dormir | ||||||
| Pecho | 2 m | 0 | 6 | 14,3% (6,7-27,8) | 0,006 | |
| 4 m | 0 | 6 | 14,6% (6,9- 28,4) | 0,006 | ||
| 6 m | 1 | 1,8% (0,3 – 9,6) | 6 | 17,6% (8,3 -33,5) | 0,012 | |
| 8 m | 0 | 5 | 14,7% (6,4- 30,1) | 0,007 | ||
| 12 m | 0 | 5 | 17,2% (7,6-34,5%) | 0,008 | ||
| Biberón | 2 m | 1 | 5,3% (0,9- 24,6) | 4 | 21,1% (8,5- 43,3) | 0,340 |
| 4 m | 1 | 5,3% (0,9- 24,6) | 4 | 20,0% (8,1- 41,6) | 0,342 | |
| 6 m | 0 | 3 | 16,7% (5,8- 39,2) | 0,105 | ||
| 8 m | 2 | 7,4% (2,1 – 23,4 | 3 | 16,7% (5,8-39,2%) | 0,375 | |
| 12 m | 0 | 3 | 21,4% (7,6- 47,6) | 0,022 | ||
| Chupete | 2 m | 1 | 3,6% (0,6-17,7) | 0 | 1,000 | |
| 4 m | 1 | 3,3% (0,6-16,7) | 0 | 1,000 | ||
| 6 m | 2 | 7,7% (2,1-24,1) | 1 | 9,1% (1,6-37,7) | 1,000 | |
| 8 m | 0 | 2 | 15,4% (4,3- 42,2) | 0,091 | ||
| 12 m | 1 | 3,7% (0,7- 18,3) | 11 | 11,8% (3,3-34,3) | 0,549 | |
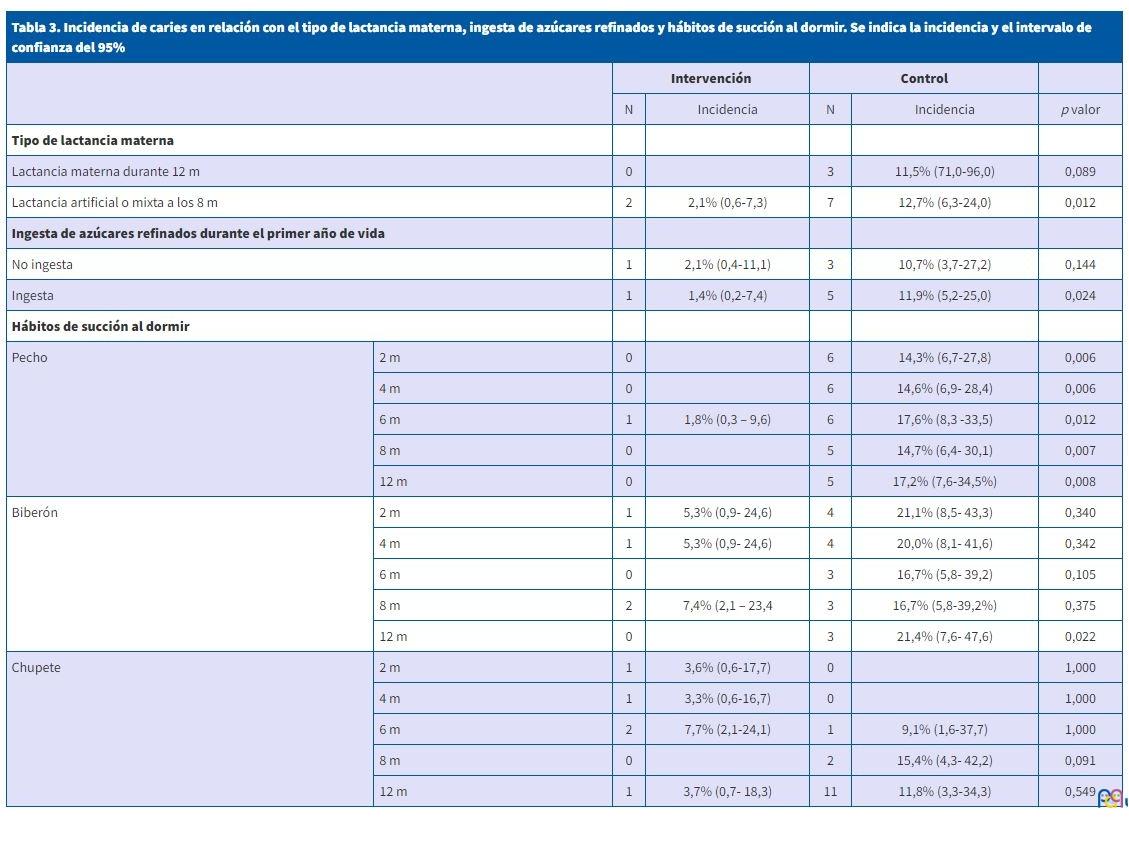
En los lactantes que se alimentaron exclusivamente de leche materna durante los primeros 12 meses de vida, la incidencia de caries no fue significativamente diferente entre el grupo control y el de intervención. En cambio, aquellos lactantes que recibieron lactancia artificial o mixta antes de los 8 meses de vida, la incidencia de caries fue significativamente mayor en el grupo control que en el de intervención (p = 0,012).
En cuanto a la ingesta de azúcares refinados, no hubo diferencias en la incidencia de caries entre el grupo control e intervención en los lactantes que no tomaron azúcar durante el primer año de vida. En cambio, en el grupo de lactantes que sí tomaron azúcar durante el primer año de vida la incidencia de caries fue significativamente superior (p = 0,024) en el grupo control en comparación al de intervención.
En referencia a los hábitos de succión para dormir, los lactantes que se duermen al pecho del grupo intervención presentan menos incidencia que aquellos del grupo control, esto es así en cualquier momento del seguimiento (2, 4, 6, 8 o 12 meses). Cuando el hábito de dormir es el biberón, solamente se observan diferencias significativas en la incidencia de caries entre intervención y control cuando este hábito se da a los 12 meses, pero no antes. No se observan diferencias cuando el hábito de dormir es el chupete en ningún momento del seguimiento.
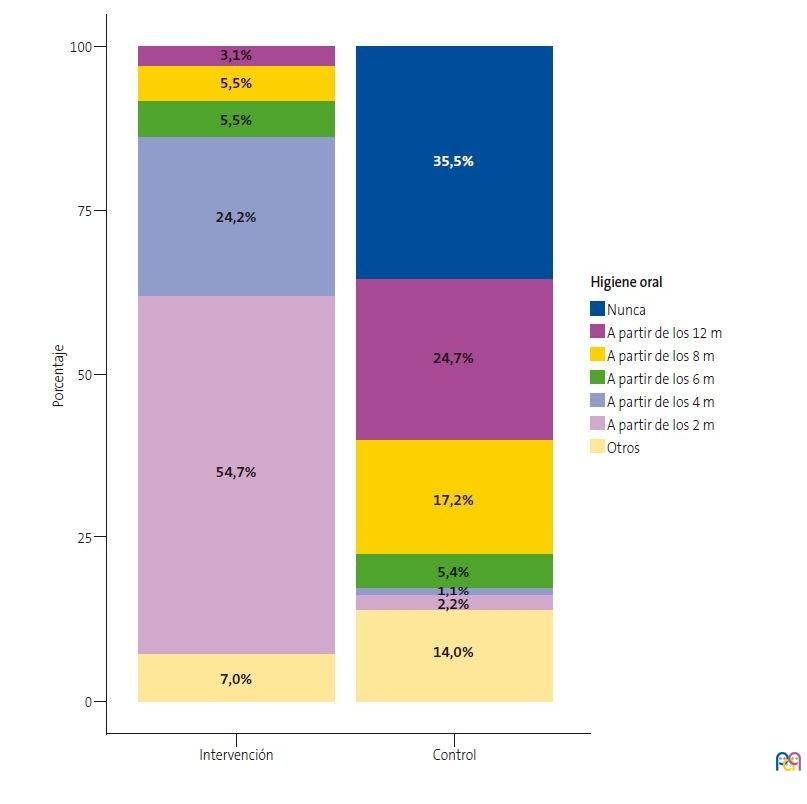
Los hábitos de higiene oral fueron diferentes en ambos grupos (p <0,01) (Figura 2). Dentro del grupo control, se observó que el 35,5% de los niños no recibieron ningún tipo de higiene oral dentro de su primer año de vida, mientras que todos los participantes del grupo intervención recibieron alguna intervención de higiene oral.
En relación con las otras variables recogidas (los padres prueban los alimentos antes de dárselos al bebé, soplan los alimentos antes de dárselos al bebé, dan besos en la boca al niño/a, limpian el chupete del bebé con la boca) no se pudo analizar su relación con la presencia de caries, puesto que después de los consejos facilitados a los padres durante la intervención no se produjeron cambios de hábitos.
| Figura 2. Porcentaje de niños que han recibido higiene oral en cada uno de los dos grupos |
|---|
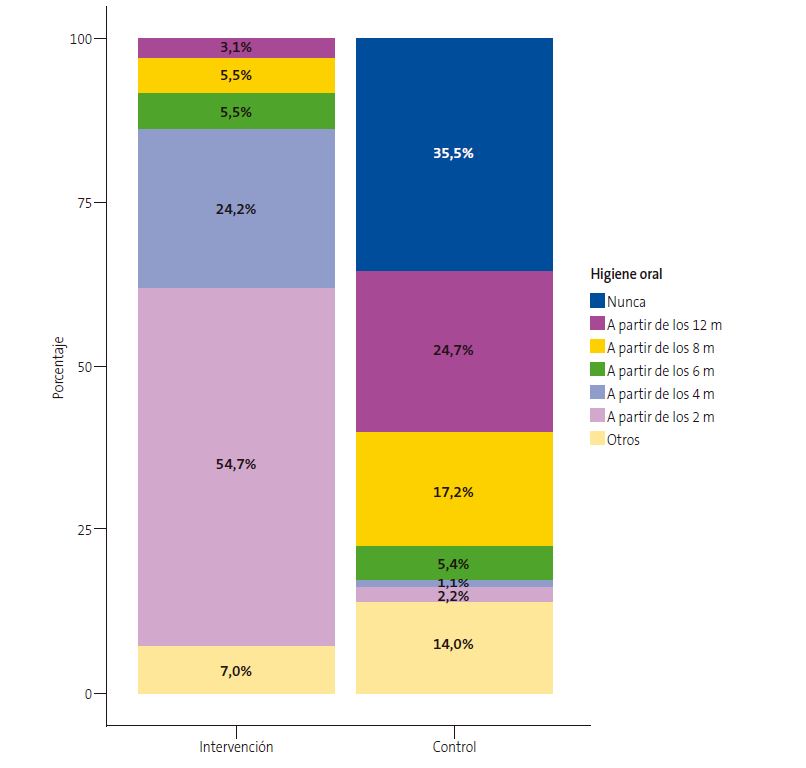 |
DISCUSION Y CONCLUSIONES
La intervención educativa para la prevención de la caries precoz integrada en las visitas de revisión rutinarias de los niños sanos en un centro de atención primaria ha resultado ser efectiva para reducir la incidencia de caries a los 18 meses de edad.
Además, en los lactantes que hacían lactancia artificial o mixta antes de los 8 meses de vida, y en aquellos a quienes se les introducían alimentos con azúcar durante el primer año de vida, la intervención se mostró efectiva. Las recomendaciones de higiene y reducción de ingesta de azucares refinados incluidas en dicha intervención están avaladas por la evidencia científica1,2.
Consideramos muy importante el enfoque multidisciplinar de la intervención, en la que han intervenido los profesionales de Pediatría, Enfermería y Odontología de los equipos de atención primaria. La experiencia ha sido muy positiva y subraya la importancia de trabajar de manera colaborativa. De hecho, también en Alemania se han implementado y evaluado programas multidisciplinarios para la prevención de la caries. En este caso, la intervención se realizaba en niños de entre 0 y 5 años, obteniendo una reducción significativa de caries en los niños entre los 3 y 4 años. Los programas implementados han sido efectivos cuando se ha comenzado la prevención antes del nacimiento en las visitas con Ginecogía y matronas, y después con pediatras, servicios sociales y odontólogos7,14. En nuestra investigación no se ha podido establecer relación entre las visitas a Odontología de cribado de las embarazadas y la presencia de caries en los lactantes, a pesar de que en estas visitas se hacen intervenciones educativas para el cuidado de la boca del bebé, siguiendo el protocolo vigente en nuestra región sanitaria.
La valoración del riesgo de caries a la edad de 18 meses12 y primera visita a Odontología alrededor del año de vida permite iniciar la prevención primaria de la caries a los lactantes con más riesgo, así como también detectar lesiones precozmente. Los resultados del estudio muestran un riesgo de desarrollo de caries superior del grupo intervención en relación con el grupo control, ya que los niños del grupo intervención tenían más probabilidad de presentar caries, pero aun así la intervención ha mostrado su efectividad.
En un ensayo clínico controlado, publicado por un grupo irlandés de odontólogos, en el que se realizaron intervenciones preventivas en niños de 2 y 3 años, no se obtuvieron diferencias estadísticamente significativas en la aparición de caries15, aunque sí se demostró efectividad en la disminución de la progresión de las caries en los niños a quienes hicieron la intervención preventiva. Este grupo promovía la higiene dental de los niños con dentífricos con concentraciones de flúor de 1450 ppm, como recomiendan los últimos protocolos odontopediátricos6,8,10, y aplicaba tratamientos preventivos con barnices de flúor a los niños de riesgo. El hecho de que la intervención llevada a cabo estuviera dirigida a edades más tempranas, explicaría que sí se hayan encontrado diferencias en la aparición de caries. Con los resultados del estudio y los encontrados por el grupo irlandés, se podría sugerir que las intervenciones preventivas desde el nacimiento ─y mantenidas durante los 3 años─ pueden ser beneficiosas tanto para disminuir la incidencia de caries como para disminuir la progresión de la misma. De cara a futuras investigaciones sería interesante analizar la incidencia de caries de los niños entre de 3 y 4 años a los que se ha valorado el riesgo de caries en el primer año de vida.
El estudio presenta como principal fortaleza el hecho de ser pionero en la evaluación de una intervención de prevención primaria de caries tipo multidisciplinar y en una edad tan precoz, no existiendo hasta la fecha estudios similares dirigidos a población pediátrica de 18 meses Las limitaciónes más importantes son las inherentes al propio diseño, ya que no ha habido aleatorización de los participantes, aunque las variables recogidas en la línea basal no fueron muy diferentes entre los dos grupos. También el hecho de que el proyecto se desarrollara durante los años 2020 y 2021, coincidiendo con la situación de pandemia de la COVID-19, influyó negativamente en el número de visitas de seguimiento de los participantes por las dificultades de acceso a los centros de atención primaria, y ha propiciado un tamaño muestral final inferior al esperado, aunque suficiente para detectar diferencias significativas en la incidencia de caries entre los dos grupos, el objetivo principal del estudio.
La conclusión principal del estudio es que la intervención interdisciplinaria de prevención primaria de la caries incorporada en los programas de salud infantil reduce la incidencia de caries a los 18 meses de edad. Además, la detección precoz de los lactantes con más riesgo de caries permite iniciar más temprano los tratamientos para la prevención de lesiones.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Contribución de los autores: redacción y revisión del manuscrito (todos), trabajo de campo (RJM, MLLRC, AFR, LCA, MMFR, SPS).
ABREVIATURAS
AP: atención primaria · CAMBRA: Caries Management by Risk Assessment · OMS: Organización Mundial de la Salud · PAPPS: Protocol d’activitats preventives i de promoció de la salut a l’edat pediátrica.
BIBLIOGRAFÍA
- Catalá Pizarro M, Cortés Lillo O. La caries dental: una enfermedad que se puede prevenir. An Pediatría Contin. 2014;12(3):147-51.
- Anil S, Anand PS. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Front Pediatr.2017;5:1-7. https://doi.org/10.3389/fped.2017.00157
- Statement P. Maintaining and Improving the Oral Health of Young Children. Pediatrics. 2014;134(6):1224-9. https://doi.org/10.1542/peds.2014-2984
- Phantumvanit P, Makino Y, Ogawa H, Rugg-Gunn A, Moynihan P, Petersen PE, et al. WHO Global Consultation on Public Health Intervention against Early Childhood Caries. Community Dent Oral Epidemiol. 2018;46(3):280-287. https://doi.org/10.1111/cdoe.12362
- Hernández M. Diagnóstico, pronóstico y prevención de la caries de la primera infancia. En: Gaceta dental: Ciencia y clínica. 2017 [en línea] [consultado el 07/11/2023]. Disponible en https://gacetadental.com/2017/12/diagnostico-pronostico-prevencion-la-caries-la-primera-infancia-15235/
- Winter J. Implementation and evaluation of an interdisciplinary preventive program to prevent early childhood caries. Clin Oral Investig. 2019 Jan;23(1):187-97. https://doi.org/10.1007/s00784-018-2426-x
- Sedrak MM, Doss LM, Doss LM. Open Up and Let Us In: An Interprofessional Approach to Oral Health. Pediatr Clin North Am. 2018 Feb;65(1):91-103. https://doi.org/10.1016/j.pcl.2017.08.023
- Bernstein J, Gebel C, Vargas C, Geltman P, Walter A, Garcia R, et al. Listening to paediatric primary care nurses: a qualitative study of the potential for interprofessional oral health practice in six federally qualified health centres in Massachusetts and Maryland. BMJ Open. 2017;7(3):e014124. https://doi.org/10.1136/bmjopen-2016-014124
- Wright JT, Hanson N, Ristic H, Whall CW, Estrich CG, Zentz RR. Fluoride toothpaste efficacy and safety in children younger than 6 years. J Am Dent Assoc. 2014;145(2):182-9. J Am Dent Assoc. 2014;145(2):182-9. https://doi.org/10.14219/jada.2013.37
- Protocol d’activitats preventives i de promoció de la salut a l’edat pediàtrica: infància amb salut. Scientia. 2008. En: Dipòsit d'Informació Digital del Departament de Salut. Generalitat de Catalunya [en línea] [consultado el 07/11/2023]. Disponible en https://hdl.handle.net/11351/1197
- Calculadora [en línea] [consultado el 07/11/2023]. Disponible en https://www.imim.cat/ofertadeserveis/software-public/granmo/
- Mateos Moreno MV. Llena Puy C, Rosario Garcillán Izquierdo M, Bratos Calvo E (revisores). Protocolos para la actuación con niños con alto riesgo de caries en diferentes edades y situaciones. 2013 [en línea] [consultado el 07/11/2023]. Disponible en https://sespo.es/wp-content/uploads/Protocolo-SESPO.-Actuacion-en-ninÌos-de-alto-riesgo-de-caries.pdf
- Maheswari SU, Raja J, Kumar A, Seelan RG. Caries management by risk assessment: A review on current strategies for caries prevention and management. J Pharm Bioallied Sci. 2015;7(2):S320-4. https://doi.org/10.4103/0975-7406.163436
- Wagner Y, Heinrich-Weltzien R. Evaluation of a regional German interdisciplinary oral health programme for children from birth to 5 years of age. Clin Oral Investig. 2017;21(1):225-35. https://doi.org/10.1007/s00784-016-1781-8
- Tickle M, O’Neill C, Donaldson M, Birch S, Noble S, Killough S, et al. A randomized controlled trial of caries prevention in dental practice. J Dent Res. 2017;96(7):741-6. https://doi.org/10.1177/0022034517702330