
Vol. 25 - Num. 99
Originales
Utilización de antibióticos en faringoamigdalitis aguda en la provincia de Albacete
Carlos Marcilla Vázqueza, Juan Ríos Laordenb, Ángeles Lloret Callejoc, Francisco Tejada Cifuentesc, M.ª José Tirado Peláezc
aServicio de Pediatría. Complejo Hospitalario Universitario. Gerencia de Atención Integrada de Albacete. Albacete. España.
bPediatra. CS Zona VI. Gerencia de Atención Integrada de Albacete. Albacete. España.
cFarmacéutico de Atención Primaria. Gerencia de Atención Integrada de Albacete. Albacete. España.
Correspondencia: C Marcilla. Correo electrónico: carlos.marcilla11@gmail.com
Cómo citar este artículo: Marcilla Vázquez C, Ríos Laorden J, Lloret Callejo A, Tejada Cifuentes F, Tirado Peláez MJ. Utilización de antibióticos en faringoamigdalitis aguda en la provincia de Albacete . Rev Pediatr Aten Primaria. 2023;25:e85-e90. https://doi.org/10.60147/7207cc49
Publicado en Internet: 02-10-2023 - Número de visitas: 13337
Resumen
Introducción: la faringoamigdalitis aguda (FAA) es una de las patologías más prevalentes en la población pediátrica y una de las principales causas de prescripción de antibióticos en este grupo de población.
Material y métodos: estudio observacional, descriptivo de utilización de antibióticos en FAA. La muestra del estudio son todos los niños del área que durante los tres años del estudio han recibido la prescripción de un antibiótico como tratamiento de una FAA.
Resultados: durante los tres años del proyecto se atendieron un total de 53 995 procesos de FAA, de los que 33 426 (61,9%) fueron tratados con antibióticos. Considerando los niños menores de 3 años, se atendieron un total de 10 901 procesos de FAA (20,2% del total de las FAA), de los que recibieron antibiótico 6494 (59,6%). En cuanto a la selección del antibiótico se utilizó preferiblemente penicilinas sensibles a betalactamasas (fenoximetilpenicilina, fenixometilpenicilina-benzatina) y amoxicilina: 60,3% el primer año, 60,9% el segundo y 66,8% el tercero; con menor uso de otros grupos antibióticos: amoxicilina-ácido clavulánico en 2475 procesos (18,2%) durante el primer año, 1754 (17,7%) durante el segundo y 1644 (16,6%) durante el tercero. También se observó menor uso de macrólidos: 2825 (20,7%) en el primer año del proyecto, 1933 (19,6%) en el segundo y 1419 (14,3%) en el último.
Conclusión: el uso de amoxicilina-ácido clavulánico y de macrólidos está muy por encima de lo esperado si consideramos la baja prevalencia de estado de portador de Streptococccus pyogenes a nivel faríngeo o la baja prevalencia de alergia a penicilina en la población pediátrica.
Palabras clave
● Antibióticos ● Faringoamigdalitis aguda ● Población pediátricaINTRODUCCIÓN
En la población pediátrica española se produce un alto consumo de antibióticos de uso sistémico a nivel comunitario1. De hecho, en 2019 ocupábamos el quinto lugar en mayor consumo de antibióticos entre los países europeos, teniendo en cuenta solo los datos relativos a consumo obtenidos con receta oficial financiada por el Sistema Nacional de Salud2. Este excesivo consumo no es exclusivo de ningún grupo etario, siendo el consumo en la población pediátrica también elevado3.
Una de las patologías más prevalentes en Pediatría es la faringoamigdalitis aguda (FAA), siendo una de las principales causas de prescripción de antibióticos en este grupo de población. Para evitar el sobretratamiento con antibióticos en esta patología, de etiología mayoritariamente vírica, se recomienda realizar estudio microbiológico, pues si nos basamos exclusivamente en la clínica hasta en un 20-25% de los pacientes realizaríamos un diagnóstico erróneo4-6. Ya en el documento de consenso sobre diagnóstico y tratamiento de FAA publicado en el año 2011 se remarca la importancia de realizar estudio microbiológico (test de detección rápida de antígeno estreptocócico o cultivo de muestra faringoamigdalar) en pacientes seleccionados, con criterios de infección estreptocócica probable y que no hayan recibido antibiótico previamente7. En la actualización de dicho documento, publicada en el año 2020, se recomienda realizar estudio microbiológico a todos los pacientes, basando la prescripción antibiótica únicamente en la clínica solo en los casos en los que no haya disponibilidad de estas pruebas microbiológicas4.
El objetivo de este trabajo es realizar un análisis del consumo y de la adecuación de la prescripción de antibióticos en la población pediátrica de la Gerencia de Atención Integrada de Albacete (España) en niños diagnosticados de FAA, analizando los resultados por grupos de población (estratificación por edades) y compararlo con las últimas recomendaciones establecidas en la actualización del documento de consenso sobre diagnóstico y tratamiento de FAA. La elevada muestra analizada permite realizar un análisis crítico de los principales puntos de inadecuación.
MATERIAL Y MÉTODOS
Estudio observacional, descriptivo, de utilización de medicamentos realizado sobre la prescripción de antibióticos en la población pediátrica de la Gerencia de Atención Integrada de Albacete.
La muestra del estudio son todos los niños del área de ambos sexos (0-14 años) que, durante el periodo del estudio de tres años de duración, han recibido la prescripción de al menos un antibiótico por un proceso de FAA. A continuación, se describen las variables que se han recogido para la realización del estudio, obtenidas del sistema de Información de AP (Turriano) del Servicio de Salud de Castilla la Mancha (SESCAM). Todos los datos se han codificado de forma anonimizada.
Los datos recogidos son:
- Día de la semana de prescripción; mes de la prescripción.
- Sexo y fecha de nacimiento del paciente.
- Diagnóstico: se utilizó la codificación del Código Internacional de Enfermedades 9.ª edición (CIE-9-MC) y de la Clasificación Internacional de AP (CIAP) (Tabla 1).
- Antibiótico: se utilizó el Sistema de Clasificación Anatómica Terapéutica, Química (ATC) del subgrupo farmacológico J01.
- Centro de salud.
| Tabla 1. Datos poblacionales, población con FAA y utilización de antibióticos | ||||
|---|---|---|---|---|
| Primer año | Segundo año | Tercer año | ||
| Población 0-14 años | Total | 38 857 | 38 303 | 38 299 |
| Atendidos por proceso de FAA | 19 868 | 16 882 | 17 245 | |
|
Atendidos por proceso de FAA y tratados con ATB (% del total) (% de los atendidos por FAA) |
13 633 (35,1%) (68,6%) |
9889 (25,8%) (58,6%) |
9904 (25,9%) (57,4%) |
|
| Población 0-3 años | Total | 6607 | 6192 | 6205 |
| Atendidos por proceso de FAA | 2999 | 4026 | 3876 | |
|
Atendidos por proceso de FAA y tratados con ATB (% del total) (% de los atendidos por FAA) |
2733 (45,4%) (91,1%) |
2187 (35,3%) (54,3%) |
1574 (25,4%) (40,6%) |
|
|
ATB: antibióticos; FAA: faringoamigdalitis aguda. |
||||
El estudio se ha realizado con arreglo a los principios de la Declaración de Helsinki y de la Ley Orgánica de Protección de Datos de entrada en vigor el 25 de mayo de 2018. Este estudio fue aprobado por el Comité Ético de Investigación con medicamentos (CEIm) del área.
RESULTADOS
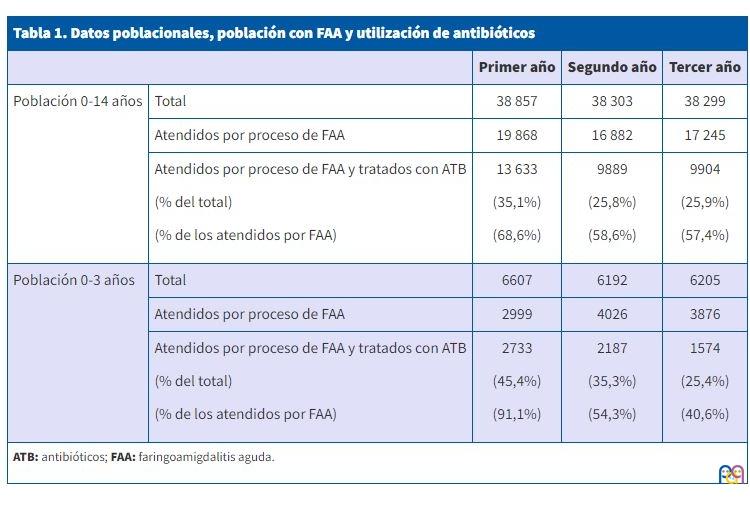
La población del estudio se mantuvo constante a lo largo de los tres años, de 38 857 niños de 0-14 años el primer año de estudio a 38 299 el último. Lo mismo ocurrió con la población menor de 3 años: 6607 en el primer año de estudio, 6192 en el segundo y 6205 en el tercero.
Durante el primer año, un 35,1% de la población pediátrica fue tratada con un antibiótico para un proceso de FAA, descendiendo posteriormente a un 25,8% en el segundo y 25,9% en el tercer año. Durante los tres años del proyecto se atendieron un total de 53 995 procesos de FAA, siendo la distribución por años muy similar: 19 868 niños en el primer año, 16 882 en el segundo y 17 245 en el tercero. Del total de procesos de FAA atendidos, fueron tratados con antibióticos 33 426 (61,9%). Si analizamos los procesos tratados por años, sí existieron importantes diferencias, descendiendo a lo largo del periodo de estudio: en el primer año recibieron tratamiento antibiótico 13 633 (68,6%), 9889 (58,6%) en el segundo y 9904 (57,4%) en el tercero.
Considerando exclusivamente los niños menores de 3 años, que padecen con menor frecuencia esta patología y en los que el agente etiológico de la FAA es predominante virus, durante el periodo total del proyecto se atendieron un total de 10 901 procesos de FAA (20,2% del total de las FAA): 2999 el primer año, 4026 el segundo y 3876 el tercero. Del total, recibieron tratamiento antibiótico 6494 (59,6%), observando la misma tendencia a prescribir menos antibióticos con el paso de los años: 2733 procesos tratados en el primer año (91,1%), 2187 (54,3%) en el segundo y 1574 (40,6%) en el tercero (Tabla 1).
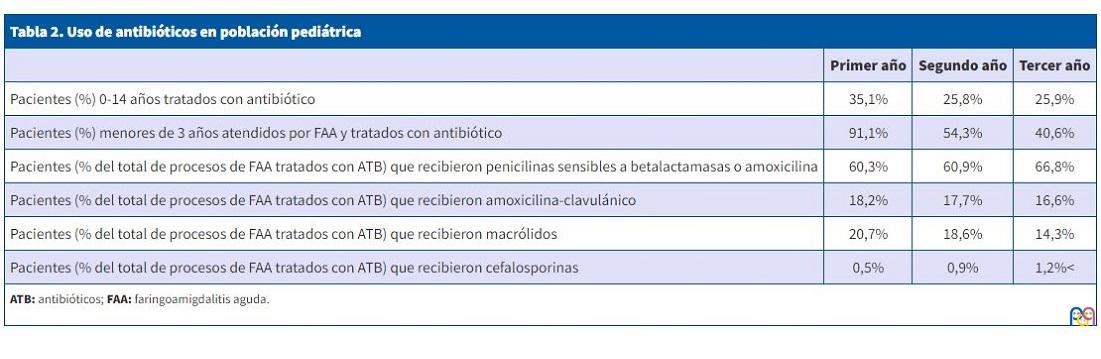
En cuanto a la selección del antibiótico para el tratamiento de FAA, al final del periodo analizado se observa un aumento del tratamiento con penicilinas sensibles a betalactamasas (incluyendo fenoximetilpenicilina y fenixometilpenicilina-benzatina) y amoxicilina, de 60,3% y 60,9 % en el primer y segundo año, respectivamente, a 66,8% en el último. Se empleó mayoritariamente la amoxicilina: 6725 procesos tratados en el primer año (81,4% del total de procesos tratados con penicilinas sensibles a betalactamasas o amoxicilina), 4760 (79%) en el segundo y 4916 (74,3%) en el tercero. Por el contrario, disminuyeron los procesos tratados con amoxicilina-ácido clavulánico respecto al total de procesos tratados con antibióticos a lo largo de los 3 años: 2475 (18,2%) en el primer año, 1754 (17,7%) en el segundo y 1644 (16,6%) en el tercero. Si consideramos el uso de este antibiótico respecto al total de diagnósticos de FAA observamos que recibieron amoxicilina-ácido clavulánico un 12,5% en el primer año, 10,4% en el segundo y 9,5% en el tercero.
Igualmente, los procesos de FAA tratados con macrólidos mostraron un descenso importante: 2825 (20,7%) en el primer año del proyecto, 1933 (19,6%) en el segundo y 1419 (14,3%) en el último. El empleo de este grupo antibiótico respecto al total de diagnósticos de FAA fue también considerable, pues el 14,2% del total de las FAA del primer año analizado fueron tratadas con macrólidos, descendiendo en los dos años posteriores a un 11,5% y 8,2%. Dentro del grupo antibiótico de los macrólidos, el más empleado fue la azitromicina: 2797 procesos tratados en el primer año (99% respecto al total de macrólidos), 1905 (98,6%) en el segundo y 1405 (99%) en el tercero.
El empleo de cefalosporinas en el tratamiento de FAA fue menor que los grupos antibióticos previamente comentados. Se utilizaron solo en 95 procesos durante el primer año (0,7%), en 159 durante el segundo (1,6%) y en 201 en el último año (2%). Respecto al total de diagnósticos de FAA, este porcentaje es prácticamente insignificante: un 0,5% de las FAA del primer año de investigación fueron tratadas con cefalosporinas, un 0,9 % del total de FAA del segundo año y un 1,2 % del tercero. Dentro de ellas, las más utilizadas fueron cefuroxima y cefixima: 82 procesos tratados en el primer año (86,3% del total de las cefalosporinas), 142 (89,3%) en el segundo y en 188 (93,5%) en el tercero (Tabla 2).
| Tabla 2. Uso de antibióticos en población pediátrica | |||
|---|---|---|---|
| Primer año | Segundo año | Tercer año | |
| Pacientes (%) 0-14 años tratados con antibiótico | 35,1% | 25,8% | 25,9% |
| Pacientes (%) menores de 3 años atendidos por FAA y tratados con antibiótico | 91,1% | 54,3% | 40,6% |
| Pacientes (% del total de procesos de FAA tratados con ATB) que recibieron penicilinas sensibles a betalactamasas o amoxicilina | 60,3% | 60,9% | 66,8% |
| Pacientes (% del total de procesos de FAA tratados con ATB) que recibieron amoxicilina-clavulánico | 18,2% | 17,7% | 16,6% |
| Pacientes (% del total de procesos de FAA tratados con ATB) que recibieron macrólidos | 20,7% | 18,6% | 14,3% |
| Pacientes (% del total de procesos de FAA tratados con ATB) que recibieron cefalosporinas | 0,5% | 0,9% | 1,2% |
|
ATB: antibióticos; FAA: faringoamigdalitis aguda. |
|||
DISCUSIÓN
La FAA es un proceso infeccioso que cursa con inflamación de las mucosas de faringe y/o amígdalas, cuya etiología más frecuente es vírica. Dentro de las causas bacterianas, la principal es el Streptococcus pyogenes, responsable del 30-40% de las FAA que acontecen en niños mayores de 3 años. Por debajo de esta edad, la etiología bacteriana se reduce a un 10-14% de las mismas7-9. Si analizamos los resultados de nuestra investigación, el porcentaje de pacientes diagnosticados de FAA que han recibido tratamiento antibiótico es acorde a la prevalencia de la infección por Streptococcus pyogenes descrita en población pediátrica mayor de 3 años (35,1% en el primer año, con descenso en los dos años posteriores a un 25,8 y 25,9%). Este descenso puede explicarse por la introducción en los centros de salud, en el año 2018, de test de detección rápida de antígeno estreptocócico, que permite tratar a aquellos pacientes con infección confirmada, evitando los errores en el tratamiento que cometeríamos si considerásemos escalas de predicción clínica hasta en un tercio de los pacientes4,10,11. Los pacientes menores de 3 años atendidos por FAA y tratados con antibióticos son desproporcionadamente elevados, de un inadmisible 91,1% en el primer año, a un descenso significativo en los dos años posteriores, al 54,3% y 40,6%; aún así, muy por encima de lo esperable para este grupo de edad.
Las penicilinas sensibles a betalactamasas (incluyendo fenoximetilpenicilina y fenixometilpenicilina-benzatina) y la amoxicilina han sido los antibióticos más utilizados para el tratamiento de las FAA, entre 60,3% y 66,8%. La penicilina oral es el antibiótico de primera elección en el tratamiento de la FAA estreptocócica, siendo la amoxicilina la primera alternativa terapéutica. Ambos antibióticos son de espectros estrechos, seguros y eficaces y permiten una rápida mejoría de la clínica, prevenir complicaciones y reducir el tiempo de contagio4,12,13. Por tanto, la utilización de los mismos ha sido adecuada, siendo los antibióticos mayoritariamente empleados en este proceso, si bien podemos considerarla algo inferior a lo esperable teniendo en cuenta la baja incidencia de población pediátrica alérgica a penicilina (que oscila entre 1,7% y 5,2%, y en cuyo caso debería utilizarse cefalosporinas o macrólidos) o los casos de fracaso terapéutico o estado de portador4,14.
El tratamiento con amoxicilina-ácido clavulánico se administró entre el 9,5% y el 12,5% de los pacientes diagnosticados de FAA, según el año. Dicho antibiótico debe limitarse a pacientes con fracaso terapéutico o estado de portador con alguna de las siguientes particularidades: antecedentes personales o familiares de fiebre reumática, brotes intrafamiliares recurrentes de FAA o enfermedad invasiva por Streptococccus pyogenes del grupo A, pacientes portadores que viven en instituciones cerradas o conviven con inmunodeprimidos o pacientes en los que se contempla la amigdalectomía como último recurso terapéutico. Teniendo en cuenta que la prevalencia de estado de portador en niños es del 12%, el porcentaje de pacientes tratados con amoxicilina-ácido clavulánico es superior al esperado y más si consideramos que, en estos casos, existen otras alternativas terapéuticas también válidas, como clindamicina o azitromicina, entre otros4,7,15,16.
El uso de cefalosporinas se limitó a entre el 0,7 y el 2% de los pacientes tratados con antibióticos, estando dichos valores dentro de lo esperable si consideramos que entre el 1,7% y 5,2% de población pediátrica es alérgica a penicilina14. Sin embargo, dentro de las cefalosporinas, la elección del antibiótico no es adecuada, objetivando un elevado uso de cefalosporinas de segunda y tercera generación (principalmente cefuroxima y cefixima, que se han empleado en más del 85% de las FAA tratadas con cefalosporinas). Las cefalosporinas de primera generación son el tratamiento de elección en niños con reacción alérgica retardada a penicilina/amoxicilina, siendo el cefadroxilo el más apropiado según la mayoría de los consensos, por su adecuada tolerancia y espectro de actividad más reducido4,12,17,18.
Quizás el punto de mayor inadecuación encontrado en el estudio esté en el elevado uso de macrólidos (entre el 8,2% y el 14,2% de las FAA recibieron tratamiento con este grupo antibiótico, representando entre el 14,3% y el 20,7% del total de las FAA tratadas con antibióticos). Esta sobreutilización está muy por encima de la esperable en función de la escasa prevalencia de alergia a penicilina comentada en el párrafo anterior14. Los macrólidos deberían limitarse exclusivamente a pacientes con alergia inmediata o anafiláctica a betalactámicos4,7,12,17. El más frecuentemente empleado ha sido la azitromicina (en más del 98% de los casos en los tres años del estudio) siendo otro punto importante de inadecuación si consideramos que en los últimos años se ha visto un aumento de resistencias del Streptococcus beta-hemolítico del grupo A a macrólidos que, si bien es inferior al 10%, en aquellos con fenotipo M pueden ser muy superiores. Estos son resistentes solo a macrólidos de 14 y 15 átomos, entre los que se encuentra la azitromicina; por lo que la mejor opción en pacientes alérgicos son los macrólidos de 16 átomos, como josamicina y diacetil-midecamicina4,19.
Tras la obtención de los datos de 2017, se llevó a cabo una intervención de tipo formativo realizada sobre profesionales sanitarios del área, consistente en varias ediciones de un curso en el que se repasaron las indicaciones de antibioterapia en la FAA, así como los antibióticos a seleccionar según las características del paciente (fracaso terapéutico, estado de portador o alergia a penicilinas). Si bien observamos un menor uso de antibióticos y una mejor utilización de los mismos (mayor utilización de amoxicilina o penicilinas sensibles a betalactamasas y menor empleo de amoxicilina-ácido clavulánico y macrólidos) no podemos atribuir completamente esta mejoría a dicha actividad formativa, pero sí ayudan a insistir en la importancia de este tipo de actividades, así como en la monitorización de indicadores.
CONFLICTO DE INTERESES
Los autores declaran no presentar conflictos de intereses en relación con la preparación y publicación de este artículo.
RESPONSABILIDAD DE LOS AUTORES
Todos los autores han contribuido de forma equivalente en la elaboración del documento.
ABREVIATURAS
FAA: faringoamigdalitis aguda
BIBLIOGRAFÍA
- Albañil MR. Plan Nacional de Resistencia a Antibióticos. Form Act Pediatr Aten Prim. 2016;9: 56-9.
- European Centre for Disease Prevention and Control. Antimicrobial consumption in the EU/EEA, annual epidemiological report for 2019. Stockholm: ECDC; 2020:4-9 [en línea] [consultado el 14/09/2023]. Disponible en www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2019
- Malo S, Bjerrum l, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Prescripción antibiótica en infecciones respiratorias agudas en Atención primaria. An Pediatr. 2014;82:412-6.
- Piñeiro R, Álvez F, Baquero F, Cruz M, De la Flor i Bru J, Fernández A, et al. Actualización del documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2020;93(3):206e.1-206e.8.
- Gerber M, Shulman S. Rapid diagnosis of pharyngitis caused by group A Streptococci. Clin Microbiol Rev. 2004;17:571-80.
- Fine A, Nizet V, Mandl K. Large-Scale validation of the Centor and McIsaac scores to predict Group A streptococcal pharyngitis. Arch Intern Med. 2012;172:847-52.
- Piñeiro R, Hijano F, Álvez F, Fernández A, Silva JC, Pérez C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75(5):342e.1-342e.13.
- Álvez Ginzález F. Faringitis estreptocócica en niños menores de 2 años. An Pediatr (Barc). 2008;68:525-39.
- Shaikh N, Leonard E, Martin J. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a metaanalysis. Pediatrics. 2010;126:557-64.
- Ochoa Sangrador C, Andrés de Llano JM. Los síntomas y signos clínicos no son suficientemente válidos para diagnosticar la faringitis estreptocócica. Evid Pediatr. 2012;8:23.
- Le Marechal F, Martinot A, Duhamel A, Ptuvost I, Dubos F. Streptococcal pharyngitis in children: a meta-analysis of clinical decisión rules and their clinical variables. BMJ Open. 2013;3(3):e001482.
- Shulman ST, Bisno AL, Clegg HV, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-82.
- Van Driel ML, De Sutter AI, Habraken H, Thorning S, Christiaens T. Different antibiotic treatments for group A streptococcal pharyngitis. Cochrane Database Syst Rev. 2016;9.CD004406.
- Baquero F, Michavila A, Suárez Rodríguez A, Hernandez A, Martínez Campos l, Calvo C, et al. Documento de consenso de la Sociedad Española de Infectología Pediátrica, Sociedad Española de Inmunología Clínica y Alergia Pediátricas, Asociación Española de Pediatría de Atención Primaria y Sociedad Española de Pediatría Extrahospitalaria y Atención Primaria sobre antibioterapia en alergia a penicilina o Amoxicilina. An Pediatr (Barc) 2017;86:99.e1-99.e9.
- Oliver J, Malliya Wadu E, Pierse N, Moreland NJ, Williamson DA, Baker MG. Group A Streptococcus pharyngitis and pharyngeal carriage: A meta-analysis. PLoS Negl Trop Dis. 2018;12(3):e0006335.
- Shulman ST, Tanz RR, Dale JB, Beall B, Kabat W, Kabat K, et al. Seven-year surveillance of north american pediatric group A streptococcal pharyngitis isolates. Clin Infect Dis. 2009;49:78-84.
- Pichichero M. Treatment and prevention of streptococcal pharyngitis. 2019 [en línea] [consultado el 14/09/2023]. Disponible en https://sso.uptodate.com/contents/treatment-and-prevention-of-streptococcal-pharyngitis-in-adults-and-children
- Campagna JD, Bond MC, Schabelman E, Hayes BD. The use of cephalosporins in penicillin-allergic patients: a literatura review. J Emerg Med. 2012;42:612-20.
- Calle Miguel l, Pérez Méndez C, Miguel Martínez MD, Lombraña Álvarez E, García García E, Solís Sánchez G. Cambios evolutivos en las tasas y fenotipos de resistencia de Streptococcus pyogenes en una población pediátrica de Asturias, España (2005-2015). Rev Esp Quimioter. 2017;30:90-5.